CE / CME
From Flare to Control in Atopic Dermatitis: Improving Outcomes in Pediatric Patients With Moderate to Severe Disease
Nurse Practitioners/Nurses: 1.00 Nursing contact hours, includes 1.00 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Released: June 27, 2025
Expiration: June 26, 2026


Activity
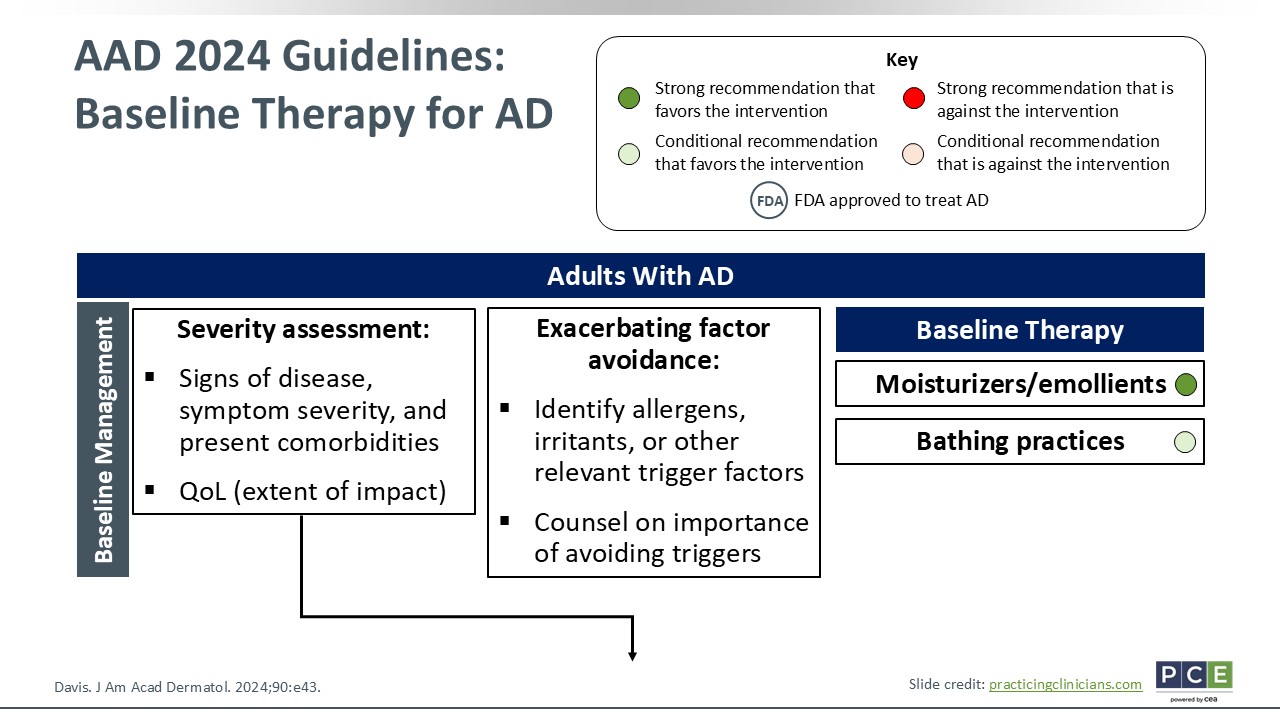
AAD 2024 Guidelines: Baseline Therapy for AD
Joy Wan, MD, MSCE:
We will start by reviewing 2024 updated guidelines for AD treatment, put forth by the American Academy of Dermatology (AAD). Now, I will preface this by stating that most of these guidelines are geared toward treating the adult population. The AAD is working on putting together pediatric treatment guidelines for AD, too, and that hopefully will come soon.
A lot of the same principles apply, whether we are talking about adults or children. We have already discussed how to assess severity, consider quality of life, and avoid particular allergens, irritants, or other triggers. Some individuals may have relevant triggers, so identifying those and avoiding them is critical.
