
CE / CME
Optimizing Mantle Cell Lymphoma Care: Case-Based Guidance From EU Experts
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
European Learners: 1.00 EBAC® CE Credit
Released: May 29, 2026
Expiration: November 28, 2026

Activity
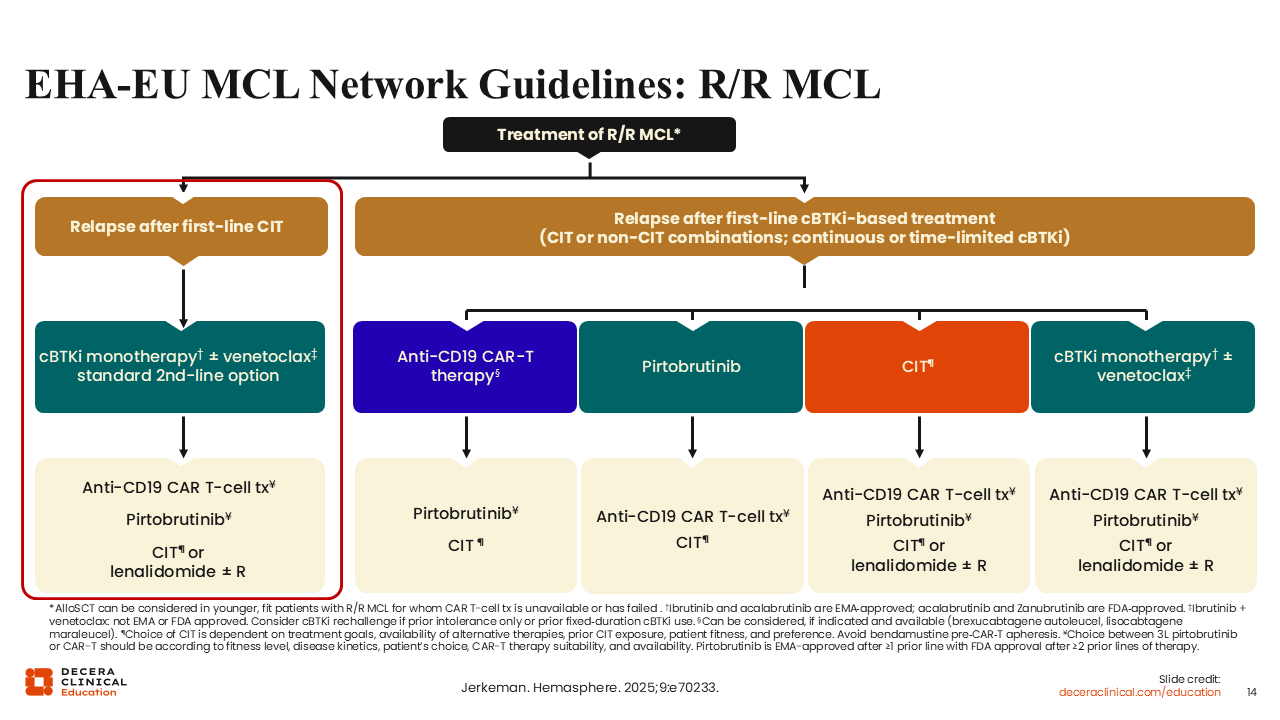
EHA-EU MCL Network Guidelines: R/R MCL
A very important factor to consider when making treatment decisions in the R/R MCL setting is whether the patient’s disease has been previously exposed to a BTK inhibitor.5 For patients who received chemotherapy only as first-line therapy without any previous exposure to a covalent BTK inhibitor, the standard second-line option is a covalent BTK inhibitor. The choice of the covalent BTK inhibitor will be based on availability in the geographic region where the patient is seeking treatment. Younger and fit patients with R/R MCL who received CIT only as frontline therapy should be considered for treatment with a covalent BTK inhibitor with or without venetoclax, a BCL2 inhibitor, in the second-line setting.
After disease progression on second-line covalent BTK inhibitor monotherapy or in combination with venetoclax, the recommended next-line treatment options include CAR T-cell therapy, the noncovalent BTK inhibitor pirtobrutinib, and lenalidomide with or without rituximab.
Of note, Decera Clinical Education has developed an Interactive Decision Support Tool, which can be found here and can be used to access recommendations from 5 EU experts for patients with R/R MCL based on multiple disease characteristics, including the presence or absence of high-risk features and/or comorbidities, age at diagnosis, and the level of fitness. The tool is accessible to all and allows all users to try various case scenarios.
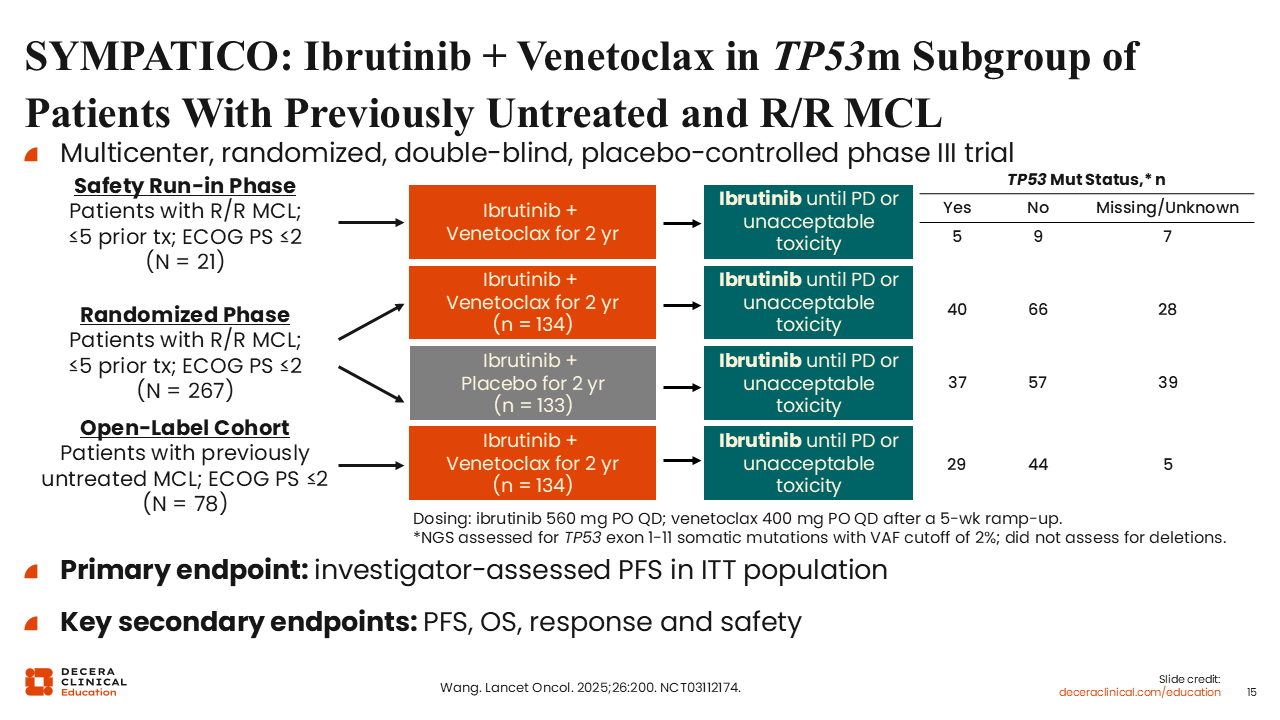
SYMPATICO: Ibrutinib + Venetoclax in TP53m Subgroup of Patients With Previously Untreated and R/R MCL
Next, I briefly review the efficacy of combining a covalent BTK inhibitor with venetoclax for patients with R/R MCL.
