CE / CME
From Flare to Control in Atopic Dermatitis: Improving Outcomes in Pediatric Patients With Moderate to Severe Disease
Nurse Practitioners/Nurses: 1.00 Nursing contact hours, includes 1.00 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Released: June 27, 2025
Expiration: June 26, 2026


Activity
Caregiver Perspective: The Burden of Pediatric AD
Katie Smiley, PA-C:
Before reviewing the patient and caregiver burden of AD, please watch the following video of a caregiver describing her perspective on how this disease affects her and her family.
Atopic Dermatitis: Epidemiology and Pathogenesis
Katie Smiley, PA-C:
AD affects up to 20% of children. It is one of the most common chronic inflammatory skin disorders we see, and it typically starts in children 3-6 months of age. Furthermore, 60% typically are diagnosed before they turn 1 year of age and 85% are diagnosed by the time they turn 5 years of age. It is an early life disease, with approximately 60% of childhood AD cases persisting into adulthood. Therefore, it is not just a pediatric condition.
There is variability in the AD disease course, too. Some children may outgrow it or experience long-term periods of remission, whereas others have more of a relapsing-remitting pattern that continues to flare and resolve throughout their lives. This is why it is important to set expectations for families—that AD may be a long-term condition and that we have evolving strategies to treat this disease as the child ages.1-4
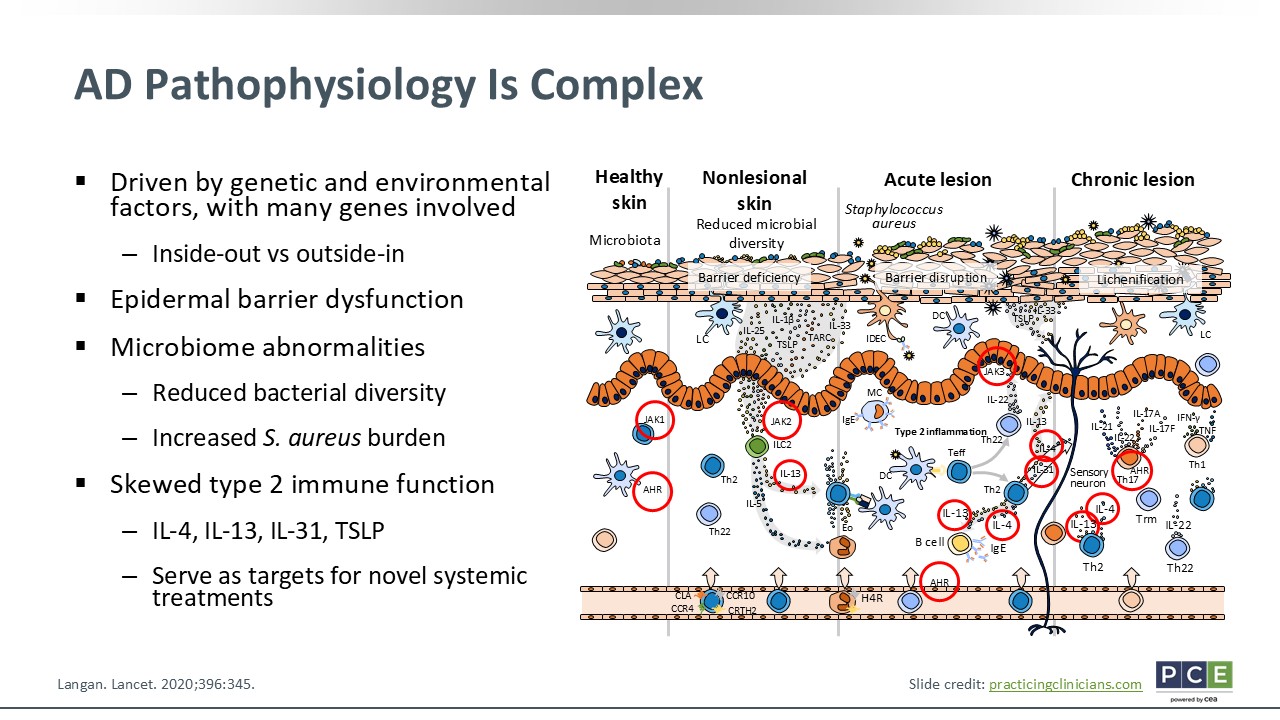
AD Pathophysiology Is Complex
Katie Smiley, PA-C:
AD is not a simple or easy disease. It is complex; it is multifactorial. It is a chronic inflammatory skin disorder that is influenced by both genetics and environmental exposures. Often we talk about the inside–out or outside–in hypotheses. These both explain the interplay between skin barrier dysfunction and immune dysregulation. The inside–out hypothesis poses the idea that immune dysregulation first occurs with overactive type 2 immune cytokines, mainly IL-4, IL-13, and IL-31. These key cytokines impair the skin barrier, which leads to decreased filaggrin and antimicrobial peptide production and a compromised skin barrier. The outside–in hypothesis poses an idea on how the skin barrier is compromised. In this model, allergens, irritants, and microbes penetrate the skin barrier more easily. Once inside, these allergens can trigger and activate an immune response.
