
CE / CME
Optimizing Mantle Cell Lymphoma Care: Case-Based Guidance From EU Experts
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
European Learners: 1.00 EBAC® CE Credit
Released: May 29, 2026
Expiration: November 28, 2026

Activity
Case Study: Individualized Upfront Treatment of a Patient With MCL Requiring Frontline Therapy
Regarding the frontline treatment of patients with MCL, I will start with a 70-year-old man with uncontrolled hypertension, atrial fibrillation, and diabetes who is newly diagnosed with a classical subtype of MCL. The initial staging revealed stage III disease involving lymph nodes in the neck and abdomen. The largest lymph node was 4 cm in size. A tissue biopsy revealed Ki-67 score of 40%. Genetic analysis showed that the disease was TP53 mutation negative.
Considering the patient’s age and level of fitness, he is not an ideal candidate for an aggressive or intensive chemotherapy regimen containing high-dose cytarabine as first-line therapy. He is better suited to receive a less intensive chemotherapy regimen such as BR or bortezomib/rituximab plus cyclophosphamide/doxorubicin/prednisone (VR-CAP). However, because of the patient’s existing comorbidities, a BR-based regimen is my preferred treatment choice.
Decera Clinical Education has developed an Interactive Decision Support Tool, which can be found here and used to access first-line treatment recommendations from 5 EU experts for patients with newly diagnosed MCL based on multiple disease characteristics, including the presence or absence of high-risk features and/or comorbidities, age at diagnosis, and the level of fitness.
EHA-EU MCL Network Guidelines: Untreated MCL
Now, I will review the frontline treatment guidelines in the European Union.
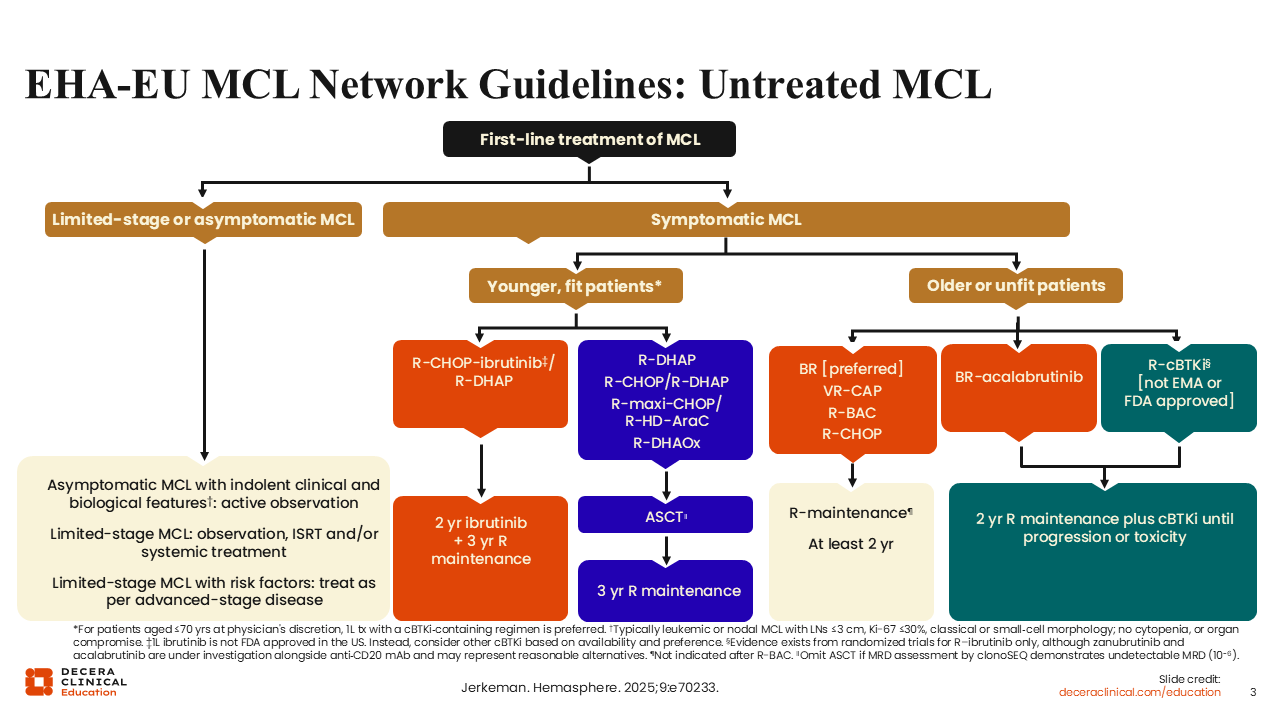
Recently, the guidelines for patients with MCL were updated by the European Hematology Association (EHA) and the European MCL Network.5 For patients who are newly diagnosed with asymptomatic MCL with indolent clinical and biologic features, the recommendation is for a watch-and-wait approach only. For those with limited-stage MCL (with stage I disease), the recommendation is for observation, involved site radiation therapy, and/or systemic treatment. For cases of limited-stage MCL with risk factors, the recommendation is to treat as if the patient had advanced-stage disease.
