CE / CME
Evolving Treatment Landscape for Early-Stage TNBC With and Without gBRCAm
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 26, 2026
Expiration: December 25, 2026

Activity
Landscape of TNBC
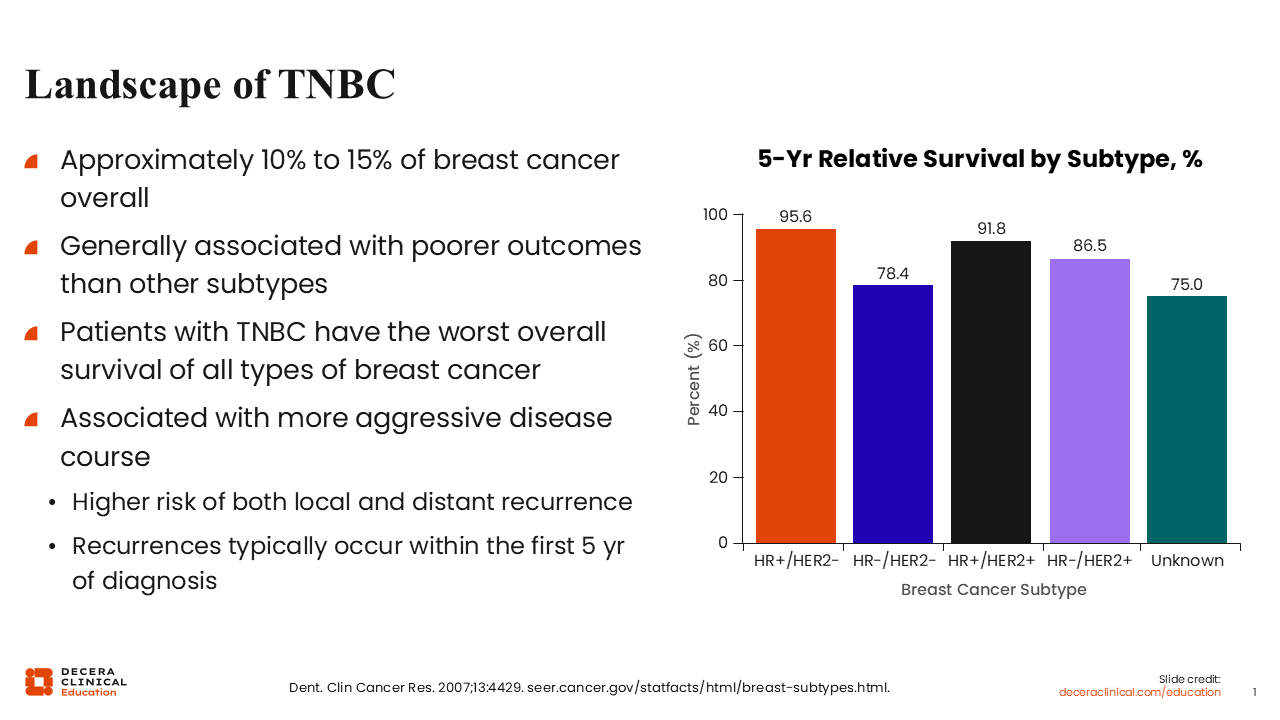
TNBC accounts for approximately 10% to 15% of breast cancers overall, but its clinical impact is disproportionate to its prevalence. Compared with other breast cancer subtypes, TNBC is generally associated with a more aggressive disease course, a higher likelihood of local and distant recurrence, and poorer overall outcomes.1
The timing of disease recurrence is also clinically important for TNBC. TNBC recurrences tend to occur earlier than those seen with some other breast cancer subtypes, most often within the first 5 years after diagnosis and commonly within the first 2-3 years. In a SEER-based survival data analysis, the 5-year relative survival for patients with hormone receptor (HR)–negative/HER2-negative breast cancer was 78.4% compared with 95.6% for HR-positive/HER2-negative breast cancer, 91.8% for HR-positive/HER2-positive breast cancer, and 86.5% for HR-negative/HER2-positive breast cancer.2
These might support why accurate diagnosis, timely treatment planning, and early identification of actionable biomarkers are central to TNBC management. In addition, because disease recurrence risk is concentrated early in the disease course, initial treatment decisions often need to account for systemic therapy, treatment sequencing, and clinical trial eligibility all within a short time frame for patients with TNBC. Moreover, because of the more aggressive biology of TNBC, treatment decisions often need to be made quickly in these patients.
