CE / CME
The Current Treatment Landscape and Unmet Needs in Head and Neck Cancers
Physician Assistants/Physician Associates: 0.25 AAPA Category 1 CME credit
Pharmacists: 0.25 contact hour (0.025 CEUs)
Physicians: maximum of 0.25 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.25 Nursing contact hour
Released: June 16, 2026
Expiration: December 15, 2026
Activity
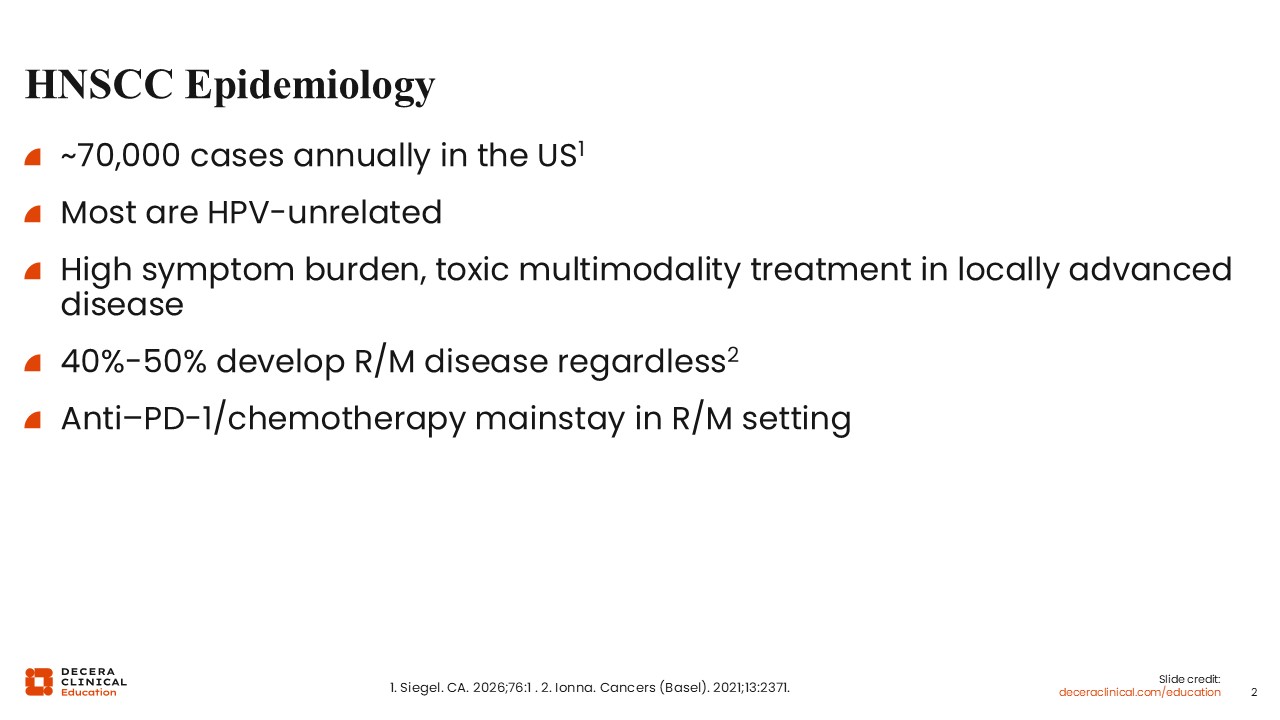
HNSCC Epidemiology
HNSCCs have an incidence of approximately 70,000 cases annually in the United States.1 Approximately 30% to 40% of these are HPV positive, but the majority are HPV negative. The disease carries a significant symptom burden because the tumors arise in the head and neck, which house several important structures, such as the airway and critical blood vessels, with vital functions (eg, swallowing).
Treatment is usually multimodal in curative-intent settings, utilizing surgery, radiation, and chemotherapy or a combination thereof, which can contribute to symptom burden. Despite multimodality treatment, approximately 40% to 50% of patients will typically experience disease recurrence or distant spread.2 At that point, palliative systemic therapy is the mainstay of treatment. Anti–PD-1 agents, specifically pembrolizumab and nivolumab, have been approved as single agents to treat adults with recurrent/metastatic HNSCC with disease progression. Pembrolizumab is approved for use in patients with recurrent/metastatic HNSCC in combination with platinum and 5-fluorouracil (5-FU) for the first-line treatment of patients or as a single agent for the first-line treatment of patients with metastatic or unresectable, recurrent HNSCC whose tumors have PD-L1 combined positive score (CPS) ≥1, or as a single agent for the treatment of patients with recurrent or metastatic HNSCC with disease progression on or after platinum-containing chemotherapy. Nivolumab is approved for use in patients with recurrent/metastatic HNSCC with disease progression on or after a platinum-based therapy.3,4