If the patient is diagnosed with symptomatic MCL, which is the more common type of presentation, treatment should be based on the patient’s age and level of fitness. Treatment options for younger, fit patients who are newly diagnosed with MCL are dependent on the availability of covalent BTK inhibitors in the frontline setting. Treatment in this setting involves the use of a CIT backbone with or without an EMA-approved covalent BTK inhibitor. As of May 2026, in the European Union, ibrutinib is approved by the EMA for younger fit patients in this setting. The choice of CIT backbones includes R-CHOP, R-DHAP, and rituximab plus dexamethasone/cytarabine/oxaliplatin with or without ASCT followed by maintenance therapy.
For older or unfit patients with symptomatic MCL, treatment recommendations include CIT with or without an EMA-approved covalent BTK inhibitor followed by maintenance therapy. In this setting, the potential CIT regimens include BR, VR-CAP, rituximab plus bendamustine/cytarabine, and R-CHOP. For older or unfit patients, the combination of a covalent BTK inhibitor with rituximab is not yet approved by the EMA as initial therapy.
Regarding younger patients newly diagnosed with MCL, there are still numerous unmet clinical needs, especially when treatment involves patients with biologically high-risk disease, including disease with blastoid histology, high proliferation rate, and of most importance, TP53 mutation–positive disease. For these patients, there is no consensus on what the best treatment approach should