CE / CME
Evolving Treatment Landscape for Early-Stage TNBC With and Without gBRCAm
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 26, 2026
Expiration: December 25, 2026

Activity
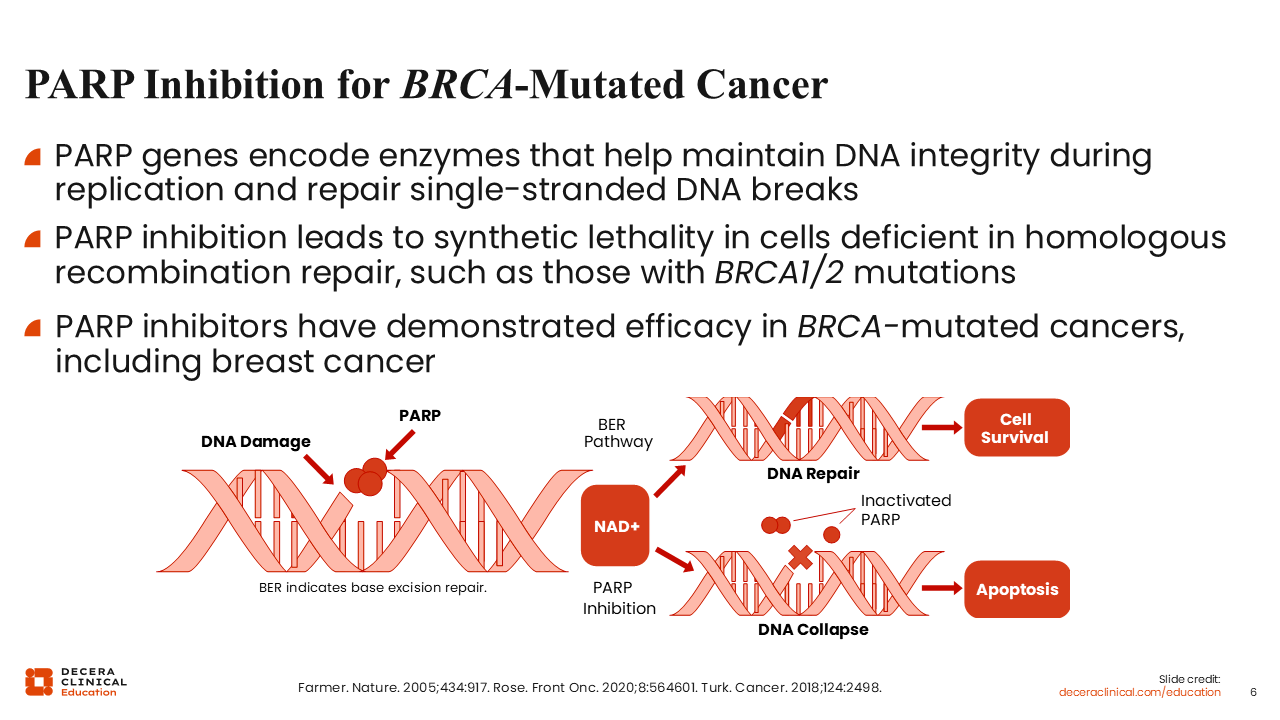
PARP Inhibition for BRCA-Mutated Cancer
PARP inhibitors exploit defective homologous recombination repair in tumors with germline BRCA1/2 mutations. By inhibiting repair of single-stranded DNA breaks, PARP inhibition increases DNA damage that BRCA-deficient cells are less able to repair, leading to synthetic lethality.21,22 This provides the biologic rationale for PARP inhibitor therapy in eligible patients with germline BRCA1/2-mutated, HER2-negative breast cancer.23
Identifying a germline BRCA1/2 pathogenic variant can inform hereditary risk counseling, family testing, and selection of systemic therapy in appropriate early-stage disease or metastatic settings. With biomarker and germline testing established, treatment selection then can be framed around disease stage, response to neoadjuvant therapy, germline BRCA1/2 status, and tolerance for therapy-related toxicity.
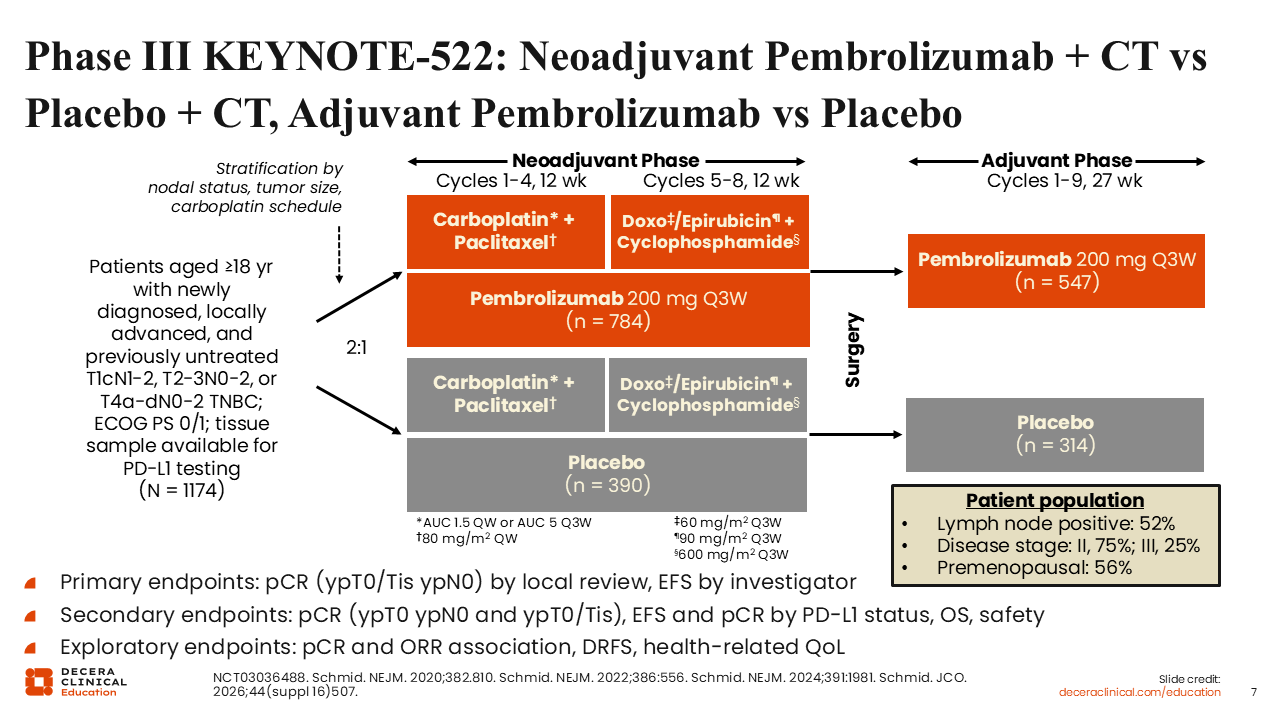
Phase III KEYNOTE-522: Neoadjuvant Pembrolizumab + CT vs Placebo + CT, Adjuvant Pembrolizumab vs Placebo
The international, randomized, double-blind phase III KEYNOTE-522 trial evaluated whether adding pembrolizumab to neoadjuvant chemotherapy, followed by adjuvant pembrolizumab after surgery, improved outcomes in patients with previously untreated stage II/III TNBC.24-26 Eligible patients were aged 18 years or older, had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0/1, and were enrolled regardless of PD-L1 expression status.