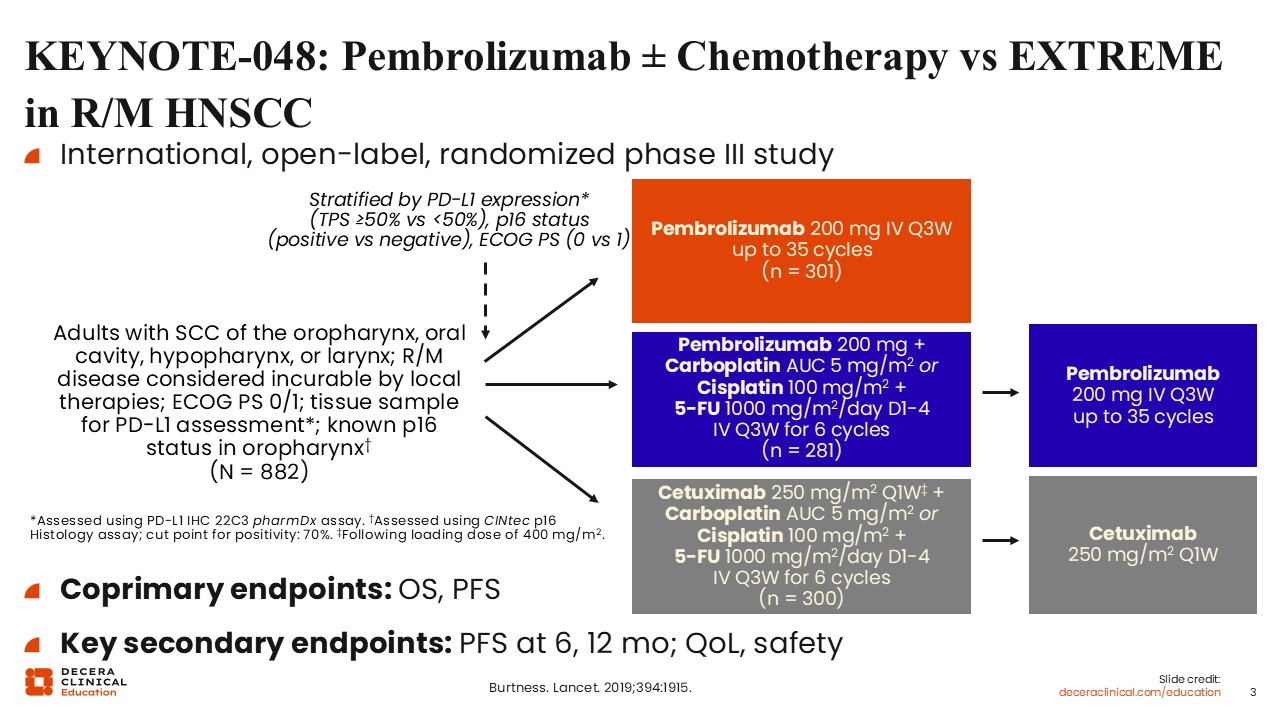
KEYNOTE-048: Pembrolizumab ± Chemotherapy vs EXTREME in R/M HNSCC
KEYNOTE-048 was a randomized phase III trial testing the best treatment in the first-line setting for patients with recurrent/metastatic HNSCC. This trial enrolled treatment-naive patients with recurrent and/or metastatic disease with an ECOG performance status of 0/1 and known p16 status (for those with oropharyngeal tumors). Patients were stratified by their PD-L1 expression (assessed retrospectively), P16 status (for oropharyngeal tumors), and ECOG performance status. Patients were randomized to receive pembrolizumab monotherapy, pembrolizumab plus chemotherapy, or the SoC (EXTREME) regimen.
The chemotherapy utilized was a platinum doublet. Investigators had the choice of either carboplatin or cisplatin in combination with 5-FU. Chemotherapy was administered in 3-week cycles for a total of 6 cycles, followed by pembrolizumab maintenance for up to 2 years.
The EXTREME regimen was a combination of platinum doublet chemotherapy and the EGFR monoclonal antibody cetuximab. The chemotherapy backbone was the same in both arms. Patients received either carboplatin or cisplatin in combination with 5-FU in 3-week cycles for a total of 6 cycles, followed by cetuximab maintenance.5
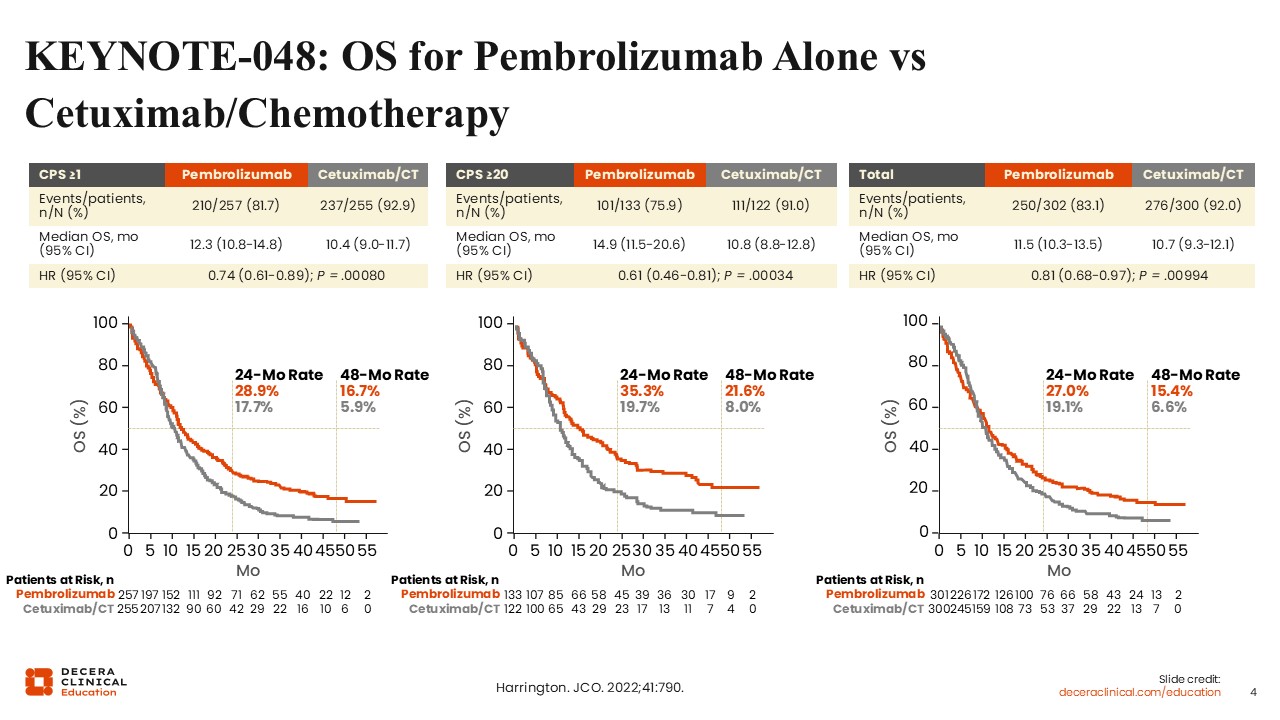
KEYNOTE-048: OS for Pembrolizumab Alone vs Cetuximab/Chemotherapy
The primary endpoint was OS. When interpreting these results, it is important to remember that the total population was not selected based on PD-L1 status.
