CE / CME
DeLIVERing Prevention: Optimizing Uptake of Hepatitis A and B Vaccination
Pharmacists: 1.00 contact hour (0.1 CEUs)
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Released: June 03, 2026
Expiration: June 02, 2027



Activity
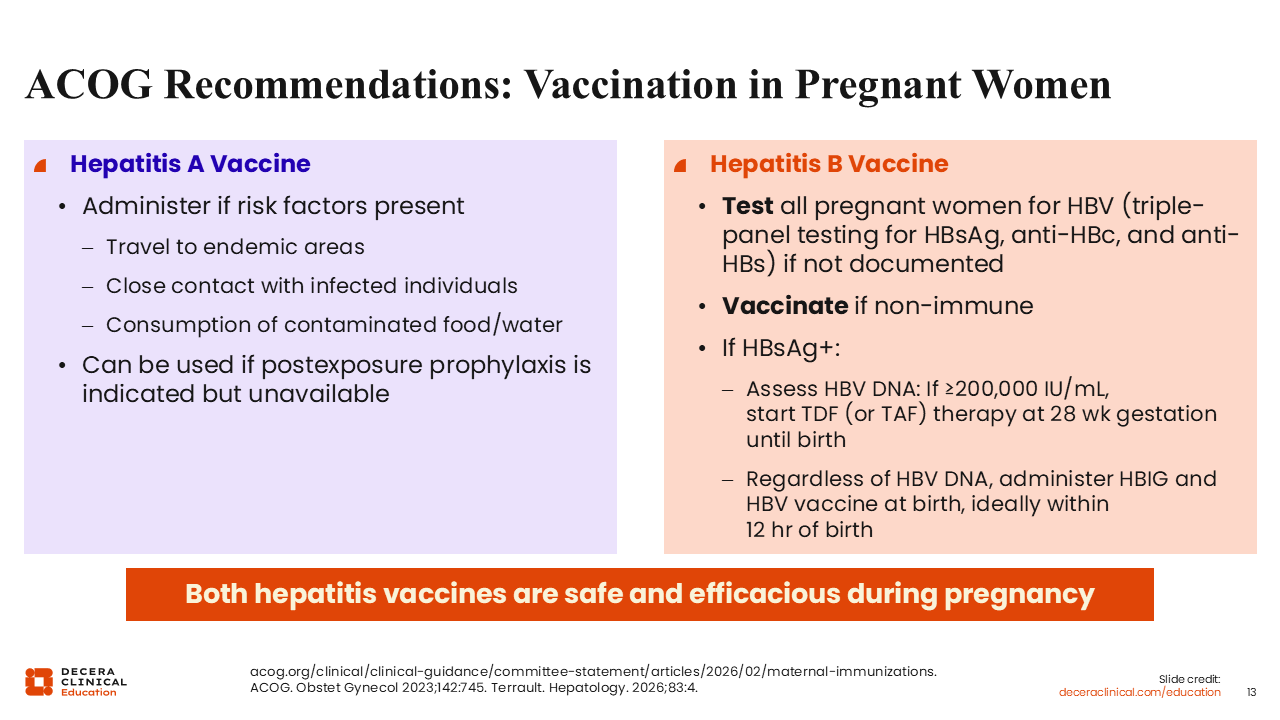
ACOG Recommendations: Vaccination in Pregnant Women
Su Wang, MD, MPH, FACP:
Let’s begin with vaccination recommendations during pregnancy from the American College of Obstetricians and Gynecologists.
For HAV, vaccination is recommended for pregnant women who have risk factors, including travel to endemic areas, close contact with infected individuals, or exposure to contaminated food or water. The vaccine may also be used if postexposure prophylaxis is indicated but unavailable.21
For hepatitis B, all pregnant women should undergo HBV testing. Current CDC recommendations include triple-panel testing with HBsAg, hepatitis B core antibody (anti-HBc), and hepatitis B surface antibody (anti-HBs). Testing should occur during every pregnancy, even if testing was performed during a prior pregnancy.21-23
If a pregnant woman is found to be nonimmune to HBV, vaccination during pregnancy is appropriate. Both HAV and HBV vaccines are considered safe and effective during pregnancy.