Patients were randomized 2:1 to receive pembrolizumab 200 mg or placebo every 3 weeks in combination with paclitaxel plus carboplatin for 4 cycles, followed by pembrolizumab or placebo with doxorubicin or epirubicin plus cyclophosphamide for 4 cycles. After surgery, patients continued adjuvant pembrolizumab or placebo every 3 weeks for up to 9 cycles.27
The dual primary endpoints were pCR and event-free survival (EFS). Key secondary endpoints included EFS and pCR by PD-L1 status, OS, and safety.25 The enrolled population included 1174 patients, with 784 assigned to the pembrolizumab-containing regimen and 390 assigned to placebo plus chemotherapy. Approximately 52% of patients had lymph node-positive disease, 75% had stage II disease, 25% had stage III disease, and 56% were premenopausal.25
KEYNOTE-522 was designed for patients with stage II/III TNBC, not for all patients with TNBC. This distinction matters when applying the data to lower-risk stage I disease, where the balance of expected benefit, treatment burden, and toxicity may differ.
In the initial analysis, the addition of pembrolizumab to neoadjuvant chemotherapy increased the pCR rate compared with chemotherapy alone (64.8% vs 51.2%).24,27
Treatment-related AEs of grade ≥3 were common in both treatment arms, occurring in 78.0% of patients in the pembrolizumab-chemotherapy arm and 73.0% in the placebo-chemotherapy arm.27 These safety findings reinforce the need to discuss treatment intensity, expected toxicities, and monitoring needs before therapy begins.
KEYNOTE-522: EFS at Interim Analysis 6
Longer follow-up confirmed that adding pembrolizumab to neoadjuvant chemotherapy and continuing pembrolizumab after surgery improved EFS compared with neoadjuvant chemotherapy followed by placebo.27 The estimated 36-month EFS rate was 84.5% with pembrolizumab plus chemotherapy followed by pembrolizumab compared with 76.8% with placebo plus chemotherapy followed by placebo. The hazard ratio for an event or death was 0.63 (95% CI: 0.48%-0.82%; P <.001).27
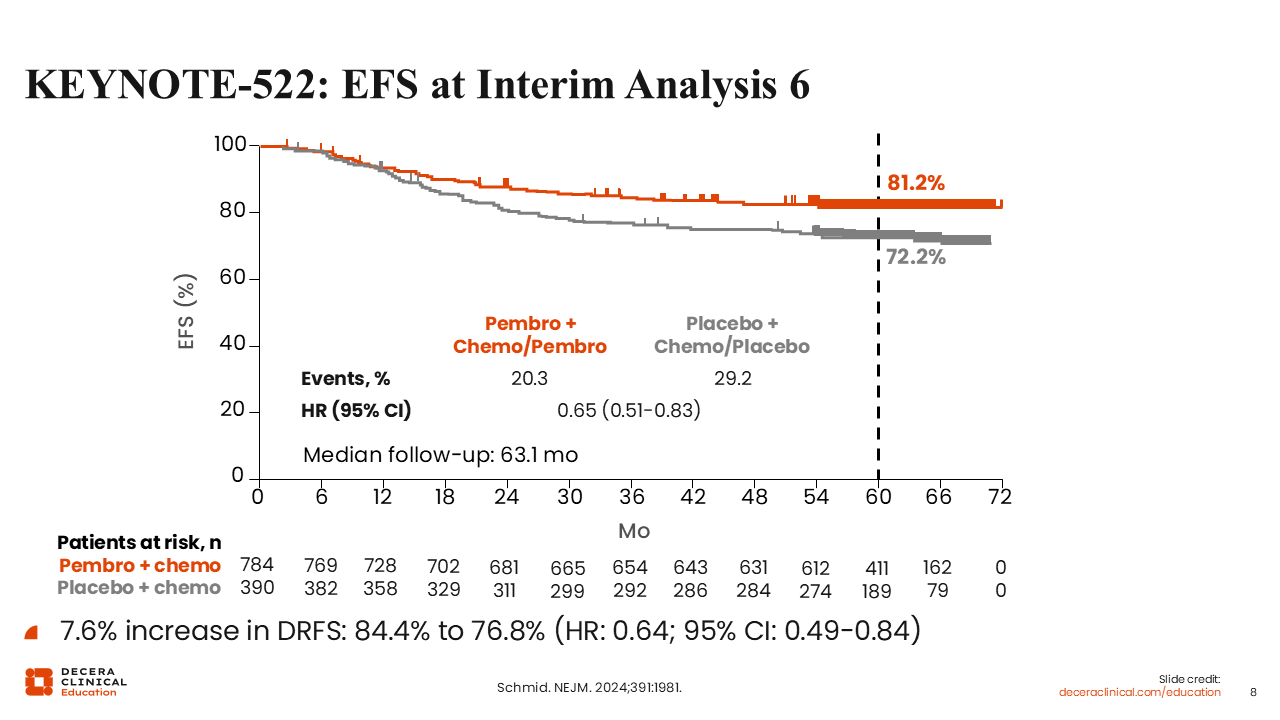
With additional follow-up, the EFS benefit remained consistent. At a later interim analysis, after a median follow-up of 63.1 months, EFS was 81.2% with pembrolizumab plus chemotherapy followed by pembrolizumab compared with 72.2% with placebo plus chemotherapy followed by placebo. Events occurred in 20.3% and 29.2% of patients, respectively (hazard ratio: 0.65; 95% CI: 0.51%-0.83%).25
Distant relapse-free survival also favored the pembrolizumab-containing regimen, with rates of 84.4% vs 76.8% (hazard ratio: 0.64; 95% CI: 0.49%-0.84%).25 Preventing distant relapse is a central goal of curative-intent therapy in early-stage TNBC.