This module focuses on 3 practical priorities: identifying patients at increased risk, completing biomarker and germline testing early, and using treatment response to guide escalation or de-escalation of therapy based on the latest clinical evidence and clinical guidelines.
Epidemiology of TNBC
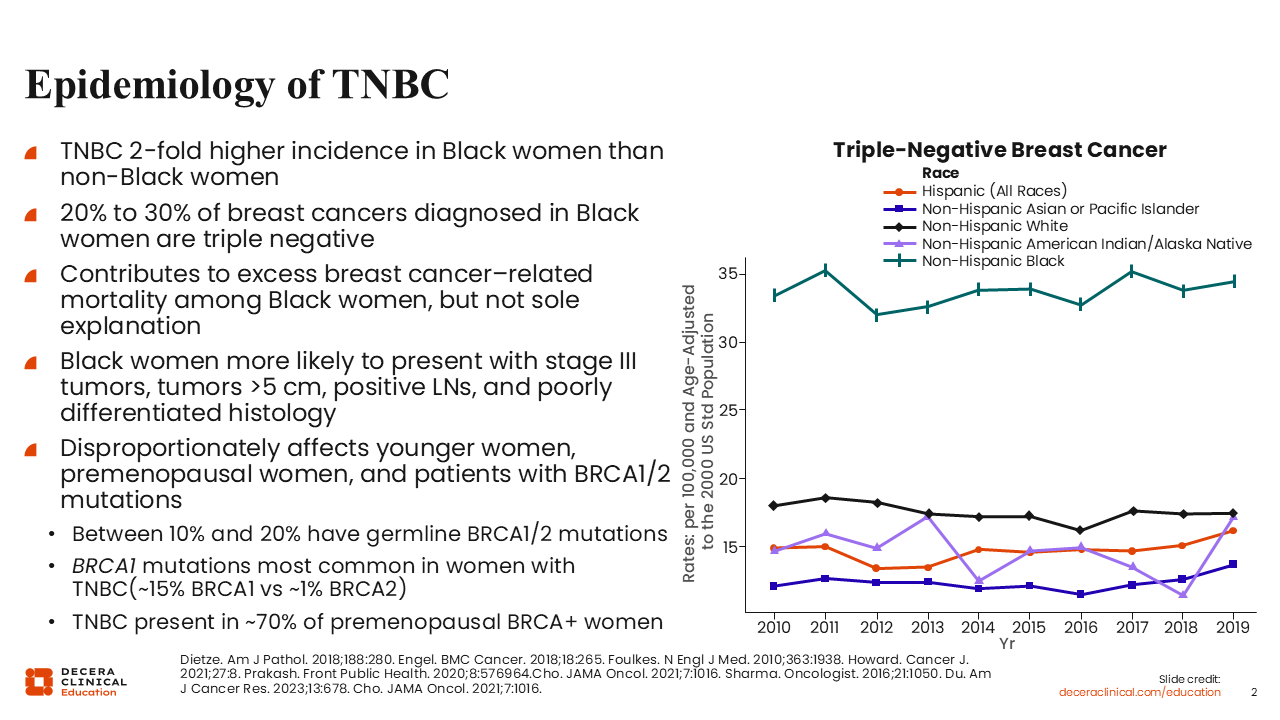
TNBC disproportionately affects Black women, younger women, premenopausal women, and patients with germline BRCA1 or BRCA2 pathogenic variants.3,4 It is approximately 2-fold more common in Black women than in non-Black women, and approximately 20% to 30% of breast cancers diagnosed in Black women are triple negative.3
The higher prevalence of TNBC contributes to excess breast cancer–related mortality among Black women, but tumor biology alone does not fully explain these disparities. Black women with TNBC are also more likely to present with more aggressive disease features, including stage III tumors, tumors >5 cm, positive lymph nodes, and poorly differentiated histology.3,5 Timely diagnostic evaluation, guideline-concordant treatment, and early identification of barriers to care are paramount and central to reducing disparities in TNBC outcomes.