Starting from the top, baseline management for all patients who present with AD, whether mild to severe, should be counseling about using moisturizers and emollients daily by incorporating them into their skin care regimen. Then HCPs should review bathing practices, which might include lukewarm baths, short showers, moisturizing immediately after bathing, using fragrance-free products to wash the skin and moisturize.15
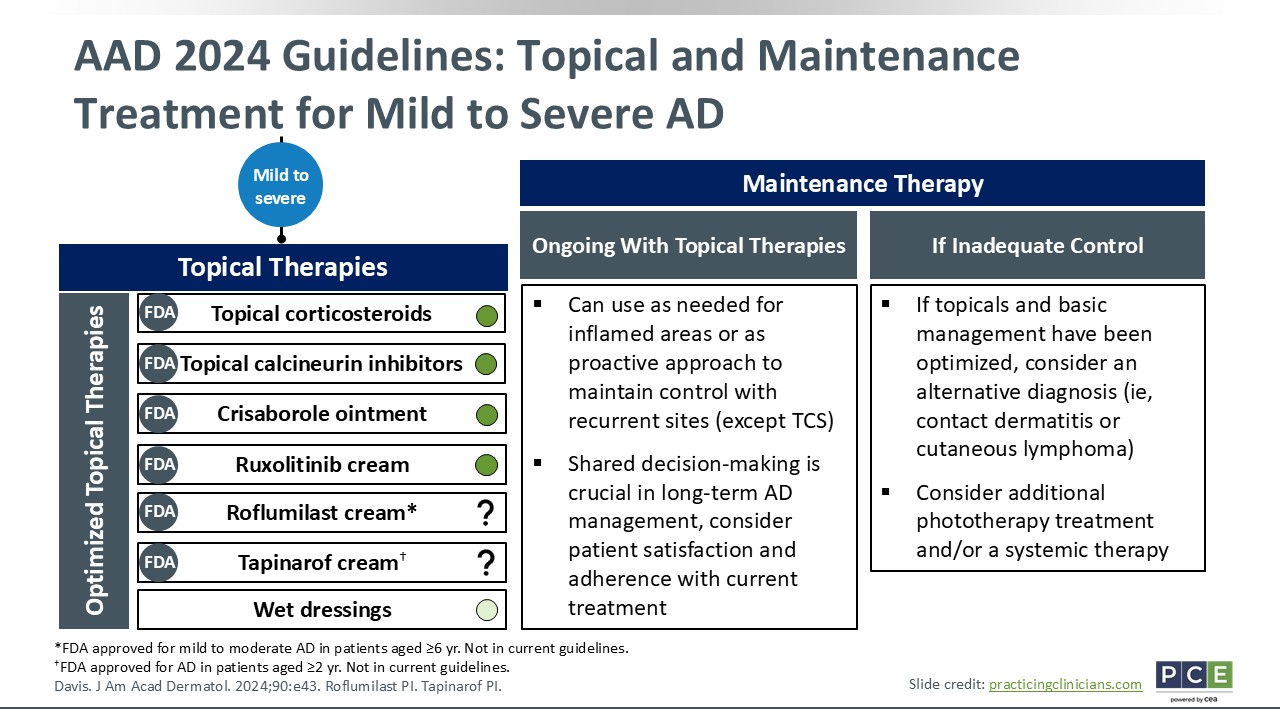
AAD 2024 Guidelines: Topical and Maintenance Treatment for Mild to Severe AD
Joy Wan, MD, MSCE:
Often HCPs are going to see patients, who despite all these baseline measures, still need something more. As I move into discussing the topical therapies for AD, these are treatments are appropriate for patients with mild to severe disease. First, I will talk a little bit about the art of treatment selection and use for AD. To quickly run through some of the topical therapies at our disposal, we have:
- Topical corticosteroids (TCS)
- Topical calcineurin inhibitors (TCIs)
- Crisaborole ointment
- Ruxolitinib cream
- Roflumilast cream
- Tapinarof cream
The treatments with the little green circle are all recommended in the AAD guidelines. Of note, roflumilast and tapinarof cream have received FDA approval to treat AD in specific patient populations, but they are not included in the 2024 guidelines. The question marks indicate that this is an evolving treatment landscape and it is not clear yet how strongly these agents are or are not recommended. But we have more and more topicals at our disposal now.