As shown here, pembrolizumab alone had noninferior OS when compared to cetuximab plus chemotherapy for the total population, but pembrolizumab did demonstrate superior OS compared to cetuximab plus chemotherapy for patients with PD-L1 CPS ≥1, as well as for patients with PD-L1 CPS ≥20.5
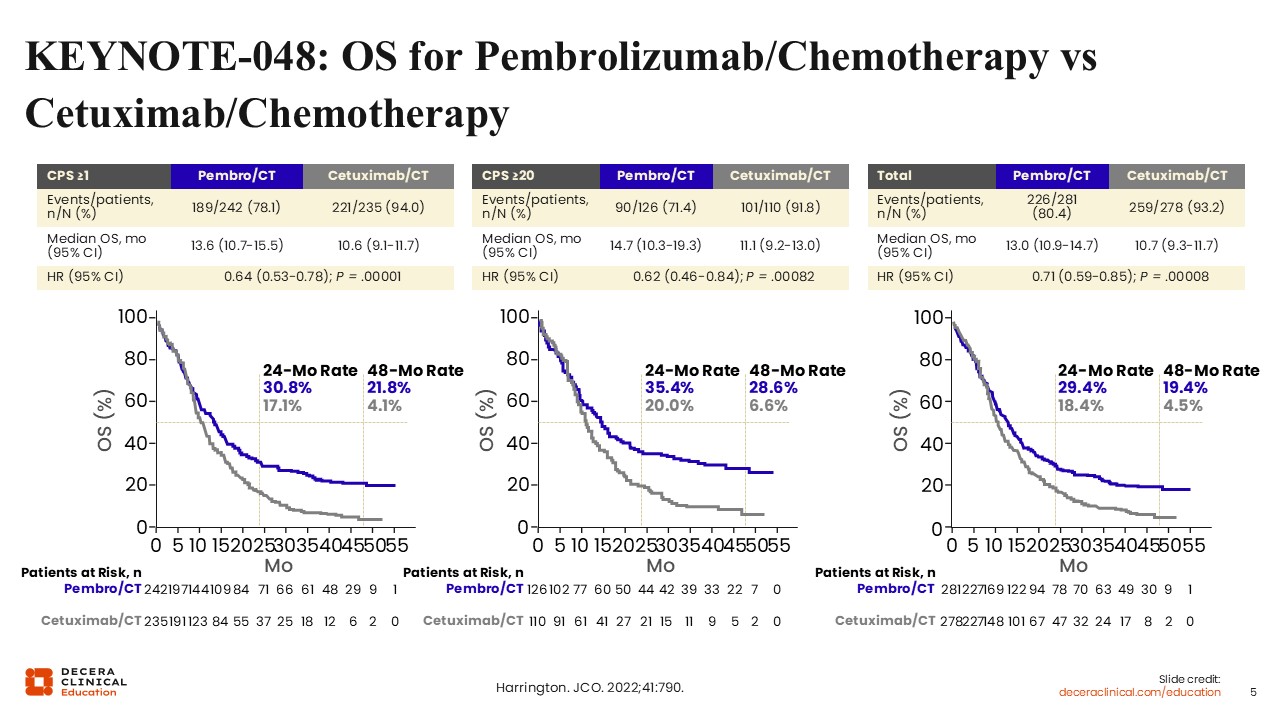
KEYNOTE-048: OS for Pembrolizumab/Chemotherapy vs Cetuximab/Chemotherapy
Likewise, OS was also compared for pembrolizumab plus chemotherapy vs cetuximab plus chemotherapy. Regardless of PD-L1 CPS, pembrolizumab plus chemotherapy demonstrated a statistically significant improvement in OS compared to cetuximab plus chemotherapy in the entire population and among CPS subgroups at both 2 and 4 years of follow-up.5
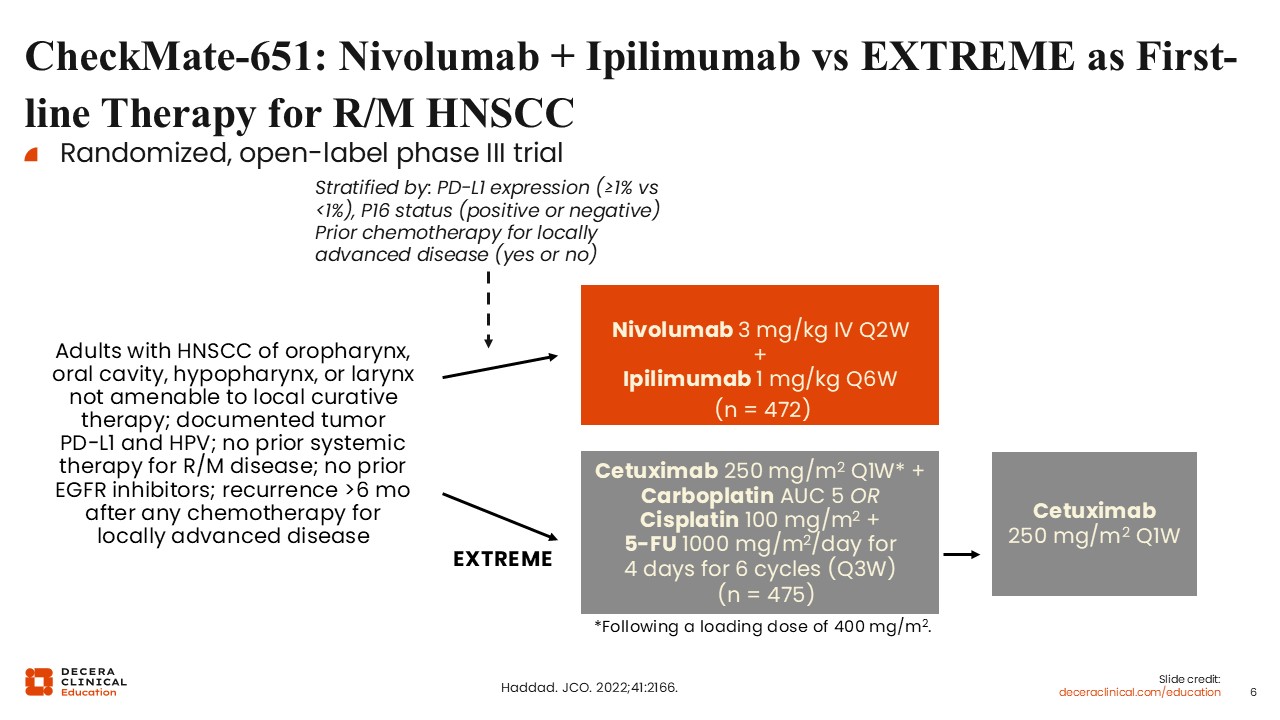
CheckMate-651: Nivolumab + Ipilimumab vs EXTREME as First-line Therapy for R/M HNSCC
CheckMate 651 was another randomized phase III trial in which treatment-naive patients with recurrent and/or metastatic disease were randomized to receive the combination of nivolumab and ipilimumab (an anti–PD-1 and anti–CTLA-4 therapy, respectively) or chemotherapy and cetuximab. Patients were stratified by PD-L1 scores, P16 status, and prior receipt of chemotherapy in the locally advanced setting. The chemotherapy regimen was similar to KEYNOTE-048, and investigators had the choice to give carboplatin or cisplatin in combination with 5-FU and cetuximab. Following 6 cycles of chemotherapy and cetuximab, patients received cetuximab maintenance.6