Final OS results published in 2024 further supported the clinical relevance of the KEYNOTE-522 regimen. At a median follow-up of 75.1 months, the estimated OS at 60 months was 86.6% with pembrolizumab plus chemotherapy followed by pembrolizumab compared with 81.7% with placebo plus chemotherapy followed by placebo (P = .002).25 Subsequent final-analysis data presented at the 2026 American Society of Clinical Oncology annual meeting showed durable benefit at a median follow-up of 93.8 months, with estimated 7-year EFS of 78.3% vs 69.8% (hazard ratio: 0.68; 95% CI: 0.54%-0.86%) and estimated 7-year OS of 85.1% vs 77.2% (hazard ratio: 0.64; 95% CI: 0.49%-0.85%) for pembrolizumab vs placebo, respectively; no new safety signals were reported.26 Moreover, AEs in the final analysis were consistent with the established safety profiles of pembrolizumab and chemotherapy.
Overall, KEYNOTE-522 established a perioperative chemoimmunotherapy approach for appropriately selected patients with stage II/III TNBC. Pembrolizumab is initiated with neoadjuvant chemotherapy and then continued after surgery, regardless of whether pCR is achieved. This approach has shaped current treatment practice and has also prompted ongoing studies evaluating whether adjuvant therapy can be safely de-escalated in patients with excellent pathologic response. Treatment discussions should include the expected duration of perioperative therapy, the potential for immune-related AEs, the need for ongoing monitoring, and the importance of care coordination across all phases of therapy. Patients who are not eligible include those with stage I TNBC, metastatic disease, contraindications to pembrolizumab or the chemotherapy backbone, or active autoimmune disease or other conditions requiring systemic immunosuppression that would make immune checkpoint inhibition unsafe.
NeoPACT: Neoadjuvant Pembrolizumab + Carboplatin/Docetaxel
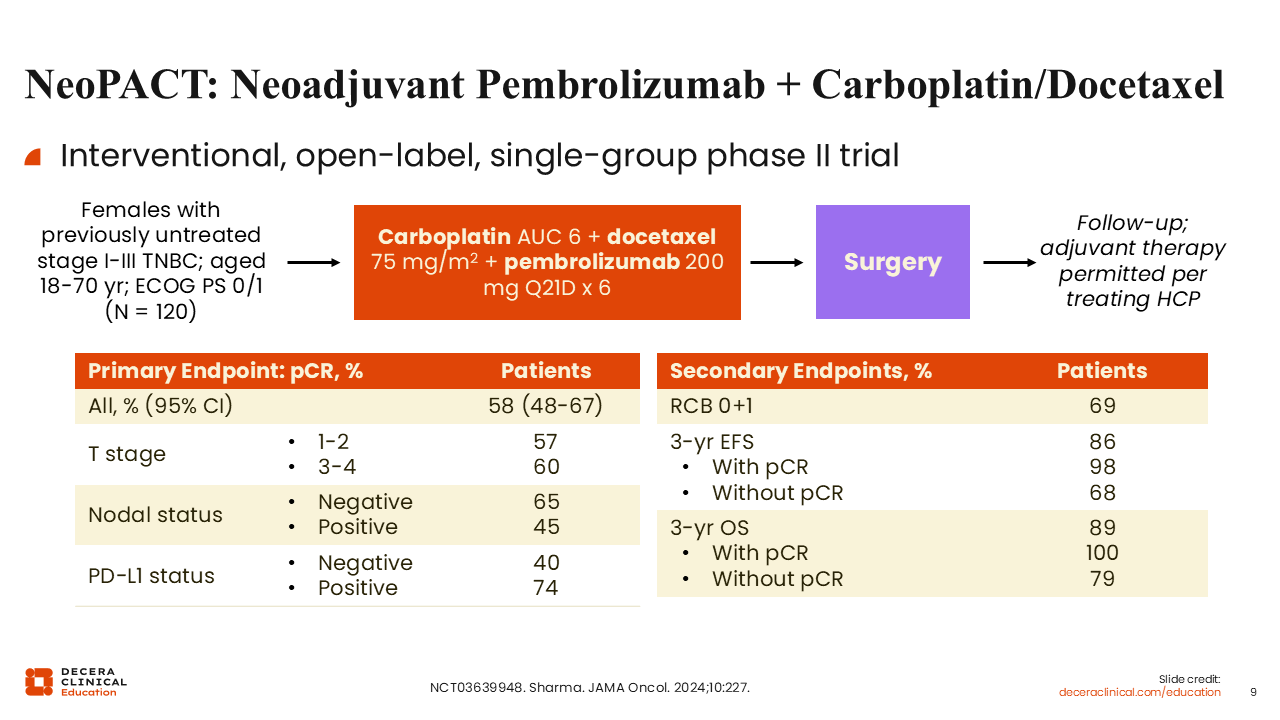
NeoPACT evaluated an anthracycline-free neoadjuvant chemoimmunotherapy approach in patients with TNBC. This open-label, single-group phase II trial enrolled women with previously untreated stage I-III TNBC at 2 centers between 2018 and 2022. Eligible patients received carboplatin area under the concentration curve 6, docetaxel 75 mg/m², and pembrolizumab 200 mg every 21 days for 6 cycles, with myeloid growth factor support administered with all cycles, followed by surgery. Postoperative systemic therapy was discretionary: Among 111 patients, 10 received adjuvant pembrolizumab and 39 received adjuvant chemotherapy, largely among those with residual disease. Adjuvant regimens included anthracycline-based chemotherapy, capecitabine, anthracycline followed by capecitabine, or platinum-based therapy.15
Among 115 evaluable patients, the median age was 50 years. Thirty-nine percent had node-positive disease, 12% had stage I disease, 75% had stage II disease, and 13% had stage III disease. Germline BRCA1/2 pathogenic variants were identified in 8% of patients, and PD-L1 combined positive score of ≥10 was detected in 46% of patients.15
These baseline characteristics limit direct comparison with KEYNOTE-522. NeoPACT included some patients with stage I disease and had a lower proportion of node-positive disease. Because NeoPACT was a single-group phase II study, it should be viewed as supportive and hypothesis generating rather than practice defining in the same way as phase III KEYNOTE-522.15,24
The primary endpoint in NeoPACT was pCR, defined as no evidence of invasive tumor in the breast and axilla. The pCR rate was 58% (95% CI: 48%-67%). Residual cancer burden 0+1 was reported in 69% of patients (95% CI: 60%-78%).15 pCR rates differed by baseline disease features. pCR was reported in 65% of patients with node-negative disease compared with 45% of patients with node-positive disease. Rates were also higher among patients with PD-L1–positive tumors than among those with PD-L1–negative tumors, at 74% vs 40%, respectively.15
At a median follow-up of 27.4 months, estimated 3-year EFS was 86% overall. Outcomes were notably better among patients who achieved pCR, with estimated 3-year EFS of 98%, compared with 68% among patients with residual disease. Estimated 3-year OS was 89% overall, 100% among patients with pCR, and 79% among patients with residual disease.15
The NeoPACT regimen was generally manageable, although AEs were common. Among 115 patients, grade ≥3 treatment-related AEs occurred in 26.9%. The most common grade ≥3 treatment-related AEs were diarrhea, anemia, and peripheral sensory neuropathy, reported in 4.3%, 3.5%, and 2.6% of patients, respectively. Immune-mediated AEs occurred in 26.1% of patients, with grade ≥3 immune-mediated AEs in 3.5%; colitis was the most common grade ≥3 immune-mediated event, reported in 1.7%.15
Treatment-related AEs led to discontinuation of any trial drug in 12% of patients. Pembrolizumab was discontinued in 7%, and chemotherapy was discontinued in 10%.15 These safety findings support anticipatory counseling, early symptom reporting, and coordinated management of chemotherapy-related and immune-mediated AEs.
