
CE / CME
From Flare to Control in Atopic Dermatitis: Improving Outcomes in Pediatric Patients With Moderate to Severe Disease
Nurse Practitioners/Nurses: 1.00 Nursing contact hours, includes 1.00 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Released: June 27, 2025
Expiration: June 26, 2026


Activity
Assess AD Severity
Joy Wan, MD, MSCE:
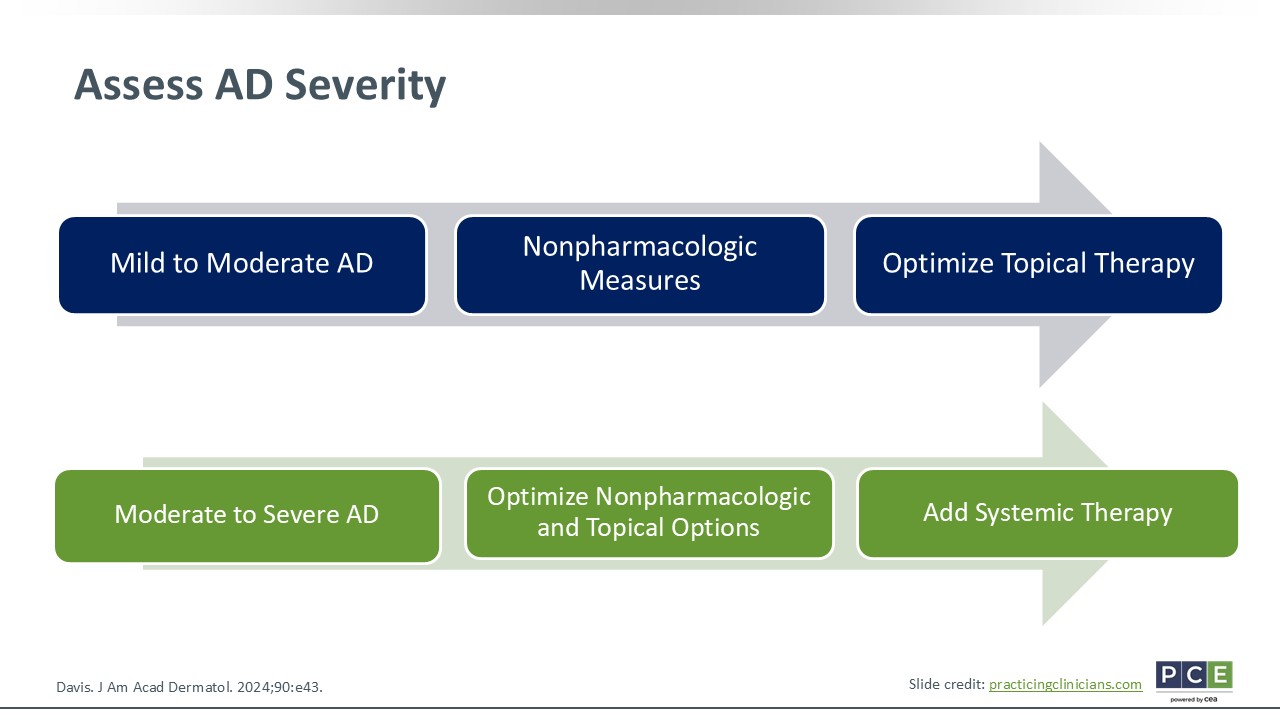
To determine which treatment will likely work best for patients, HCPs first must assess the severity of patients’ AD. You can use normalized instruments to determine if the AD is mild, moderate, or severe.