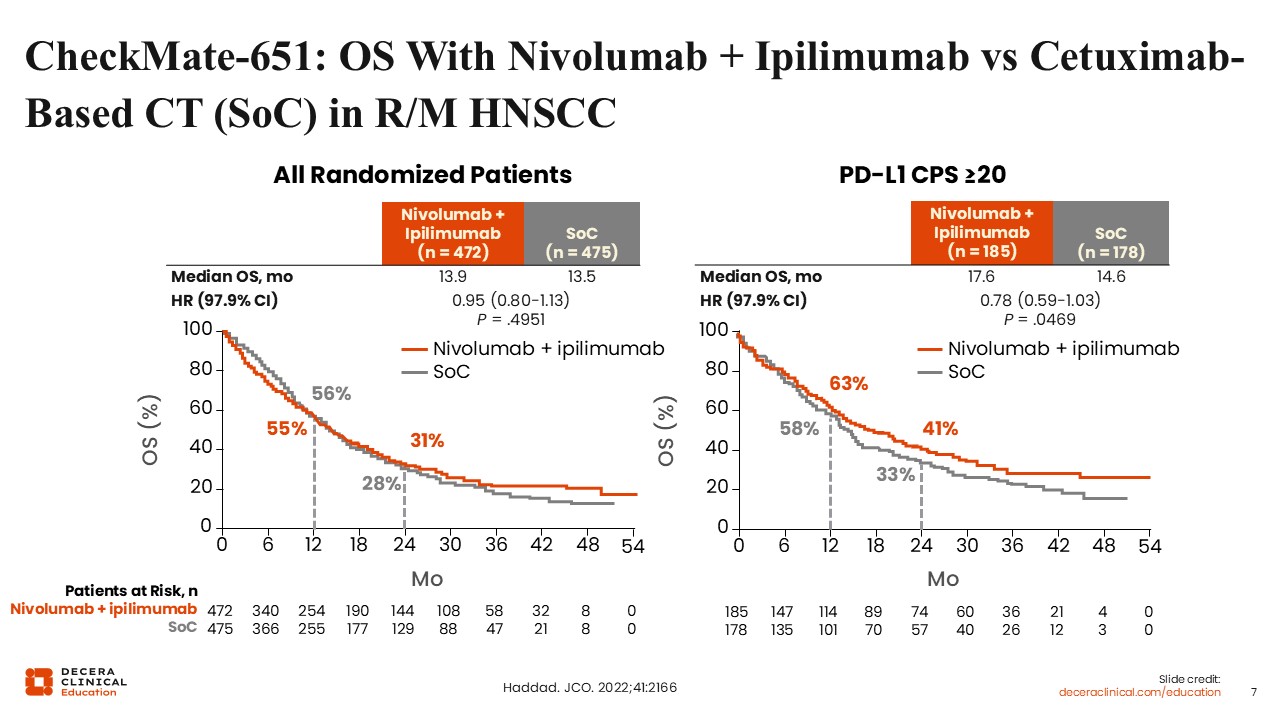
CheckMate-651: OS With Nivolumab + Ipilimumab vs Cetuximab-Based CT (SoC) in R/M HNSCC
Unfortunately, this trial did not meet its primary endpoint of OS improvement since there was no significant difference between treatment arms. In fact, these are overlapping curves for OS when you compare the dual immune checkpoint inhibitor (ICI) therapy to SoC in the total population, so unselected for PD-L1 status. In the PD-L1 CPS ≥20, there was a trend to improvement in OS with dual ICI therapy vs SoC, but it did not meet statistical significance. The study was unfortunately not powered for this subset of patients.6
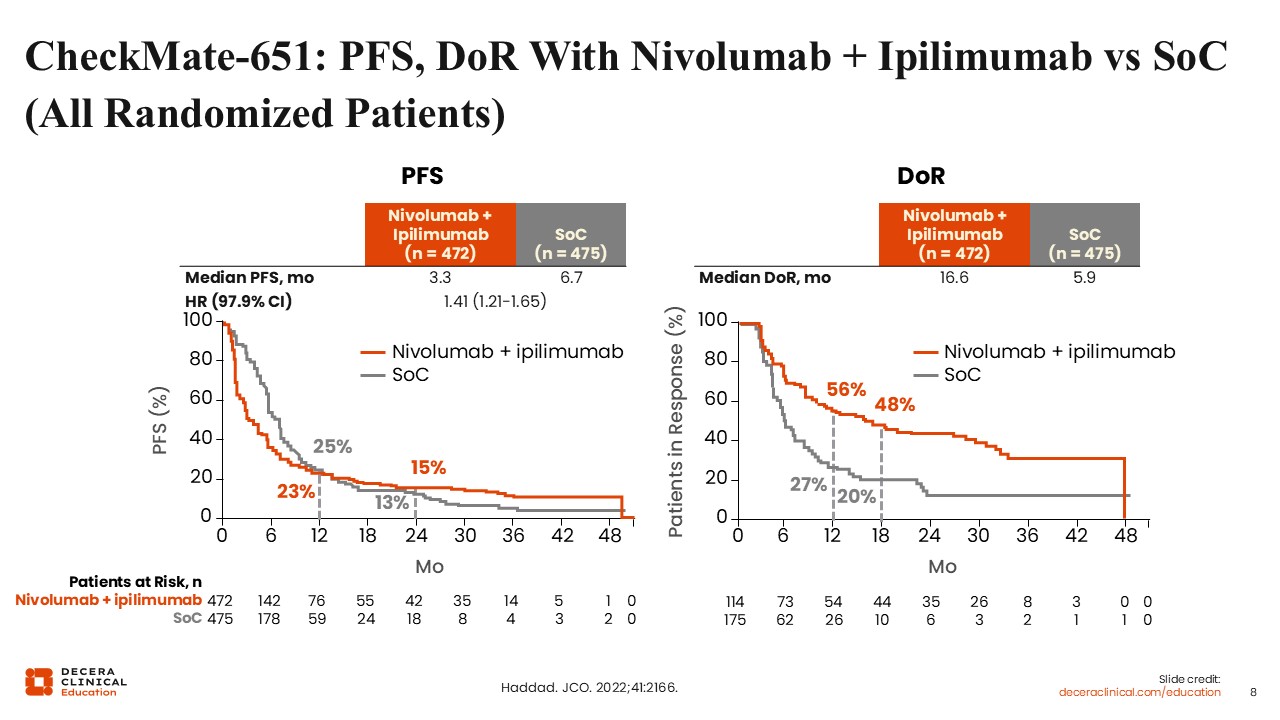
CheckMate-651: PFS, DoR With Nivolumab + Ipilimumab vs SoC (All Randomized Patients)
In addition, the progression-free survival (PFS) was not improved. In fact, it was worse on the ipilimumab and nivolumab arm vs chemotherapy and cetuximab. However, there was improvement in the duration of response for the total population. It was approximately 17 months with dual ICI therapy vs 6 months with SoC. This trend was amplified for patients with PD-L1 CPS ≥20, where the duration of response was 32 months vs 7 months for dual ICI therapy vs SoC, respectively.6 Unfortunately, the study missed its primary endpoint, so this was not overall practice changing, but the NCCN guidelines do list ipilimumab and nivolumab as an option to be carefully considered in patients with high CPS scores.