For individuals who are HBsAg positive, HBV DNA levels should be assessed. If HBV DNA is ≥200,000 IU/mL, antiviral therapy with tenofovir disoproxil fumarate or tenofovir alafenamide should be initiated at approximately 28 weeks of gestation, according to the latest American Association for the Study of Liver Diseases guidance. Therapy may be discontinued after delivery or continued depending on clinical considerations.22,23
For infants born to women with HBV infection, hepatitis B immune globulin (HBIG) and HBV vaccination should be administered within 12 hours of birth.22,23
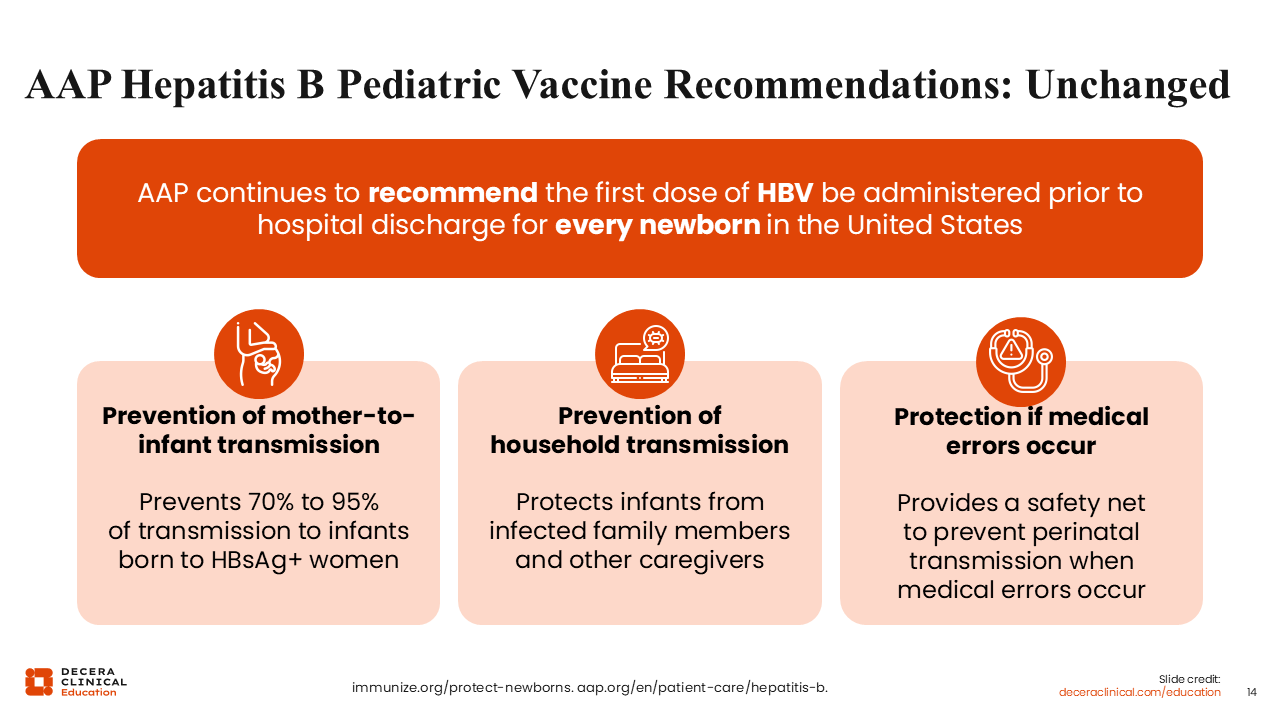
AAP Hepatitis B Pediatric Vaccine Recommendations: Unchanged
Su Wang, MD, MPH, FACP:
Although it seems like vaccine recommendations are constantly changing and evolving, the AAP continues to recommend that the first dose of HBV vaccine (often referred to as the birth dose) be administered within 24 hours of birth for every newborn in the United States.
The AAP has been recommending universal infant immunization against HBV since 1991. This has had a major impact on preventing mother-to-child transmission, reducing transmission to infants born to HBsAg-positive women by approximately 70% to 95%. Furthermore, universal newborn vaccination has had far-reaching effects on reducing the rate of acute HBV infection across the United States.24-27
The birth dose also helps prevent household transmission. Although maternal HBV status may be known, other household members or caregivers may not have been tested. Vaccination provides protection against exposure from infected caregivers or family members. In addition, the birth dose provides protection in the event of rare medical errors or other early exposures, including injection-related exposures.28