SYMPATICO is a randomized, double-blind, placebo-controlled phase III study that investigated ibrutinib plus venetoclax for patients with MCL.23 The randomized portion of the trial included 267 patients who had received 1-5 previous lines of therapy. Patients were randomly assigned to receive ibrutinib plus placebo vs ibrutinib plus venetoclax. All patients received ibrutinib until disease progression or unacceptable toxicity. Approximately 40% of these patients had disease harboring a TP53 mutation.
The primary endpoint was PFS by investigator assessment in the intention-to-treat population, and the key secondary endpoints included OS, response, and safety.
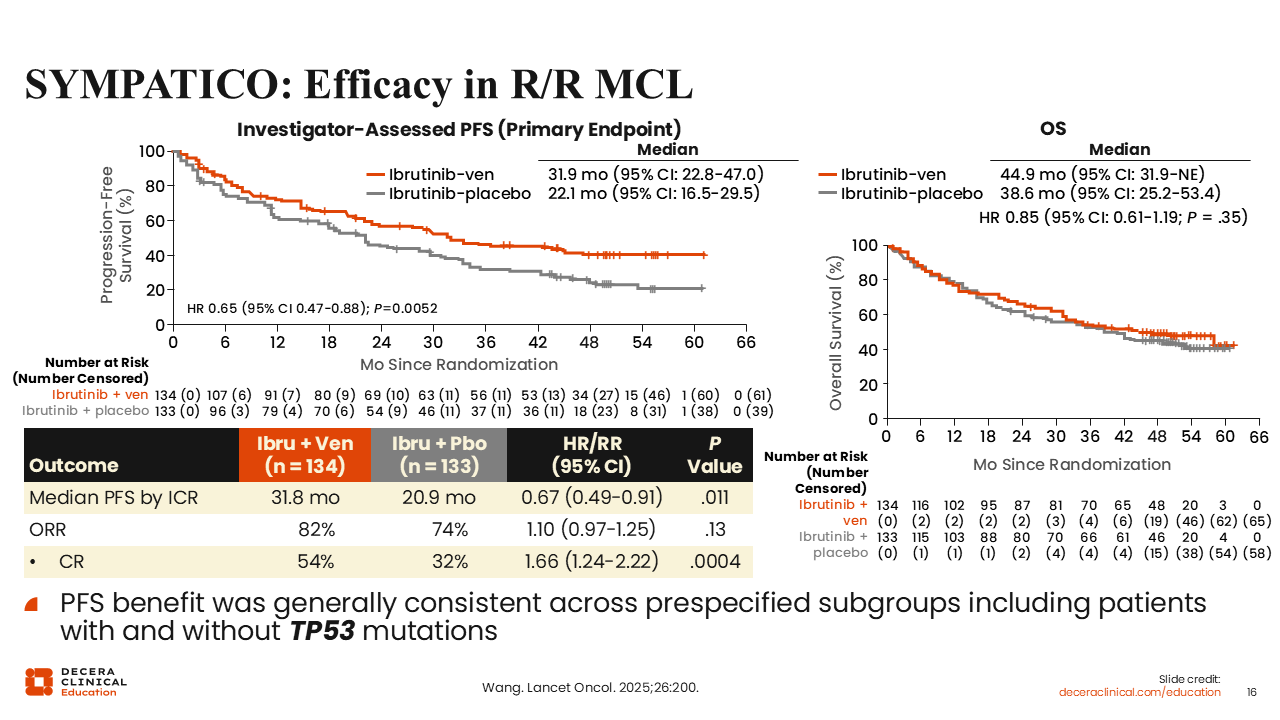
SYMPATICO: Efficacy in R/R MCL
After a median follow-up of 51.2 months, results from patients with R/R MCL in the randomized SYMPATICO trial demonstrated that ibrutinib in combination with venetoclax significantly prolonged the median PFS by approximately 10 months compared with ibrutinib plus placebo among patients with R/R MCL (31.9 vs 22.1 months; HR: 0.65; 95% CI: 0.47-0.88; P = .0052). The PFS benefit was generally consistent across prespecified subgroups including patients with and without TP53 mutations. Furthermore, the CR rates were superior with the addition of venetoclax compared with ibrutinib alone (54% vs 32%; P = .0004). However, there was no significant difference in the median OS between arms (44.9 vs 38.6 months; HR: 0.85; 95% CI: 0.61-1.19; P = .35).
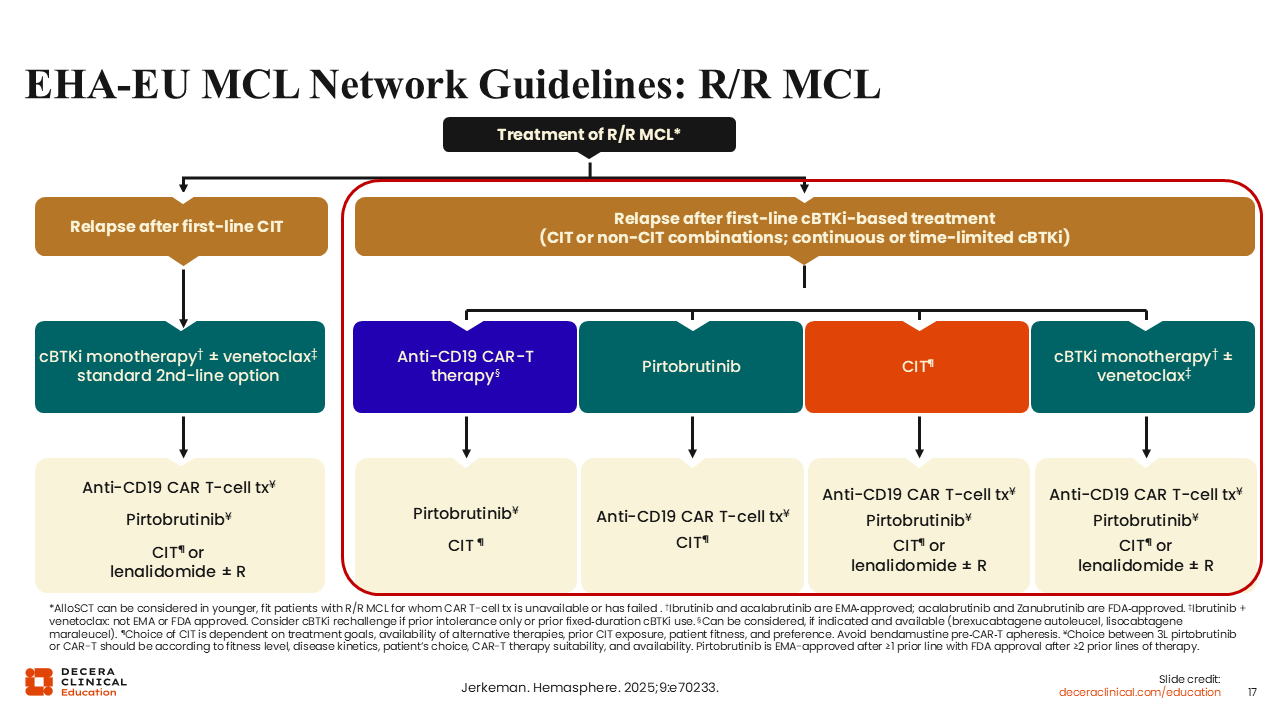
EHA-EU MCL Network Guidelines: R/R MCL
Regarding patients with MCL with disease progression after first-line covalent BTK inhibitor–based treatment, there are several available options based on the patient’s age, level of fitness, preexisting medical conditions, and the treatment being received at the time of relapse or the duration of time since completion of last-line therapy.5 For these patients, the second-line treatment options to consider include CAR T-cell therapy, pirtobrutinib, and CIT.