For those with mild to moderate AD, HCPs should always start with nonpharmacologic measures and ensure any topical therapies are optimized. For moderate to severe AD, HCPs can still use nonpharmacologic measures and optimize topical therapy, but these patients are going to start thinking about adding a systemic therapy.15
Candidates for Systemic Therapy for AD
Joy Wan, MD, MSCE:
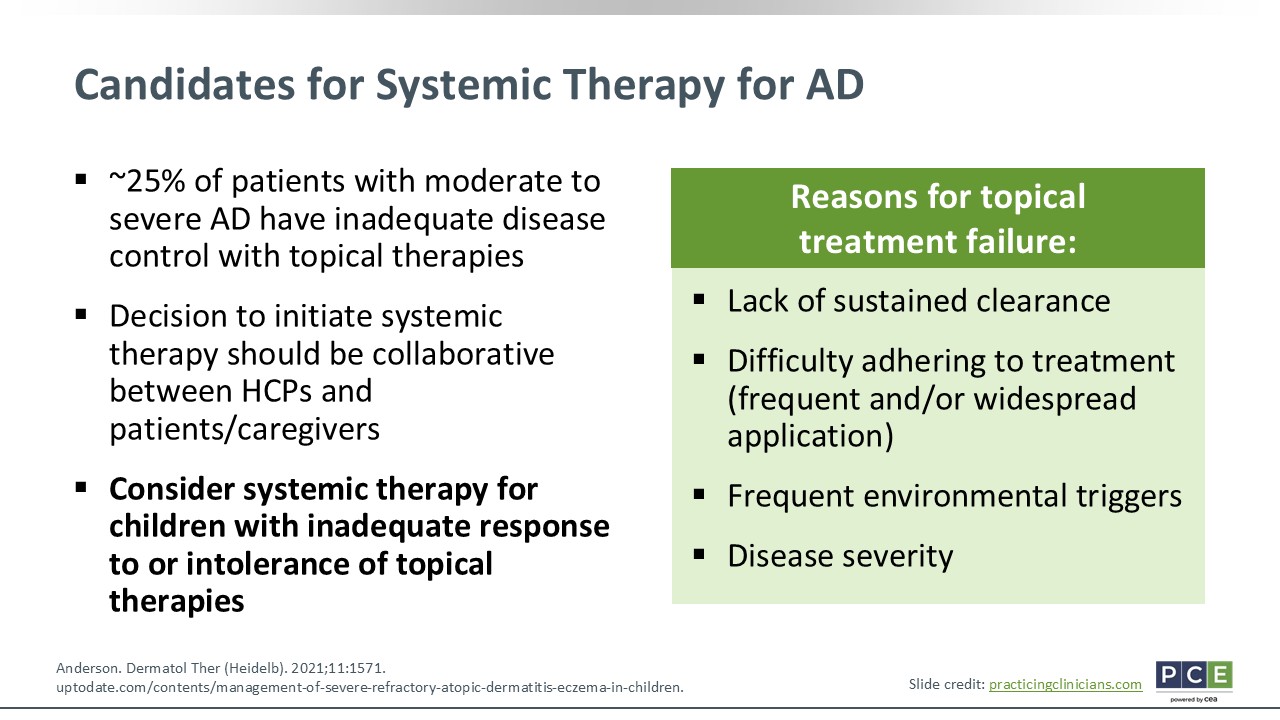
Approximately one quarter of patients with moderate to severe AD have inadequate disease control with topical therapies. So HCPs should start conversations early with patients for whom you think are moving toward the need for systemic therapy. Some of the reasons for which topical treatments fail patients is they do not keep patients’ skin clear after working for a week or 2. Another potential reason for treatment failure is centered on adherence. I hear from families that topical therapies require too much to apply twice daily to a large area of the body. It is hard to keep up with and if they cannot practically use these topicals, that makes response hard to follow. For some children, they experience environmental triggers that exacerbate things. Despite using topical therapies, it may add fuel to the fire. And we have already discussed disease severity, which is a very real reason why some topical therapies fail patients.
