CE / CME
From Flare to Control in Atopic Dermatitis: Improving Outcomes in Pediatric Patients With Moderate to Severe Disease
Nurse Practitioners/Nurses: 1.00 Nursing contact hours, includes 1.00 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Released: June 27, 2025
Expiration: June 26, 2026


Activity
Avoid Common Triggers
Katie Smiley, PA-C:
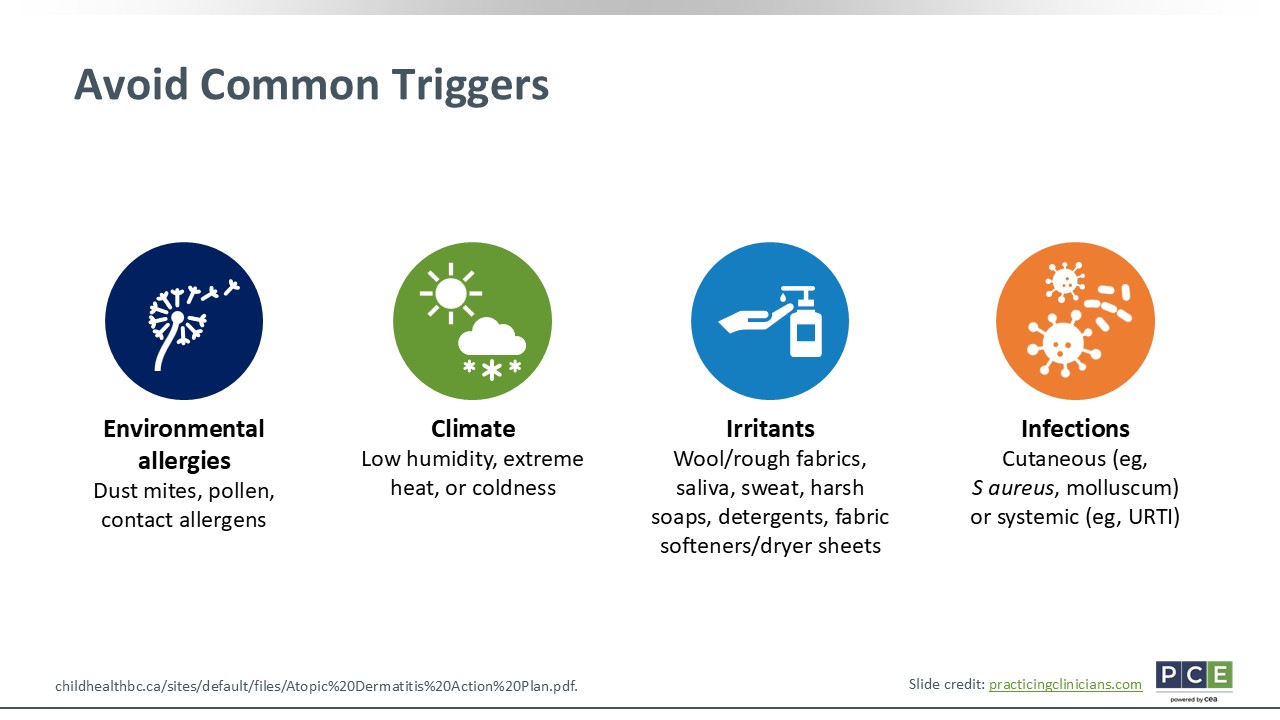
An often overlooked but practical treatment strategy is avoiding triggers. As previously mentioned, AD is a multifactorial disease, but sometimes we are able to pinpoint what exactly exacerbates the disease or causes flare-ups. I work in allergy, so I talk a lot about environmental allergies with patients who have both AD and allergic rhinitis. I talk extensively about dust mite precautions, reducing pollen exposures, and addressing contact allergens. I often see children with AD who flare-up in drier/low humidity environments because their skin dries, although others who experience extreme hot and cold can have exacerbated lesions as well.
