CE / CME
Evolving Treatment Landscape for Early-Stage TNBC With and Without gBRCAm
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 26, 2026
Expiration: December 25, 2026

Activity
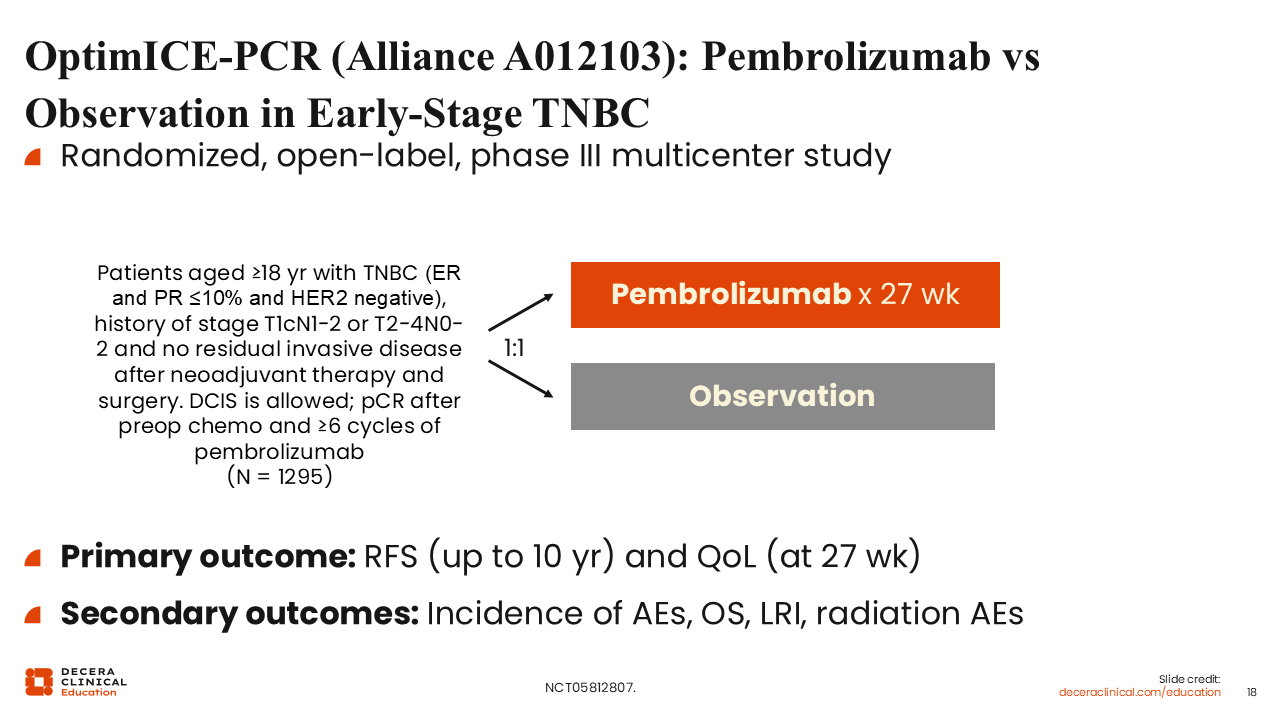
OptimICE-PCR (Alliance A012103): Pembrolizumab vs Observation in Early-Stage TNBC
OptimICE-PCR is an ongoing randomized, open-label phase III study evaluating whether adjuvant pembrolizumab can be omitted in selected patients with early-stage TNBC who achieve pCR after neoadjuvant chemoimmunotherapy (NCT05812807). Eligible patients include adults with TNBC, defined as ER and PgR ≤10% and HER2 negative, with a history of stage T1cN1-2 or T2-4N0-2 disease and no residual invasive disease after neoadjuvant therapy. Patients must have achieved pCR after preoperative chemotherapy and received ≥6 cycles of pembrolizumab. Patients are randomized 1:1 to receive pembrolizumab for 27 weeks or observation. The primary outcomes are recurrence-free survival up to 10 years and quality of life (QoL) at 27 weeks. Secondary outcomes include incidence of AEs, OS, locoregional recurrence interval, and radiation-associated AEs. Because OptimICE-PCR is ongoing, no efficacy conclusions can yet be drawn. Its clinical importance lies in the de-escalation question that it is designed to answer: whether selected patients with pCR can safely avoid additional treatment exposure, visit burden, cost, and potential immune-related toxicity.