entail. Fortunately, there are several new and evolving drug classes and treatment combinations under development for patients who fall under this high-risk category. The emerging novel agents include CAR T-cell therapies, BTK inhibitor–based strategies, bispecific antibodies and BCL2 inhibitors.
Next, I explain in more detail the available evidence guiding treatment decision-making for patients who are newly diagnosed with MCL.
TRIANGLE: Randomized Phase III Trial of ASCT After Rituximab/Ibrutinib/Ara-C Induction in MCL
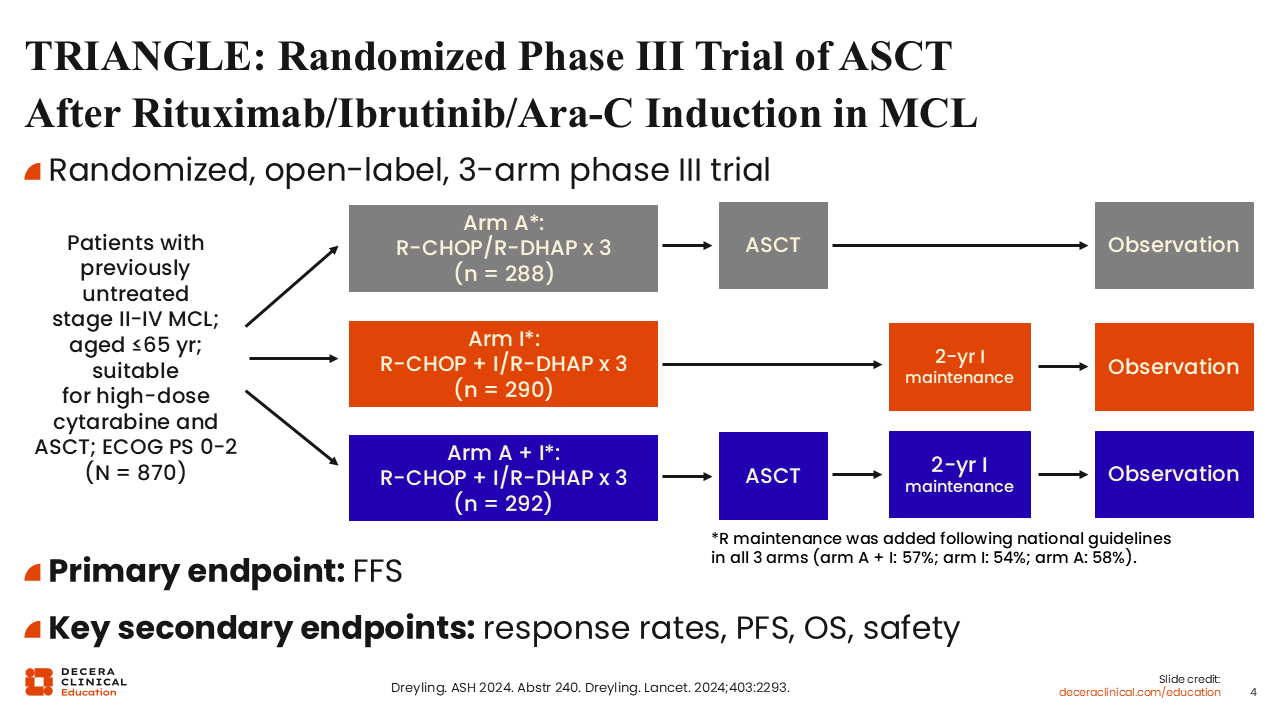
Covalent BTK inhibitors are very important in the treatment of MCL. Ibrutinib is a first-in-class covalent BTK inhibitor that revolutionized the treatment of hematologic malignancies. TRIANGLE is an important randomized, 3-arm phase III trial that investigated alternating R-CHOP/R-DHAP with or without ibrutinib.3 This trial was conducted by the European MCL Network. There were 2 ibrutinib-containing arms; patients on one of these arms received ASCT (Arm A + I) and patients on the other ibrutinib-containing arm did not receive ASCT (Arm I). On both ibrutinib-containing arms, treatment with or without ASCT was followed by 2 years of ibrutinib maintenance therapy. Rituximab maintenance could be given, according to national guidelines in all responding patients regardless of treatment arm. On the trial, 870 patients aged 65 years or younger with previously untreated stage II-IV MCL who are ASCT eligible and suitable to receive treatment with high-dose cytarabine were enrolled.