Alternate Approaches in First-line Therapy for R/M HNSCC
Following the 2019 approval of pembrolizumab, alone or with chemotherapy, as first-line treatment for recurrent/metastatic disease, a follow-up trial called KEYNOTE-B10 was conducted. This phase IV, single-arm registrational study evaluated the effectiveness of a regimen that does not include 5-FU, which can be difficult to use in clinical practice. Administering 5-FU typically requires a port and infusion pump to deliver the drug over 4-5 days, as well as an additional visit for pump removal.
KEYNOTE-B10 showed that a combination of pembrolizumab, platinum, and paclitaxel had a significant response rate of 50% and median OS of 13 months, similar to KEYNOTE-048, thus establishing this regimen as an alternative to a 5-FU–based plan for patients who would rather avoid the pump administration of chemotherapy.7
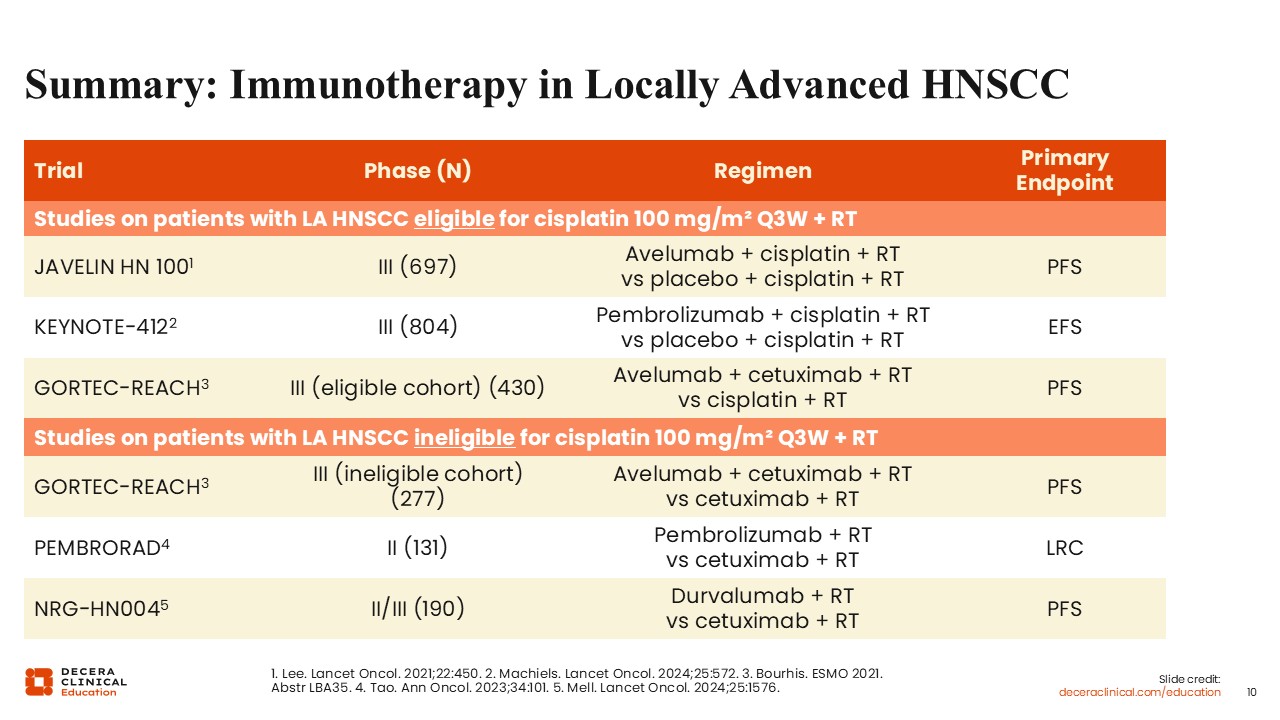
Summary: Immunotherapy in Locally Advanced HNSCC
Following the success of ICI therapy in recurrent/metastatic HNSCC, there were several trials that looked at administering immunotherapy in combination with definitive therapy for patients who had locally advanced HNSCC, as summarized in this table.
JAVELIN looked at the addition of avelumab to cisplatin and radiation in a randomized phase III trial comparing the administration of just cisplatin and radiation, which is the SoC. KEYNOTE-412 was similarly a randomized phase III trial that looked at pembrolizumab plus cisplatin plus radiation vs placebo plus cisplatin plus radiation.
Both trials were unfortunately negative and did not improve PFS or event-free survival, respectively.8,9 Similarly, there were trials designed for cisplatin-ineligible patients. These trials compared cetuximab and radiation vs anti–PD-1 or anti–PD-L1 agents with radiation. These trials also missed the mark in terms of meeting their primary endpoint, and overall were not practice changing.