These points illustrate why it is critical to start these conversations early. Take a collaborative approach with your patients and their families. Consider systemic therapies for children with AD who cannot tolerate or who have inadequate response to topical therapies.24,25
Systemic Therapy Considerations
Joy Wan, MD, MSCE:
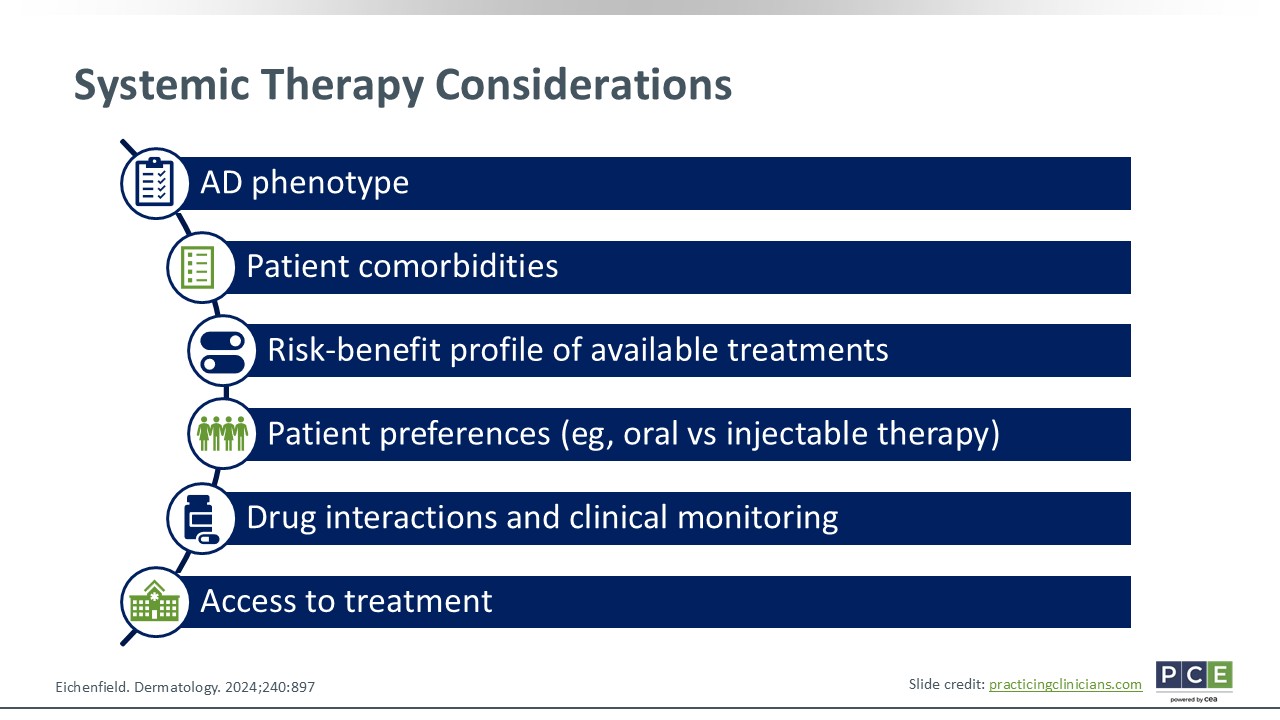
Things to consider when deciding if patients should start systemic therapy include the clinical phenotype of their AD—how severe it is and what areas of the body it is affecting. HCPs also should consider patients’ comorbidities. Some of these systemic therapies also have FDA approval for other indications (eg, asthma or inflammatory bowel disease). Therefore, you might be able to kill 2 or 3 birds with 1 stone, as they say, with the same systemic agent. Furthermore, HCPs should consider the risk–benefit profile of the available treatments and patient preferences (ie, oral vs injectable treatment). Depending on the age of the