Risk Factors for TNBC
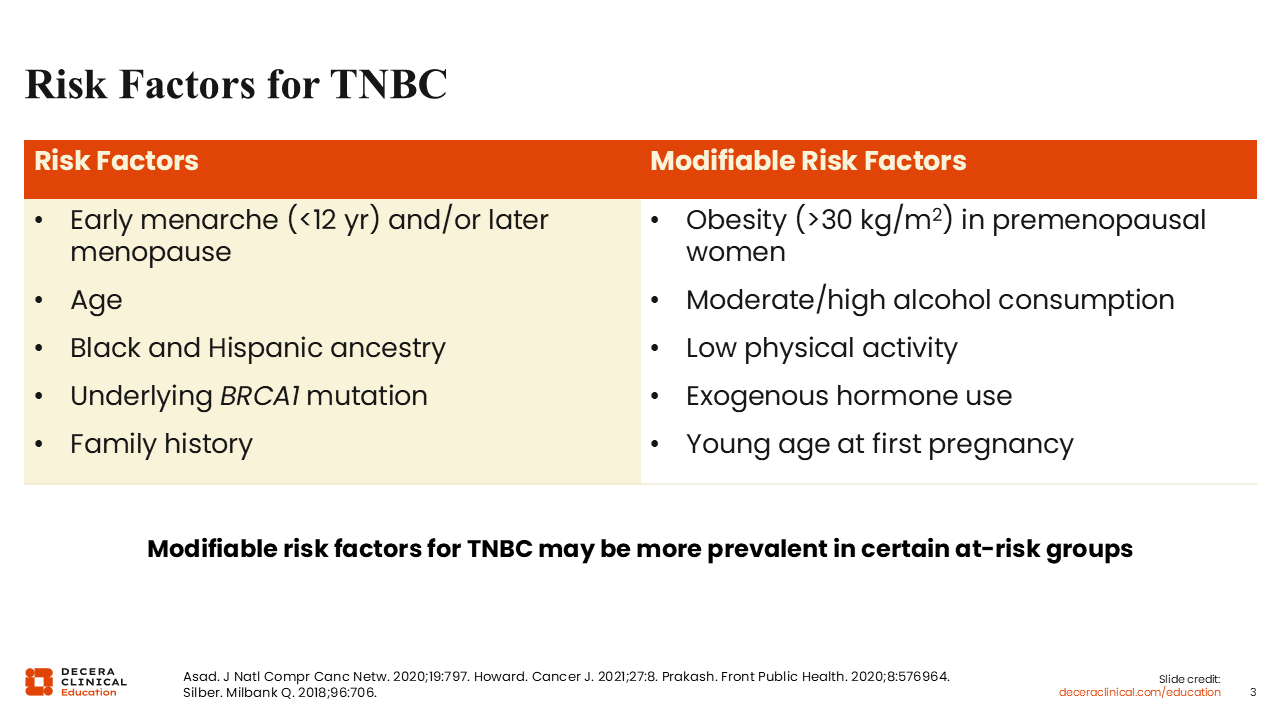
TNBC risk is multifactorial. Nonmodifiable risk factors include early menarche (onset of a girl’s first menstrual period: before 12 years of age) and/or later menopause onset, younger age, Black and Hispanic ancestry, underlying BRCA1 mutation, and family history.5-7 Modifiable factors associated with TNBC risk include obesity, particularly in premenopausal women; moderate or high alcohol consumption; low physical activity; exogenous hormone use; and younger age at first pregnancy.6,7 These factors should be discussed carefully and in context with each individual patient.