Then wet dressings are something that I have patients use in conjunction with their other topical therapies. This can include a modified wet wrap where patients apply their emollients or pharmacologic topical therapies and then apply a damp layer that could include a tight cotton pajama onesie, followed by an outer second layer that is dry. That essentially seals in the medicine and intensifies the emollients and/or pharmacologic topical therapies that patients are using.
In terms of topicals and how to use them, I often tell patients to use them as needed. When their AD is inflamed, I will tell them to apply their topical therapies for “X” amount of time. It might be twice daily for a week or 2, depending on what body area is affected and what strength of medicine is being used. That is a reactive approach to treatment. Another way that patients can use topical therapies is in a more proactive approach. Once patients have gotten a flare to calm down, they can use their topicals to maintain disease control. It also hopefully helps prevent the frequent flare-ups that some patients experience.
With any therapy, it is important to engage your patients in SDM. Talk with them about treatment adherence because this is one of the biggest challenges patients face. Also counsel them on potential adverse drug event and the like. If patients have inadequate control with their topicals, HCPs should step back and ask themselves if they have the correct diagnosis. Is this really AD or perhaps it is something else? If it is AD, this is when HCPs should begin considering escalation to other forms of therapy.15
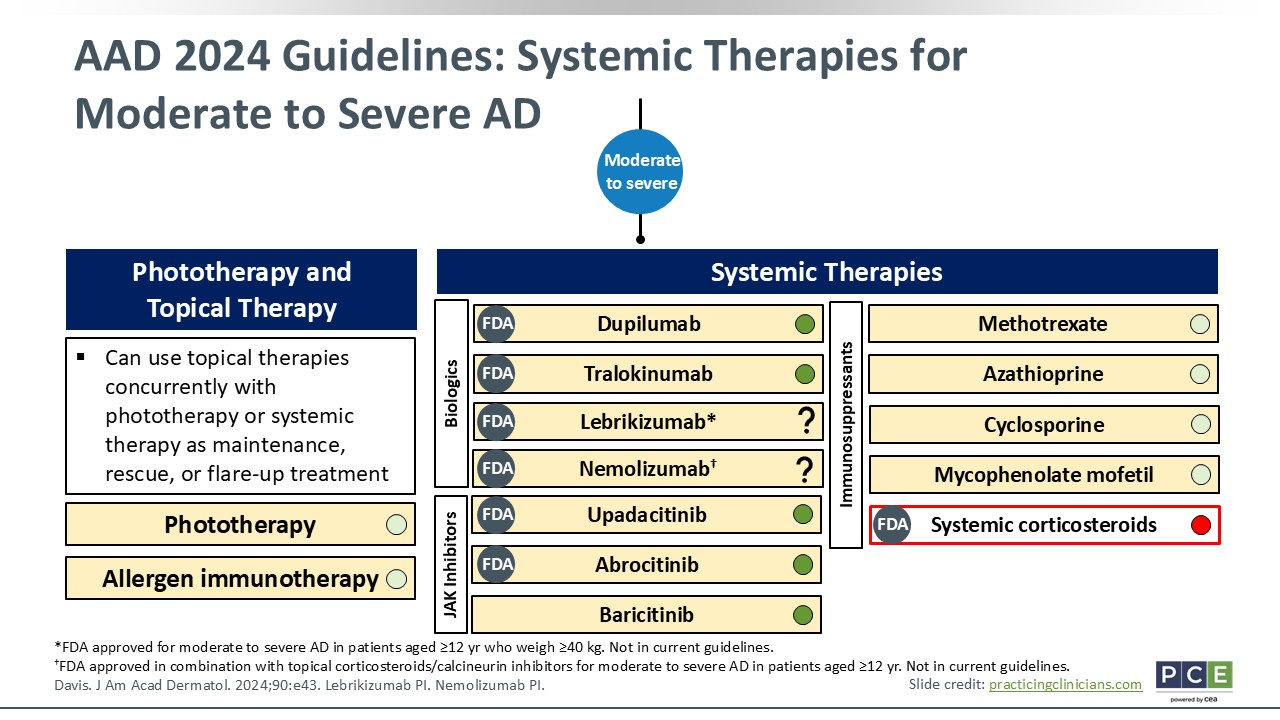
AAD 2024 Guidelines: Systemic Therapies for Moderate to Severe AD
Joy Wan, MD, MSCE:
Moving down the treatment algorithm, we have phototherapy and systemic therapies for moderate to severe AD that is not responsive to topical therapies. A quick word about phototherapy: It is usually done with ultraviolet B rays and sometimes ultraviolet A rays. This, in most cases, is given in the hospital setting, so patients need to be able to access it. You can use phototherapy concomitant with topical or systemic therapies. You also can consider allergen immunotherapy, especially in cases where allergens are thought to be directly relevant to patients’ AD flare-ups. But I do not recommend allergen immunotherapy for any allergen test that comes back positive for children with AD. There can be false positives.