NeoPACT provides clinically relevant evidence for an anthracycline-free neoadjuvant chemoimmunotherapy regimen, particularly for patients who may not be ideal candidates for anthracycline-based therapy. Its findings may help inform ongoing efforts to optimize chemotherapy backbones and explore treatment de-escalation strategies in selected patients with TNBC.
Capecitabine
Capecitabine is an oral fluoropyrimidine prodrug and nucleoside metabolic inhibitor that is converted to 5-fluorouracil. It has an established role in metastatic breast cancer and is also used in the postneoadjuvant setting for selected patients with HER2-negative breast cancer who have residual invasive disease after neoadjuvant chemotherapy.19,20
In early-stage TNBC specifically, capecitabine remains clinically relevant for selected patients with residual disease after neoadjuvant chemotherapy, particularly when PARP inhibitor therapy is not indicated or when postneoadjuvant treatment selection is being individualized as part of a shared decision-making discussion with the patient. Common AEs associated with capecitabine include stomatitis (67%), nausea (45%), diarrhea (67%), vomiting (35%), edema (33%), abdominal pain (30%), palmar–plantar erythrodysesthesia syndrome (63%), and alopecia (41%).19 These AEs should be discussed before therapy begins so that patients know what to report and when to contact the care team.
CREATE-X: Adjuvant Capecitabine vs SoC in Patients With Residual Disease After Neoadjuvant CT
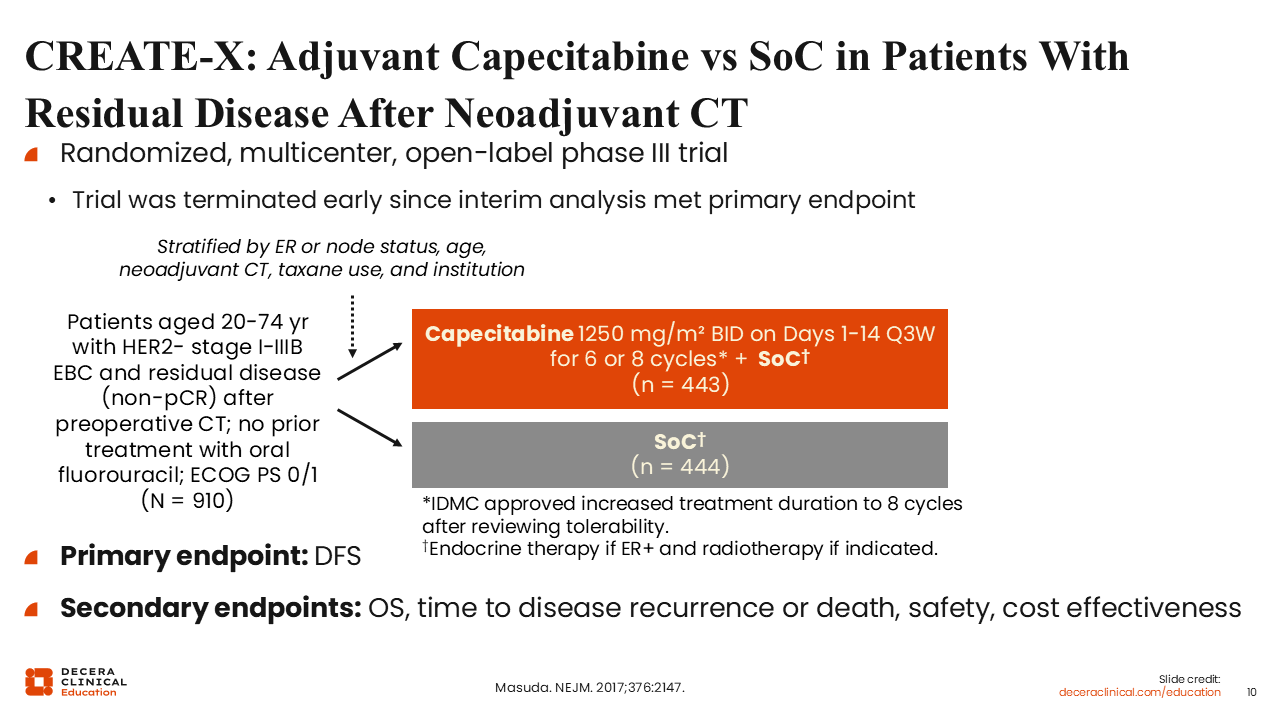
The pivotal phase III CREATE-X was a randomized, multicenter, open-label trial that established the role of adjuvant capecitabine in patients with HER2-negative breast cancer who had residual invasive disease after standard neoadjuvant chemotherapy.20 Eligible patients were 20-74 years of age and had stage I-IIIB HER2-negative breast cancer, residual disease after preoperative chemotherapy, no prior treatment with oral fluorouracil, and ECOG PS 0/1. Patients were randomized to receive capecitabine plus standard postsurgical treatment or standard postsurgical treatment alone. Capecitabine was administered at 1250 mg/m2 twice daily on Days 1-14 of a 21-day cycle for 6 or 8 cycles. Standard postsurgical treatment included endocrine therapy for patients with ER-positive disease and radiotherapy when indicated.
The primary endpoint was DFS, with secondary endpoints including OS, time to recurrence or death, safety, and cost-effectiveness.20 The study design addressed a high-risk postneoadjuvant population of patients who had already received preoperative chemotherapy but still had residual invasive disease at surgery.