The aforementioned factors support risk-reduction counseling and patient education, but they do not fully explain TNBC risk or the disparities observed across patient populations. Lifestyle counseling is best framed as one component of comprehensive breast cancer risk education rather than as a substitute for screening, timely evaluation, or equitable access to care.8
The clinical implications of TNBC extend beyond prevalence. Earlier recurrence, visceral metastatic patterns, and disparities in diagnosis and treatment access make timely testing, treatment planning, and care coordination especially important.1,3,5
Recommended Biomarker and Molecular Testing
For any patient with a new diagnosis of breast cancer, accurate biomarker testing is foundational to informing treatment planning. Estrogen receptor (ER), progesterone receptor (PgR), and HER2 status should be assessed in all patients with breast cancer because these results determine whether endocrine therapy, HER2-directed therapy, or a TNBC treatment pathway is appropriate.9
ER, PgR, and HER2 status should be assessed at diagnosis. ER and PgR are evaluated by immunohistochemistry (IHC), and HER2 is assessed using a validated IHC assay, with reflex or concurrent dual-probe in situ hybridization when HER2 IHC test result is equivocal.9 Patients should not be classified as having TNBC unless ER, PgR, and HER2 negativity status have been accurately confirmed. Misclassification may lead to missed opportunities for endocrine therapy or HER2-directed therapy, both of which can substantially inform treatment selection and outcomes.9
Additional testing becomes important as the clinical scenario evolves. In locally recurrent unresectable or metastatic TNBC, PD-L1 testing can help determine eligibility for immune checkpoint inhibitor–based therapy, depending on the regimen and current guidance.9 Germline BRCA1/2 testing should also be performed if it has not already been completed because mutation status may inform eligibility for adjuvant olaparib in patients with germline BRCA1/2-mutated, HER2-negative, high-risk early-stage breast cancer (EBC) after neoadjuvant or adjuvant chemotherapy.10
The broader clinical goal is to avoid missed treatment opportunities. Biomarker and molecular assessment should be revisited at recurrence or metastasis when additional therapeutic options may become relevant. Although we attempt to follow best practice and guidelines regarding testing, the reality is that some of our patients slip through the cracks because of socioeconomic factors.