We have an increasing number systemic therapies at our disposal. Previously, we only had what is shown on the far right of the slide: broad immunosuppressive therapies like methotrexate, azathioprine, cyclosporine, and mycophenolate. Because these agents are broadly immunosuppressive, they are not targeted specifically for AD. That is all that we had at the time and we relied on these therapies for our pediatrics who needed systemic therapy.
A quick word about systemic corticosteroids: Although they have received FDA approval to treat AD, you can see on the slide that there is a big red dot next to it because the guidelines dissuade the use of systemic corticosteroids for the long-term management of AD. In rare situations, HCPs might use it for a short period of time, often as a bridge to other long-term systemic therapies. But that is a rare situation. Yes, systemic corticosteroids definitely would help AD in the short run, but it really will not help in the long run. It comes with a lot of potential adverse drug events and can lead to worsening or flare-ups of AD after discontinuation.
Today, we have several novel systemic therapies at our disposal. The biologic therapies include dupilumab, tralokinumab, lebrikizumab, and nemolizumab. These have all been approved by the FDA to treat moderate to severe AD, but note that lebrikizumab and nemolizumab were approved after the 2024 guidelines were published. They have question marks because we do not yet know what degree of recommendation the AAD would put forth for these 2 agents. That being said, in my mind, the biologics are all available, are approved by the FDA, and are options at your disposal. Then we have 3 oral JAK inhibitors, including upadacitinib and abrocitinib, which are the 2 FDA-approved options for AD in the United States. Baricitinib is approved for treating AD in Europe. All 3 are small molecule inhibitors that have proven efficacy in AD treatment.15
Available Topical Therapies
Joy Wan, MD, MSCE:
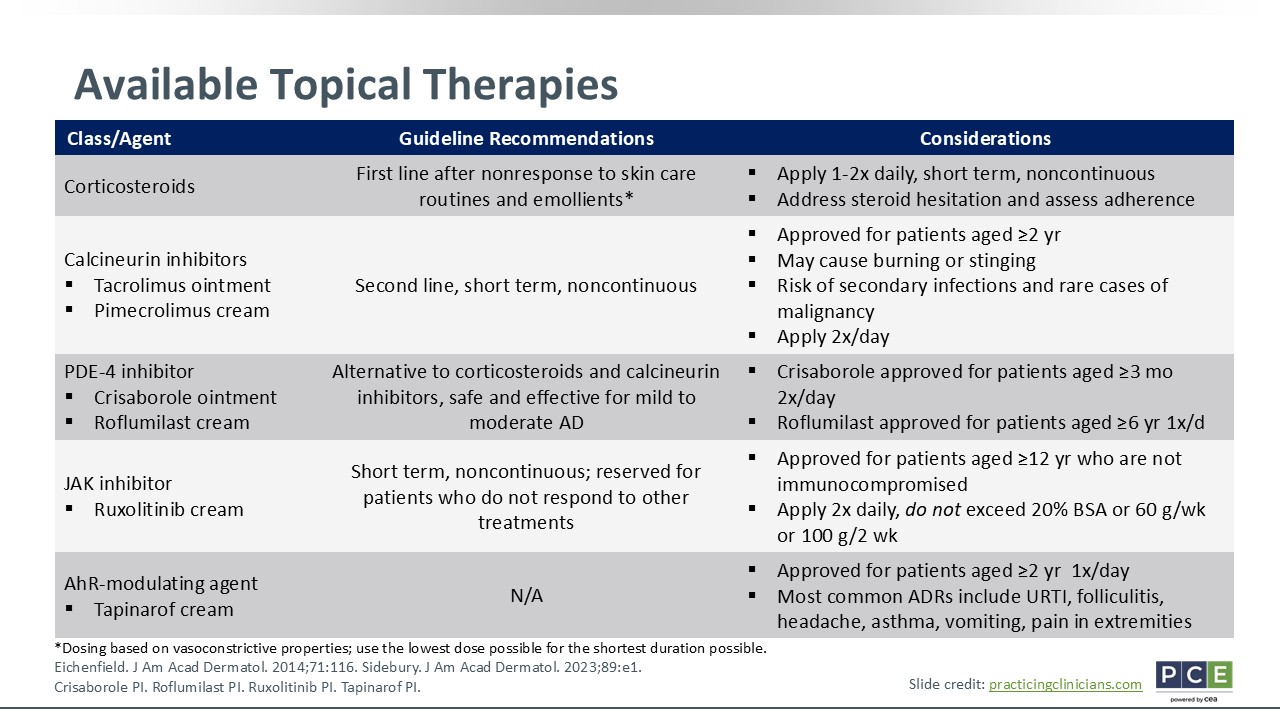