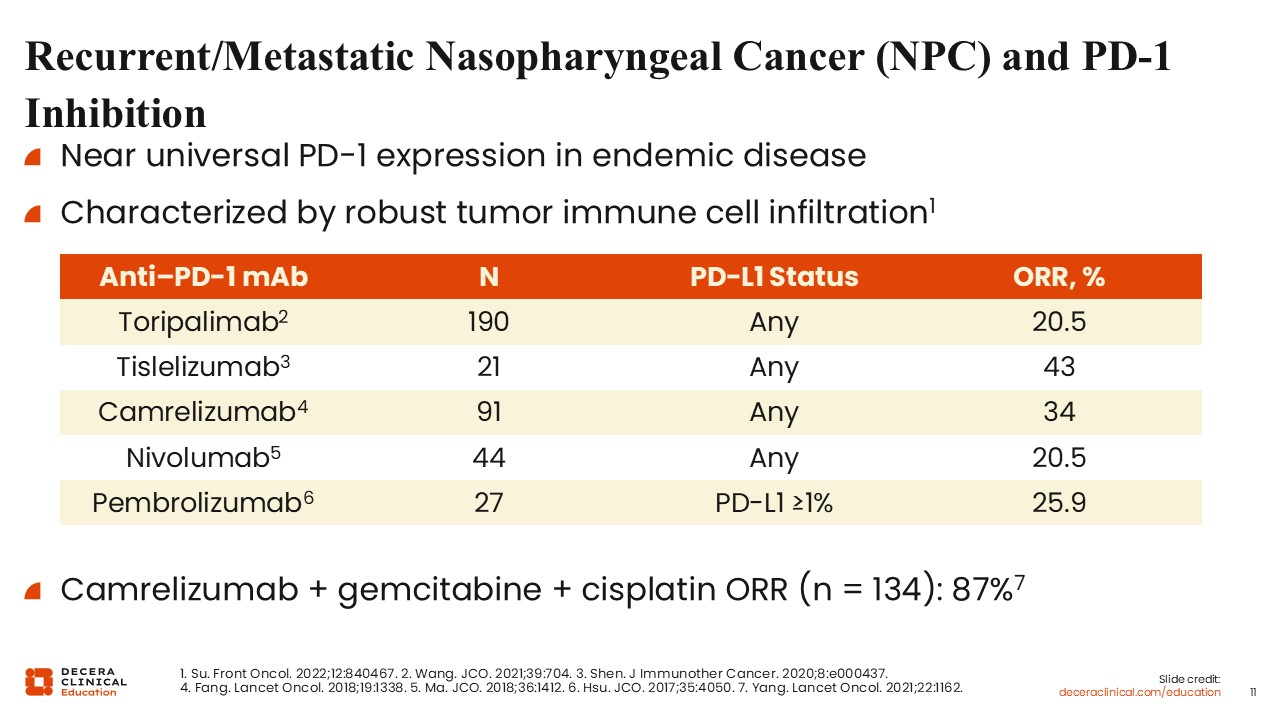
Recurrent/Metastatic Nasopharyngeal Cancer (NPC) and PD-1 Inhibition
There are similar clinical efficacy data with ICI therapy in patients with recurrent and metastatic nasopharyngeal cancer (NPC), a distinct, virally mediated subtype of head and neck tumors. NPC is most common in Asia and is typically associated with the Epstein-Barr virus (EBV). In the United States, NPC may also be linked to HPV or occur without a viral cause, though EBV-associated disease remains the predominant form worldwide.10
NPC tumors tend to be more responsive to chemotherapy and radiation but have a higher risk of distant metastasis. They are also highly inflamed, with strong immune cell infiltration in the tumor microenvironment and near universal PD-1 expression, especially in EBV-positive disease.
In the past, these tumors were called lymphoepithelioma because they were characteristically surrounded by a rich lymphocytic infiltrate on immunohistochemical staining.11
Historically, standard first-line treatment in the recurrent/metastatic setting for NPC was platinum plus gemcitabine. Several subsequent trials evaluated anti–PD-1 agents in the second-line setting after progression on this regimen. Across studies of toripalimab, tislelizumab, camrelizumab, nivolumab, and pembrolizumab, single-agent therapy produced overall response rates of approximately 20% to 30%. In contrast, when these agents were combined with gemcitabine and cisplatin, response rates were much higher.12-17
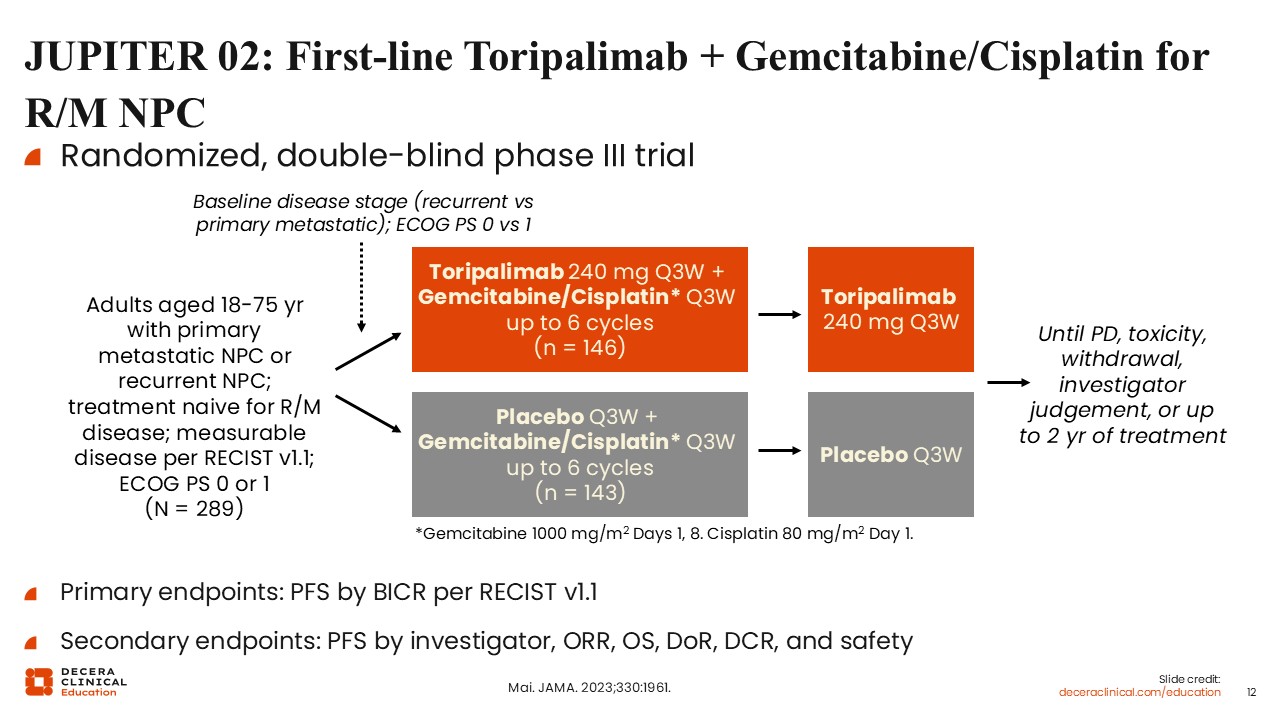
JUPITER 02: First-line Toripalimab + Gemcitabine/Cisplatin for R/M NPC
As a follow-up to this evidence, there were multiple phase III trials that looked at adding anti–PD-1 agents to platinum and gemcitabine-based chemotherapy in the first-line setting for recurrent/metastatic NPC. Among these trials was JUPITER-02, a phase III study that randomized patients with treatment-naive, recurrent, or metastatic NPC, regardless of PD-L1 status, to either placebo or toripalimab, an anti–PD-1 agent in combination with gemcitabine/cisplatin.