child and more, these things might be important. Finally, things like drug interactions, clinical monitoring, and accessibility are all important considerations.26
Biologic Targets
Joy Wan, MD, MSCE:
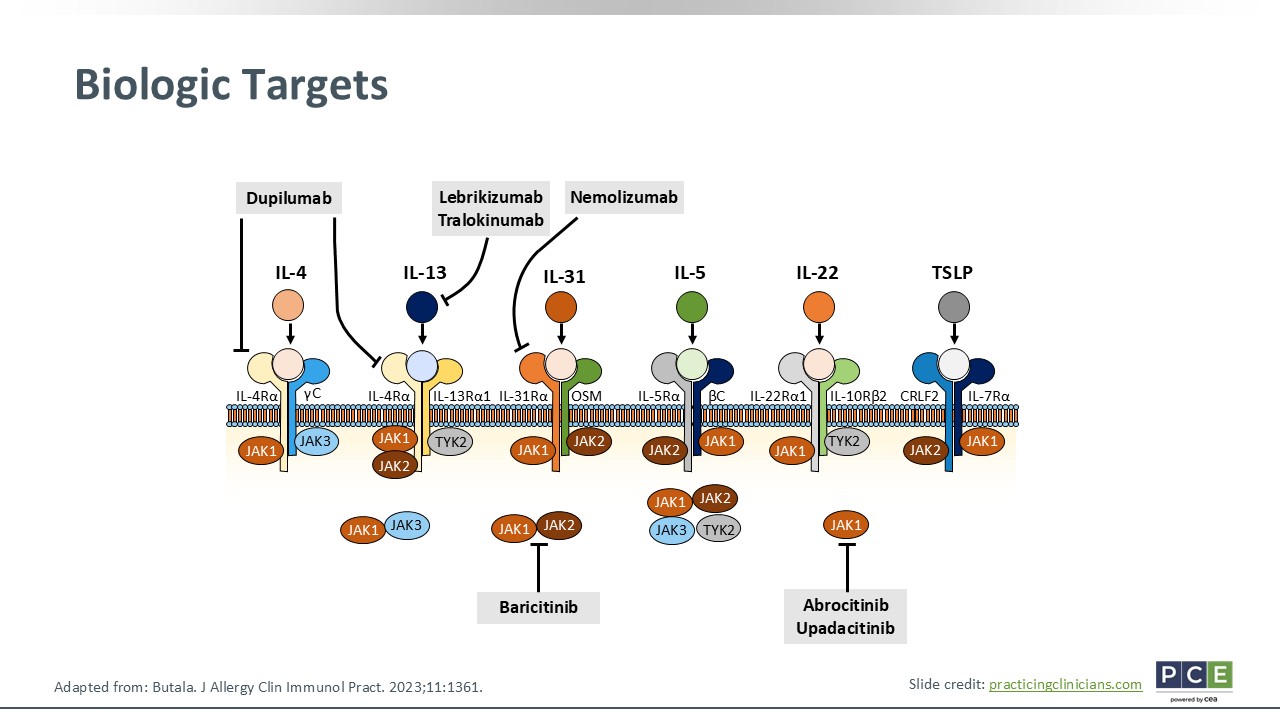
Now we have more sophisticated novel systemic therapies that target specific cytokines that are known to play a role in the pathogenesis of AD: Dupilumab is an IL-4 receptor alpha inhibitor, lebrikizumab and tralokinumab both are IL-13 inhibitors, and nemolizumab is an IL-31 inhibitor. For the oral JAK inhibitors, baricitinib blocks both JAK1 and JAK2, whereas abrocitinib and upadacitinib block JAK1.27
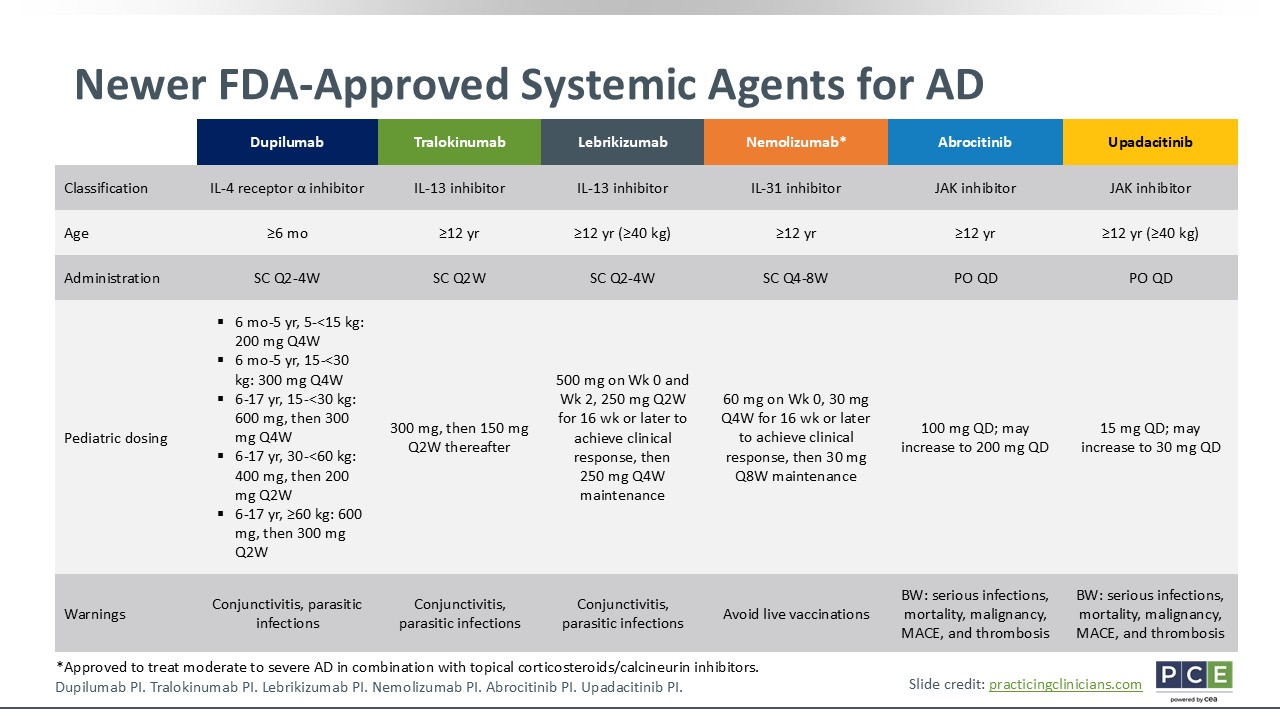
Newer FDA-Approved Systemic Agents for AD
Joy Wan, MD, MSCE:
I will note on this slide that dupilumab is the only biologic approved for use in patients as young as 6 months of age. All other biologics and the oral JAK inhibitors are approved for use in patients aged 12 years or older. In terms of the administration, biologics