HBIG and Birth Dose Administration Based on Maternal HBsAg
Su Wang, MD, MPH, FACP:
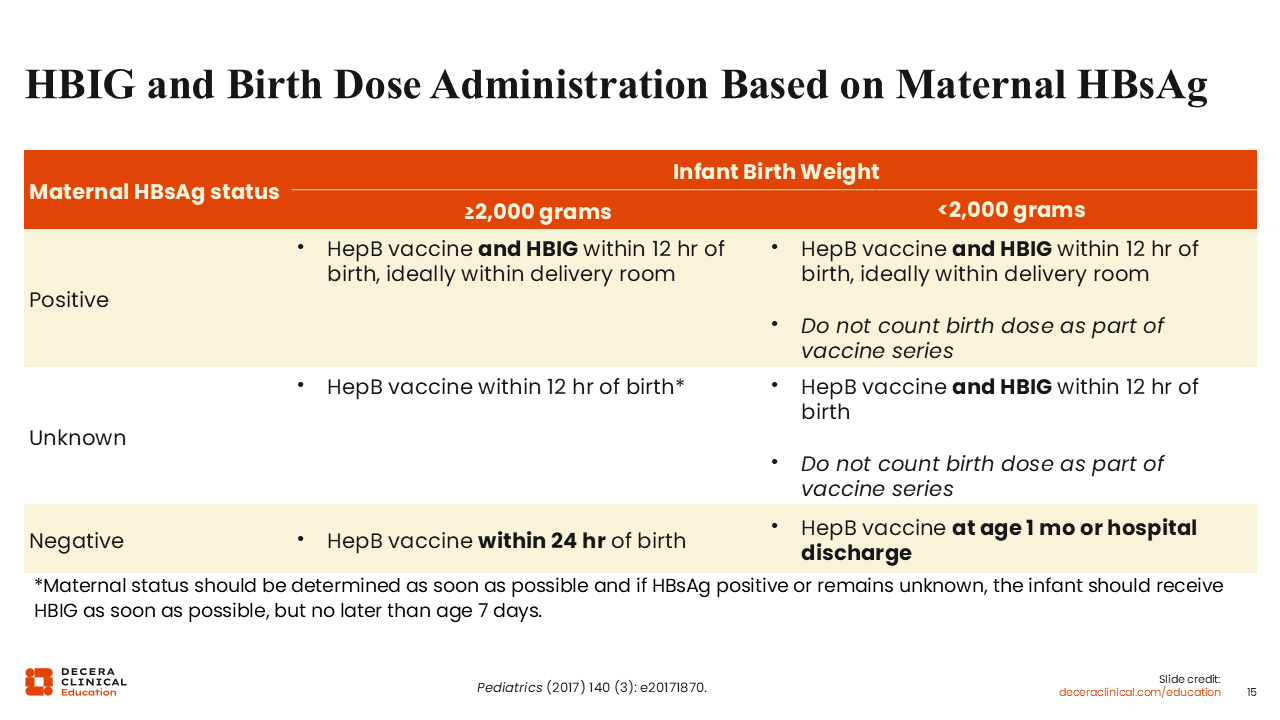
Let’s talk about the timing of the hepatitis B vaccine birth dose and when we give HBIG. When the mother has HBV infection or if her status is unknown, we need to give the HepB vaccine birth dose plus the HBIG within 12 hours. If the mother does not have hepatitis B based on her tests, then the birth dose of HepB vaccine can be given with 24 hours.22,23
HBIG provides passive protection that is immediate, whereas the vaccine requires time for the infant’s immune system to develop protective antibodies.28
The recommendations differ slightly depending on whether the infant weighs at least 2000 g. Infants weighing at least 2000 g should receive both HBV vaccine and HBIG within 12 hours of birth. For infants weighing <2000 g, the birth dose is not counted as part of the vaccine series, and additional doses are required.28
If maternal HBV status is unknown, infants should initially be managed as though the mother is infected until testing is completed.29
For infants born to HBsAg-negative mothers, HBV vaccination should still be administered within 24 hours of birth, and HBIG is not required.29
Pediatric Vaccine Recommendations: Hepatitis A
Su Wang, MD, MPH, FACP:
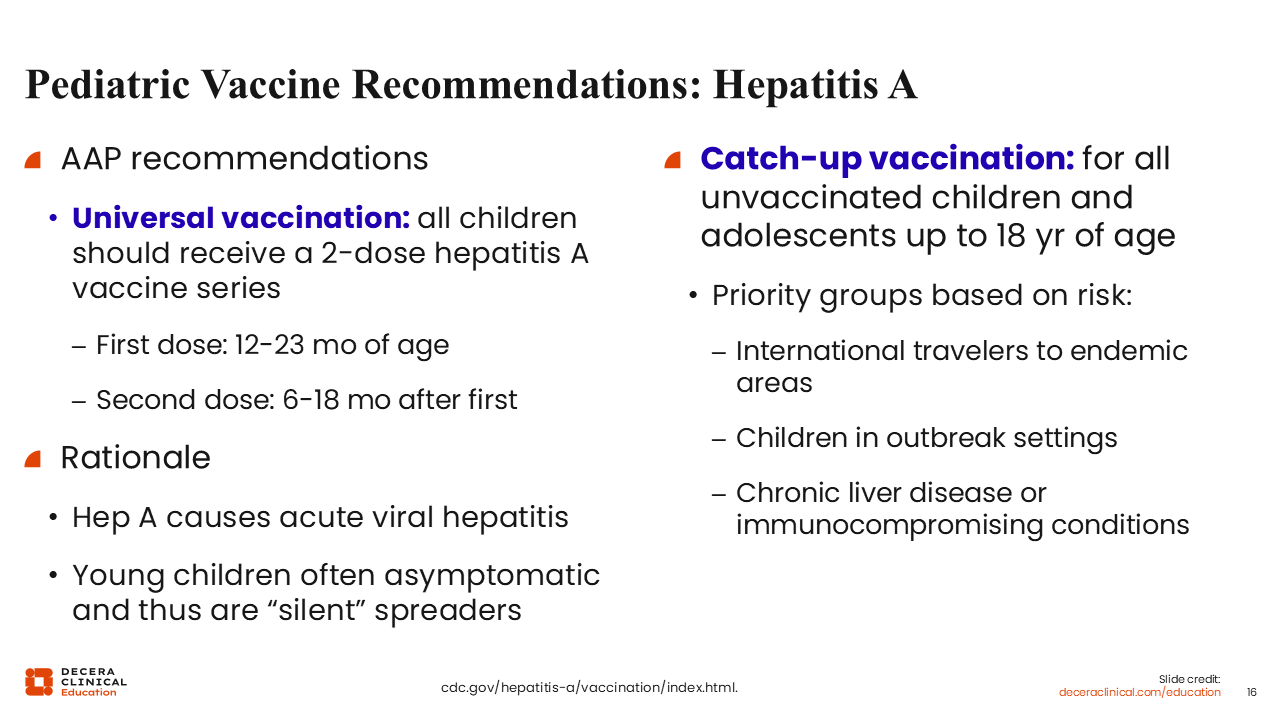
Turning now to HAV, the AAP likewise recommends universal HAV vaccination for children using a 2-dose series. The first dose should be administered between 12 and 23 months of age, and the second dose should be given 6-18 months later.25
HAV causes acute viral hepatitis, and young children are often asymptomatic. However, even asymptomatic children can transmit infection to adults, who may develop more severe disease. Vaccination, therefore, also helps prevent ongoing community transmission.30