The primary endpoint was failure-free survival (FFS), and the secondary endpoints included response rates, PFS, overall survival (OS), and safety.
TRIANGLE: 4-Year FFS and 4-Year OS
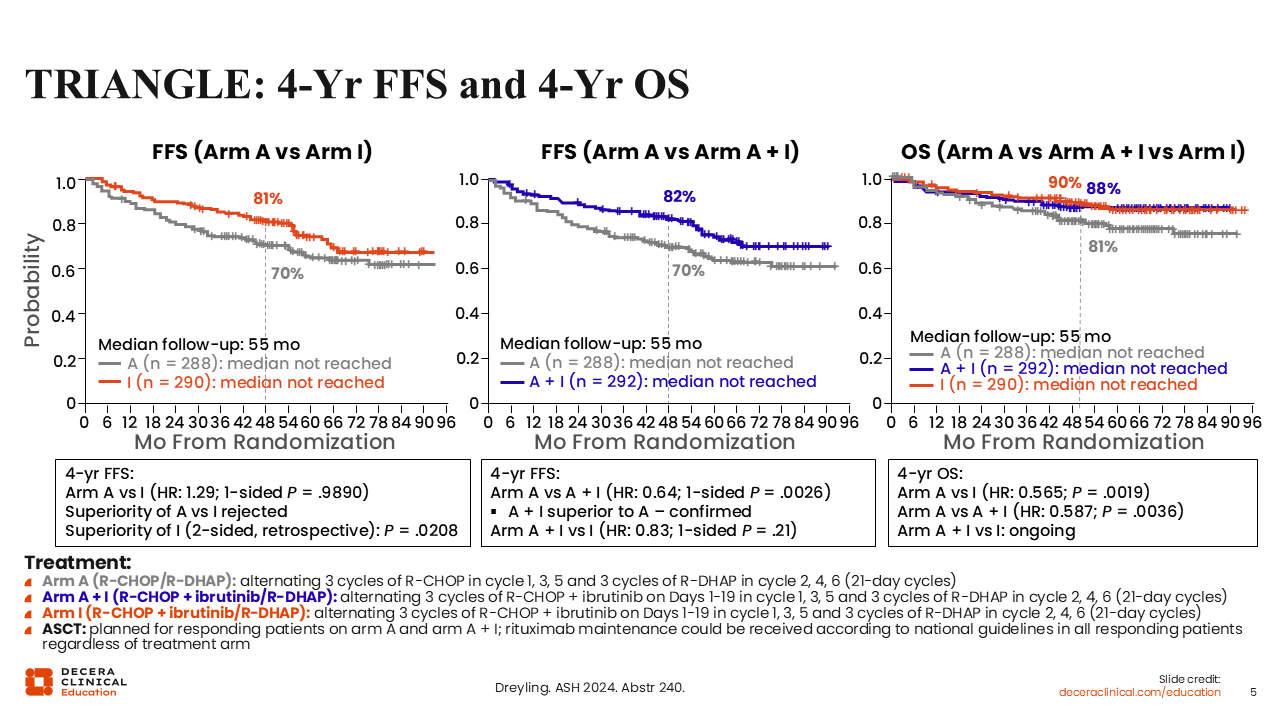
After a median follow-up of 55 months, TRIANGLE demonstrated the superiority of CIT plus ibrutinib with ASCT (Arm A + I) vs standard CIT alone (without ibrutinib) followed by ASCT (Arm A) regarding both the 4-year FFS rates (82% vs 70%, respectively; HR: 0.64; P = .0026) and the 4-year OS rates (88% vs 81%, respectively; HR: 0.587; P = .0036). The 4-year FFS rates demonstrated that Arm A + I was not superior to Arm I in which patients received CIT plus ibrutinib without ASCT (82% vs 81%; HR: 0.83; P = .21). In addition, after a median follow-up of 55 months, the FFS superiority of Arm A to Arm I was not confirmed (70% vs 81%; HR: 1.29; P = .9890). In terms of OS, the results demonstrated the superiority of Arm I and Arm A + I vs Arm A (90% vs 88% vs 81%, respectively). These results confirm the superiority of adding ibrutinib to CIT without ASCT (Arm I) over ASCT-containing treatment without ibrutinib (Arm A) regarding both FFS and OS.
Of importance, the lack of a difference in OS between Arm I and Arm A + I indicates that ASCT is no longer required for younger patients (aged 65 years or younger) with MCL if ibrutinib, a covalent BTK inhibitor, is added in the induction phase and maintenance therapy includes rituximab and 2 years of ibrutinib. Therefore, Arm I is the current standard of care for younger patients with MCL.