For patients who received time-limited covalent BTK inhibitor in the frontline setting, such as those in Arm I or Arm A + I of the TRIANGLE trial, where they received 2 years of ibrutinib maintenance, treatment with a covalent BTK inhibitor alone or in combination with venetoclax is an option. So, if the patient experienced relapse after the discontinuation of the previously used covalent BTK inhibitor, the patient can be rechallenged with either the same or different covalent BTK inhibitor.
In this setting, it is important to note that allogeneic stem cell transplant can be considered for younger, fit patients with R/R MCL for whom CAR T-cell therapy is unavailable or has failed.
ZUMA-2: Brexucabtagene Autoleucel in MCL
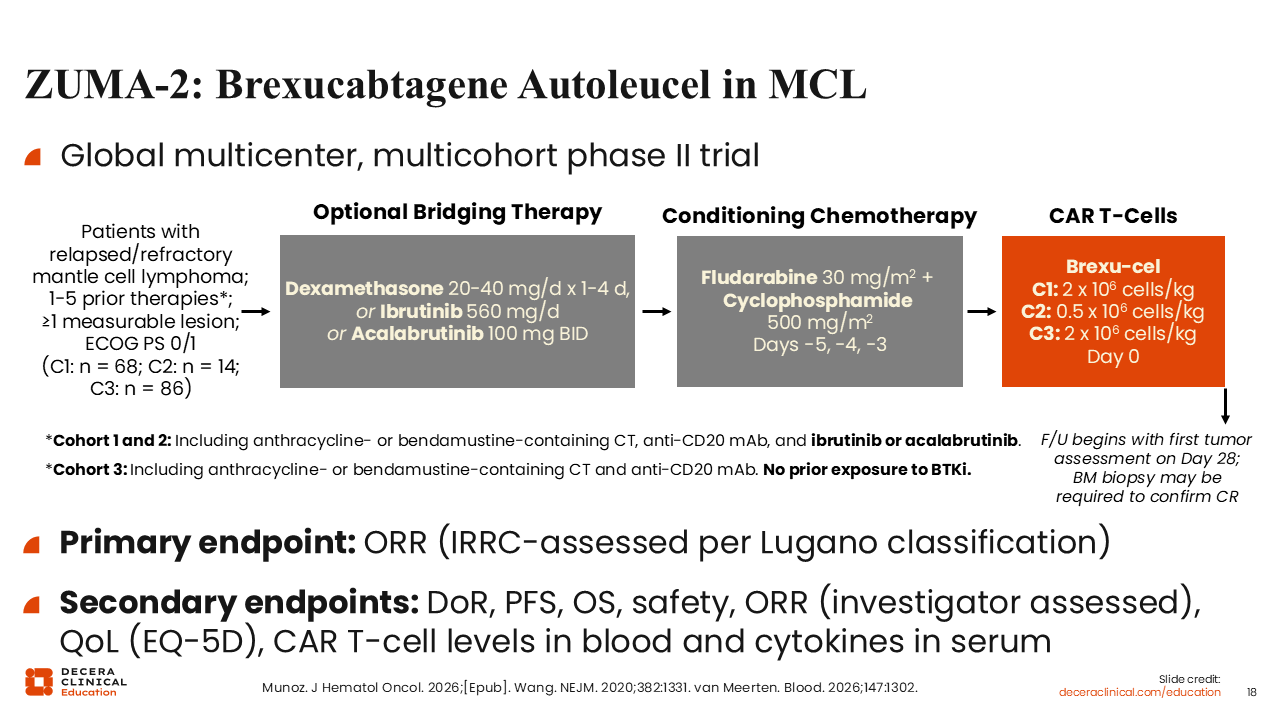
In the EU, there are 2 available CAR T-cell therapies for patients with MCL: brexucabtagene autoleucel and lisocabtagene maraleucel.24-27 Both of these therapies are directed at CD19. The EMA’s approval of brexucabtagene autoleucel in MCL was based on the results of the global, multicohort phase II ZUMA-2 trial.25 Patients with R/R MCL and ≥1 measurable lesions who had received 1-5 previous therapies were enrolled on ZUMA-2.28,29
In cohorts 1 and 2, patients must have previously received anthracycline- or bendamustine-containing chemotherapy, an anti-CD20 monoclonal antibody, and a covalent BTK inhibitor (either ibrutinib or acalabrutinib) (NCT02601313). In cohort 3, no prior exposure to a BTK inhibitor was allowed (NCT04880434). Following leukapheresis and prior to receiving conditioning therapy, patients with high disease burden received optional bridging therapy with steroids or a covalent BTK inhibitor (ibrutinib or acalabrutinib), followed by conditioning chemotherapy with fludarabine in combination with cyclophosphamide. Thereafter, patients received a single infusion of brexucabtagene autoleucel. Patients received 2 x 106 CAR T-cells/kg, 0.5 x 106 CAR T-cells/kg, and 2 x 106 CAR T-cells/kg on Day 0 in cohort 1, cohort 2, and cohort 3, respectively (NCT02601313, NCT04880434).
The primary endpoint was ORR, and the secondary endpoints included PFS, OS, safety, quality of life, and determination of CAR T-cell levels in blood and cytokines in serum.
ZUMA-2: Clinical Outcomes—Cohorts 1 and 2 (After a Prior BTKi)
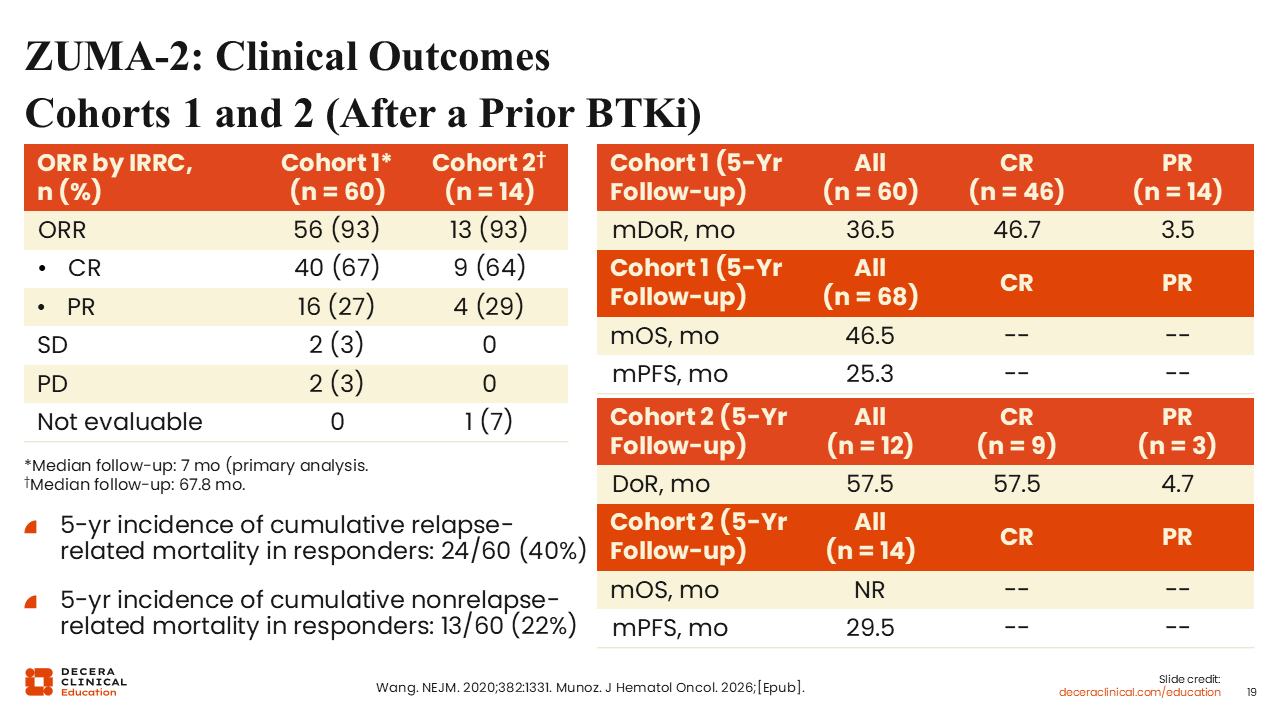
In the cohort of patients with R/R MCL who had previously been exposed to a BTK inhibitor (cohorts 1 and 2), the ORR was impressive at 93%.28,30 In cohort 1, the CR rate was 67% and the PR rate was 27% at the time of primary analysis after a median follow-up of 7 months. In cohort 2, the CR rate was 64% and the PR rate was 29% after a median follow-up of 67.8 months. After an extended duration of follow-up (67.8 months), the median duration of response was 36.5 months in cohort 1 compared with 57.5 months in cohort 2 among respondents. In cohorts 1 and 2, the median PFS was longer than 2 years. In both cohorts, the 5-year incidence of cumulative relapse-related mortality among responders was 40%, and the 5-year incidence of cumulative nonrelapse-related mortality among responders was 22%.