CREATE-X: DFS and OS
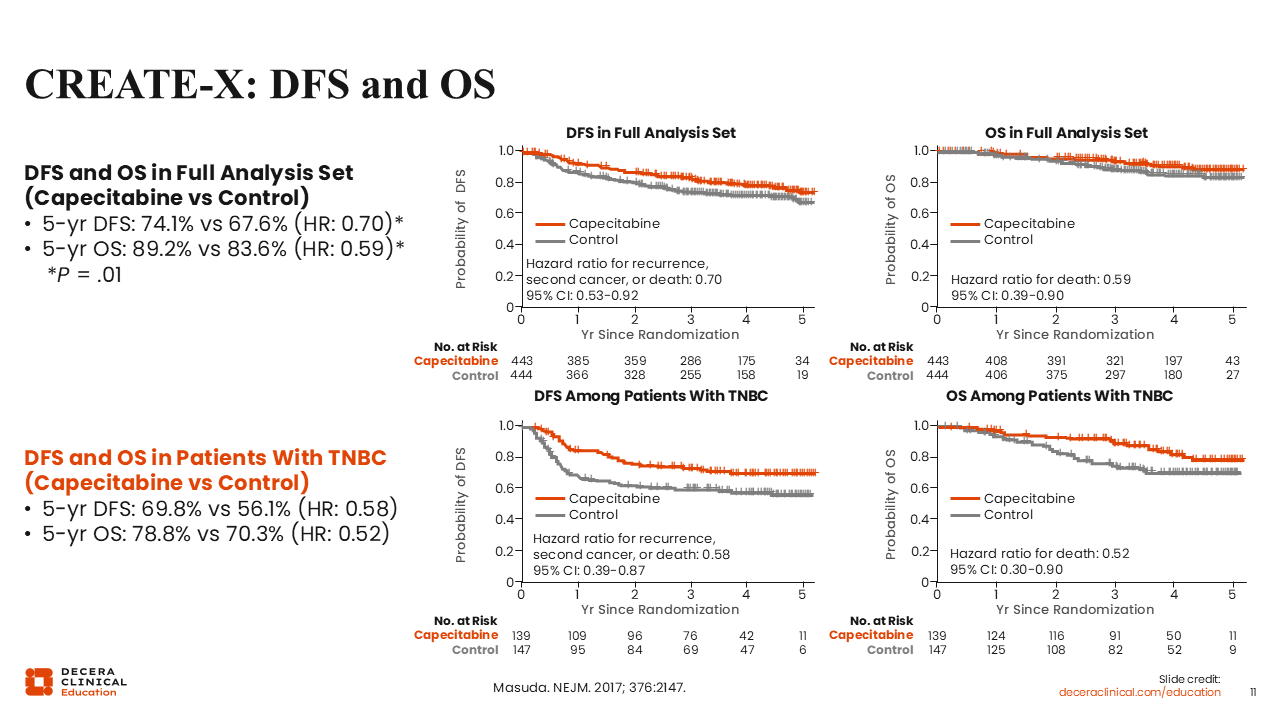
The trial was stopped early after an interim analysis discovered that the study had met the primary endpoint of improving DFS vs the standard of care at the time. In the full analysis set, adjuvant capecitabine improved 5-year DFS compared with the control standard-of-care arm (74.1% vs 67.6%, respectively). The hazard ratio for recurrence, second cancer, or death was 0.70 (95% CI: 0.53-0.92; P = .01). The 5-year OS was also higher with capecitabine than with control, at 89.2% vs 83.6%, respectively (hazard ratio for death: 0.59; 95% CI: 0.39-0.90; P = .01).20
Among patients with TNBC, 5-year DFS with capecitabine was 69.8% compared with 56.1% with the standard-of-care control arm. The hazard ratio for recurrence, second cancer, or death was 0.58 (95% CI: 0.39-0.87). Five-year OS in the TNBC subgroup was also higher with capecitabine, at 78.8% vs 70.3%, respectively. The hazard ratio for death was 0.52 (95% CI: 0.30-0.90).
Because CREATE-X was conducted before the routine use of perioperative pembrolizumab, capecitabine should now be considered within a broader postneoadjuvant framework that accounts for prior pembrolizumab exposure, germline BRCA1/2 status, olaparib eligibility, residual disease burden, toxicity profile, and patient preferences. Safety counseling remains important. Hand–foot syndrome was the most common AE to capecitabine in CREATE-X, occurring in 73.4% of patients receiving capecitabine.20 Patients should be counseled to report skin changes, pain, diarrhea, stomatitis, and other symptoms early so that supportive care, treatment interruption, or dose modification can be used when appropriate.
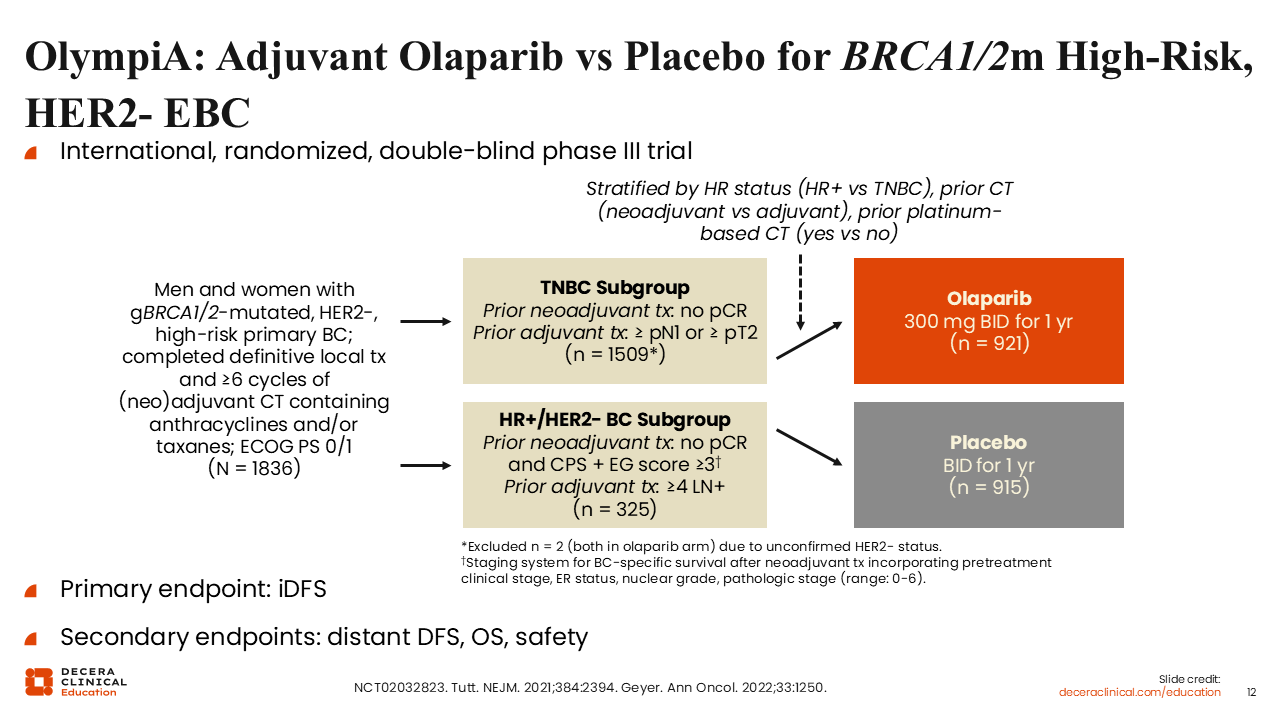
OlympiA: Adjuvant Olaparib vs Placebo for BRCA1/2m High-Risk, HER2-EBC
The international, randomized, double-blind phase III OlympiA trial evaluated 1 year of adjuvant olaparib vs placebo in patients with germline BRCA1/2-mutated, HER2-negative, high-risk EBC.18,28 Eligible patients had completed definitive local therapy and ≥6 cycles of neoadjuvant or adjuvant chemotherapy containing anthracyclines, taxanes, or both; platinum chemotherapy was permitted. Patients were also required to have ECOG PS 0/1.