I covered some of these in the previous AAD guidelines treatment algorithm. In terms of the available topical therapies, I like to use TCS in the first-line setting, particularly for acute flares, because they tend to work pretty quickly. Now, HCPs cannot let patients use TCS continuously for weeks or months on end; we must allow patients to take breaks. That is where the bottom 4 categories of nonsteroidal topical therapies become useful.
Our TCI options include tacrolimus ointment and pimecrolimus cream. I like to use these as a maintenance therapy for disease control after using TCS for an acute flare. TCIs are helpful for mild flares, too, for some patients. What is nice about nonsteroidal topical therapies is that they can be used anywhere on the body, whereas we must be careful about potency and affected areas with using TCS. And patients should not use too potent TCS on sensitive areas, such as the face or groin.
In terms of other available nonsteroidal topical therapies, there are phosphodiesterase-4 inhibitors. Two of these are now available: crisaborole ointment and roflumilast cream. They are approved for use in patients at different ages. Crisaborole ointment is approved for patients as young as 3 months of age and roflumilast cream is approved for patients as young as 6 years of age. Crisaborole ointment is a useful nonsteroidal topical, especially for the infant/toddler age group. Roflumilast cream is only meant to be applied once daily so some families may prefer this treatment.16,17 The topical JAK inhibitor ruxolitinib cream is only approved for use among patients 12 years of age or older and who are not immunocompromised. HCPs might feel limited in terms of what age group they can use this therapy. Of note, there also are limits on how much of this agent patients can use in a week's time or what percentage of the body surface area they can apply it. Again, this is because of concerns of immunosuppression from the systemic versions of these types of JAK inhibitors.18 Finally and most recently approved, we have tapinarof cream, which is an aryl hydrocarbon receptor modulating agent. This is approved for use in patients as young as 2 years of age.18-20