Patients with AD also have impaired stratum corneum, which leads to reduced lipid content in the skin, decreased filaggrin expression, and increased trans epidermal water loss. Thus, creating dry skin and making it more penetrable to the irritants and microbes. In AD, the skin also has a decrease in its microbial diversity. There are increased colonies of disease causing Staphylococcus aureus, too, that tend to flare or become even more prominent during times of flare-ups. Yet the hallmark of AD is the skewed type 2 inflammatory response with those prominent cytokines (IL-4, IL-13, IL-31 and thymic stromal lymphopoietin) being major players. These are the therapeutic targets for new and emerging systemic agents.5,6
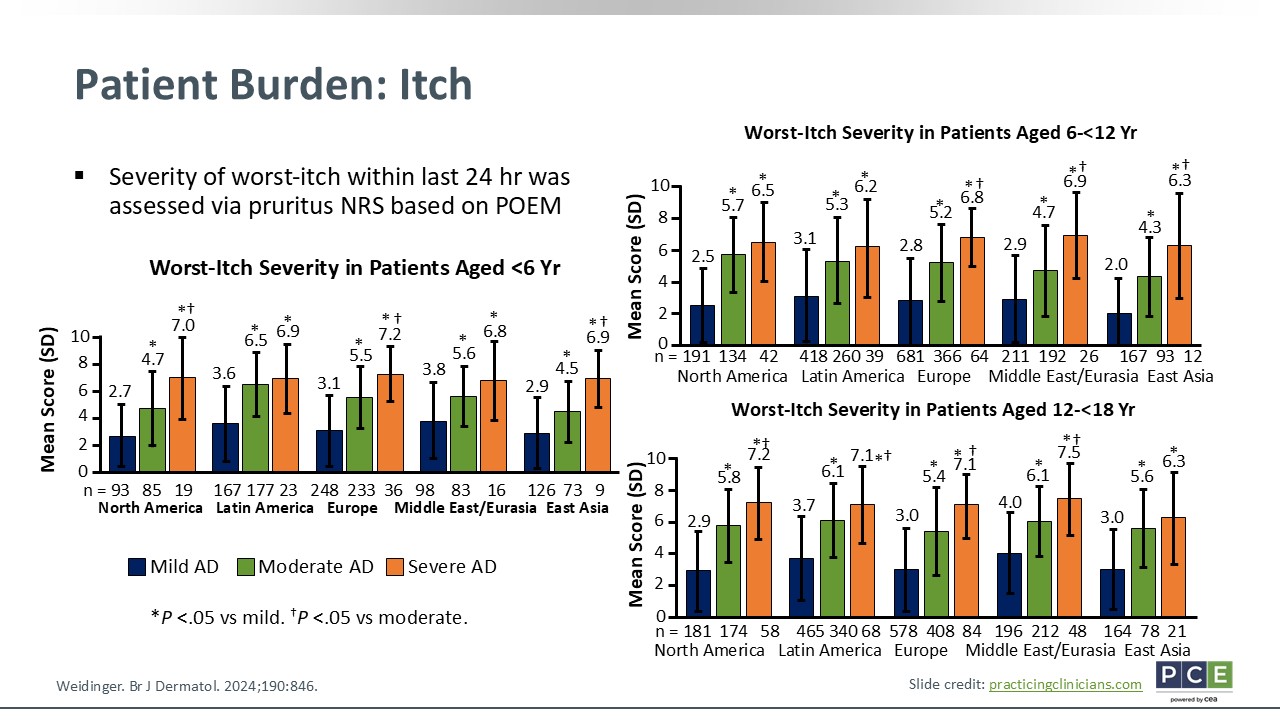
Patient Burden: Itch
Katie Smiley, PA-C:
Now, let us look at the different factors of the patient experience measured by the Patient-Oriented Eczema Measure (POEM). Of course, itch is likely the most