In my clinical practice, I would consider using this regimen for younger, fit patients with previously untreated MCL up to approximately 70 years of age.
ECHO: BR With or Without Acalabrutinib for Previously Untreated MCL
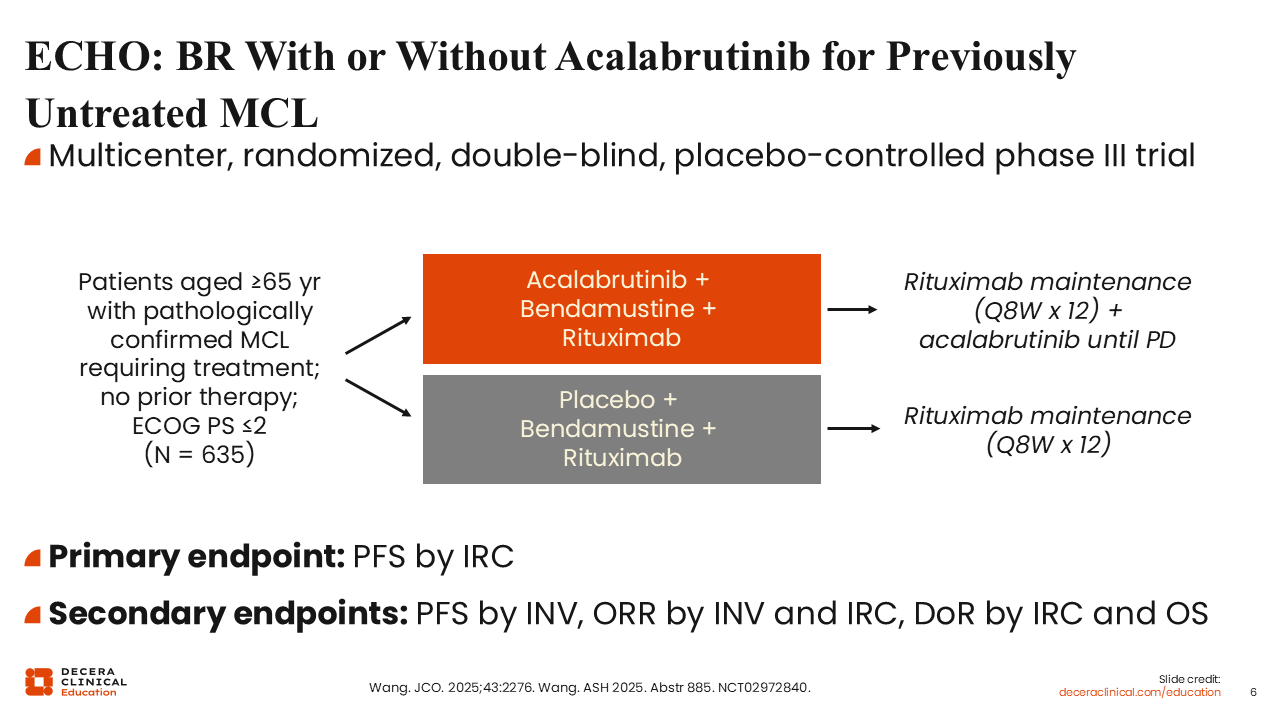
Of importance, the second-generation covalent BTK inhibitors acalabrutinib and zanubrutinib are more selective for BTK than the first-generation covalent BTK inhibitor ibrutinib. Another important randomized trial for the frontline treatment of patients with MCL is the phase III ECHO trial (NCT02972840). Compared with the TRIANGLE trial, ECHO investigated acalabrutinib plus BR vs placebo plus BR in an older population of patients with MCL. On the ECHO trial, 635 patients aged 65 years or older with previously untreated MCL who were ineligible for ASCT were randomly assigned to receive treatment.7 Acalabrutinib or placebo was given until disease progression or unacceptable toxicity. On both arms, maintenance rituximab was administered for 2 years in patients who achieved complete response (CR)/partial response (PR) to induction therapy. Of note, crossover from the placebo arm to the acalabrutinib arm was allowed after disease progression.
The primary endpoint was PFS by independent review committee (IRC), and the secondary endpoints included ORR, OS, and safety.
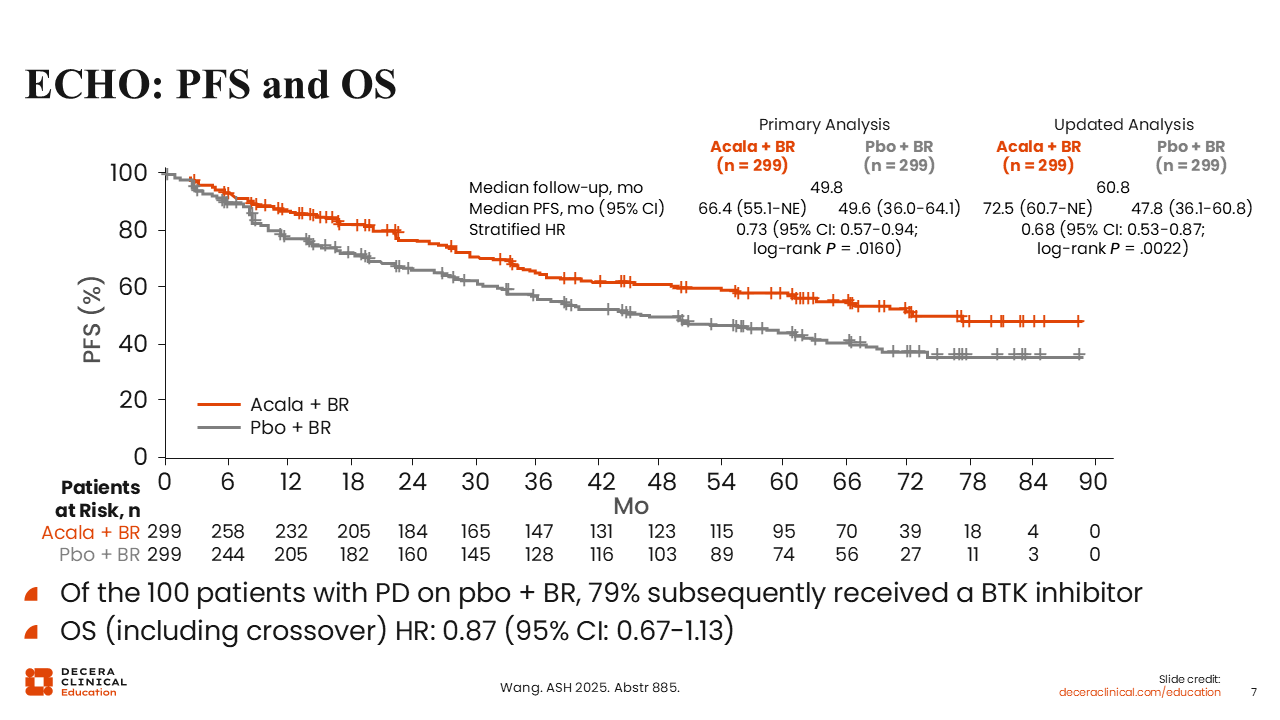
ECHO: PFS and OS