ZUMA-2: OS
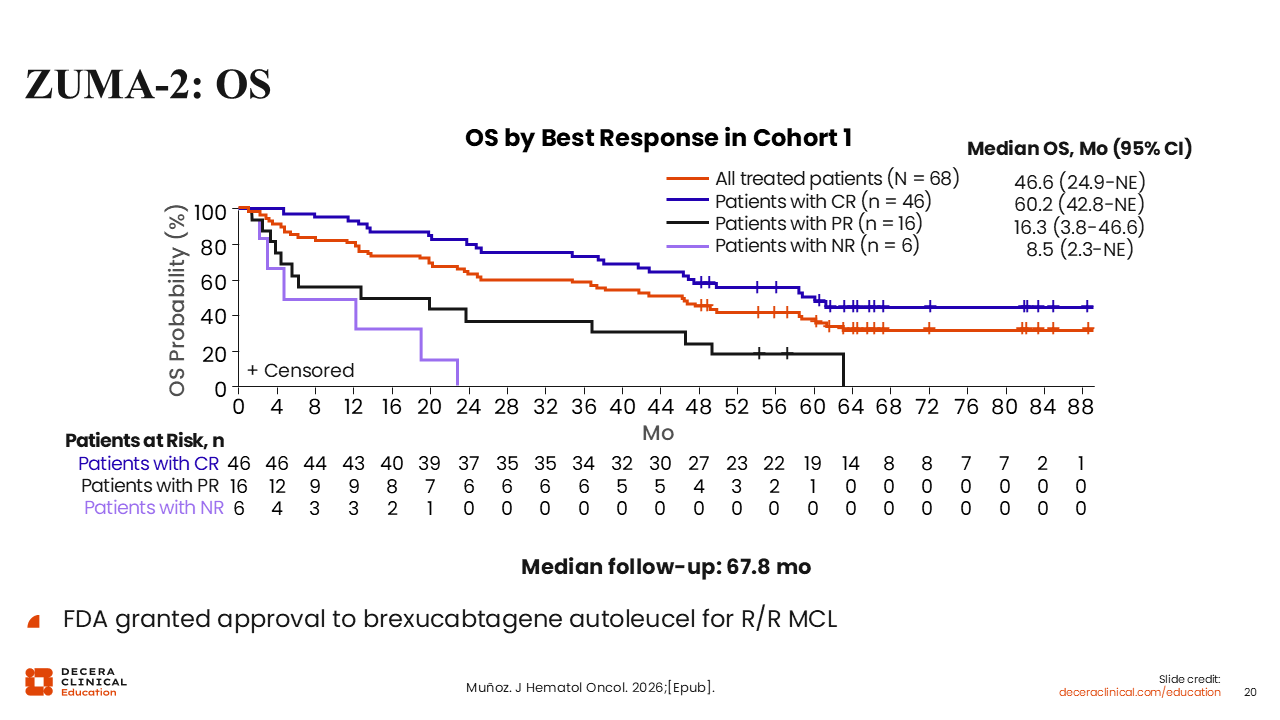
Of importance, brexucabtagene autoleucel infusion is approved by the EMA for use at 2 x 106 CAR T-cells/kg, the dose investigated in cohorts 1 and 3.28,30,31 After a median follow-up of 67.8 months in cohort 1, the median OS in all treated patients (n = 68) was 46.6 months.30 Among 46 patients who achieved a CR, the median OS was 60.2 months. Among 16 patients who achieved a PR, the median OS was dismal at 16.3 months.
ZUMA-2: ORR and ORR in Key Subgroups—Cohort 3 (No prior BTKi)
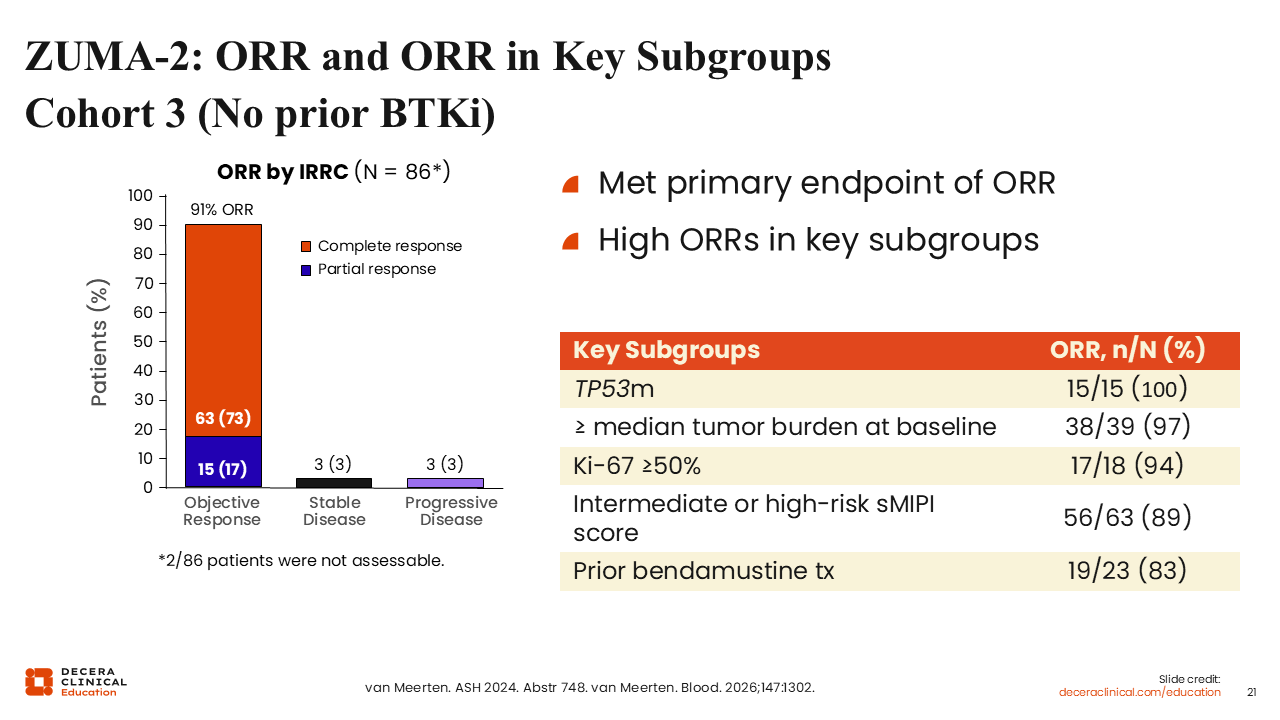
In the cohort of patients with R/R MCL who had no prior exposure to a BTK inhibitor (cohort 3), the ORR was impressively high at 91%, including a CR rate of 73% and a PR rate of 17%.31 All 15 patients (100%) with disease harboring a TP53 mutation responded to brexucabtagene autoleucel. Among 18 patients with a Ki-67 score of ≥50%, 17 (94%) achieved a response. Similarly, the ORR was high among patients with intermediate-risk or high-risk MCL International Prognostic Index score (89%) and those who had previously received bendamustine (83%).
