CE / CME
Evolving Treatment Landscape for Early-Stage TNBC With and Without gBRCAm
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 26, 2026
Expiration: December 25, 2026

Activity
Management of Common and Potentially Severe Toxicities Associated With Sacituzumab Govitecan
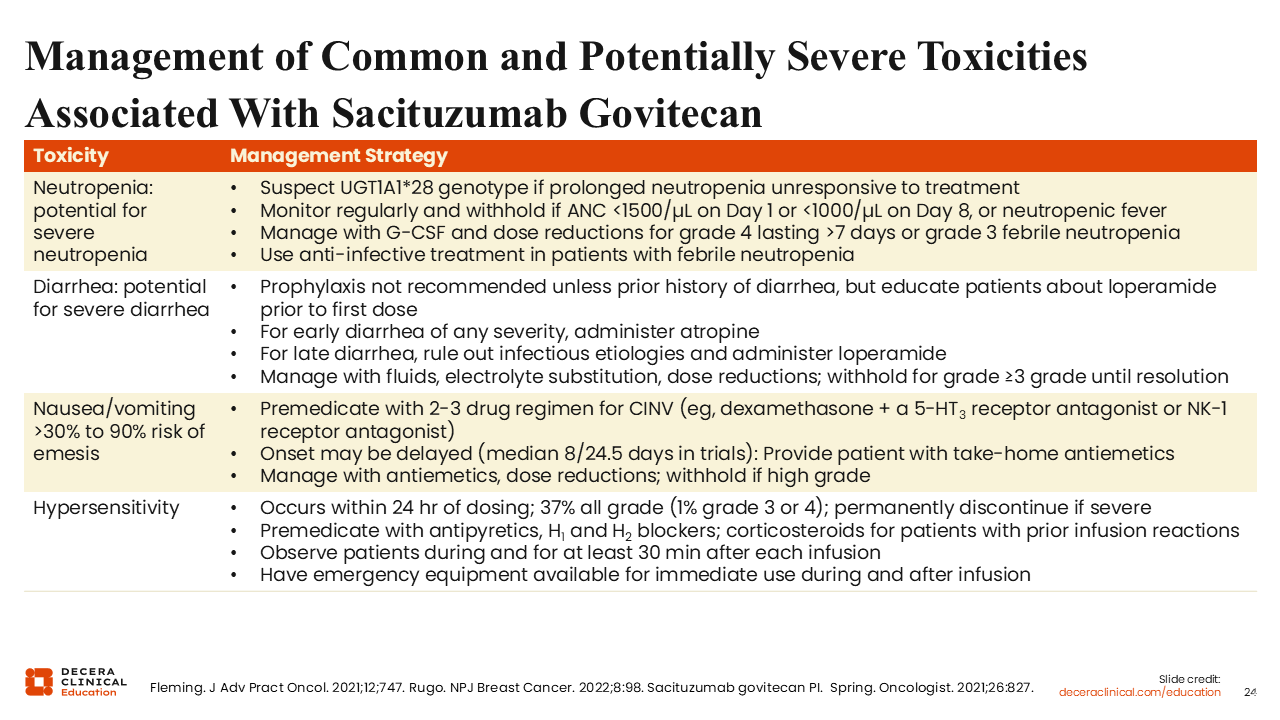
Clinically important AEs associated with sacituzumab govitecan include neutropenia (64%), diarrhea (64%), nausea (64%) and vomiting (35%), and hypersensitivity (35%) reactions.37,43,44 Because sacituzumab govitecan is administered on Days 1 and 8 of a 21-day cycle, symptom assessment and blood count monitoring are important before each dose.
Neutropenia can be severe (grade ≥3: 49%) and may require treatment delay, dose reduction, granulocyte colony–stimulating factor support, and anti-infective therapy if febrile neutropenia occurs. Treatment should be withheld for an absolute neutrophil count <1500/μL on Day 1, <1000/μL on Day 8, or for neutropenic fever.37 Prolonged or difficult-to-manage neutropenia should prompt consideration of factors that may increase toxicity risk, including reduced UGT1A1 activity. UGT1A1*28 homozygosity is associated with an increased risk of neutropenia, febrile neutropenia, and anemia.37 This reinforces the need for close monitoring and early intervention, particularly in patients who develop recurrent or severe cytopenias.