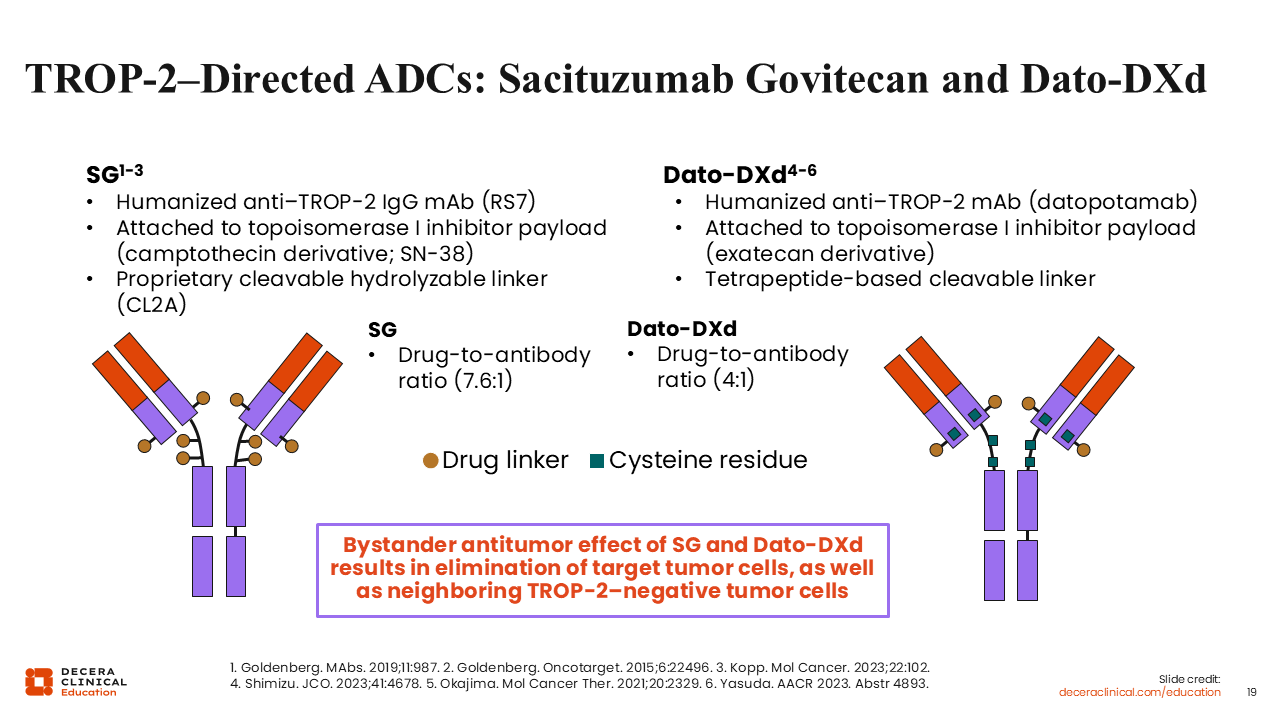
TROP-2–Directed ADCs: Sacituzumab Govitecan and Dato-DXd
TROP-2–directed ADCs are being evaluated in TNBC because TROP-2 is commonly expressed in epithelial tumors, including breast cancer. ADCs are designed to deliver cytotoxic payloads to tumor cells while also producing a bystander antitumor effect in nearby tumor cells.33,34
Sacituzumab govitecan and Dato-DXd both target TROP-2, but they should not be viewed as interchangeable agents. Sacituzumab govitecan is a humanized anti–TROP-2 IgG monoclonal antibody linked to SN-38, a topoisomerase I inhibitor payload, through a cleavable hydrolyzable linker. Its reported drug-to-antibody ratio is approximately 7.6:1.33,34 Dato-DXd is a humanized anti–TROP-2 monoclonal antibody linked to an exatecan-derivative topoisomerase I inhibitor payload through a tetrapeptide-based cleavable linker, with a reported drug-to-antibody ratio of approximately 4:1.35,36
These structural differences are clinically meaningful because the AE profiles and monitoring needs differ by agent. For sacituzumab govitecan, neutropenia, diarrhea, nausea and vomiting, and hypersensitivity reactions are key management considerations. For Dato-DXd, stomatitis or oral mucositis, ocular surface toxicity, and interstitial lung disease (ILD)/pneumonitis require particular attention.37,38
ADC selection and counseling should be agent specific. Patients need clear expectations about the AEs most likely to affect daily functioning, when to contact the care team, and how early supportive care or dose modification may help prevent manageable AEs from becoming treatment limiting.