Financial Burden of Topical Therapy
Joy Wan, MD, MSCE:
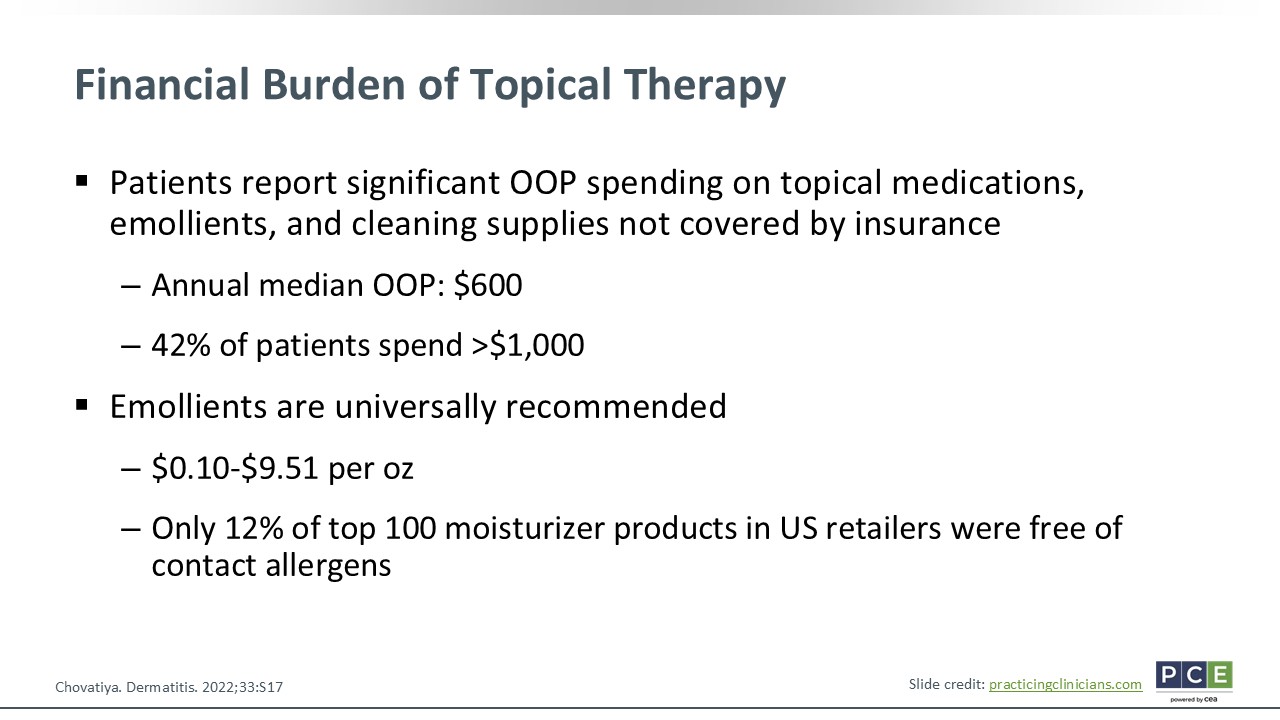
Topical therapies are expensive. Furthermore, a lot of the over-the-counter topicals like emollients are not covered by insurance. There are reports showing that the annual median out-of-pocket costs for these topical therapies is approximately $600 for patients. Then 42% of patients spend more than $1,000 to pay for these treatments.
That being said, emollients are universally recommended. They are a baseline treatment that we recommend for all patients with AD. The different emollients and their brands are going to vary in affordability. I find it helpful to tell families not one particular brand works best; rather, it is a little bit of trial and error. Regardless, I want patients to use something very thick, either a cream or an ointment. That is the main thing that I care about. I do not care what brand. I just want patients to find something that is affordable and works for them. Another thing to note is that may moisturizer products in the United States have other ingredients and/or allergens in them that can worsen patients’ AD. So HCPs must be mindful of some of these things.21 It comes as no surprise when patients tell us that they tried a moisturizer that ended up making their AD worse or just does not help much. That is why I encourage all my patients that it can be a process of trial and error.
Safety Concerns With Topical Corticosteroids
Joy Wan, MD, MSCE:
We use TCS a lot and are often concerned about the potential adverse drug events with families who are not using these agents appropriately. These ADRs are quite rare, especially if patients are using the correct potency for the correct area of the body or percentage of body surface area. HCPs should counsel families about this. I often tell them to apply TCS for no more than 14 days if the affected area is on the body or for no more than 7 days if the affected area is on the face. Those are rough estimates, and there is a little bit of leeway.