Diarrhea may occur early or later during treatment and should be managed according to timing, severity, and clinical context. For early-onset diarrhea, atropine may be used when clinically appropriate. For later-onset diarrhea, infectious causes should be ruled out, and management may include loperamide, oral or intravenous fluids, electrolyte replacement, treatment interruption, and dose reduction for more severe or persistent symptoms.37,44
Patients should receive loperamide instructions before the first dose so that diarrhea can be addressed promptly. This counseling should include when to start antidiarrheal therapy, when to call the care team, and which symptoms require urgent evaluation, such as persistent diarrhea, dizziness, fever, or signs of dehydration.
Nausea and vomiting can also be clinically meaningful. Premedication with a 2- or 3-drug antiemetic regimen is recommended, often including dexamethasone plus a 5-HT3 receptor antagonist and/or an NK1 receptor antagonist. Take-home antiemetics should also be provided because symptoms may be delayed.37,45
Hypersensitivity reactions can occur within 24 hours of dosing. Premedication may include antipyretics, H1 and H2 blockers, and corticosteroids for patients with prior infusion reactions. Patients should be observed during the infusion and for ≥30 minutes after each infusion. Severe hypersensitivity should prompt permanent discontinuation.37
Sacituzumab govitecan toxicity management should be structured before treatment begins. Patients should understand the importance of reporting fever, diarrhea, dehydration, nausea or vomiting, and infusion-related symptoms early. This approach can help reduce complications, support safe dosing, and prevent avoidable treatment discontinuation.
Management of Common and Potentially Severe Toxicities Associated With Datopotamab Deruxtecan (Dato-DXd)
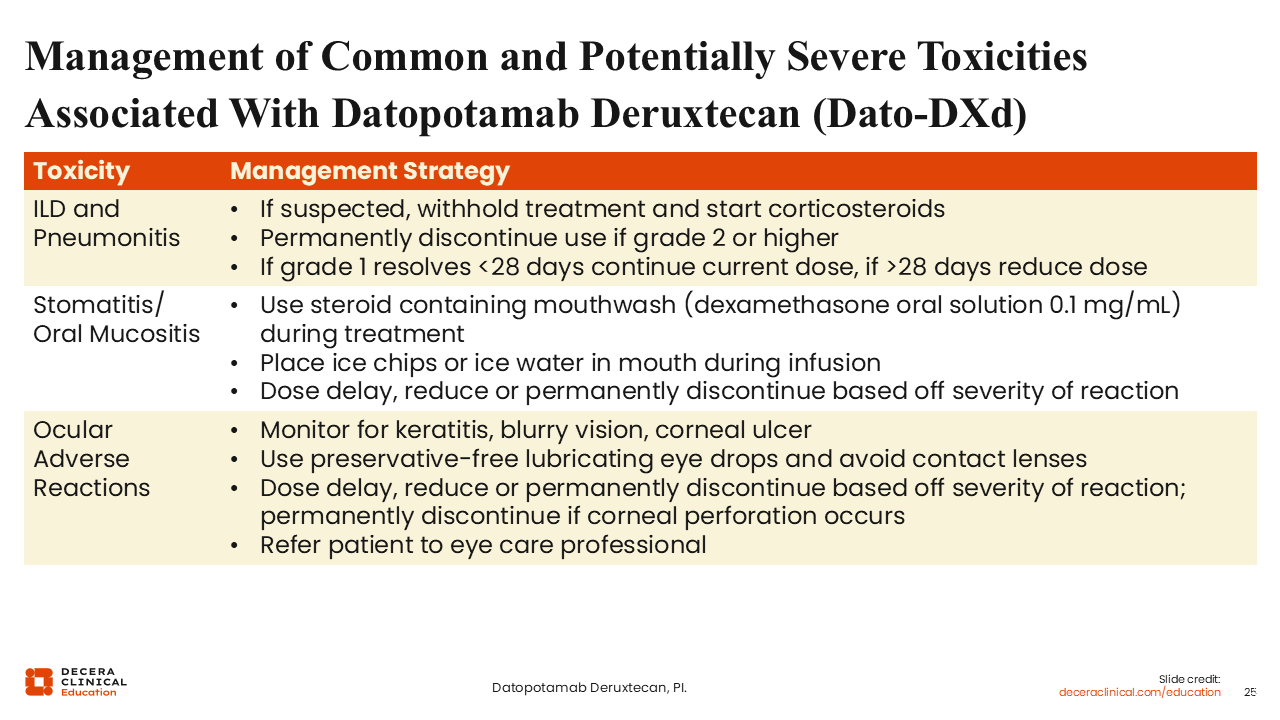