The ECHO trial showed a clear advantage in terms of PFS with the addition of acalabrutinib to BR. After a median follow-up of 60.8 months, the median PFS on the acalabrutinib plus BR arm was 72.5 months vs 47.8 months on the placebo plus BR arm (HR: 0.68; 95% CI: 0.53-0.87; P = .0022). Among the 100 patients with disease progression on the placebo plus BR arm, 79% subsequently received a BTK inhibitor.
At the time of data analysis, the OS data were immature, but there was a trend toward an OS advantage on the acalabrutinib-containing arm despite the inclusion of patients who crossed over to the acalabrutinib arm after experiencing disease progression on the placebo arm (HR: 0.87; 95% CI: 0.67-1.13).
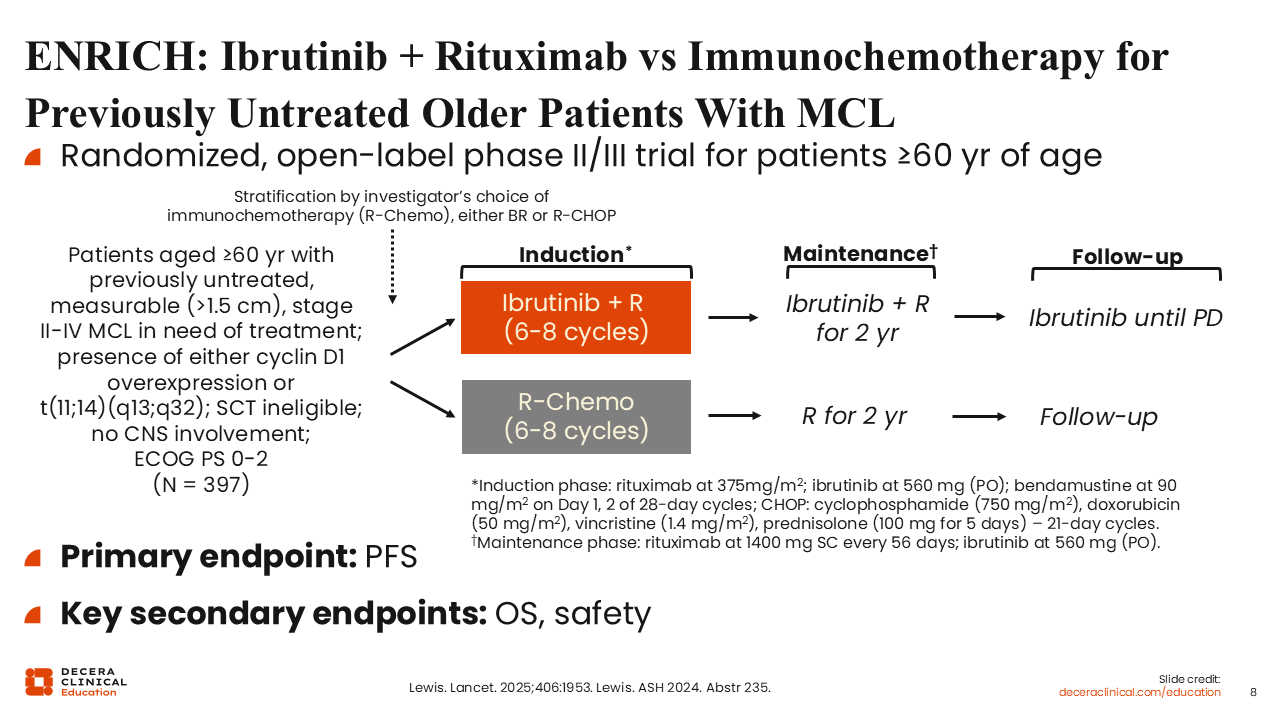
ENRICH: Ibrutinib + Rituximab vs Immunochemotherapy for Previously Untreated Older Patients With MCL
ENRICH is another important trial for an older patient population. The phase III ENRICH trial was conducted for SCT-ineligible patients aged 60 years or older with previously untreated, measurable, stage II-IV MCL harboring either cyclin D1 overexpression or t(11;14)(q13;q32) without any central nervous system involvement.8 Patients were stratified by investigator’s choice of R-CHOP or BR. Thereafter, patients were randomly assigned to receive either ibrutinib plus rituximab or rituximab-based chemotherapy. Those who received ibrutinib plus rituximab as induction therapy also received maintenance ibrutinib plus rituximab for 2 years, and those on the rituximab-based chemotherapy arm received maintenance rituximab for 2 years. In total, 397 patients were enrolled on the ENRICH trial.