are subcutaneous injections and oral JAK inhibitors are not. The frequency of administration will vary depending on the particular biologic, but it can range anywhere between every 2-8 weeks. Oral JAK inhibitors are taken once daily.28-33
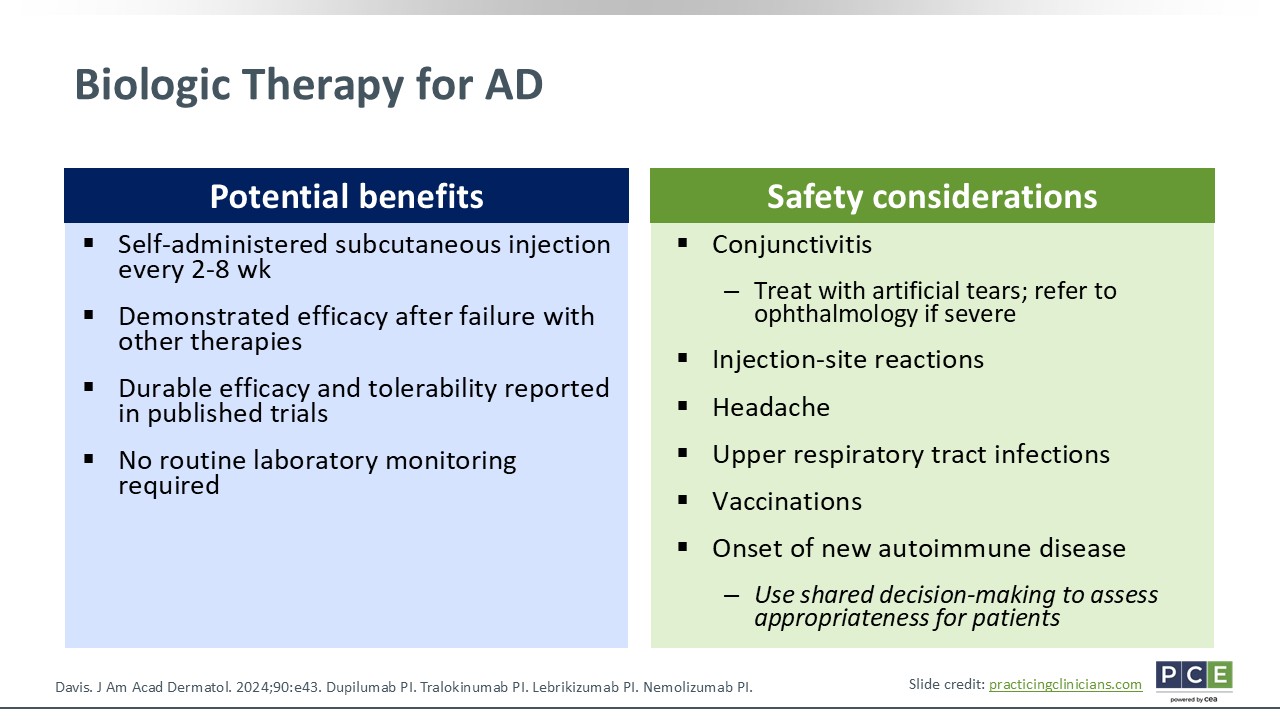
Biologic Therapy for AD
Joy Wan, MD, MSCE:
A benefit with biologic therapies includes self-administration. These are given at home by a caregiver who is trained to do it. Often, once patients start a biologic, they can work well and likely better than all the topicals they previously used. I hear that positive feedback a lot when I start my pediatric patients on biologics. The efficacy and tolerability with these agents are quite durable. Because the first biologic for AD was approved in 2017 for adults, we have relatively long-term data on it. As we accumulate that data on all agents, hopefully we will continue to see that durable efficacy and tolerability. Another nice thing about biologics is that there is no routine laboratory monitoring required.
In terms of safety, conjunctivitis is probably the most common adverse drug event observed with biologics. There are no predictive factors that we can rely on to tell families if their child might be at greater risk. When conjunctivitis happens, we certainly treat it appropriately. In severe cases, HCPs should refer patients to ophthalmology because patients might need medicated eye drops. Injection site reactions with biologics certainly are possible. Some other common adverse drug events are headache and upper respiratory tract infections.
A quick word regarding vaccinations: Live vaccinations should be avoided with the biologics and oral JAK inhibitors for AD. I think that things will evolve as more data on the safety of vaccinations become available. I think that there is movement toward using SDM with respect to determining if children can get some of their needed live vaccinations, even when they are receiving some of these agents.