common burden that we discuss in patient visits, and it is a focus of research. The figure on this slide illustrates the worst-itch within the past 24 hours, stratified by age, geographic location, and disease severity. Across all age groups, symptom scores rose significantly as patients’ disease severity increased. With adolescents and adults specifically, POEM itch-related scores ranged from 6.3-7.5 out of 10.0 for those with severe AD. Furthermore, these graphs reinforce the idea that itch is incredibly burdensome for patients; it is not just a number. It also shows that persistent and disruptive itch affects sleep, quality of life, and patients’ ability to participate in school, sports, and activities—all the things that children love to do.4,7
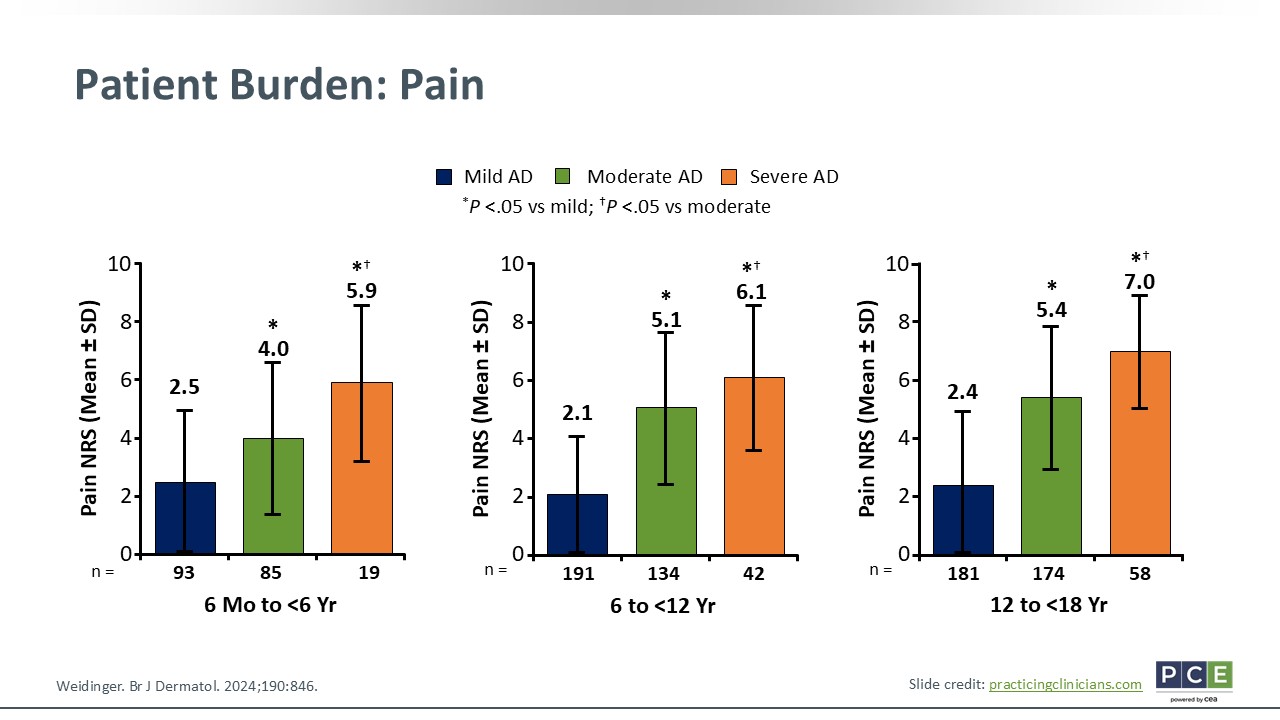
Patient Burden: Pain
Katie Smiley, PA-C:
I think a more underrepresented symptom of AD is pain. When discussing itch, researchers have connected this symptom with sleep, but we do not necessarily talk about pain. Pain can stem from excoriated lesions, infections, and nerve sensitization with chronic inflammatory areas. This slide illustrates the burden of pain in AD. Like itch, pain scores increase as disease severity worsens. Adolescents and adults reported a mean score of 7.0 among those with severe AD compared with 2.4 among those with mild disease.4
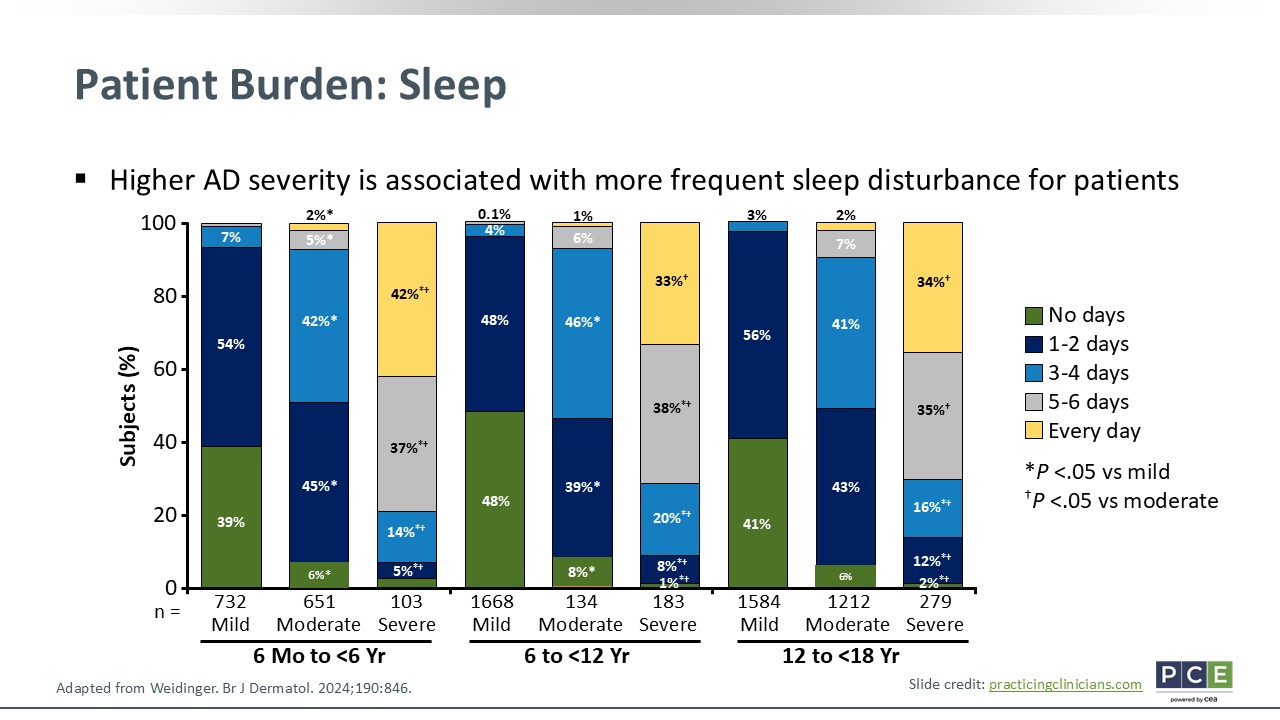
Patient Burden: Sleep
Katie Smiley, PA-C:
Moving onto sleep, obviously, this is a big concern that should be addressed in patient care. It is the consequence of both itch and pain. So this figure breaks down the days of sleep disruption patients experienced over the past week, stratified by age and disease severity. I want to call out among middle and elementary school-aged children, the vast majority with severe AD had more than 5 nights with sleep disturbances, which was statistically significant when compared with moderate disease.