Overall, clinical outcomes from the ZUMA-2 trial clearly demonstrate that brexucabtagene autoleucel is very effective in patients with R/R MCL regardless of previous exposure to a BTK inhibitor.
TRANSCEND-MCL: Lisocabtagene Maraleucel in MCL (MCL Cohort of TRANSCEND NHL 001)
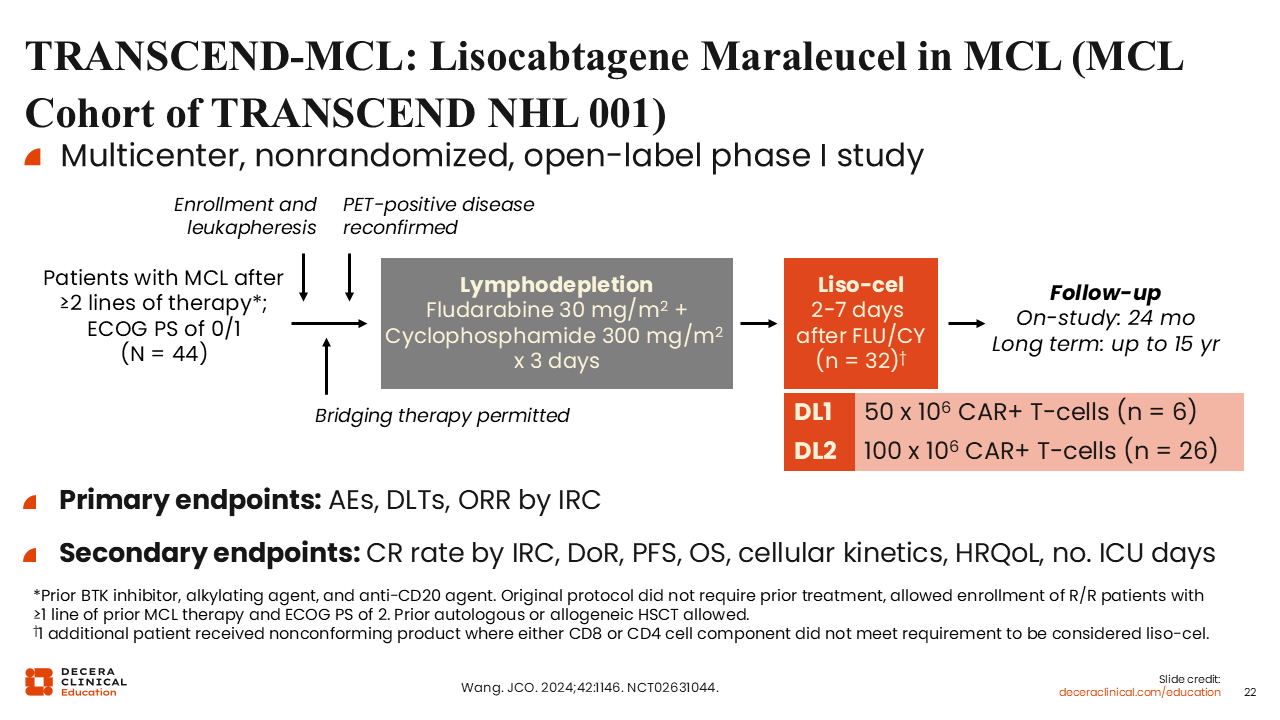
Lisocabtagene maraleucel is the other EMA-approved CAR T-cell product in MCL based on the results of the phase I TRANSCEND NHL 001 trial, which investigated the pharmacokinetics, efficacy, and safety of lisocabtagene maraleucel for patients with R/R B-cell NHL (NCT02631044). The trial included patients with R/R MCL, diffuse large B-cell lymphoma, follicular lymphoma, and primary mediastinal B-cell lymphoma. TRANSCEND-MCL focuses on the group of patients with R/R MCL who had received ≥2 prior lines of therapy, including a BTK inhibitor, alkylating agent, and an anti-CD20 antibody (N = 44).32
Patients underwent leukapheresis, and bridging therapy was permitted during the manufacture of lisocabtagene maraleucel for disease control. PET-positive disease reconfirmation by the investigator was a requirement before lymphodepletion treatment with fludarabine and cyclophosphamide for 3 days. Lisocabtagene maraleucel infusion occurred 2-7 days after lymphodepletion at 2 different dose levels: 50 x 106 CAR T-cells (dose level 1) or 100 x 106 CAR T-cells (dose level 2).
The primary endpoints were treatment-related AEs, dose-limiting toxicities, and ORR.
TRANSCEND-MCL: Efficacy
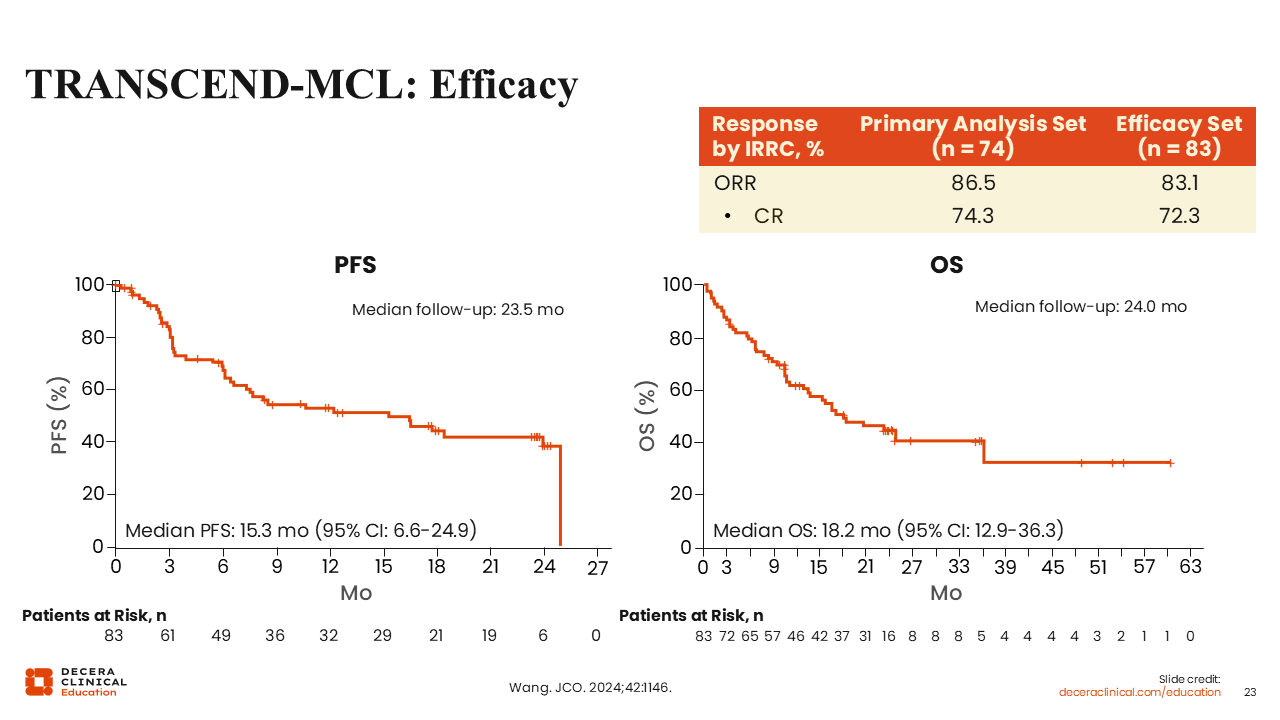
Among patients with R/R MCL, the ORR was 86.5% in the primary analysis set (n = 74), including a CR rate of 74.3%. In the efficacy set (n = 83), the ORR was 83.1% including a CR rate of 72.3%. The median PFS was 15.3 months, and the median OS was 18.2 months. Unlike what is normally observed in diffuse large B-cell lymphoma, there was no clear plateau in the PFS curve in the TRANSCEND-MCL trial; it is unclear if lisocabtagene maraleucel will be curative in MCL.