For children and adolescents who were not vaccinated during infancy, catch-up vaccination is recommended through 18 years of age. Priority groups include international travelers, children in outbreak settings, and individuals with chronic liver disease or immunocompromising conditions.30
Childhood Vaccination: Shared Clinical Decision-making
Su Wang, MD, MPH, FACP:
In contrast to the AAP recommendations for universal, routine HAV and HBV immunization, federal recommendations shifted in 2026 from routine childhood immunization to immunization based on shared clinical decision-making.31
This term “shared clinical decision-making” has been coming up more and more lately. It emphasizes the importance of providing information on risks and benefits while creating opportunities for patients and families to ask questions. In many ways, healthcare professionals (HCPs) have already been incorporating these principles into routine practice by discussing risks, benefits, patient preferences, and individual clinical scenarios.32
One critical message from the AAP is that vaccines included under shared clinical decision-making remain important and that the underlying science has not changed.32
Conversations with Families: How to Navigate?
Su Wang, MD, MPH, FACP:
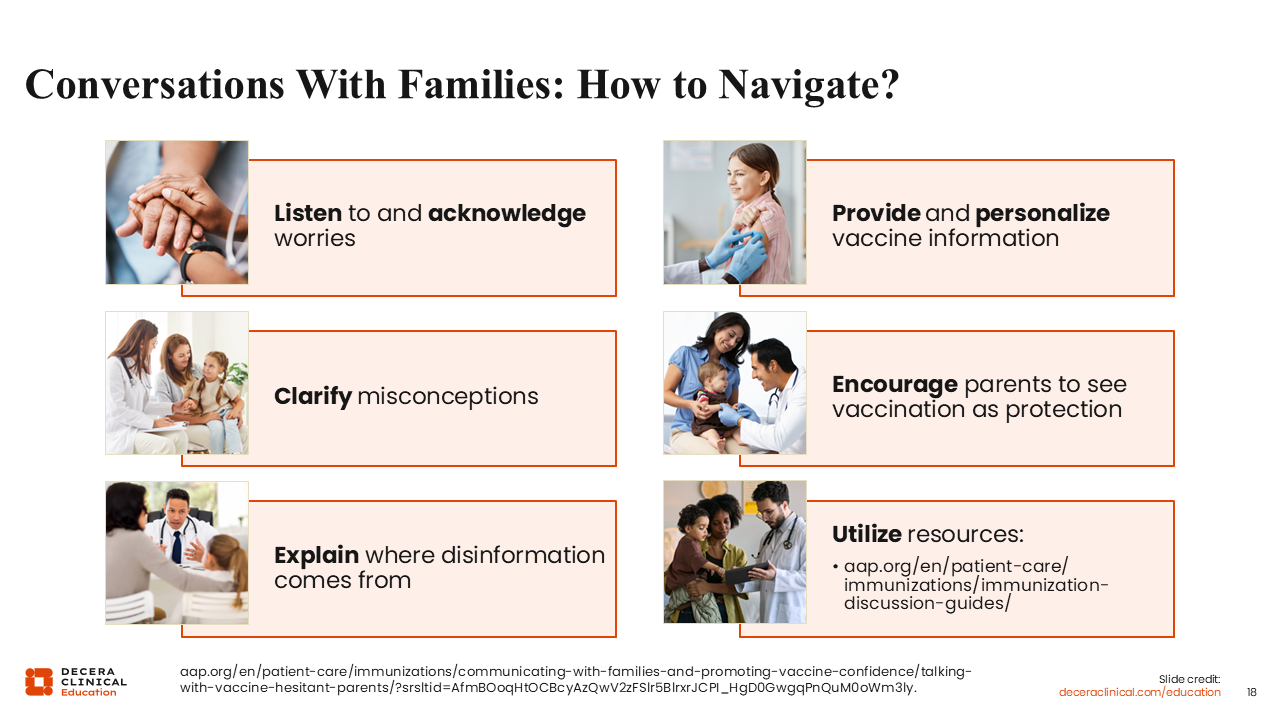
When navigating these conversations with families, it is important to listen to and acknowledge concerns, clarify misconceptions, and explain where misinformation may originate. It is also important to personalize vaccine information so families understand why vaccination is relevant to them and their children.