Dato-DXd requires proactive counseling and early toxicity surveillance because several AEs of special interest may begin subtly but become treatment limiting if not recognized and managed promptly. In the advanced disease setting, TROPION-Breast01, stomatitis/oral mucositis was the most common AE of special interest, occurring in 59% of patients treated with Dato-DXd vs 13% with investigator’s choice chemotherapy; grade ≥3 events occurred in 7% vs <1%, respectively. Median time to onset was 22 days, supporting the need for oral care counseling before treatment initiation, early symptom reporting, and prompt use of supportive measures such as steroid-containing mouthwash when clinically appropriate.38,46
Ocular surface events also require anticipatory management, occurring in 51% of patients receiving Dato-DXd vs 19% with chemotherapy; grade ≥3 events were reported in 3% vs 2%, respectively. Because these events may present as dry eye, blurred vision, keratitis, increased lacrimation, photophobia, or ocular discomfort, patients should be counseled to use prophylactic lubricating eye drops, avoid contact lenses unless directed otherwise, and report new or worsening eye symptoms early.38
ILD/pneumonitis was less frequent but clinically important because of its potential seriousness. Adjudicated ILD/pneumonitis occurred in 4.2% of patients treated with Dato-DXd vs 2.5% with chemotherapy; grade ≥3 events occurred in 1.1% vs 0%, respectively, and ILD/pneumonitis led to treatment discontinuation in 2.5% of Dato-DXd-treated patients. Patients should be counseled to report new or worsening cough, dyspnea, fever, or other respiratory symptoms promptly, and healthcare professionals should evaluate suspected cases early because dose interruption, corticosteroids, or permanent discontinuation may be required depending on severity.38,46
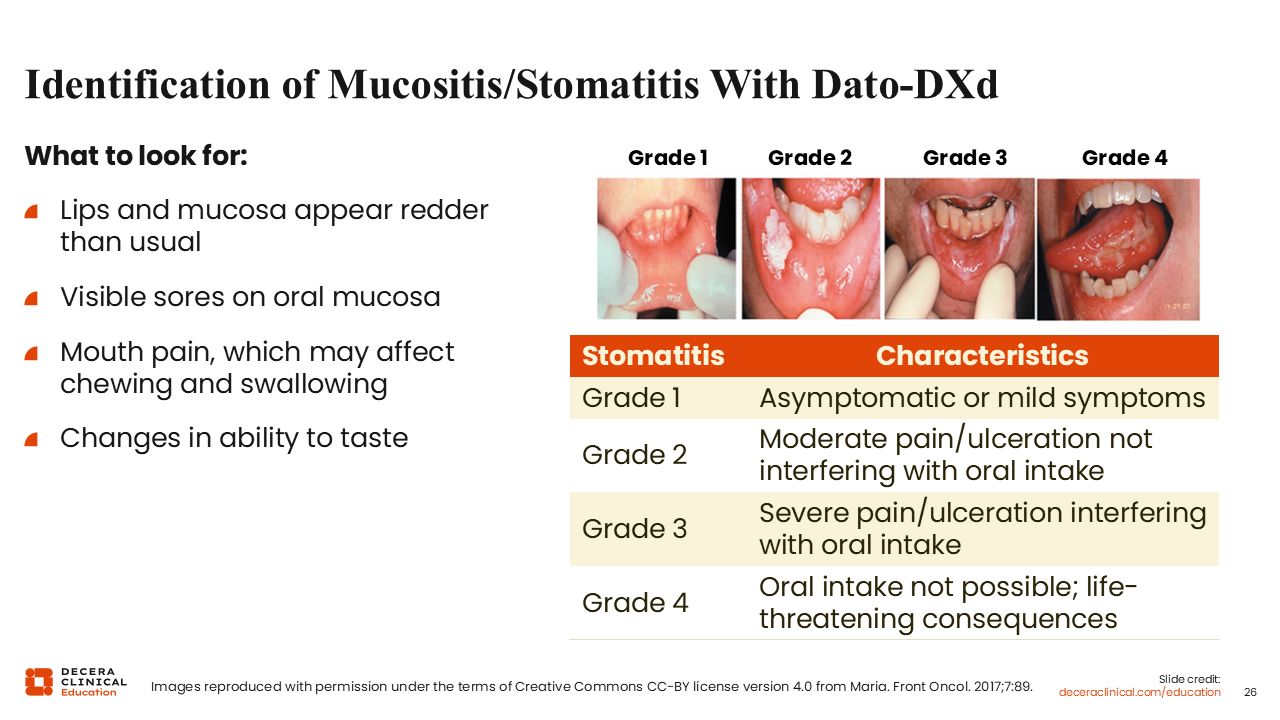
Identification of Mucositis/Stomatitis With Dato-DXd
Stomatitis and oral mucositis can affect oral intake, hydration, QoL, and treatment continuity. Early signs can include redness of the lips or oral mucosa, visible sores, mouth pain, changes in chewing or swallowing, and altered taste.46 Healthcare professionals should ask patients specifically about oral discomfort, food avoidance, swallowing difficulty, and hydration because patients may not always describe these symptoms as mucositis or stomatitis.