Ensure that you counsel patients regarding the potential ADRs if they were to use it inappropriately for too long. I usually recommend that they apply it twice daily, but some studies have shown that once daily application is still better than nothing. That schedule might be considered for some families because life gets in the way and it is hard to keep up treatment.22,23
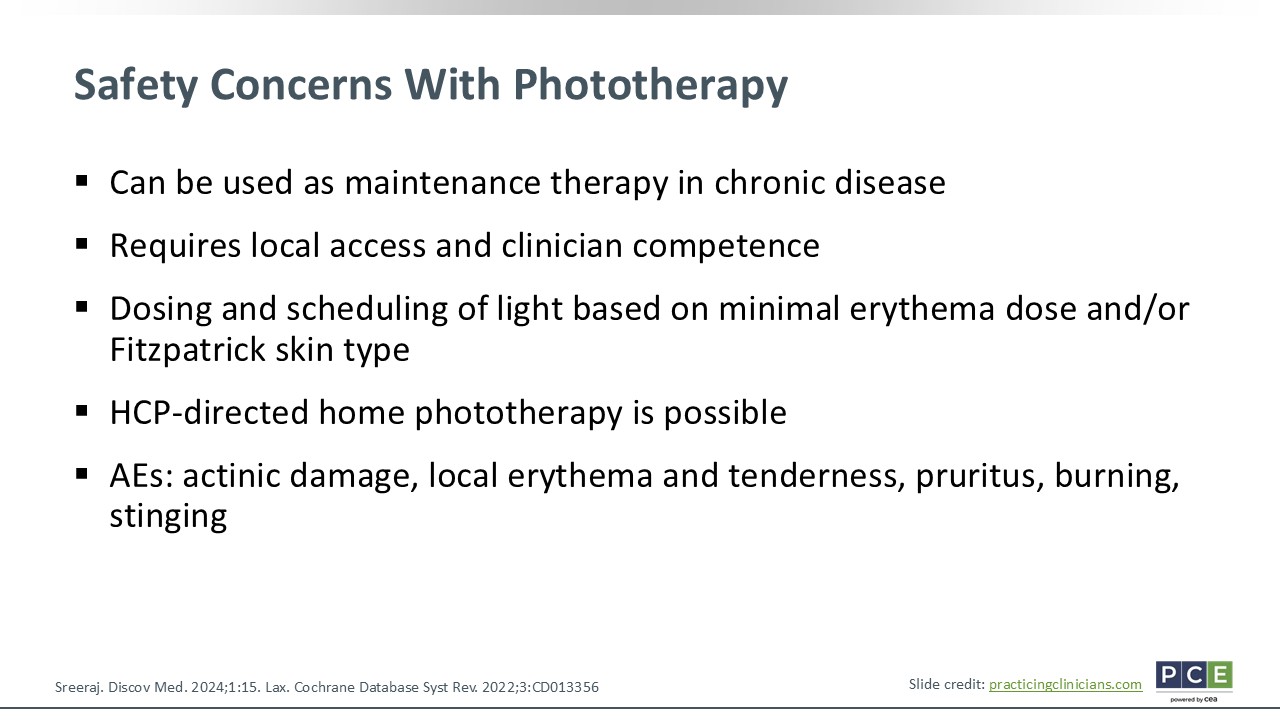
Safety Concerns With Phototherapy
Joy Wan, MD, MSCE:
With phototherapy, there are some safety concerns of which to be mindful. Again, patients need to have access to this treatment, so they need to be able to travel to the facility that offers phototherapy. Home phototherapy is possible in some situations, but health insurance coverage is all over the place. In addition, to purchase the machine is an out-of-pocket cost and can be quite expensive.
In terms of how phototherapy is done, it usually is based on patients’ Fitzpatrick skin type or minimal erythema dosing. It will start at a certain dose and then escalate to a degree where they are seeing an effect and achieving clearance. Sometimes phototherapy can be used as maintenance every so often to keep patients’ skin clear. The main adverse drug events with phototherapy include sun damage, localized burning, tenderness, erythema, and itch. HCPs should minimize this by selecting the appropriate dosing and escalation for patients.22,23