To me, shared decision-making means bringing patients into the conversation but it does not mean considering all options as being completely equal. The data shows that pediatric vaccinations are inarguably beneficial for preventing potentially devastating diseases and one of public healths’ greatest success to keep children healthy., Thus, the case for childhood vaccines are a much stronger recommendation than many interventions. With shared decision-making, we should show our patients that the evidence is clear that the benefits far exceed the risks for vaccination. Walking them through our decision making process and educating is a big part of making parents feel like they are part of the decision.
Vaccination should be framed as protection that helps children remain healthy and avoid serious illness. Providing educational resources can also be helpful when parents have questions. Organizations such as the AAP and the Hepatitis B Foundation offer great materials in multiple languages for patients and families.33
Jewel Mullen, MD, MPH, MPA, FACP:
I also want to emphasize that HCPs have always discussed these issues with patients and caregivers. Shared clinical decision-making should not be interpreted to mean that vaccines are less important. If these vaccines were not important, we would not be having this conversation.
At the same time, people value evidence-based guidance from their HCPs. Strong recommendations from HCPs often improve confidence in vaccination. Shared clinical decision-making is really about balancing patient autonomy with clear communication of evidence-based recommendations.
Paul Kwo, MD:
I agree. Shared clinical decision-making recommendations have been historically data-driven and carefully vetted. One example is HBV vaccination in adults older than 60 years, which also uses a shared decision-making framework. Patients and HCPs should understand that these recommendations are based on substantial evidence demonstrating reductions in morbidity and mortality associated with chronic liver disease.
Hepatitis Vaccine Recommendations: Adults
Su Wang, MD, MPH, FACP:
That is the perfect segue to adult vaccination recommendations for HAV and HBV.
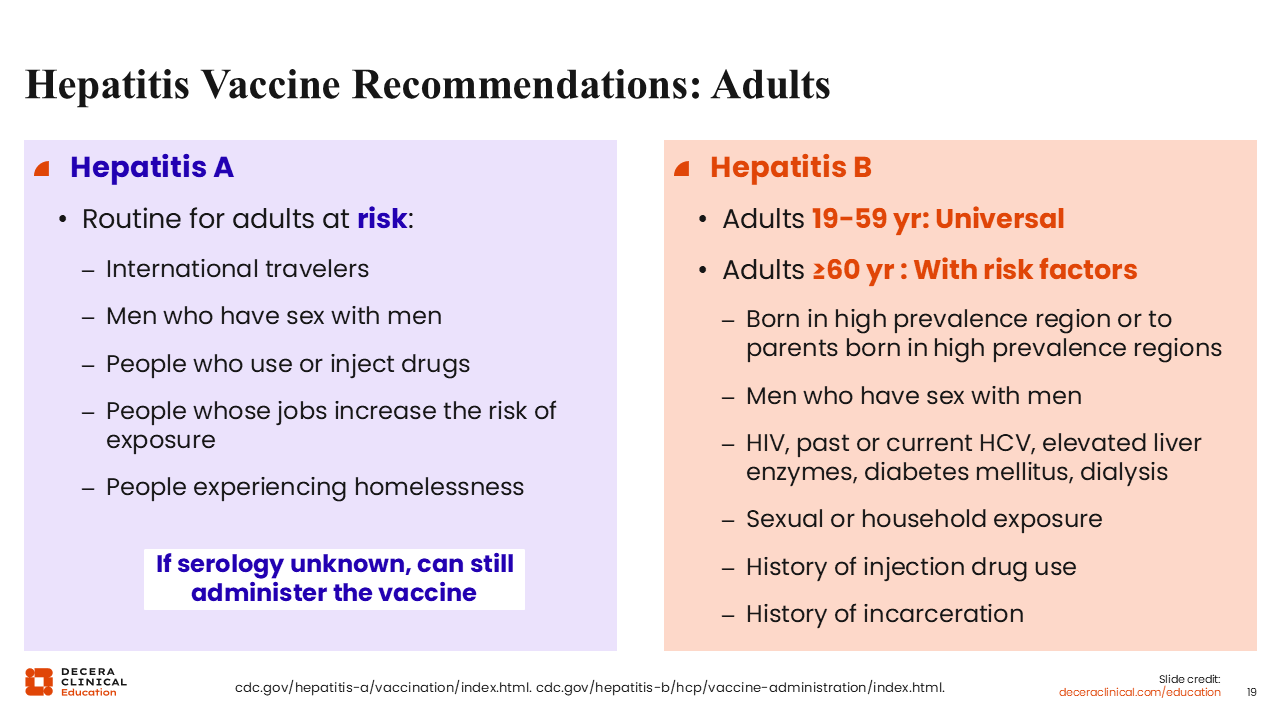
For HAV, vaccination is recommended for adults at risk, as listed on this slide.30 In my experience, a major challenge in practice is that patients often receive the first dose before travel and then forget to return for the second dose. We need to remind patients that the HAV vaccine is a 2-dose series. Even if the recommended interval has passed, patients should still return for completion of the series.