Then finally, there are some case reports of new-onset of autoimmune disease with the use of these biologics. This is not a major thing that I counsel every single patient about, but it is something of which I am aware.15,28-31
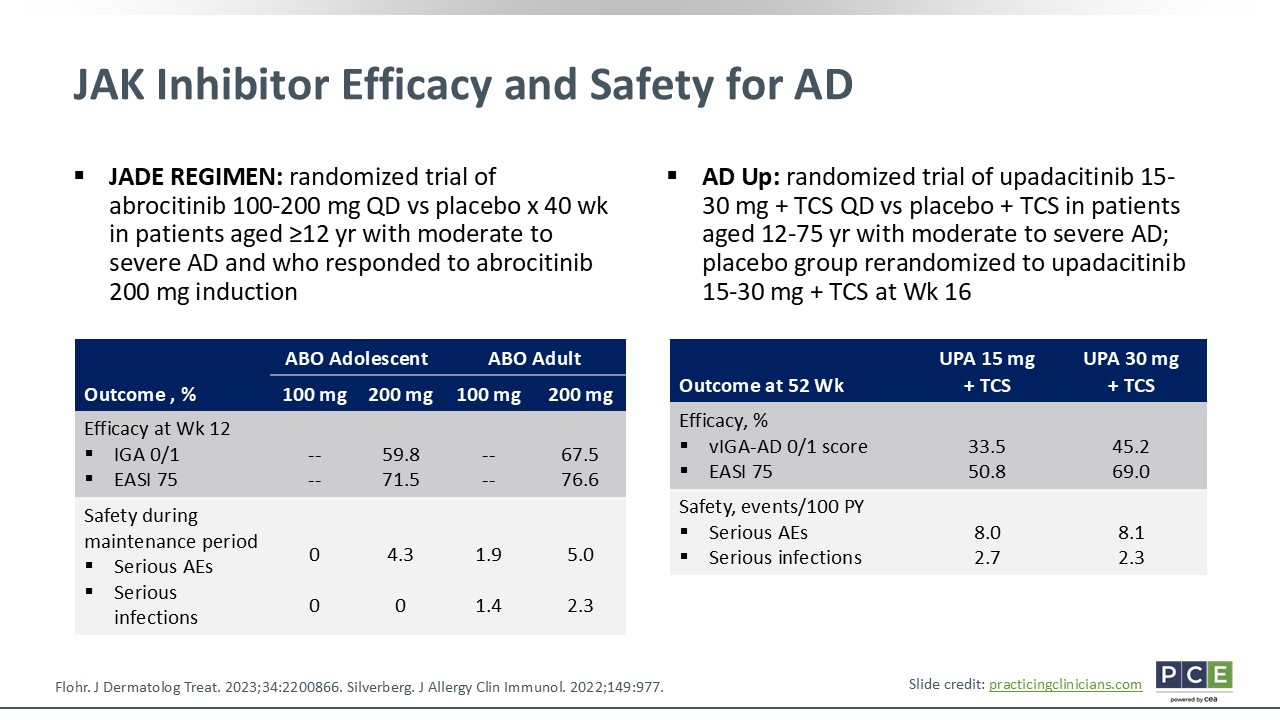
JAK Inhibitor Efficacy and Safety for AD
Joy Wan, MD, MSCE:
There have been randomized trials done with JAK inhibitors in adults and adolescents with AD. As highlighted on this slide, abrocitinib and upadacitinib have good efficacy across the board. However, there were reported adverse drug events, primarily infections, which is something that I counsel families about.34,35
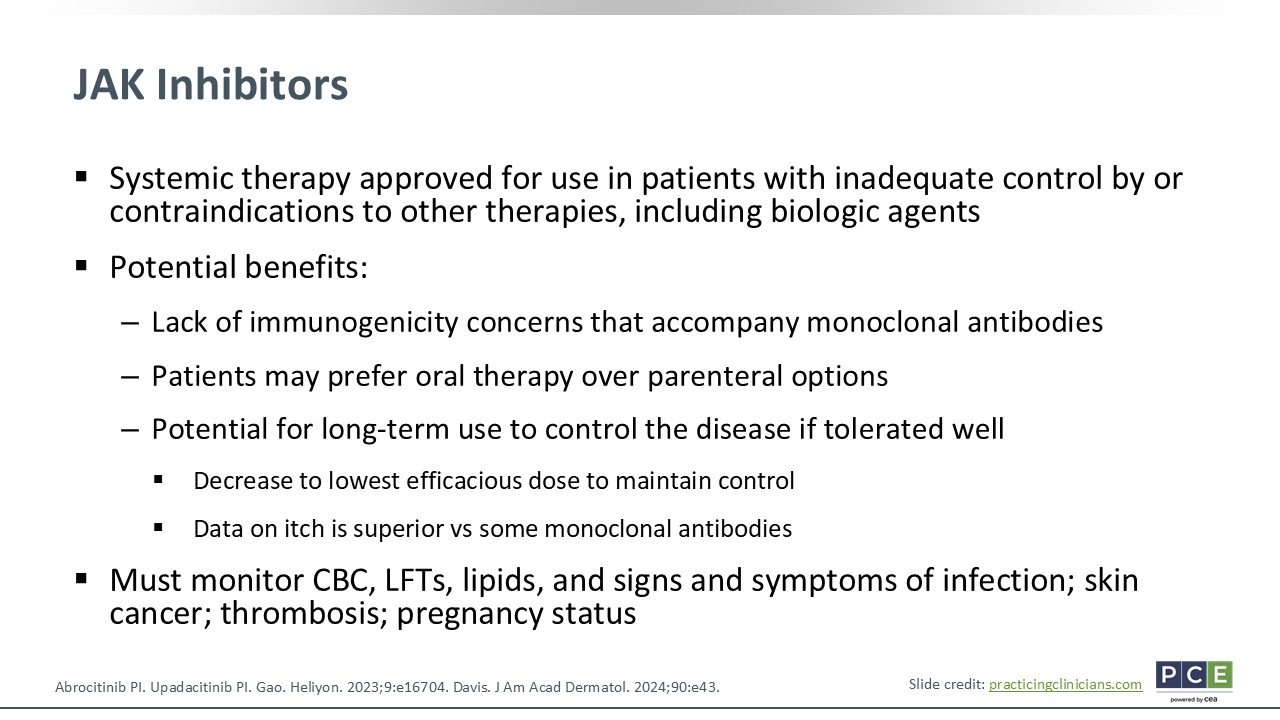
JAK Inhibitors
Joy Wan, MD, MSCE:
JAK inhibitors do not have that immunogenicity that occurs with monoclonal antibodies, so will not have antidrug antibodies. In addition, they may prefer oral therapy over injectable treatments, and JAK inhibitors have a couple of dosing options. It is recommended that if patients respond well, they can move to the lower dose to maintain disease control. There also is some suggestion that itch response may be better with JAK inhibitors than biologics.
That said, JAK inhibitors require active lab monitoring with complete blood count, liver function test, lipid panel, and monitoring for the signs/symptoms of infection. Then there is a black box warning with these agents because some of the safety signals that came out with this class of agents years ago in studies. All JAK inhibitors have this black box warning. Right now, that warning concerns risk of cancer, thrombosis, infection, and major cardiovascular events. So these are things of which HCPs must be aware. Yet long-term safety data are needed to determine if these warnings are necessary in generally healthy children with AD who use these therapies.15,32,33,36,37
Emerging Therapeutic Agents
Joy Wan, MD, MSCE:
There are some emerging therapeutics, as this is a quickly evolving field. Here are 4, including baricitinib which in is not yet approved in the United States. The other emerging agents are amlitelimab and rocatinlimab (OX40 ligand inhibitors) and etrasimod (an S1P receptor modulator).38-41. I think that this list will continue to expand over time, too.
Patient Case: 10-Year-Old Girl With AD That Is Not Well Controlled With TCS
Joy Wan, MD, MSCE:
Moving on to a patient case: A 10-year-old girl with AD that is not well controlled with TCS presents to your office. She has very dry, itchy skin. She has some pustules. She also reports that she gets horrible sleep, which significantly affects her and her family members’ quality of life. The patient has allergic rhinitis and some mild asthma as comorbidities. She has tried many different topicals, primarily TCS and antihistamines, bleach baths, and more.
Upon examination, you find that there are additional areas of involvement. This is affecting nearly 80% of the patient’s body surface area. She has an IGA score of 4, which is severe. Her EASI score is 35.7, which is also puts her in the severe category. How will you discuss other treatment options with her?
In this case, I think it is important for this patient and her family to understand that she has already tried many topical therapies. She has a horrible quality of life; her disease is severe. So we should be discussing systemic therapy or phototherapy by going through the risks and benefits of those options.
Of note, the patient is 10 years of age. Therefore, some of the systemic agents may not have FDA approval for her at this age. I would start the conversation by talking about the need for treatment escalation and introducing an agent like dupilumab given her age. That biologic is approved by the FDA for a 10-year-old patient with moderate to severe AD. We could also discuss phototherapy by going through, again, the details of the risks and benefits associated with that treatment option.