Phase III ASCENT-05/OptimICE-RD: Sacituzumab Govitecan + Pembrolizumab in TNBC With no pCR After Surgery + Neoadj Tx
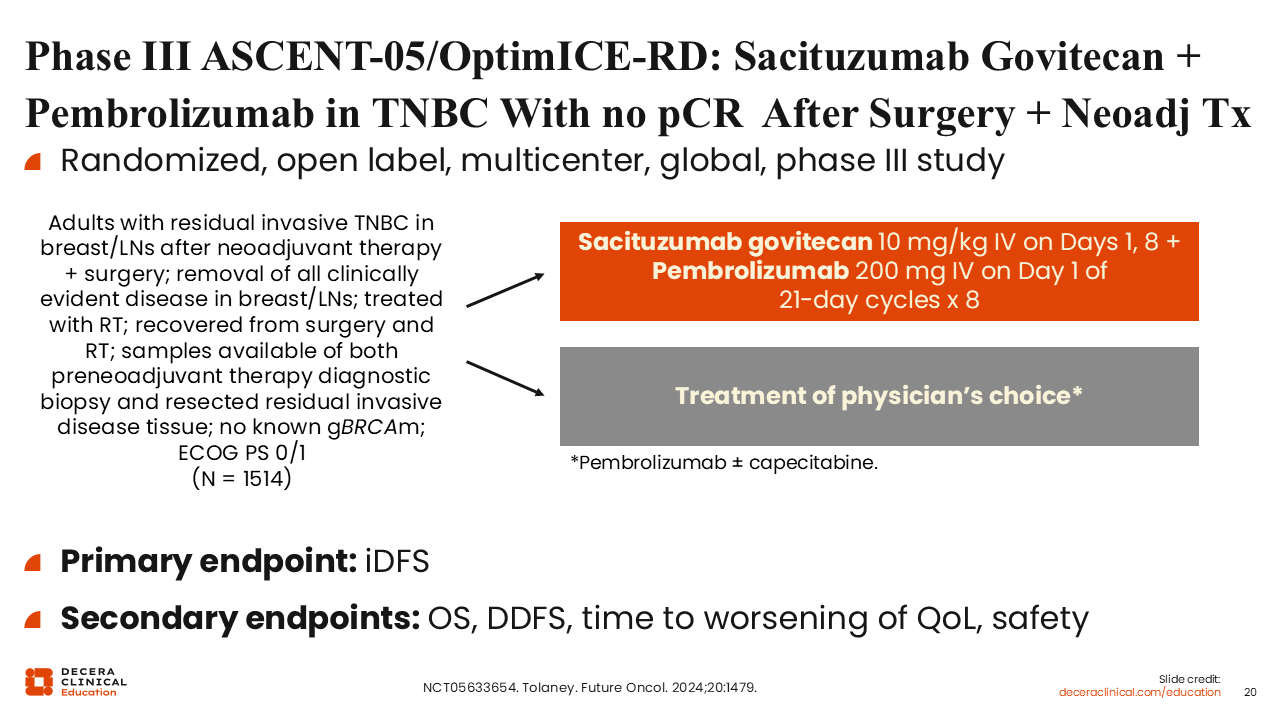
ASCENT-05/OptimICE-RD is an ongoing randomized, open-label phase III trial evaluating whether adjuvant sacituzumab govitecan plus pembrolizumab can improve outcomes compared with treatment of physician choice in patients with residual TNBC after neoadjuvant therapy and surgery (NCT05633654).39 Eligible patients include adults with residual invasive TNBC in the breast and/or lymph nodes after neoadjuvant therapy and surgery, no known germline BRCA mutation, ECOG PS 0/1, and recovery from surgery and radiotherapy. Tissue must be available from both the pretreatment diagnostic biopsy and the resected residual invasive disease.