On the control arm, patients received 6 cycles of chemotherapy followed by placebo every 3 weeks, and on the experimental arm, patients received the same chemotherapy backbone but in combination with toripalimab. Following 6 cycles of chemotherapy, patients received either placebo or toripalimab maintenance for 2 years or until disease progression.
The primary endpoints were PFS by independent clinical assessment or by independent clinical review, and secondary endpoints were PFS by the investigator, objective response rate, and OS, among other endpoints.18
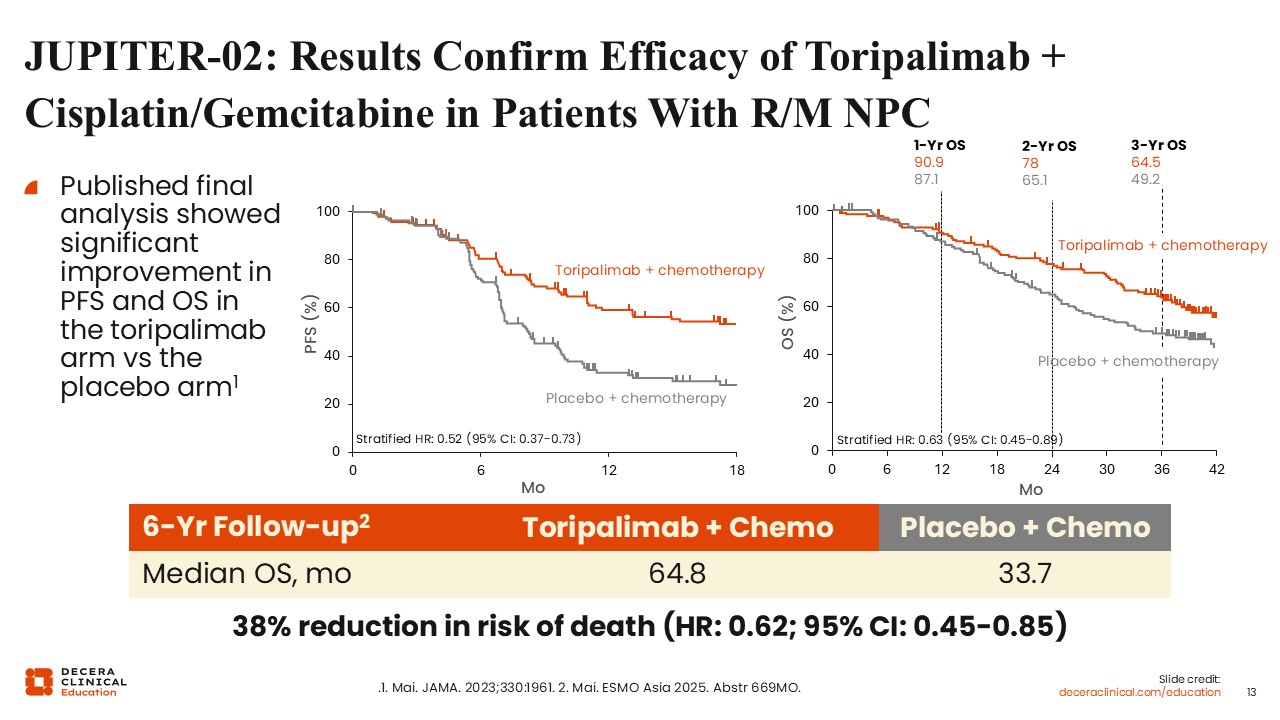
JUPITER-02: Results Confirm Efficacy of Toripalimab + Cisplatin/Gemcitabine in Patients With R/M NPC
JUPITER-02 demonstrated that the combination of chemotherapy and toripalimab significantly improved PFS.18 A subsequent analysis at 6-year follow-up also confirmed an improvement in OS.19
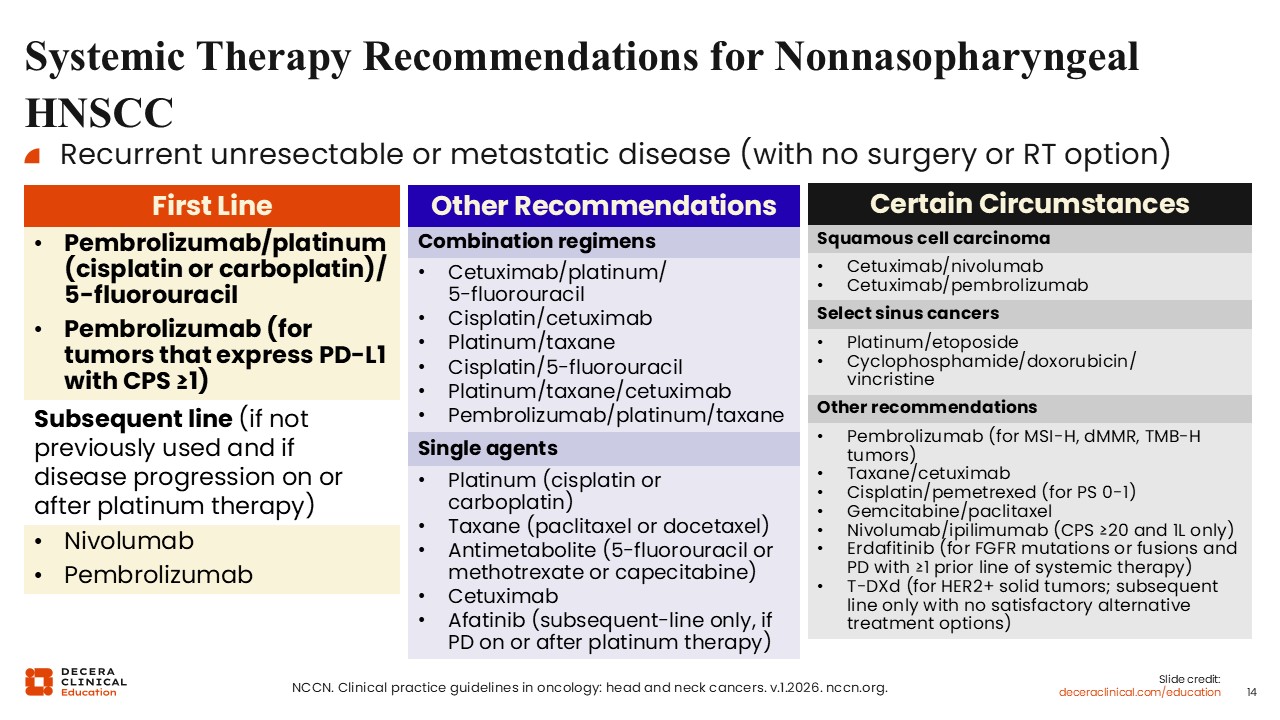
Systemic Therapy Recommendations for Nonnasopharyngeal HNSCC
Based on data from KEYNOTE-048 and the nasopharyngeal trials, the 2026 NCCN guidelines now reflect what standard first-line treatment is. For patients with nonnasopharyngeal recurrent/metastatic HNSCC, the first-line preferred regimens are pembrolizumab monotherapy (for patients who have PD-L1 CPS ≥1) or pembrolizumab in combination with chemotherapy. For patients who are unable to or do not receive ICIs in the first line, both nivolumab and pembrolizumab are approved in the second-line setting.