We also discuss irritants. With infants, the high traffic area of their drool and saliva is often a common trigger, so we will try to reduce that exposure using emollients as a barrier. I then talk a lot about their products and detergents, fabric softeners, and dryer sheets that could potentially worsen their AD. I recommend to all my patients with AD that they use fragrance-free, dye-free products. Finally, infections can also drive flare-ups. Both cutaneous infections with S aureus or molluscum and common colds or systemic infections can lead to AD worsening.42
Pediatric AD Action Plan
Katie Smiley, PA-C:
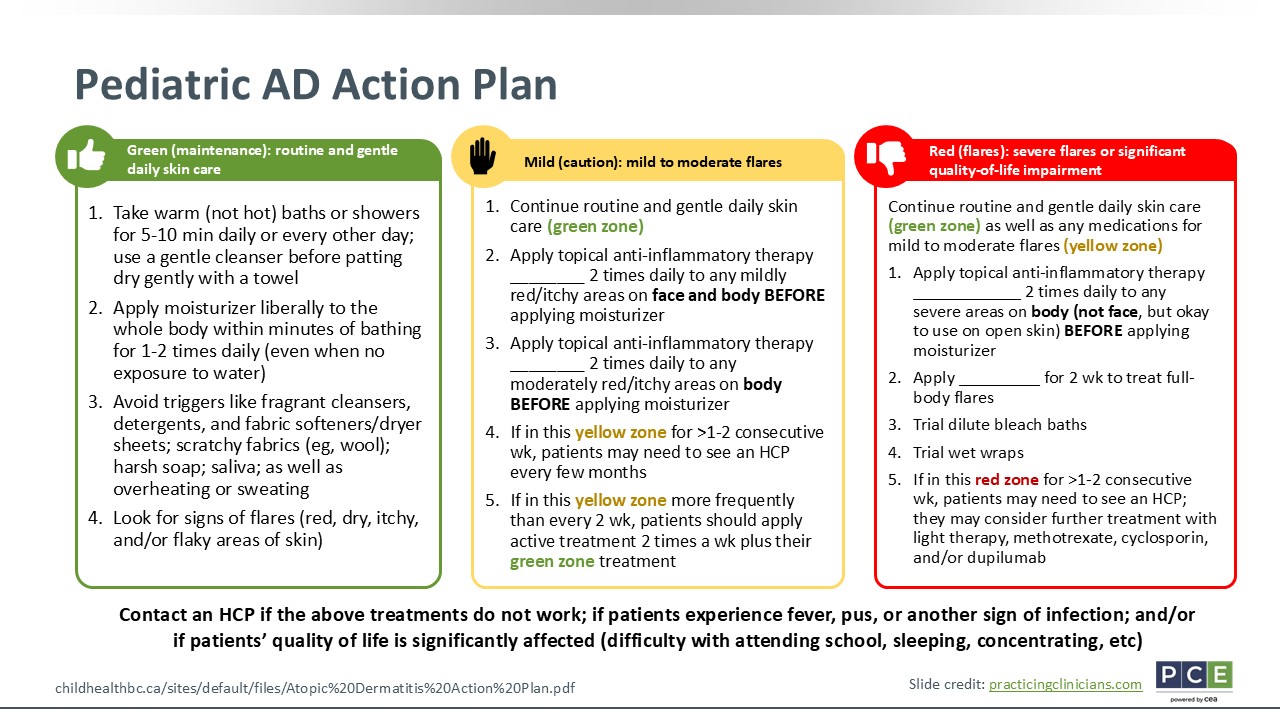
This slide outlines the pediatric AD action plan. It should look similar to an asthma action plan for those of us that work in allergy. Green is for everyone with AD. Mild to moderate flares are shown in yellow, and severe disease is in red.
When patients are in “green,” that means that their skin is doing well. Patients are recommended to take warm (not hot) baths or showers daily or every other day, followed by a gentle pat dry and moisturization right after that. I agree with Dr Wan; I like creams or emollients rather than lotions because they really help moisturize the skin. Patients ideally should moisturize twice daily, but at minimum at least once daily. Then they should avoid triggers, like I mentioned previously. HCPs also should counsel patients on how to recognize flare-ups. They differ from patient to patient. If a flare is considered to start as soon as a patient gets itchy, then we might decide to move on to the yellow box. Or maybe it is when they start to notice a rash develop, then we move on to the yellow zone. This is really based on individualized discussions with patients to determine what they consider to be a flare-up for themselves.
Moving on to the “yellow zone,” this is when patients have mild to moderate flare-ups. HCPs should recommend a topical anti-inflammatory therapy to patients. I typically have patients use a TCS with mild to moderate potency before applying their moisturizer. As their AD gets better, I will step that TCS therapy down and add something else to their regimen to apply twice weekly to patients affected areas or hotspots to help them maintain clear skin.
For the “red zone,” this occurs when patients experience severe flare-ups, which significantly affects their quality of life, including itch and sleep. In this case, I typically increase the potency of the prescribed topical therapy to apply before moisturizer. Especially if patients are prone to skin infections, I will discuss bleach baths with them and have them try wet wraps as much as they are able to tolerate them. Then I always counsel patients if they are using a moderate to high potency TCS for more than one half a month in particular. I will tell them that we cannot just get by with this treatment, so we need to discuss their other options.42
I also like to talk about how there is no cure for AD. It is a chronic disease. We have tools in our toolbox both for when skin clearance is achieved and when moderate to severe flare-ups occur. If needed, we can use targeted precision agents that are now more available to patients, too.