Patients are randomized to receive sacituzumab govitecan 10 mg/kg intravenously on Days 1 and 8 plus pembrolizumab 200 mg intravenously on Day 1 of each 21-day cycle for 8 cycles, or treatment of physician choice. Treatment of physician choice consists of pembrolizumab with or without capecitabine. The primary endpoint is iDFS, and secondary endpoints include OS, DDFS, time to worsening of QoL, and safety.40
Phase III TROPION-Breast03: Postneoadjuvant Dato-DXd ± Durva vs Investigator’s Choice for STAGE I-III TNBC
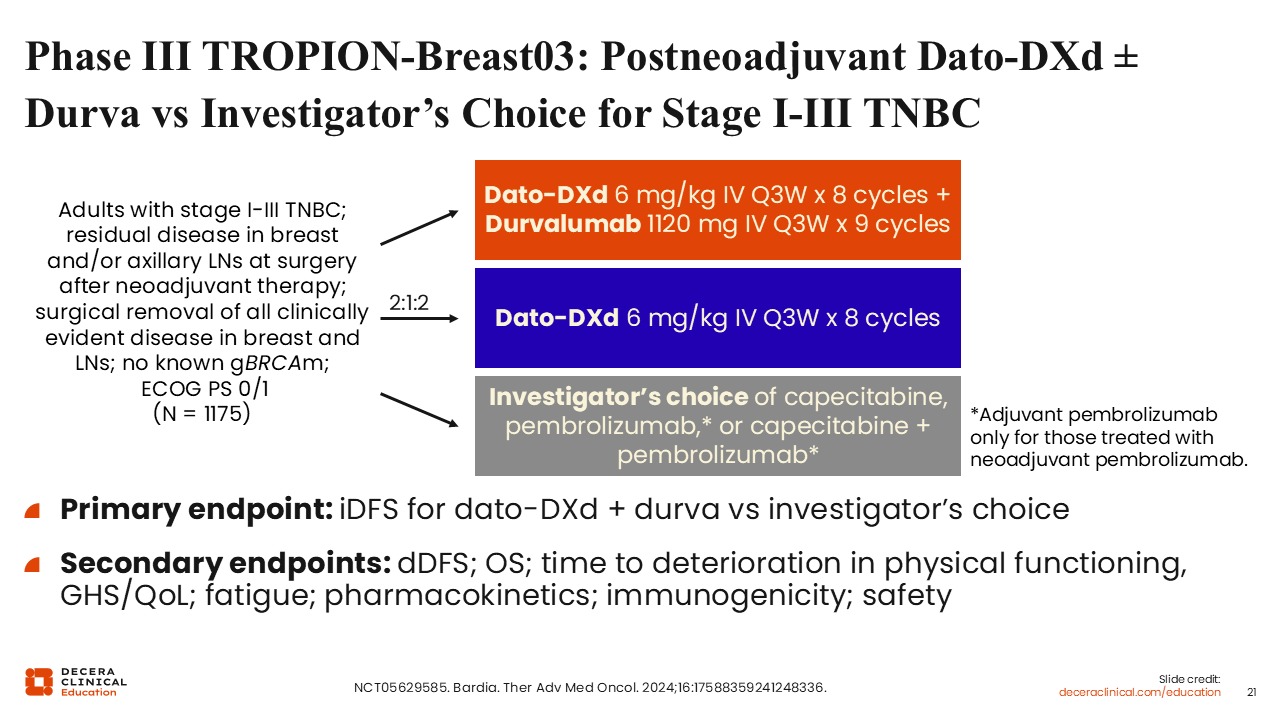
TROPION-Breast03 is an ongoing randomized, open-label, international phase III trial evaluating Dato-DXd, with or without durvalumab, compared with investigator's choice therapy in patients with stage I-III TNBC and residual invasive disease after neoadjuvant therapy and surgery (NCT05629585). Eligible patients have residual invasive disease in the breast and/or axillary lymph nodes at surgery after neoadjuvant systemic therapy, no known germline BRCA mutation, and ECOG PS 0/1. Patients are randomized in a 2:1:2 ratio to receive Dato-DXd plus durvalumab, Dato-DXd alone, or investigator's choice therapy.41
Investigator’s choice may include capecitabine, pembrolizumab, or capecitabine plus pembrolizumab. Adjuvant pembrolizumab is included only for patients previously treated with neoadjuvant pembrolizumab. The primary endpoint is iDFS for Dato-DXd plus durvalumab compared with investigator’s choice. Secondary endpoints include DDFS, OS, time to deterioration in physical functioning and global health status/QoL, fatigue, pharmacokinetics, immunogenicity, and safety.