OlympiA included both patients with TNBC and patients with HR-positive/HER2-negative breast cancer, but high-risk eligibility criteria differed by subtype and prior treatment approach. For patients with TNBC who had received neoadjuvant therapy, eligibility required residual invasive disease, defined as no pCR. For patients with TNBC who underwent surgery first and then received adjuvant chemotherapy, eligibility required at least pN1 disease or a primary tumor of at least pT2.28
Patients were randomized to receive olaparib 300 mg twice daily for 1 year or matching placebo. The primary endpoint was invasive DFS (iDFS), and secondary endpoints included distant DFS (DDFS), OS, and safety.28
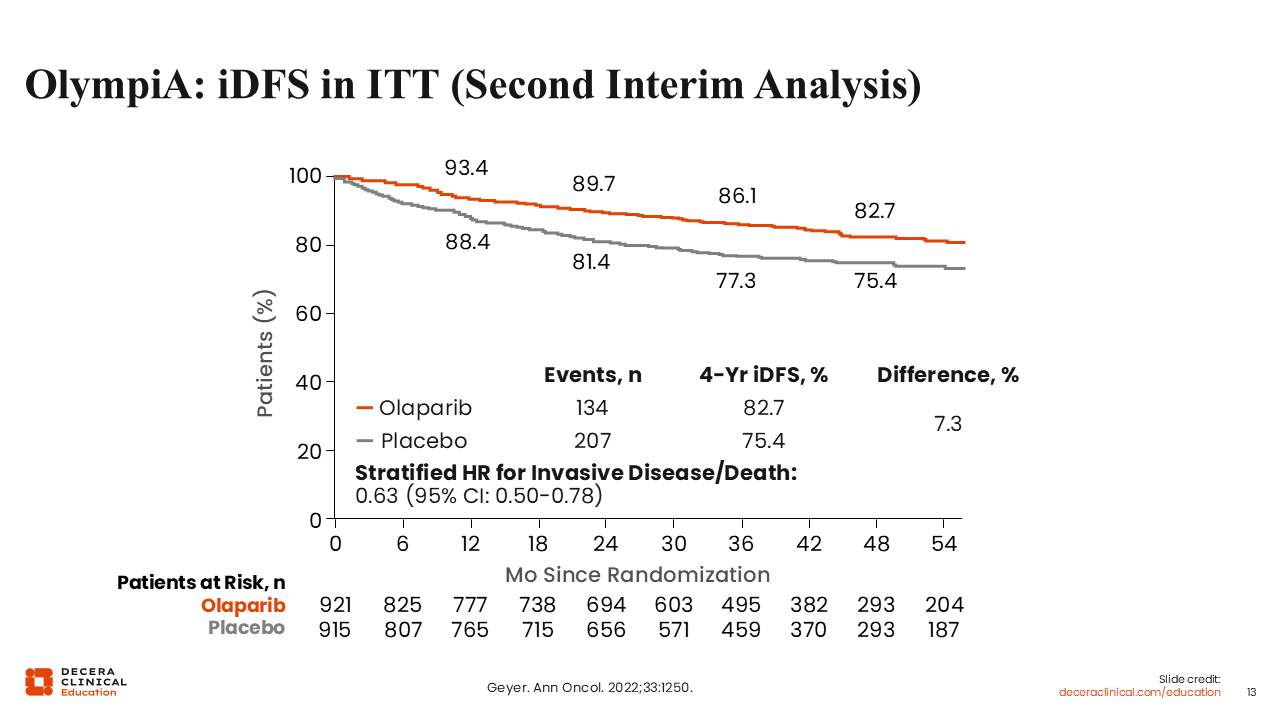
OlympiA: iDFS in ITT (Second Interim Analysis)
At the prespecified event-driven second interim analysis, investigators showed adjuvant olaparib for 1 year significantly improved iDFS compared with placebo. The 4-year iDFS was 82.7% with olaparib and 75.4% with placebo, corresponding to an absolute difference of 7.3 percentage points (hazard ratio for invasive disease or death: 0.63; 95% CI: 0.50-0.78).18
OS data also supported adjuvant olaparib in this population of early-stage TNBC with residual invasive disease. At the second interim analysis, 4-year OS was 89.8% with olaparib compared with 86.4% with placebo, corresponding to an absolute difference of 3.4 percentage points. The hazard ratio for death was 0.68 (98.5% CI: 0.47-0.97; P = .009).18
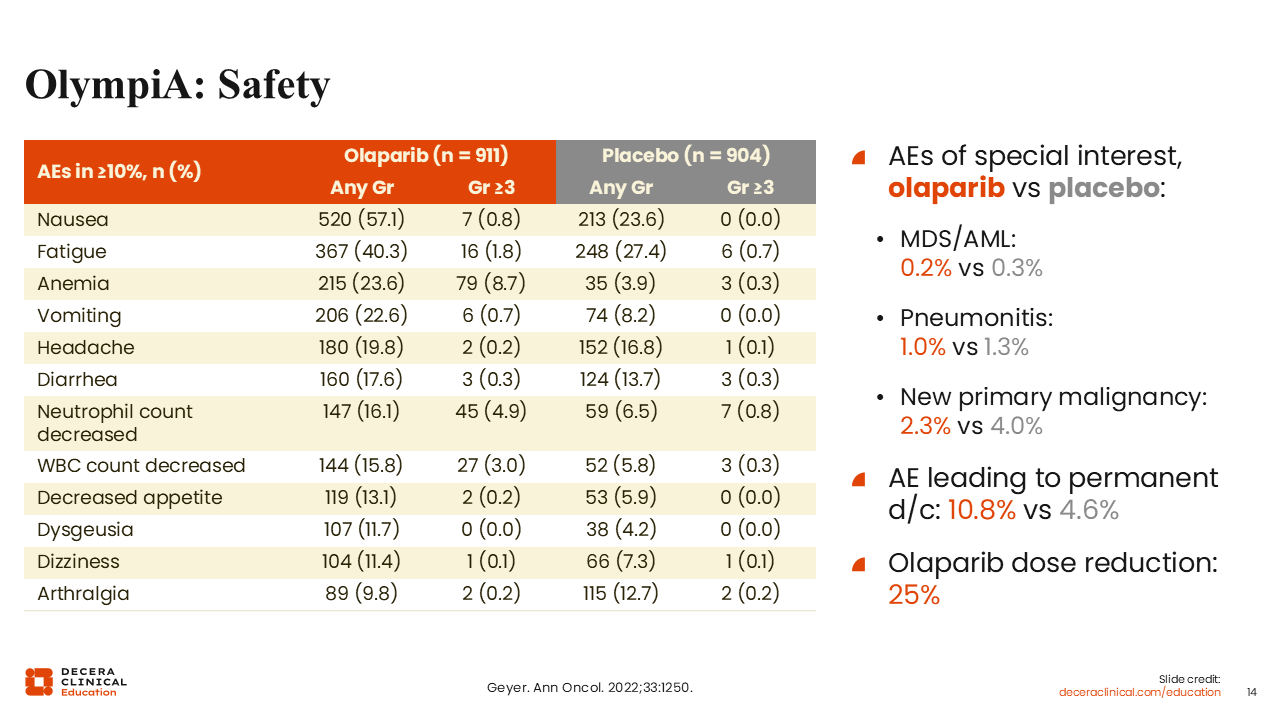
OlympiA: Safety
The safety profile of adjuvant olaparib in OlympiA was consistent with the known toxicity profile of PARP inhibition. The most common AEs occurring in ≥10% of patients receiving olaparib included nausea (57.1%), fatigue (40.3%), anemia (23.6%), vomiting (22.6%), headache (19.8%), diarrhea (17.6%), decreased neutrophil count (16.1%), decreased white blood cell count (15.8%), decreased appetite (13.1%), dysgeusia (11.7%), dizziness (11.4%), and arthralgia (9.8%).18
Nausea was the most common AE, occurring in 57.1% of patients receiving olaparib compared with 23.6% receiving placebo. Grade ≥3 nausea was uncommon, occurring in 0.8% vs 0%, respectively. Fatigue occurred in 40.3% vs 27.4%, with grade ≥3 fatigue in 1.8% vs 0.7%.