Patient Case Discussion: 12-Year-Old Girl Presents With Worsening AD
Katie Smiley, PA-C:
Looking at another patient case, a 12-year-old girl presents with worsening AD that started when she was 8 years of age. At that time, it only affected her antecubital and popliteal fossa and neck, but now it has spread to other areas of her body. It is worse in the winter and better in the summer, so she might have that low humidity exacerbating trigger.
The patient has used various TCS and nonsteroidal topical therapies. She is allergic to dogs, trees, and chickens for which she takes cetirizine 10 mg daily. There are no pets at home. She also has allergic rhinitis, but no food allergies or asthma. Her mother and sister have AD, and her dad has vitiligo.
The patient has AD involvement on numerous areas of her body: the face, neck, and trunk. The affected body surface area is 60% to 70%. How should we address treatment for this patient using SDM?
SDM Principles
Katie Smiley, PA-C:
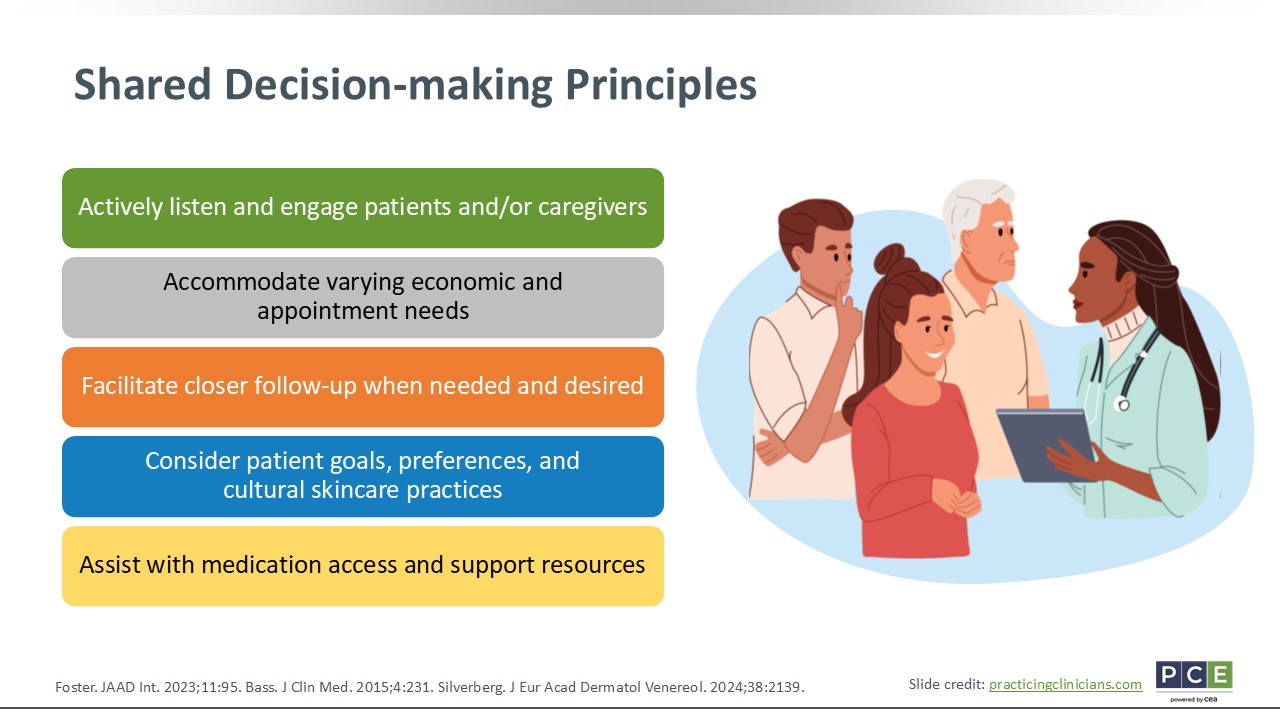
The patient in our case has used a lot of topical therapies. Therefore, these topicals alone are not controlling her AD. In this case, I think it is critical to validate the patient and family's experience. She has experienced flare-ups for years and has had limited response to the therapies that she used. This patient is also likely struggling with some psychosocial involvement. She is a preteen and has AD on her face, which probably has some effect on her emotional well-being.
I always review treatment goals with patients. I ask open-ended questions about what their goals for treatment are. What is most important for them? Is it itch they want to clear? Is it their skin lesions they want to clear? I often ask them what sport or activity do they do or not do because of their AD. Do they want to use that activity as a treatment goal?
I also like to present the available therapeutic options clearly. I believe in SDM, and more specifically informed SDM. That includes presenting all the available treatment options, their benefits and risks, and what we as HCPs do if there is any necessary monitoring. Based on patients’ affected body surface area and severity, we determine together if they would qualify for various treatments and I educate them on their available options. Then I work with them to decide what treatment fits best in their lifestyle. Some patients worry about injections, whereas others worry about taking a daily medication. Fortunately there are different options for patients, so we can work with everyone to find the therapy that works best for them.