We know that sleep quality among children also affects their caregivers. When patients are not sleeping, their parents are not sleeping. This affects everyone's mood and behavior. In addition, it affects patients’ ability to interact and participate in school and classes, which hinders their academic performance.4,7
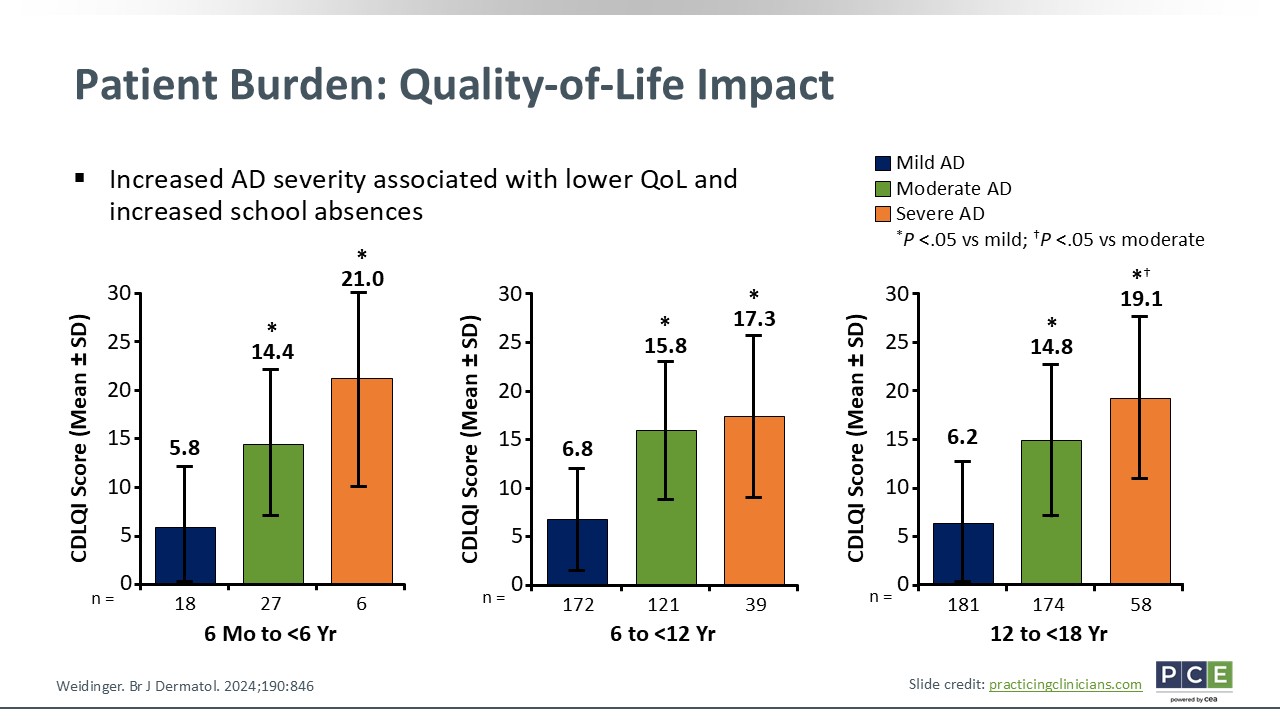
Patient Burden: Quality-of-Life Impact
Katie Smiley, PA-C:
Quality of life often is measured in pediatrics by the Children's Dermatology Life Quality Index. This scale captures the daily impact of AD on school, friendship, self-esteem, and emotional well-being. Across all age groups, the slide shows how quality of life was markedly worse in the patients with mild to moderate AD. Among adolescents and adults with mild disease, their quality of life score was 6.2 compared with 19.1 among those with severe AD. That is more than a threefold increase in how much their lives were affected by AD.
I think quality of life is important to highlight. When treating AD, we are not just treating the skin. We should be treating patients as a whole; therefore, intentionally treating to improve their quality of life.4
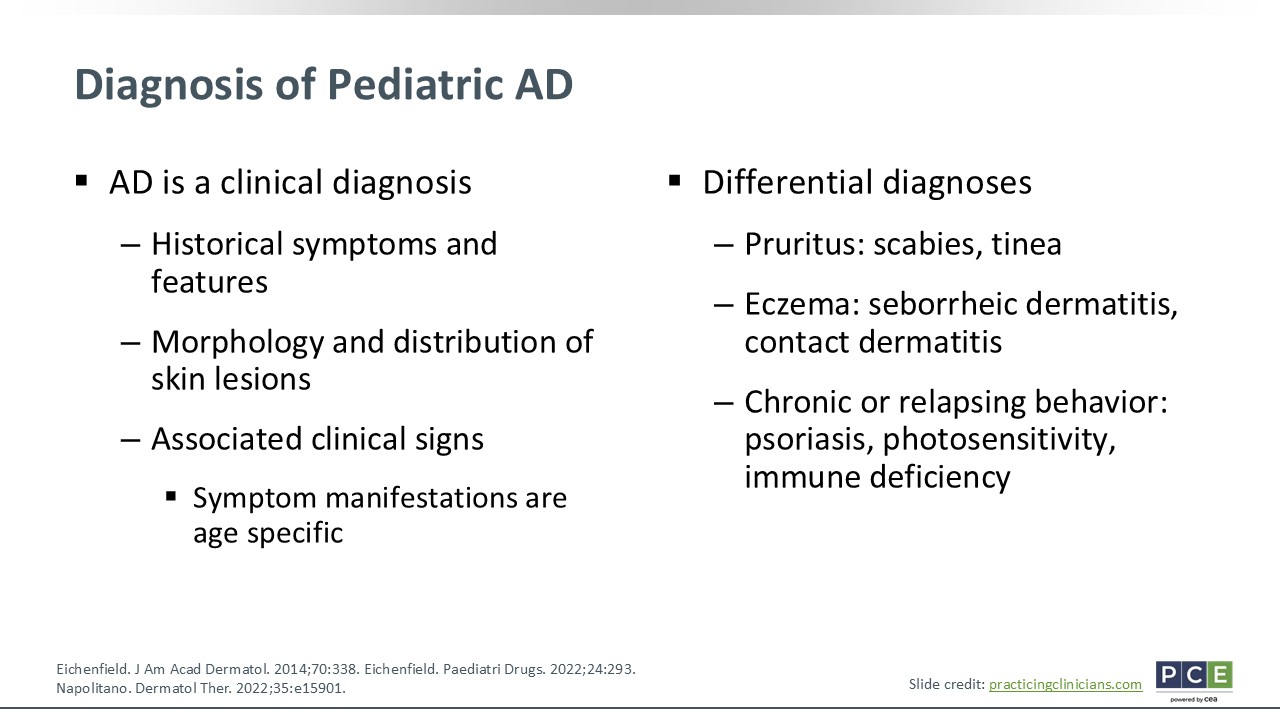
Diagnosis of Pediatric AD
Katie Smiley, PA-C:
AD requires a clinical diagnosis. There are no specific lab tests and we typically do not biopsy the skin. Rather, HCPs should rely on patients’ history, the recognition of lesion patterns, and common symptoms like itch. Sometimes there is a personal or family history of atopic conditions, and the clinical presentation can differ as patients age.
Differential diagnoses of AD among patients presenting with pruritus include scabies or tinea, especially if the skin lesions do not fit in the classic AD picture. HCPs should consider seborrheic dermatitis or contact dermatitis with eczema, and psoriasis, photosensitivity, or immune deficiency if there is marked chronic/relapsing behavior. These differential diagnoses should be considered if patients’ disease is refractory to treatment or if they have an atypical presentation.8-10
Clinical Presentation Variability
Katie Smiley, PA-C:
As previously mentioned, AD presentation can change as patients age. In babies, there is a lot of activity on the face. I call it a high traffic area because of all the saliva and drool that is going on. AD also affects the extensor extremities and flexural creases. As children age, AD affects their face, neck, and hands, specifically. It sometimes has activity on feet and flexural creases, rather than the extensor surfaces of extremities. In adults, often AD is seen in their flexural creases and on the hands and feet.11