Hematologic AEs are particularly important for counseling and monitoring. Anemia occurred in 23.6% of patients receiving olaparib compared with 3.9% receiving placebo, with grade ≥3 anemia in 8.7% vs 0.3%. Decreased neutrophil count occurred in 16.1% vs 6.5%, with grade ≥3 events in 4.9% vs 0.8%, respectively.
AEs of special interest were uncommon, although myelodysplastic syndrome or acute myeloid leukemia occurred in 0.2% of patients receiving olaparib and 0.3% receiving placebo. Pneumonitis occurred in 1.0% vs 1.3%, and new primary malignancies occurred in 2.3% vs 4.0%, respectively.
AEs led to permanent discontinuation in 10.8% of patients receiving olaparib and 4.6% receiving placebo. Dose reduction was required in 25% of patients receiving olaparib. These findings support counseling before treatment begins and reinforce that dose interruption or dose reduction can be an appropriate AE management strategy.
For patients who have already received perioperative pembrolizumab, randomized comparative data do not yet define the optimal sequencing or combination of adjuvant pembrolizumab, olaparib, and/or capecitabine. In this setting, treatment selection should be individualized for each patient.
OlympiA established adjuvant olaparib as a treatment option for appropriately selected patients with germline BRCA1/2-mutated, HER2-negative, high-risk EBC. This reinforces the need to complete germline testing early enough to support adjuvant treatment planning, particularly for patients with residual disease after neoadjuvant therapy or other high-risk features after upfront surgery.
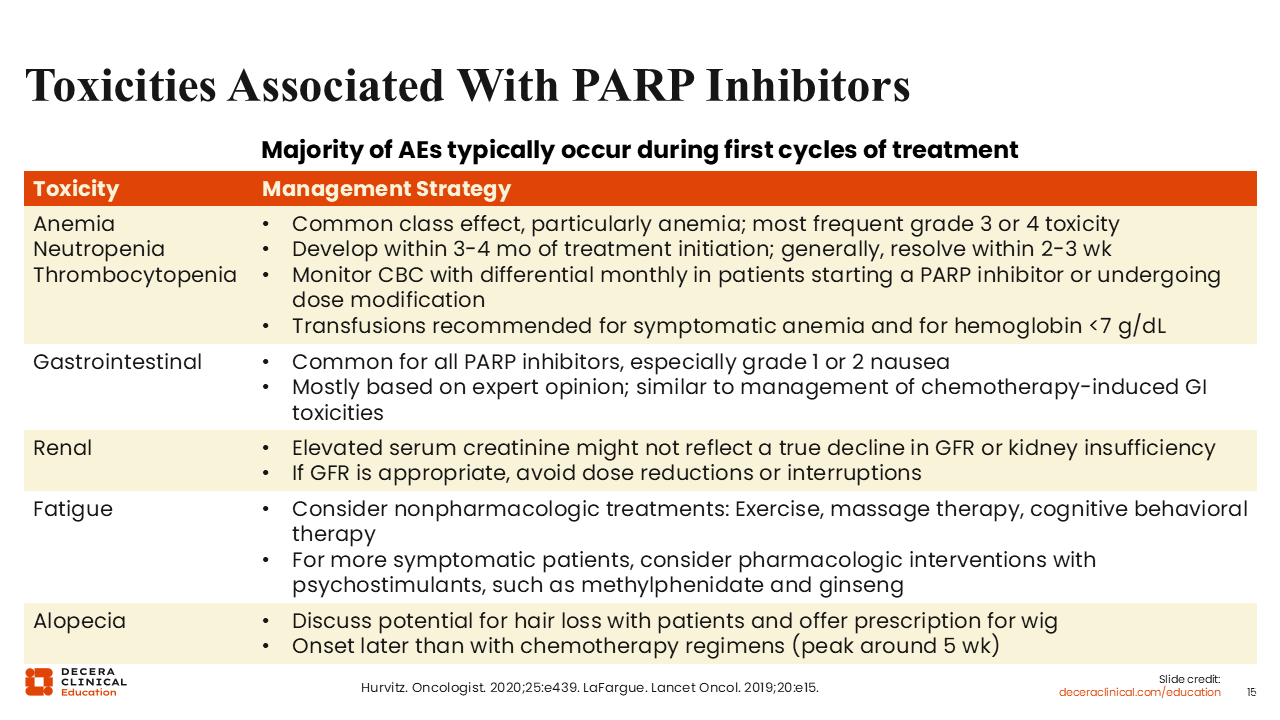
Toxicities Associated With PARP Inhibitors
AEs with PARP inhibitors can be common but are generally manageable. AEs often occur early during the first several cycles of treatment.10
Hematologic AEs are among the most clinically relevant class effects, particularly anemia (any grade: ~24%-53%; grade ≥3: ~9%-39%), which is the most frequent grade 3/4 AE. Neutropenia (any grade: ~16%-35%) and thrombocytopenia (any grade: ~11%-27%) may also occur, typically developing within the first 3-4 months and often resolving within several weeks.10,29 Routine complete blood count monitoring with differential is recommended at treatment initiation and during dose modification, with transfusion considered for symptomatic anemia or hemoglobin <7 g/dL.30,29