The primary endpoint was PFS and the secondary endpoints included OS and safety. Of importance, ENRICH is the first trial to challenge the use of aggressive CIT for older patients with MCL in the frontline setting. It was conducted by the British Lymphoma Group in collaboration with the Nordic group.
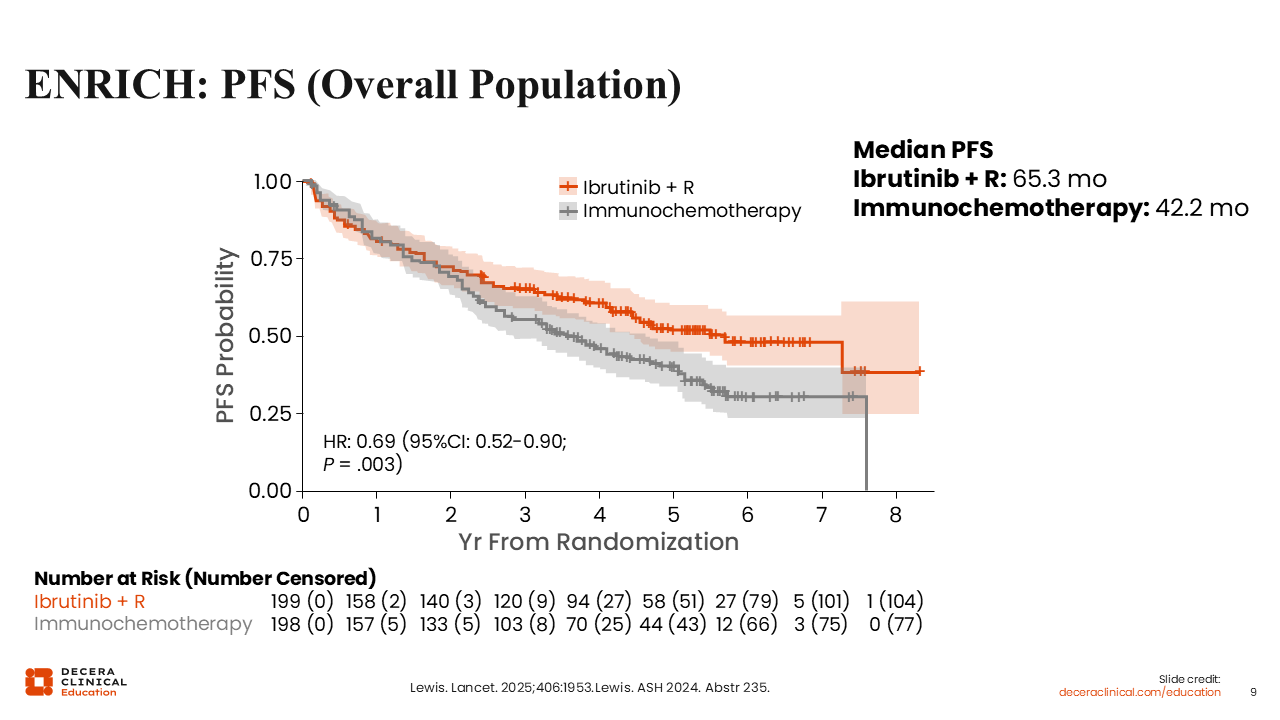
ENRICH: PFS (Overall Population)
In the overall patient population, the median PFS among patients who received ibrutinib plus rituximab was 65.3 months vs 42.2 months among those who received rituximab-based chemotherapy (HR: 0.69; 95% CI: 0.52-0.90; P = .003). This was a positive trial showing a clear advantage in terms of PFS for the covalent BTK inhibitor–based, chemotherapy-free regimen.