Presentation on Varying Skin Tones
Katie Smiley, PA-C:
The presentation of AD also differs based on skin tone. This is important because it can look differently on patients with skin of color. For example, patients with darker skin tones can have inflammation that looks more papular or violaceous. Whereas on lighter skin tones, AD has a more pink/red appearance. Postinflammatory hyperpigmentation or hypopigmentation is also important to note. Sometimes I have patients who are more bothered by their postinflammatory hyperpigmentation than the AD itself.12
Clinical Assessment Tools
Katie Smiley, PA-C:
There are a couple of clinical assessment tools that HCPs can use in the clinic that are also used in clinical trials. There is the Eczema Area and Severity Index (EASI). This score gives a breakdown by body surface area and lesion severity across 4 body regions: the head/neck, trunk, upper extremities, and lower extremities. It provides a more quantitative scoring of patients' disease.13 The Investigator Global Assessment (IGA) is a scale scored from 0-4. It provides an overall impression of patients' AD.14 Both the EASI and IGA are objective tools that can help you track disease control and improvements/treatment response.
Also we have a couple patient-reported outcomes scoring tools. One is the SCORing Atopic Dermatitis Calculator, and the other is the POEM. The SCORing Atopic Dermatitis Calculator incorporates visual signs to track patient-reported symptoms like itch and sleep disturbances, whereas the POEM is fairly quick and easy to complete by capturing how often certain symptoms bother patients throughout the week.
Differentiating AD Severity
Katie Smiley, PA-C:
Once HCPs diagnose a patient with AD, they also need to determine disease severity. HCPs must be able to differentiate AD severity. Mild disease includes small, dry patches of skin with some itching and a minimal impact on quality of life or sleep. With moderate disease, patients will have dry skin that is frequently itchy with excoriations, redness, and a significant impact on quality of life and sleep. Then severe disease presents with large areas of dry skin that is constantly itchy with redness and excoriation that strongly impedes patients’ daily routines and sleep.9