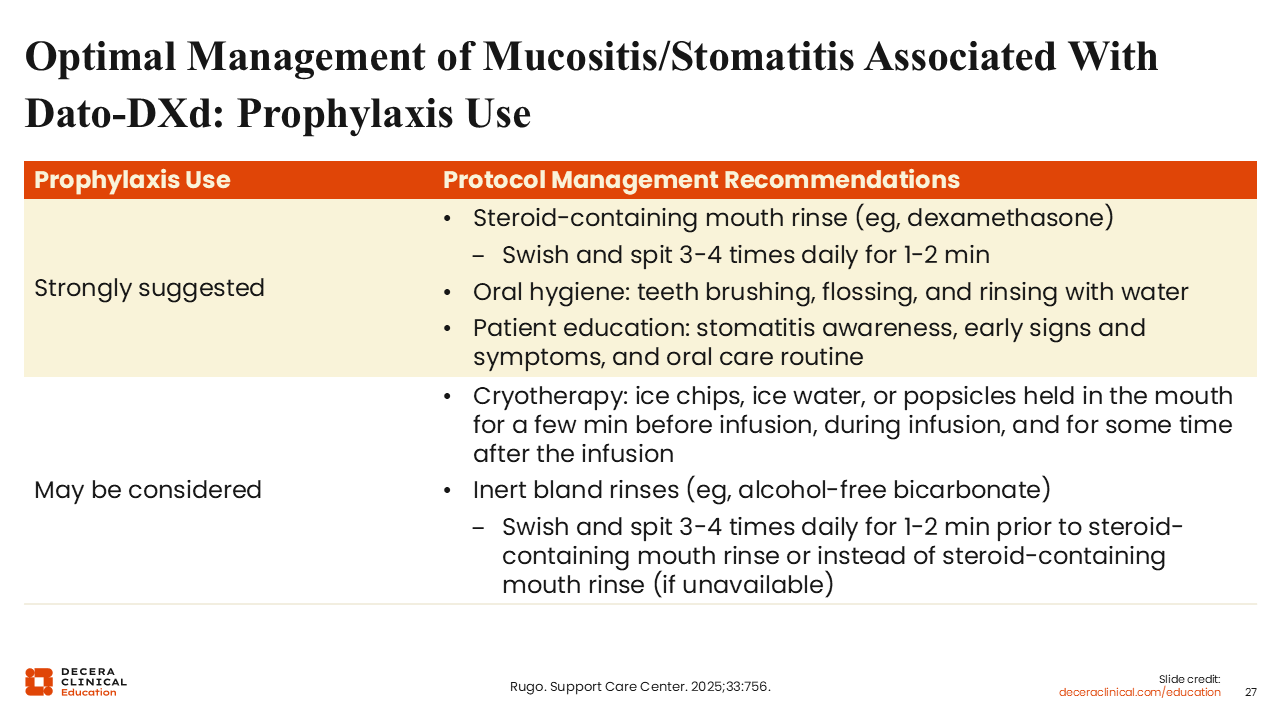
Optimal Management of Mucositis/Stomatitis Associated With Dato-DXd: Prophylaxis Use
Preventive oral care is central to reducing the burden of Dato-DXd–associated stomatitis and mucositis. A steroid-containing mouth rinse, such as dexamethasone, is strongly suggested during treatment. Patients should swish and spit 3-4 times daily for 1-2 minutes and should be counseled to follow the prescribed oral care routine consistently. Cryotherapy with ice chips, ice water, or popsicles held in the mouth before, during, and after infusion may also be considered. Bland rinses, including alcohol-free bicarbonate rinses, may be used before steroid-containing mouth rinse or in place of it, if steroid rinse is unavailable.46
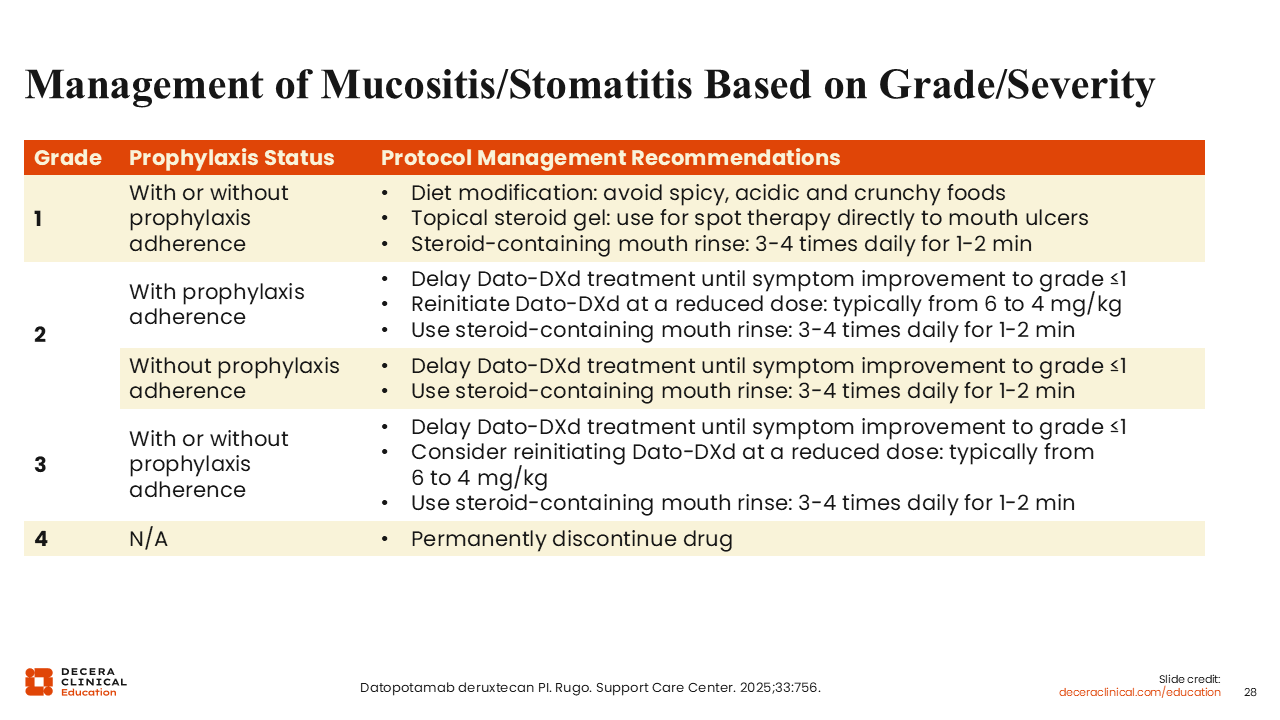
Management of Mucositis/Stomatitis Based on Grade/Severity
Severity is generally graded by symptoms and effect on oral intake. Grade 1 stomatitis is asymptomatic or associated with mild symptoms. Grade 2 involves moderate pain or ulceration that does not interfere with oral intake. Grade 3 involves severe pain or ulceration that interferes with oral intake. Grade 4 indicates that oral intake is not possible and may be associated with life-threatening consequences.38,46
Management depends on severity and whether prophylactic oral care has been used. For grade 1 symptoms, dietary modification, topical steroid gel applied directly to mouth ulcers, and steroid-containing mouth rinse 3-4 times daily for 1-2 minutes may be used.38,46 Patients should avoid spicy, acidic, or crunchy foods that may worsen oral discomfort.
For grade 2 symptoms, Dato-DXd should generally be delayed until symptoms improve to grade ≤1. If symptoms occur despite prophylaxis, treatment is typically reinitiated at a reduced dose, often from 6 mg/kg to 4 mg/kg, with continued steroid-containing mouth rinse.
For grade 3 symptoms, treatment should be delayed until improvement to grade ≤1, and reinitiation at a reduced dose may be considered.
Grade 4 stomatitis requires permanent discontinuation of Dato-DXd.