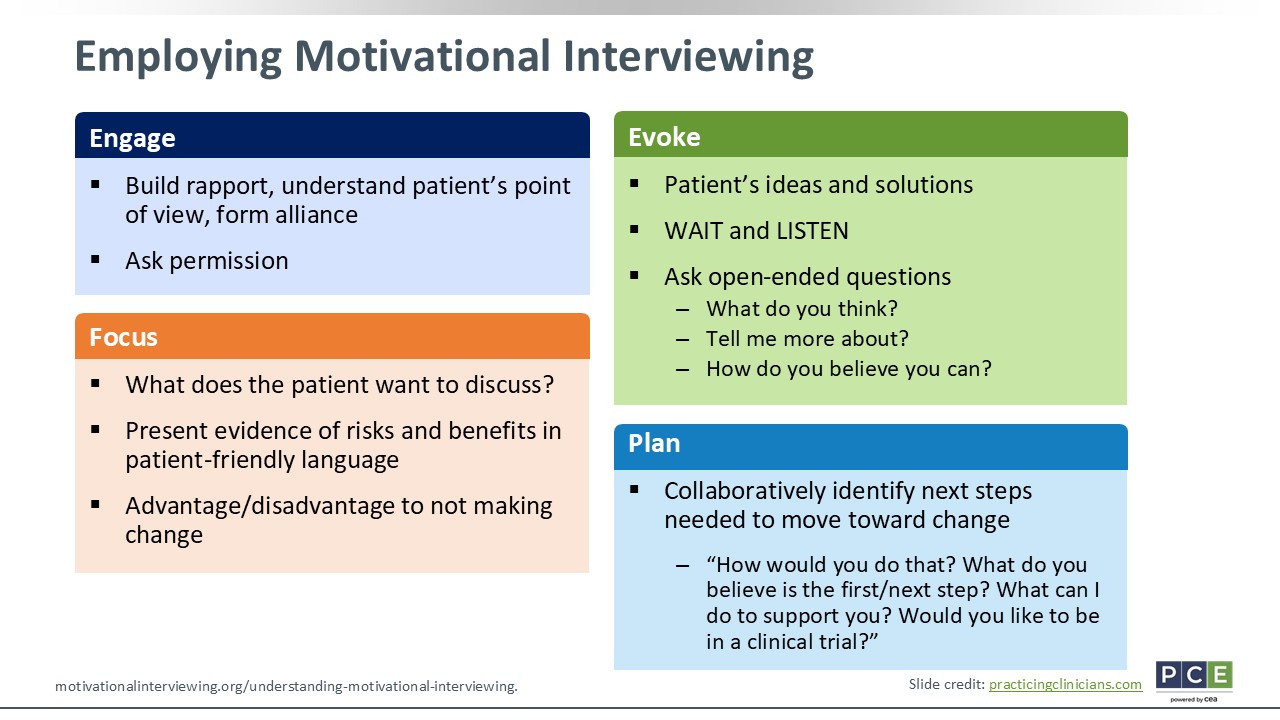
Employing Motivational Interviewing
Katie Smiley, PA-C:
Motivational interviewing is important to use: engage, focus, evoke, and plan. By engaging patients and their families, you will build rapport. Ask those open-ended questions to continue building that trust. Ask permission. Would be okay to talk about your skincare regimen? Things like that.
For focus, let patients drive the discussion. What do they want to work on? What do they want to improve? What is their treatment goal? That puts them at the center as the quarterback or captain of their AD.
Then evoke—ask patients what their ideas or solutions are. With my patients who are teenagers, I ask them what they have read about online. Sometimes their information is accurate, but most of it is not. But this approach lets them be the quarterback or lead the show. I wait, listen, and give them time to ask questions by not speeding through their visit.
Then finally is plan. HCPs should collaboratively identify the next steps needed to make change. How should we do this? How best can we work with patients to move forward in a better direction?43
Key Takeaways
Katie Smiley, PA-C:
For key takeaways, AD significantly impairs the quality of life of patients and their caregivers. It affects them through symptoms like itch, sleep disturbance, and pain that continue affecting quality of life. Topical therapies are typically our first-line treatments. However, they come with burdens. There now are new systemic options that are available to patients with more severe or refractory AD.
It is important to engage patients and their caregivers in SDM. Work with them to build rapport, which promotes trust, treatment adherence, self-confidence, and management. That will lead to better outcomes. Furthermore, developing patient-specific action plans and individualizing care can help them recognize early flare-ups and help HCPs know when/how to escalate treatment and address any barriers to care.