ZUMA-2 and TRANSCEND-MCL: Safety
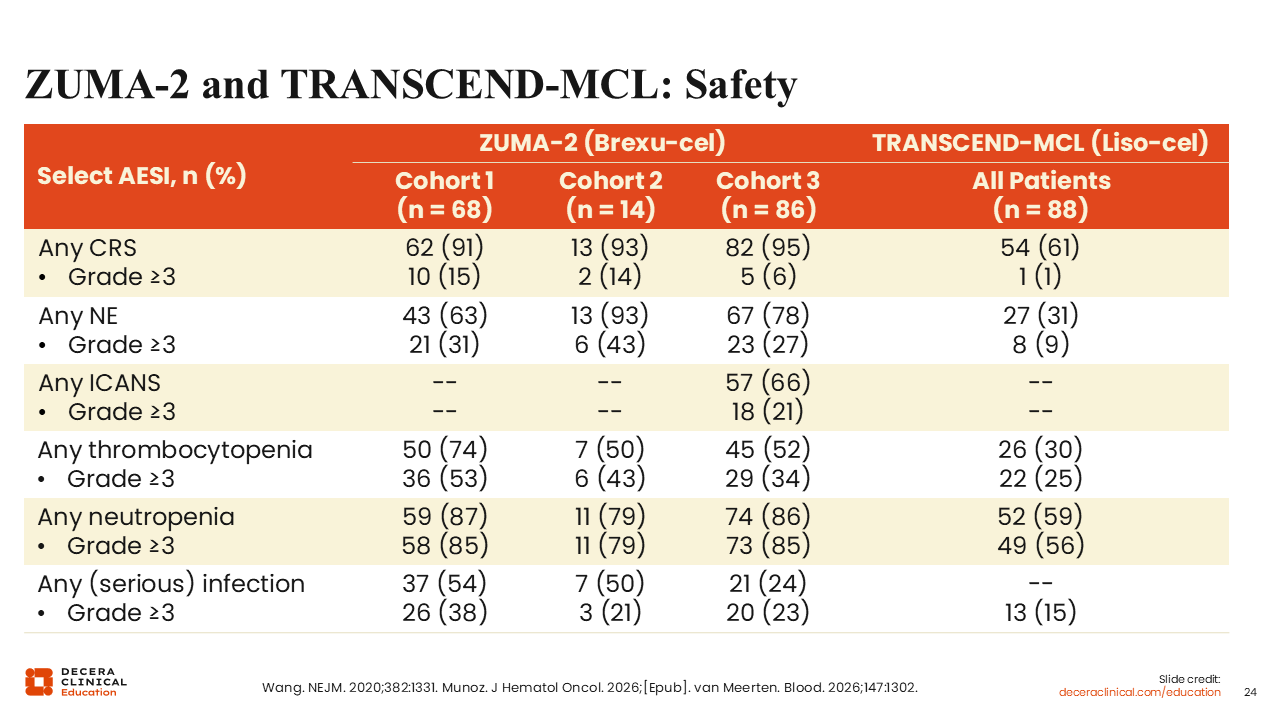
In terms of safety, the AEs of special interests associated with brexucabtagene autoleucel and lisocabtagene maraleucel include cytokine release syndrome (CRS), neurologic events, immune effector cell–associated neurotoxicity syndrome (ICANS), cytopenias, and infection.28,30,31 Most cases of these AEs were low grade. CRS and ICANS can be appropriately mitigated and managed with the use of tocilizumab and/or corticosteroids. One clear difference between these 2 CAR T-cell products is the lower frequency of grade 3/4 ICANS with lisocabtagene maraleucel.
BRUIN (MCL Population): Responses and AEs in R/R MCL
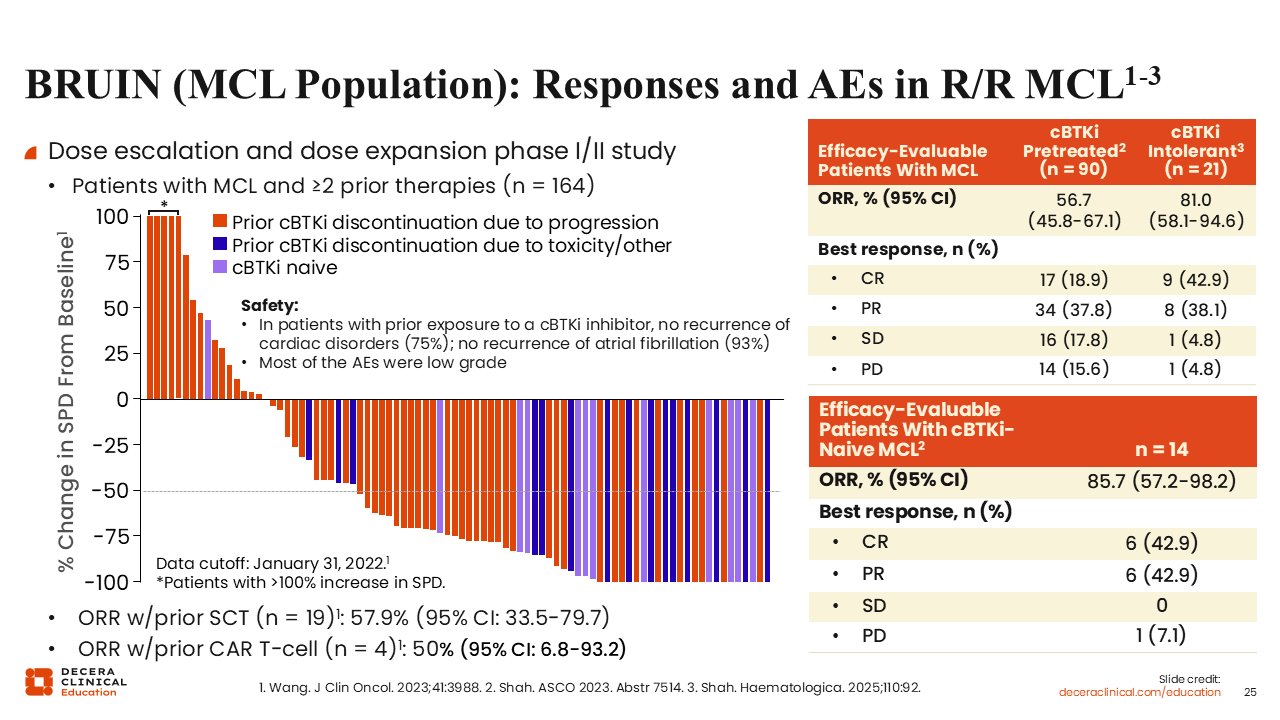
In the European Union, the EMA’s approval of pirtobrutinib in MCL was based on the results of the single-arm phase I/II BRUIN trial that investigated pirtobrutinib monotherapy in adult patients with MCL after previous exposure to ≥2 lines of therapy including a covalent BTK inhibitor (NCT03740529).33 The primary endpoints for the phase I portion of the BRUIN trial were the maximum tolerated dose and the recommended phase II dose, and for the phase II portion, the primary endpoint was ORR. The secondary endpoints included safety, pharmacokinetics, response, and survival.