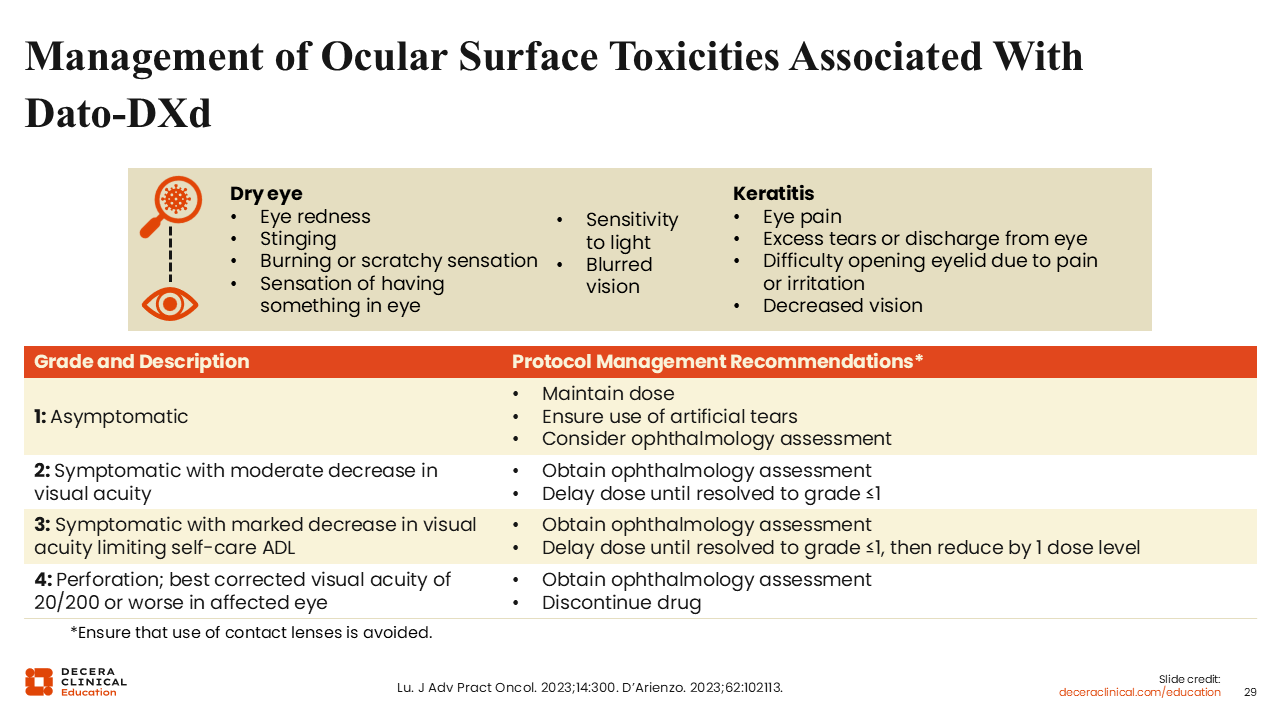
Management of Ocular Surface Toxicities Associated With Dato-DXd
Ocular AEs may include dry eye, keratitis, blurred vision, corneal ulceration, and other ocular surface symptoms. Dry eye may present with redness, stinging, burning, scratchy sensation, a foreign-body sensation, sensitivity to light, or blurred vision. Keratitis may present with eye pain, excessive tearing or discharge, difficulty opening the eyelid because of pain or irritation, or decreased vision.38,47
Patients should be counseled to report ocular symptoms promptly and to avoid contact lenses unless directed otherwise by an eye care professional. Preservative-free lubricating eye drops should be used to reduce ocular surface dryness.38,47
Ocular AE management depends on severity. Asymptomatic grade 1 ocular toxicity may allow continued dosing with artificial tears and consideration of ophthalmology assessment.
Grade 2 symptoms with moderate decrease in visual acuity should prompt ophthalmology assessment and dose delay until improvement to grade ≤1.
Grade 3 symptoms with marked decrease in visual acuity, limiting self-care activities of daily living, should prompt ophthalmology assessment, dose delay until improvement to grade ≤1, and dose reduction when treatment is resumed.
Grade 4 toxicity, including corneal perforation or severely impaired visual acuity, requires discontinuation.