Incidence of BRCA Mutations
Germline BRCA1/2 pathogenic variants are more common in TNBC than in non-TNBC breast cancer. Approximately 10% to 20% of patients with TNBC have germline BRCA1/2 mutations, with BRCA1 mutations occurring more frequently than BRCA2 mutations in this population.4,11 TNBC has also been reported in approximately 70% of premenopausal women with germline BRCA1/2 mutations, although estimates vary by population and mutation type.12
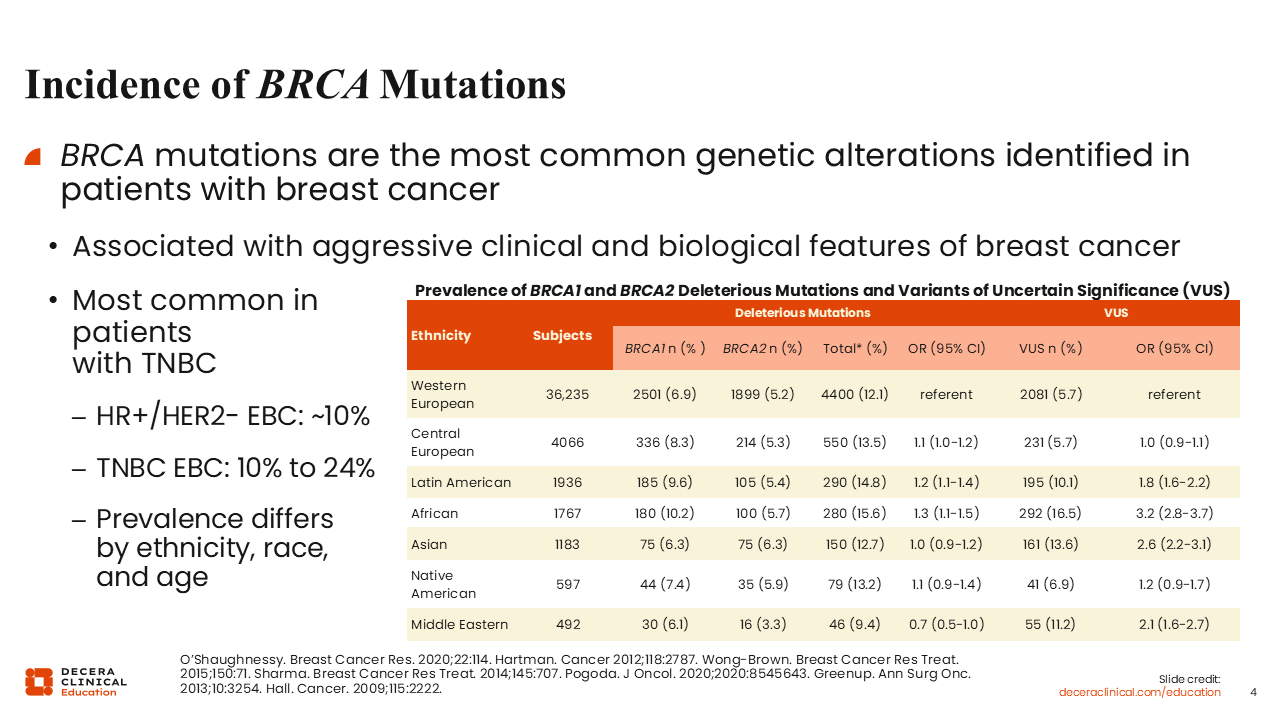
BRCA mutations are among the most clinically relevant inherited alterations identified in breast cancer and are associated with more aggressive clinical and biologic features.13 In EBC, BRCA mutations are reported in approximately 10% to 24% of patients with TNBC compared with approximately 10% of patients with HR-positive/HER2-negative disease.14,15
The prevalence of deleterious BRCA1/2 mutations varies by ethnicity, race, and age. Reported rates include 12.1% among individuals with Western European ethnicity, 14.8% with Latin American ethnicity, 15.6% with African ethnicity, 12.7% with Asian ethnicity, and 13.2% with Native American ethnicity.16 These data help counter the misconception that BRCA mutations are primarily relevant only for patients of European ancestry. In TNBC, germline testing should be approached broadly and equitably so that hereditary risk assessment, family counseling, and treatment implications are not missed.
An important limitation of germline testing is the identification of variants of uncertain significance (VUS). VUS were reported more frequently in several non-European populations, including 16.5% of individuals with African ethnicity, 13.6% with Asian ethnicity, 11.2% with Middle Eastern ethnicity, and 10.1% with Latin American ethnicity, compared with 5.7% of individuals with Western European ethnicity.16 These differences reinforce the need for equitable testing, genetics referral, and clear counseling about the distinction between pathogenic variants and VUS. VUS should not be treated as pathogenic alterations for treatment selection, but patients may need follow-up with genetics counseling professionals if reclassification occurs.