Most patients with R/R MCL achieved tumor regression with pirtobrutinib.21,34 The ORR among 19 patients who had previously undergone SCT was approximately 60%, and among 4 patients who had previously received CAR T-cell therapy, the ORR was 50%. Of interest, among 90 efficacy evaluable patients who had previously received a covalent BTK inhibitor, the ORR was 56.7% (CR: 18.9%). Among 21 patients with covalent BTK inhibitor intolerance, the ORR was 81.0% (CR: 42.9%). In the small group of 14 patients without any prior exposure to a covalent BTK inhibitor, the ORR was 85.7% (CR: 42.9%).
In patients with prior exposure to a covalent BTK inhibitor, there was no recurrence of cardiac disorders in 75% and no recurrence of atrial fibrillation in 93%.34 Of note, most of the AEs were low grade. Overall, pirtobrutinib was safe and well tolerated in patients with prior BTK inhibitor intolerance.
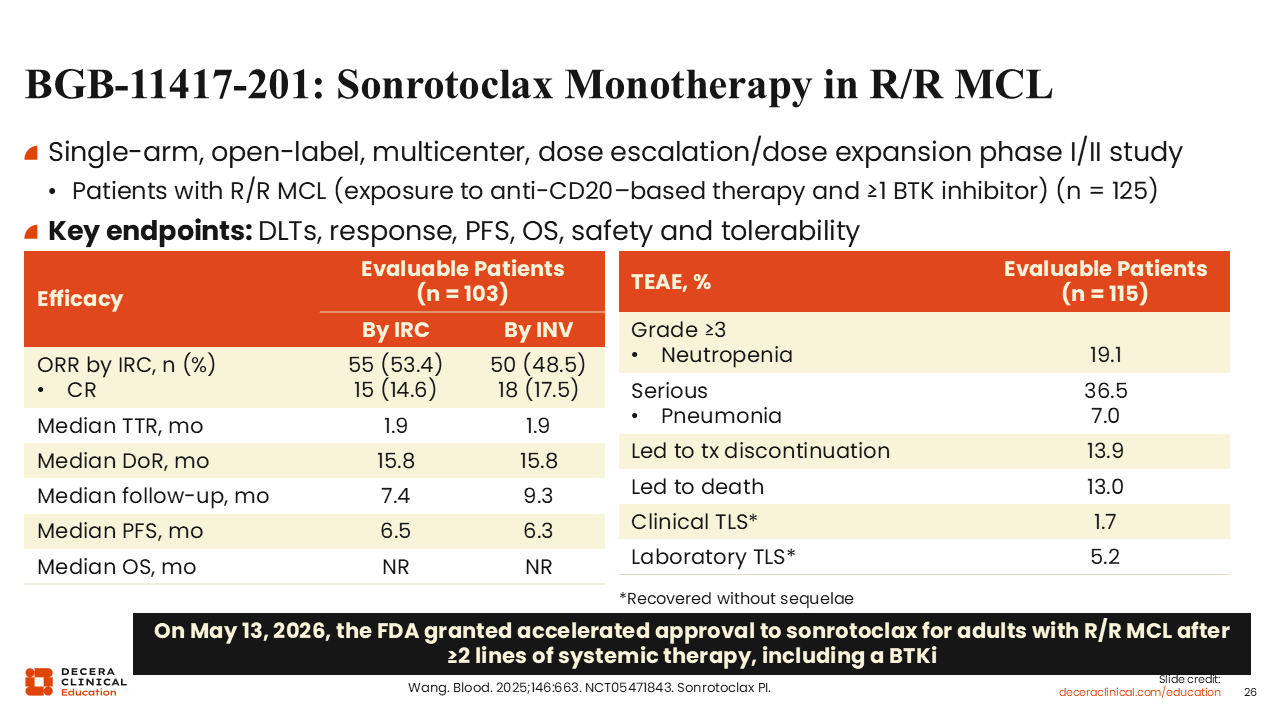
BGB-11417-201: Sonrotoclax Monotherapy in R/R MCL
Another novel agent in the treatment landscape for patients with R/R MCL is sonrotoclax, a next-generation, highly selective, and orally bioavailable BCL2 inhibitor. Sonrotoclax was investigated in the single-arm phase I/II BGB-11417-201 study for patients with R/R MCL, including an anti-CD20–based therapy and ≥1 covalent or noncovalent BTK inhibitor (NCT05471843). Preliminary analysis of data from this trial demonstrated an ORR of 53.4% by IRC, including a CR rate of 15%.35 The median duration of response was 15.8 months, the median PFS was 6.5 months, and the median OS has not yet been reached.
The treatment-emergent AEs included grade ≥3 neutropenia, which was reported in approximately 20% of patients. Serious treatment-emergent AEs were reported in 36.5% of patients, and this included pneumonia (7%). The incidence of clinical tumor lysis syndrome was 1.7% and the incidence of laboratory tumor lysis syndrome was 5.2%. Treatment-emergent AEs that led to treatment discontinuation were reported in 13.9%, and treatment-emergent AEs led to death in 13.0% of the patients.
Based on these results, the FDA granted accelerated approval to sonrotoclax for adult patients with R/R MCL after ≥2 lines of systemic therapy including a BTK inhibitor on May 13, 2026.36 In the European Union, however, sonrotoclax has not yet received EMA approval for use in patients with MCL.
Of interest, the randomized phase III CELESTIAL-RRMCL trial is investigating the efficacy and safety of sonrotoclax in combination with zanubrutinib vs placebo plus zanubrutinib for patients with R/R MCL (NCT06742996).