Interstitial Lung Disease Associated With Dato-DXd
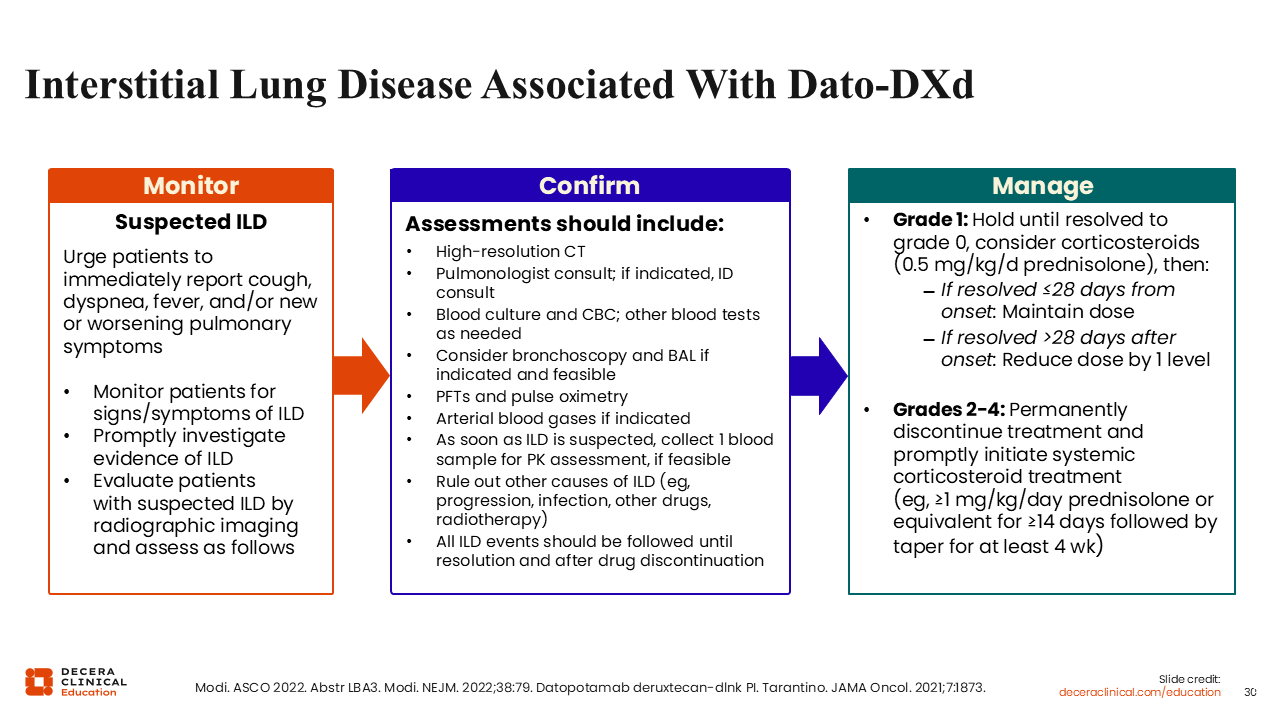
ILD and pneumonitis are uncommon but potentially serious AEs associated with several ADCs, including Dato-DXd.38,48 Patients should be counseled to report new or worsening cough, dyspnea, fever, or other pulmonary symptoms immediately. Routine symptom monitoring is important because early recognition may reduce the risk of severe or irreversible toxicity.
If ILD is suspected, Dato-DXd should be withheld and the patient should undergo prompt evaluation. Workup may include high-resolution CT, pulmonology consultation, infectious disease consultation when indicated, blood cultures and complete blood count, pulse oximetry, pulmonary function testing, arterial blood gases when indicated, bronchoscopy and bronchoalveolar lavage when feasible, and assessment for alternative causes such as disease progression, infection, other medications, or prior radiotherapy.38,48
For grade 1 ILD or pneumonitis, treatment should be held until resolution to baseline, and corticosteroids may be considered. If symptoms resolve within 28 days of onset, treatment may be resumed at the same dose. If resolution takes longer than 28 days, treatment should be resumed at a reduced dose.38
For grade 2-4 ILD or pneumonitis, Dato-DXd should be permanently discontinued, and systemic corticosteroids should be initiated promptly, such as prednisolone or equivalent at 1 mg/kg/day or higher for ≥14 days, followed by a taper for ≥4 weeks.38
Pulmonary symptoms require urgent attention. Patients should be instructed not to wait for scheduled visits if they develop new cough, shortness of breath, fever, or worsening respiratory symptoms. Early evaluation and treatment interruption are central to safe management.