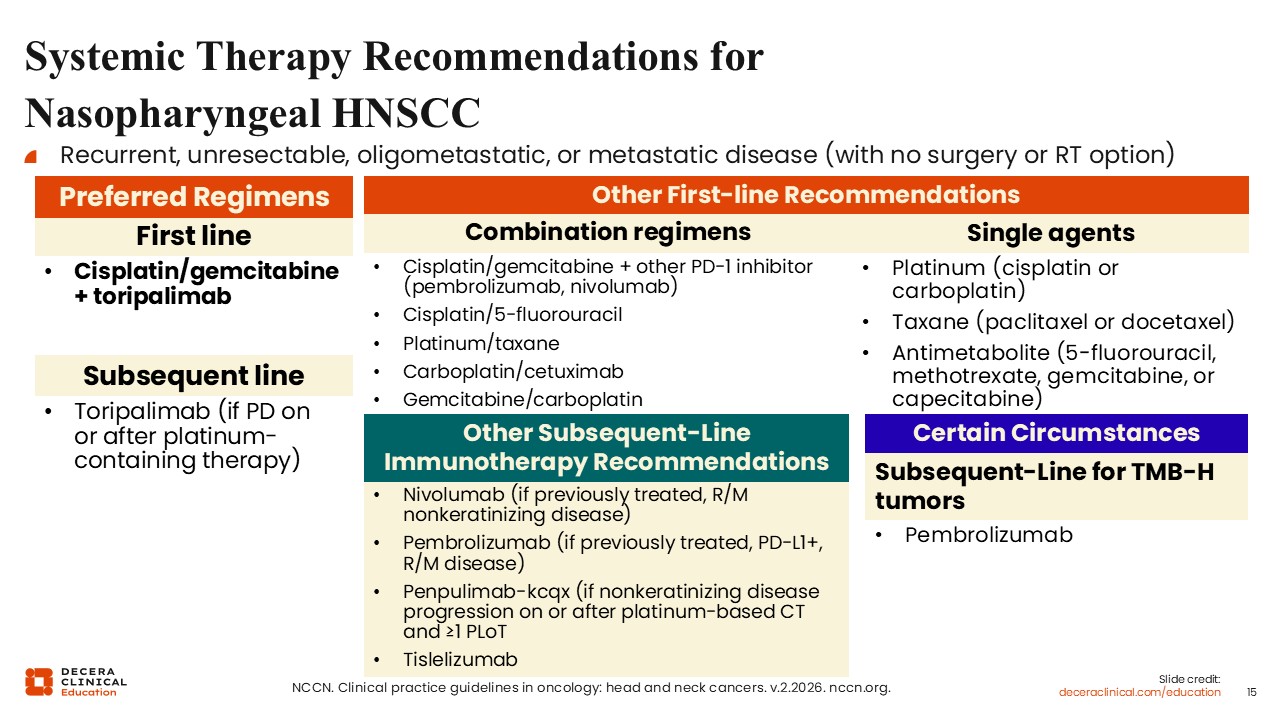
Systemic Therapy Recommendations for Nasopharyngeal HNSCC
Likewise, for nasopharyngeal recurrent/metastatic HNSCC, the preferred first-line regimens in the NCCN guidelines are platinum and gemcitabine in combination with toripalimab. Other first-line recommendations include pembrolizumab or nivolumab in combination with chemotherapy. Second-line therapy options include nivolumab, pembrolizumab, or tislelizumab.
Unmet Needs
Despite the efficacy that we have seen with ICIs in head and neck cancers, only a small percentage of patients clinically benefit from their use as monotherapy, where response rates tend to hover in the 20% to 30% range.12-16 Moreover, most patients eventually develop immunotherapy resistance, so there is a clear need for more effective therapies that can be added to ICIs or the development of targeted therapies, which can provide synergy.20
There is also a need to select patients based on HPV status. HPV-positive disease is a distinct biologic subset that responds differently to chemotherapy and ICIs.21 Other agents, such as HPV therapeutic vaccines, will also hopefully be developed soon.HPV-negative disease is a more aggressive subset with lower response rates and shorter survival with today’s current SoC. For more information on newer therapies in development for patients with HNSCC, be sure to look for additional text modules in this program that are coming soon.