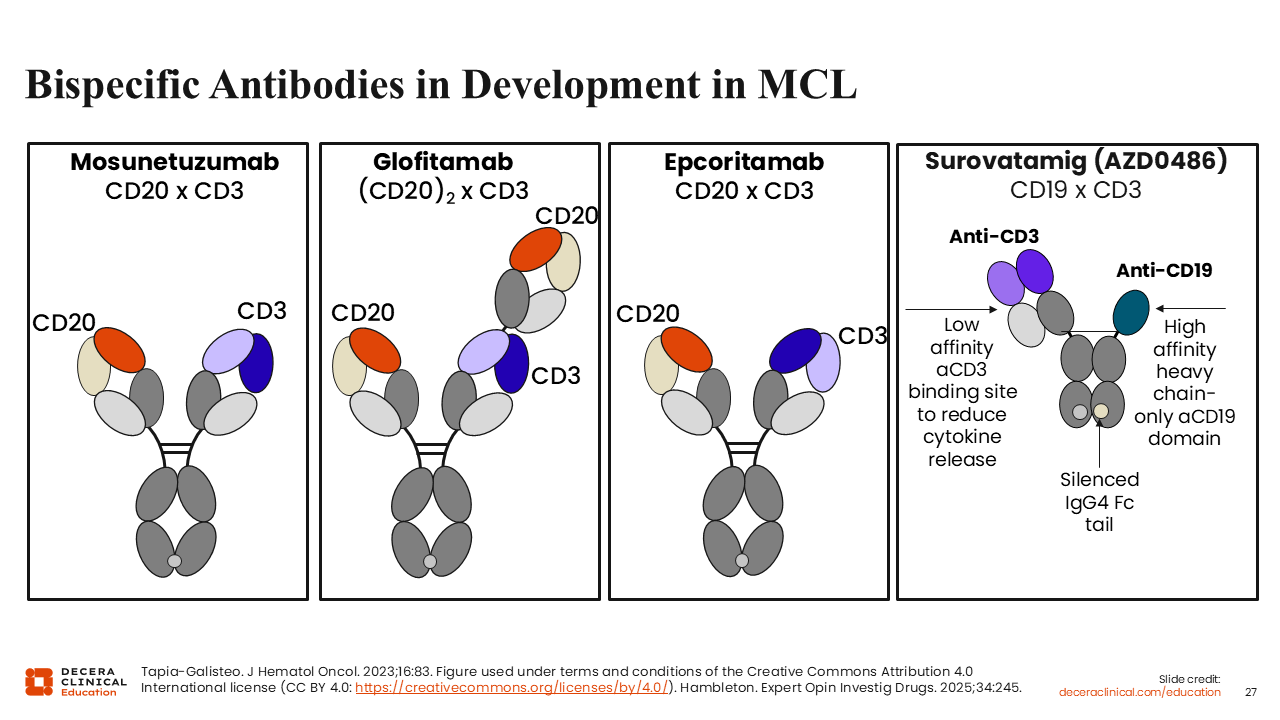
Bispecific Antibodies in Development in MCL
Finally, T-cell–directed bispecific antibodies, an emerging class of agents, have promising activity in patients with R/R MCL. Mosunetuzumab, glofitamab, and epcoritamab are bispecific antibodies with EMA approval for use in follicular lymphoma and/or diffuse large B-cell lymphoma. However, none of these agents has received approval for use in MCL. All 3 bispecific antibodies bind to CD20 and CD3 on T-cells.37
Surovatamig (AZD0486) is another bispecific antibody that is investigational in the clinical pipeline in MCL.38 Unlike mosunetuzumab, glofitamab, and epcoritamab, surovatamig binds to CD19 and CD3 on T-cells. Among these 4 bispecific antibodies, glofitamab is furthest along in clinical development in MCL. An important distinguishing factor is that glofitamab has a 2:1 tumor T-cell–binding configuration, whereas mosunetuzumab, epcoritamab, and surovatamig have 1:1 binding configuration.
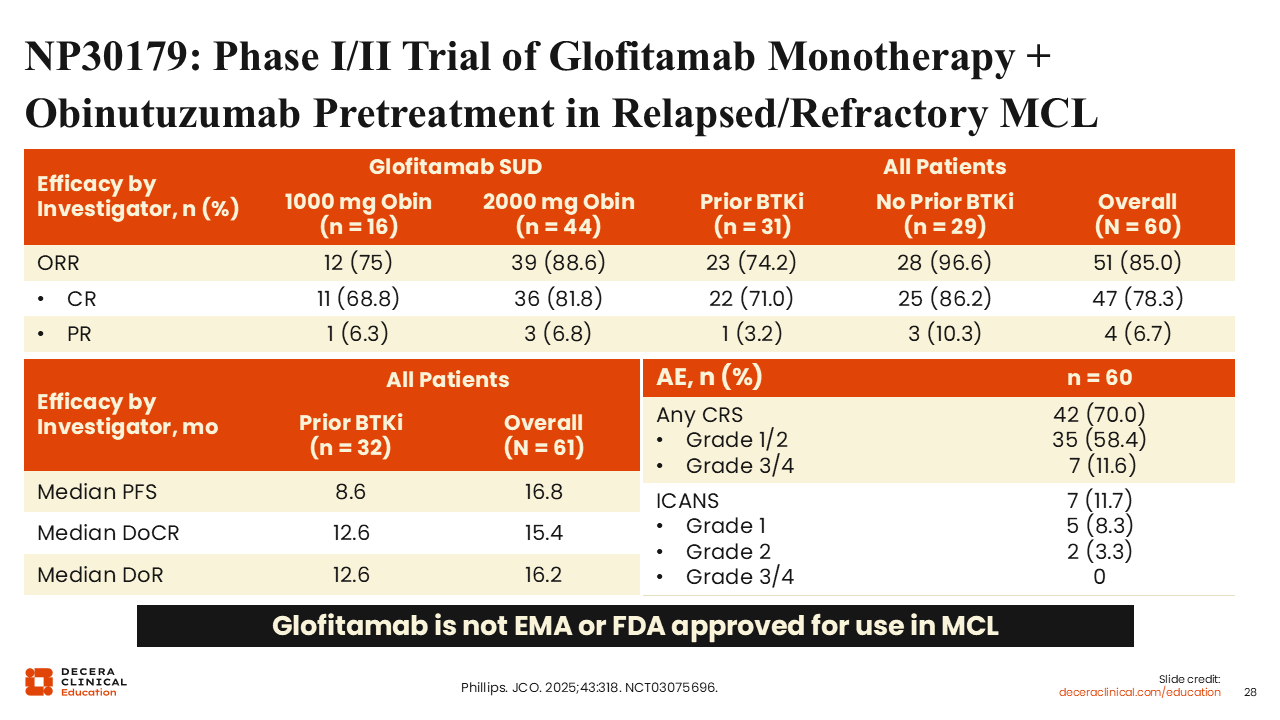
NP30179: Phase I/II Trial of Glofitamab Monotherapy + Obinutuzumab Pretreatment in Relapsed/Refractory MCL
The phase I/II NP30179 trial investigated the efficacy and safety of escalating doses of glofitamab as a single agent after a fixed, single dose of obinutuzumab pretreatment in patients with R/R B-cell NHL (NCT03075696).39 Step-up glofitamab dosing was administered once daily on Day 8 (2.5 mg) and Day 15 (10 mg) of cycle 1, with a target dose of 16 or 30 mg once every 3 weeks from Day 1 of cycle 2 onward, for a total of 12 cycles. The median number of previous therapies was 2 (range: 1-5). Among 60 evaluable patients, the ORR was 85.0%, including a CR rate of 78.3%. Among patients without previous exposure to a BTK inhibitor, the ORR was 74.2%, including a CR rate of 71.0%. After glofitamab administration, CRS was reported in 70% of the patients, and most were grade 1/2 (70%). Grade 1/2 ICANs occurred in 11.7% of the patients without any reported grade 3/4 ICANS.
As of May 2026, glofitamab is not approved for use in MCL by the EMA or FDA. However, the randomized phase III GLOBRYTE trial is investigating glofitamab monotherapy vs investigator’s choice of BR or rituximab plus lenalidomide for patients with R/R MCL who have received ≥1 line of prior systemic therapy, including a BTK inhibitor and an additional systemic therapy (NCT06084936).
Other Key Ongoing Trials of Bispecific Antibodies in MCL
There are several ongoing early-phase trials of glofitamab-based treatment approaches in MCL. For instance, there is a single-arm phase II trial that is evaluating glofitamab in combination with lenalidomide in high-risk R/R MCL (NCT07460362). The phase II GOLD trial is assessing glofitamab for patients with MCL with inadequate response or treatment relapse after receiving CAR T-cell therapy (NCT07453095). A phase II trial is investigating glofitamab in combination with pirtobrutinib and obinutuzumab in R/R MCL (NCT06252675). Another phase II trial (GOlDiLOX) is investigating glofitamab plus pirtobrutinib in patients with R/R MCL after prior exposure to a BTK inhibitor (NCT05833763). In addition, the phase II GLOASIS trial is investigating glofitamab plus venetoclax with or without zanubrutinib for patients with newly diagnosed or R/R high-risk MCL (NCT06558604).
A phase I/II trial is investigating the efficacy and safety of mosunetuzumab plus the antibody–drug conjugate polatuzumab vedotin for patients with B-cell NHL (NCT03671018). Epcoritamab is being investigated in a phase I/II trial in combination with antineoplastic agents in NHL (NCT05283720). Finally, a phase I/II trial is evaluating surovatamig alone or in combination with other anticancer agents for patients with mature B-cell malignancies (NCT06564038).