Phase III TROPION-Breast04: Dato-DXd ± Durva vs SoC for Early-Stage TNBC
Unlike the postneoadjuvant escalation trials focused on residual disease after surgery, TROPION-Breast04 evaluates whether an ADC plus immunotherapy approach can be incorporated earlier in the treatment pathway (NCT06112379). Although Dato-DXd now has a US indication for unresectable or metastatic TNBC in patients who are not candidates for PD-1/PD-L1 inhibitor therapy, its use in early-stage TNBC remains investigational.38
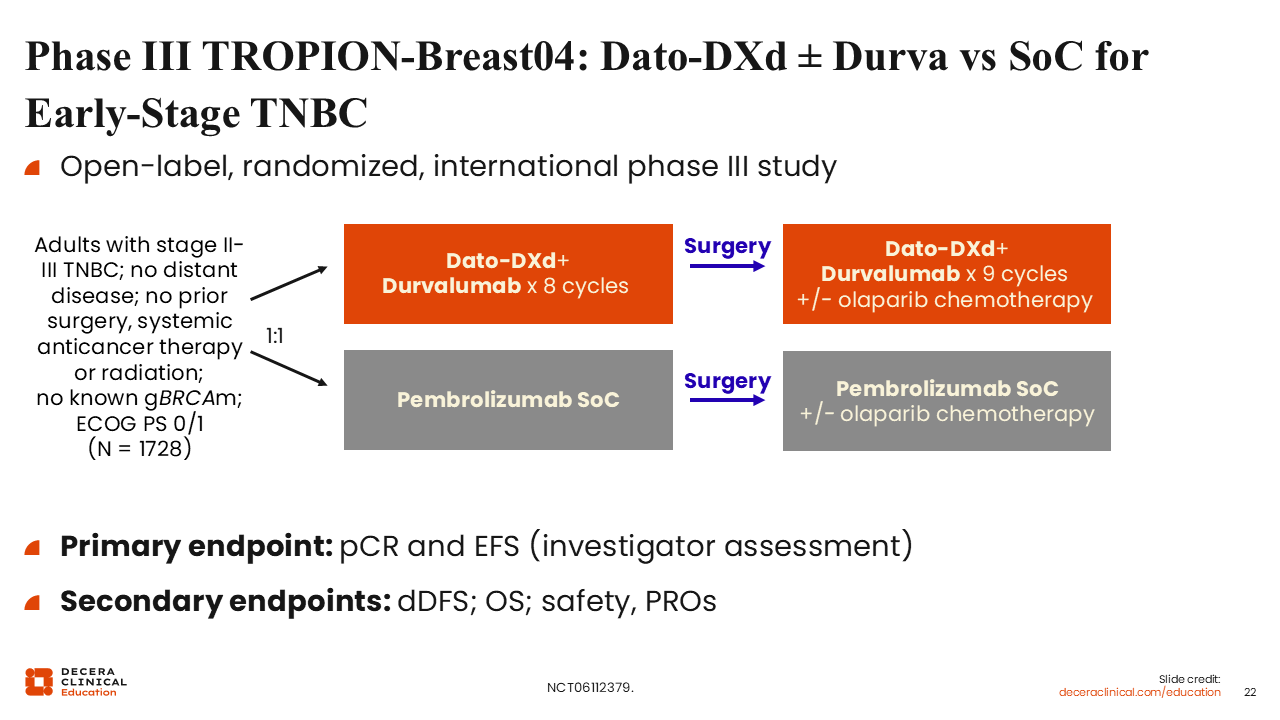
TROPION-Breast04 is an ongoing randomized, open-label, international phase III study evaluating Dato-DXd plus durvalumab as part of a perioperative strategy for treatment-naive early-stage TNBC or HR-low/HER2-negative breast cancer.42 Eligible patients include adults with previously untreated stage II/III TNBC or HR-low/HER2-negative breast cancer, no distant disease, no prior surgery, systemic anticancer therapy, or radiation for the current breast cancer, no known germline BRCA mutation, and ECOG PS 0/1.42
Patients are randomized to neoadjuvant Dato-DXd plus durvalumab followed by surgery and adjuvant durvalumab-based therapy, or to standard-of-care neoadjuvant pembrolizumab plus chemotherapy followed by surgery and adjuvant pembrolizumab-based therapy. In the adjuvant phase, protocol-permitted therapy may also include olaparib when appropriate. The primary endpoints are pCR and investigator-assessed EFS. Secondary endpoints include DDFS, OS, safety, and patient-reported outcomes.