For HBV, recommendations have moved from risk based to universal HBV vaccination. In 2022, CDC started recommending hepatitis B vaccine for all adults aged 19-59 years. For adults aged 60 years or older, vaccination is recommended for those with risk factors. For those aged 60 years or older but without risk factors it may also be considered using shared clinical decision-making and if a patient requests to be vaccinated, that is sufficient reason alone.[cdc.gov/hepatitis-b/hcp/vaccine-administration/index.html.]
One point that stands out in the CDC recommendations is that for some high-risk populations, vaccination may proceed even without prior serologic testing (such as people with housing instability or with history of substance use).
So, putting this all together, for adults 19-59 years old, you should recommend the HBV vaccine because it is universally recommended at those ages, and you should recommend the HAV vaccine if they have risk factors such as international travel or unstable housing. You can do this even if their immune status is unknown.
Hepatitis A Vaccine Uptake in the United States
Su Wang, MD, MPH, FACP:
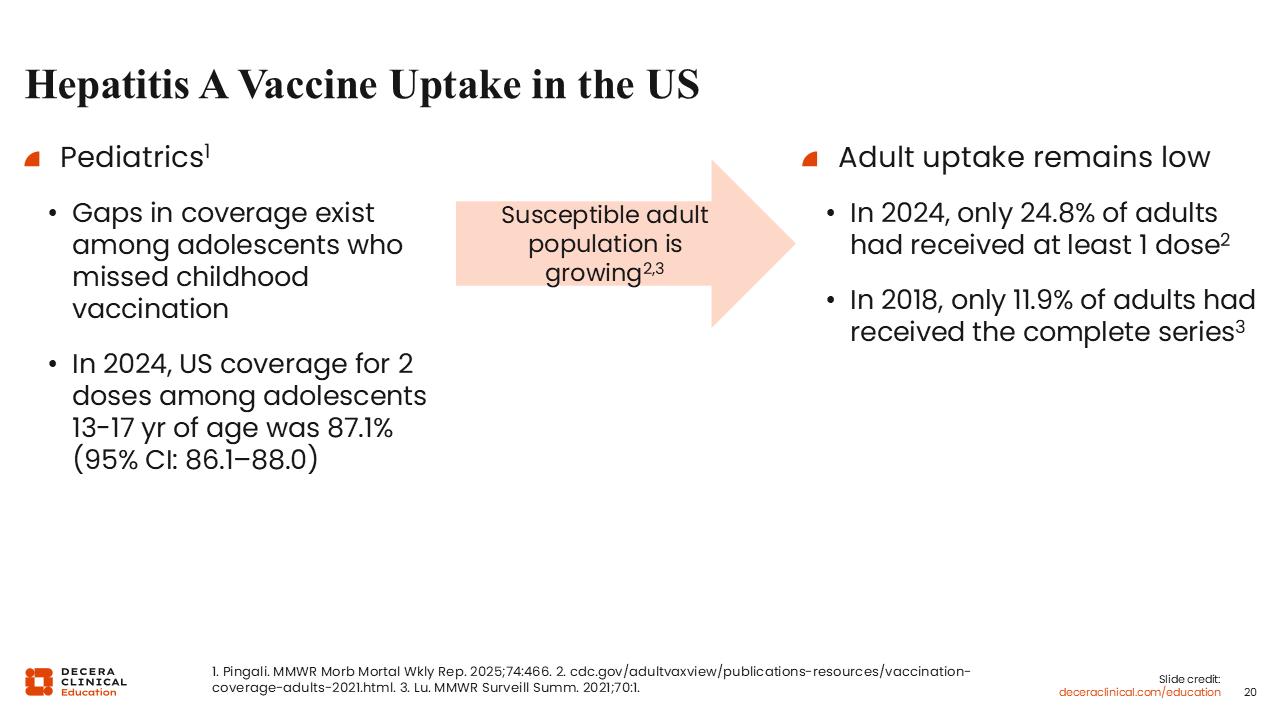
Despite long-standing recommendations and vaccine availability, HAV vaccine uptake in the United States is still lacking.
Among pediatric populations, vaccination gaps remain among adolescents who missed childhood vaccination.35
Adult uptake remains substantially lower. I think this is likely because HAV vaccination for adults is based primarily on risk factors rather than universal recommendations.36,37
However, recent outbreaks have highlighted the necessity of HAV vaccination. Outbreaks have occurred not only in traditionally recognized high-risk settings, but also in restaurants, delis, and other community settings. Vaccination provides long-term protection and helps reduce these risks.