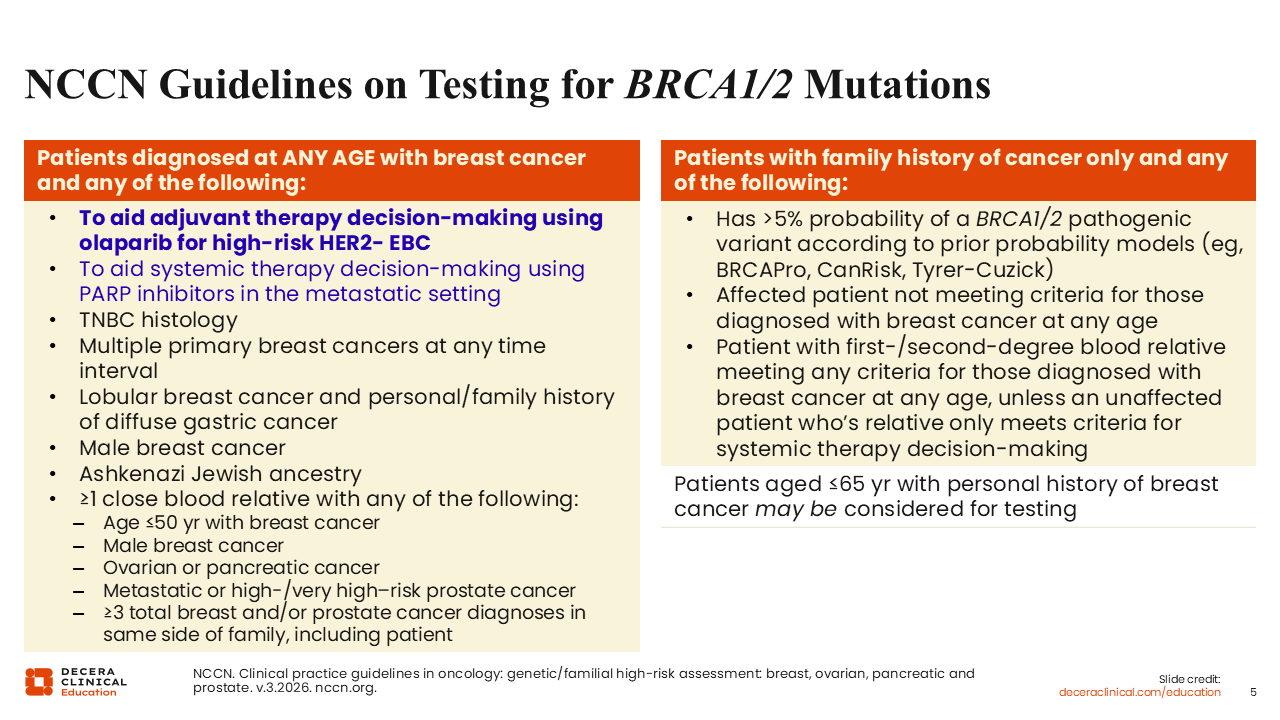
NCCN Guidelines on Testing for BRCA1/2 Mutations
National Comprehensive Cancer Network genetic/familial high-risk assessment guidance recommends BRCA1/2 testing for several groups of patients with breast cancer, including patients whose results may guide treatment selection.7 Genetic testing may inform adjuvant therapy decision-making with olaparib for high-risk HER2-negative EBC and systemic therapy decision-making with PARP inhibitors in the metastatic setting.17
For patients with breast cancer diagnosed at any age, testing is recommended for those with TNBC histology, multiple primary breast cancers, male breast cancer, Ashkenazi Jewish ancestry, or relevant personal or family history features.17
Relevant family history features include a close blood relative with breast cancer diagnosed at age 50 years or younger, male breast cancer, ovarian cancer, pancreatic cancer, metastatic or high-risk/very high–risk prostate cancer, or multiple breast and/or prostate cancer diagnoses on the same side of the family.17
Testing may also be appropriate based on family history alone, including when prior probability models estimate >5% probability of a BRCA1/2 pathogenic variant or when a first-degree or second-degree relative meets testing criteria. Patients aged 65 years or younger with a personal history of breast cancer may also be considered for testing.17
For patients with TNBC, the practical recommendations may be straightforward: Germline testing should occur early in the care pathway. Results may inform treatment planning, hereditary risk assessment, family counseling, and clinical trial considerations. Early testing also helps avoid delays later, particularly if adjuvant or metastatic targeted therapy options become relevant at a later time.