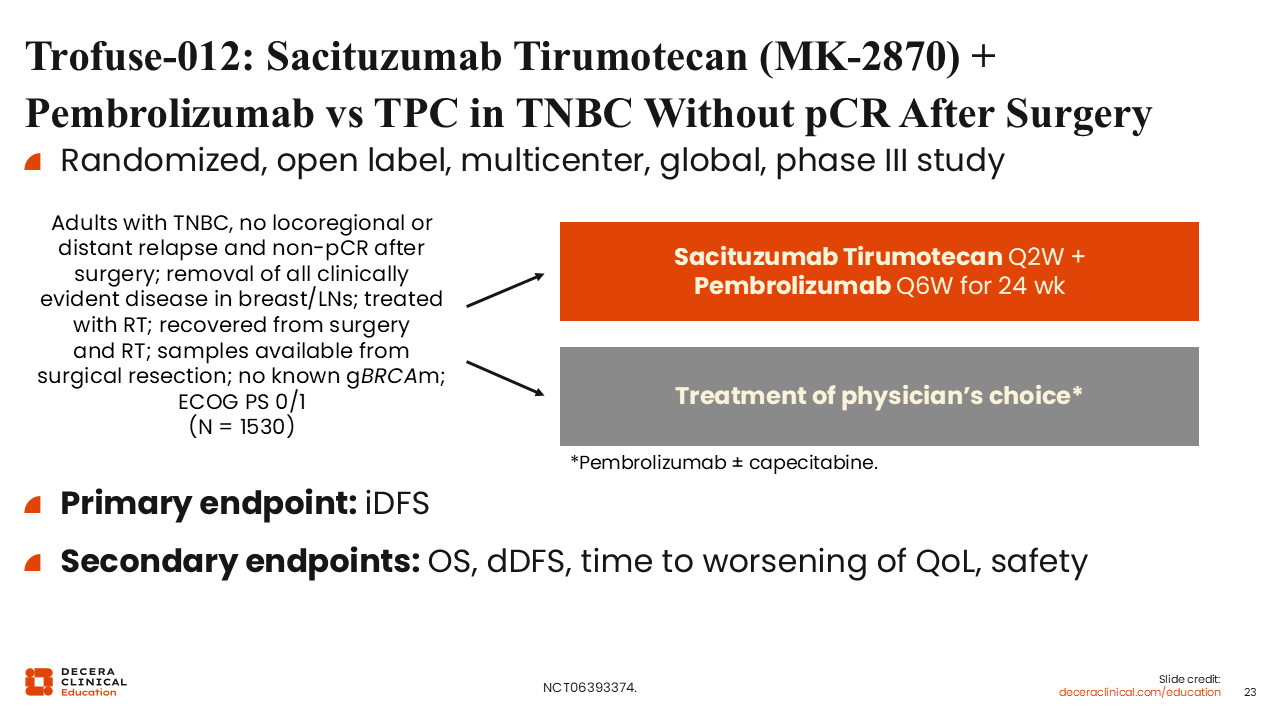
Trofuse-012: Sacituzumab Tirumotecan (MK-2870) + Pembrolizumab vs TPC in TNBC Without pCR After Surgery
MK-2870-12 is an ongoing randomized, open-label phase III trial evaluating adjuvant sacituzumab tirumotecan, also known as MK-2870, plus pembrolizumab compared with treatment of physician choice in patients with TNBC who received neoadjuvant therapy and did not achieve pCR at surgery (NCT06393374). Eligible patients include adults with TNBC who have no locoregional or distant relapse and have residual disease after surgery following neoadjuvant therapy. Patients must have had surgical removal of all clinically evident disease in the breast and lymph nodes, received radiotherapy, recovered from surgery and radiotherapy, and have available tissue from surgical resection, no known germline BRCA mutation, and ECOG PS 0/1.
Patients are randomized to receive sacituzumab tirumotecan plus pembrolizumab or treatment of physician choice, which may include pembrolizumab with or without capecitabine. The primary endpoint is iDFS, and secondary endpoints include OS, DDFS, time to worsening of QoL, and safety (NCT06393374).
Together, these studies reflect 2 major directions in early-stage TNBC research. OptimICE-PCR addresses de-escalation for patients with excellent response to neoadjuvant therapy. ASCENT-05/OptimICE-RD, Trofuse-012, and TROPION-Breast03 are evaluating ADC-based approaches in the postneoadjuvant setting, and TROPION-Breast04 is testing whether this strategy can be moved earlier into neoadjuvant/perioperative treatment. Until mature data are available, ADC-based approaches should be discussed as investigational in early-stage TNBC.