Hepatitis B Vaccine Uptake in the United States: Newborns
Su Wang, MD, MPH, FACP:
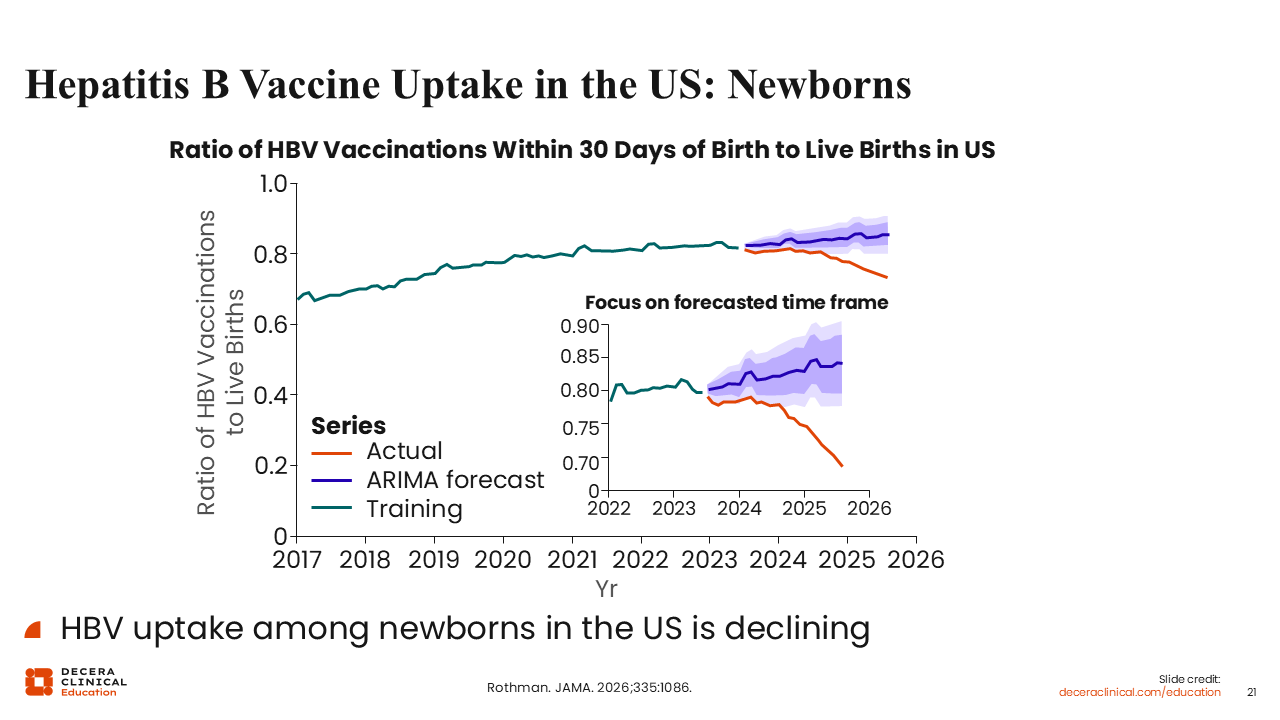
For HBV, the recommendation for universal infant vaccination has led to relatively high rates of vaccine uptake in the United States. The rate of HBV vaccination within 30 days of birth has generally approached 80%, although the target remains 90%.38
This metric is particularly important because universal birth-dose vaccination is central to HBV elimination efforts and preventing mother to child transmission, which is a WHO target.
However, there has been some decline in uptake recently. This is particularly concerning because these gaps may contribute to future increases in chronic HBV infection and liver disease burden in the near future.38
Hepatitis B Vaccine Uptake in the United States: Pediatrics
Su Wang, MD, MPH, FACP:
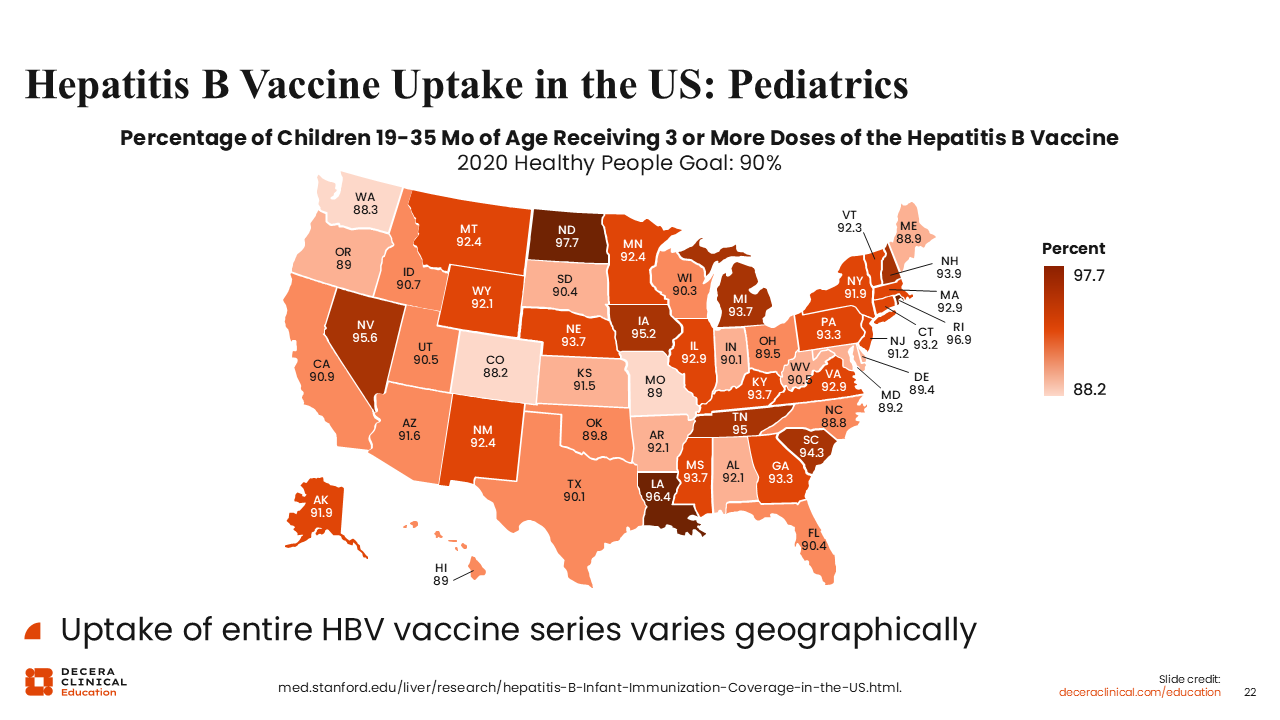
Vaccine uptake varies by state.