Nonhematologic AEs should also be monitored and managed proactively. GI events, particularly low-grade nausea (~49%-58%), are common across PARP inhibitors and are generally managed similarly to chemotherapy-associated GI AE.29 Serum creatinine elevations may occur without indicating a true decline in glomerular filtration rate (~3%).10,18 Thus, dose interruption or dose reduction may be avoidable when renal function is otherwise appropriate. Fatigue (~37%-62%) may be addressed first with nonpharmacologic strategies, with pharmacologic approaches considered for more symptomatic patients. Alopecia (<20%) should be discussed in advance, including its later onset compared with many chemotherapy regimens, so that supportive measures can be offered early.10,29,30
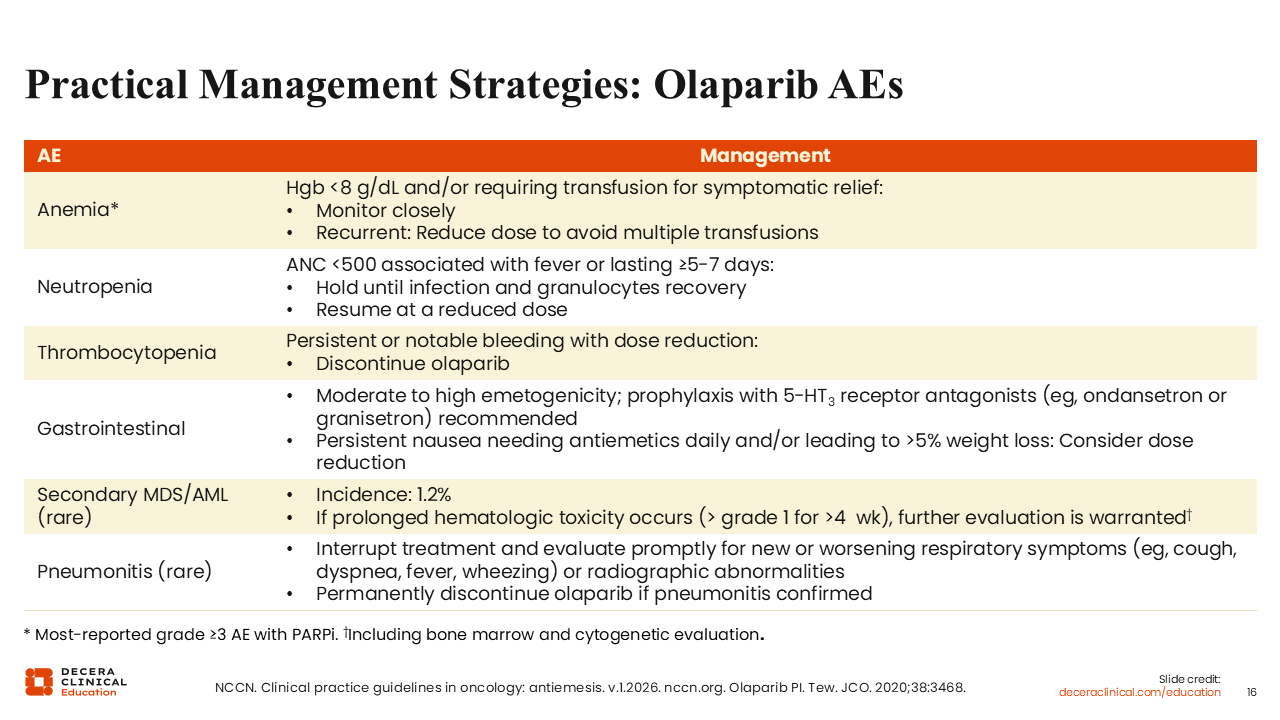
Practical Management Strategies: Olaparib AEs
Practical management of olaparib-associated AEs centers on early recognition, supportive care, and dose modification when clinically needed. For anemia, the most commonly reported grade ≥3 AE with PARP inhibitors, patients with hemoglobin <8 g/dL and/or symptomatic anemia requiring transfusion should be monitored closely; recurrent transfusion need may warrant dose reduction to avoid repeated transfusions.10,31
Management of neutropenia and thrombocytopenia should be guided by severity, persistence, and clinical context. For febrile neutropenia or absolute neutrophil count <500/μL lasting ≥5-7 days, olaparib should be held until infection has resolved and granulocytes have recovered and then resumed at a reduced dose. For thrombocytopenia with persistent or notable bleeding despite dose reduction, discontinuation of olaparib should be considered.10,31
Nonhematologic and rare serious AEs also require proactive management. For example, GI toxicity may warrant antiemetic prophylaxis because olaparib has moderate to high emetogenic potential; persistent nausea requiring daily antiemetics and/or associated with >5% weight loss may warrant dose reduction.10,32 Although secondary myelodysplastic syndromes/acute myeloid leukemia are rare (~1.2%), prolonged hematologic AE above grade 1 for more than 4 weeks should prompt further evaluation, including bone marrow and cytogenetic assessment. New or worsening respiratory symptoms or radiographic abnormalities should prompt treatment interruption and evaluation for pneumonitis; olaparib should be permanently discontinued if pneumonitis is confirmed.10,31