Many states continue to achieve vaccination rates near or >90%, which aligns with elimination targets.39
However, many states remain below this threshold. Given recent changes in federal vaccine recommendations, there is growing concern that widening coverage gaps could lead to increases in acute HBV infection, chronic HBV infection, cirrhosis, and liver cancer over time.39
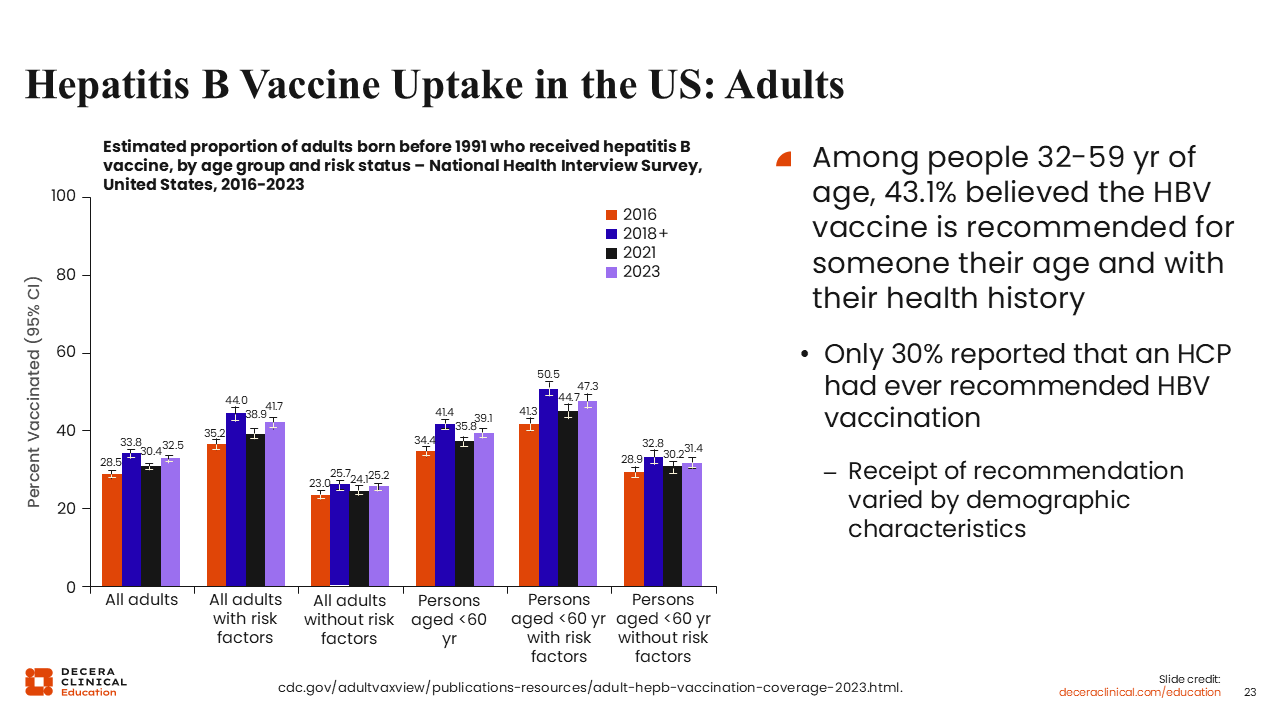
Hepatitis B Vaccine Uptake in the United States: Adults
Su Wang, MD, MPH, FACP:
We explained how HBV vaccination is recommended for all adults aged 19-59 years. Yet uptake in adults also varies. Few people recognize when vaccination is recommended for them, and only 30% report that an HCP has ever recommended vaccination to them.40
This suggests there is still substantial opportunity for HCPs to improve vaccine recommendations and patient education. Pharmacies are also increasingly helping by reminding patients to return for HBV vaccination.
The data also demonstrate that individuals without recognized risk factors are less likely to be vaccinated. Ensuring that all eligible adults are given the opportunity for HBV vaccination remains important.40