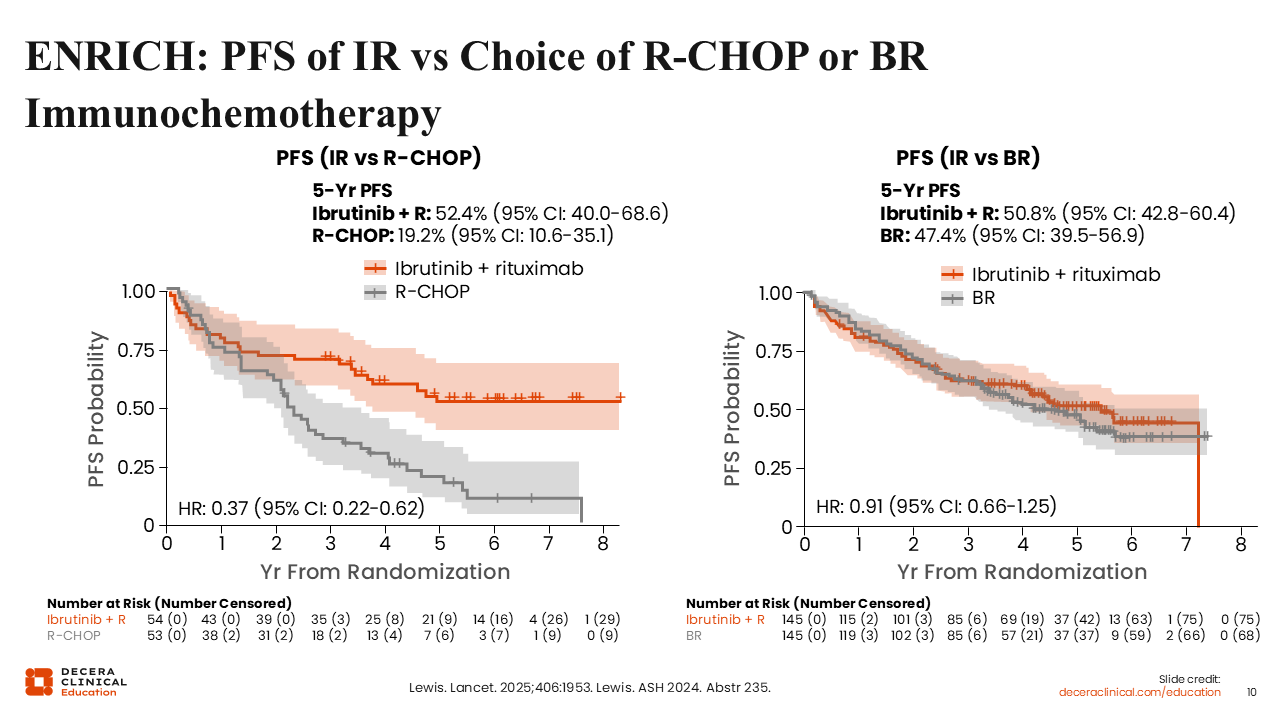
PFS of IR vs Choice of R-CHOP or BR Immunochemotherapy
Of interest, PFS benefit with the addition of ibrutinib was very dependent on the choice of CIT. The 5-year PFS among patients on the ibrutinib plus rituximab arm was 52.4% vs 19.2% for those who received R-CHOP (HR: 0.37; 95% CI: 0.22-0.62). Among those who received BR, the 5-year PFS was 47.4% vs 50.8% among those who received ibrutinib plus rituximab (HR: 0.91; 95% CI: 0.66-1.25). The PFS advantage of adding ibrutinib to rituximab was more evident when compared with R-CHOP, demonstrating that patients aged 60 years or older with MCL fare poorly when treated with R-CHOP compared with ibrutinib plus rituximab, a chemotherapy-free regimen, in the frontline setting. In all, R-CHOP is an inferior treatment option and one that should be avoided for older patients with MCL compared with ibrutinib plus rituximab or BR.
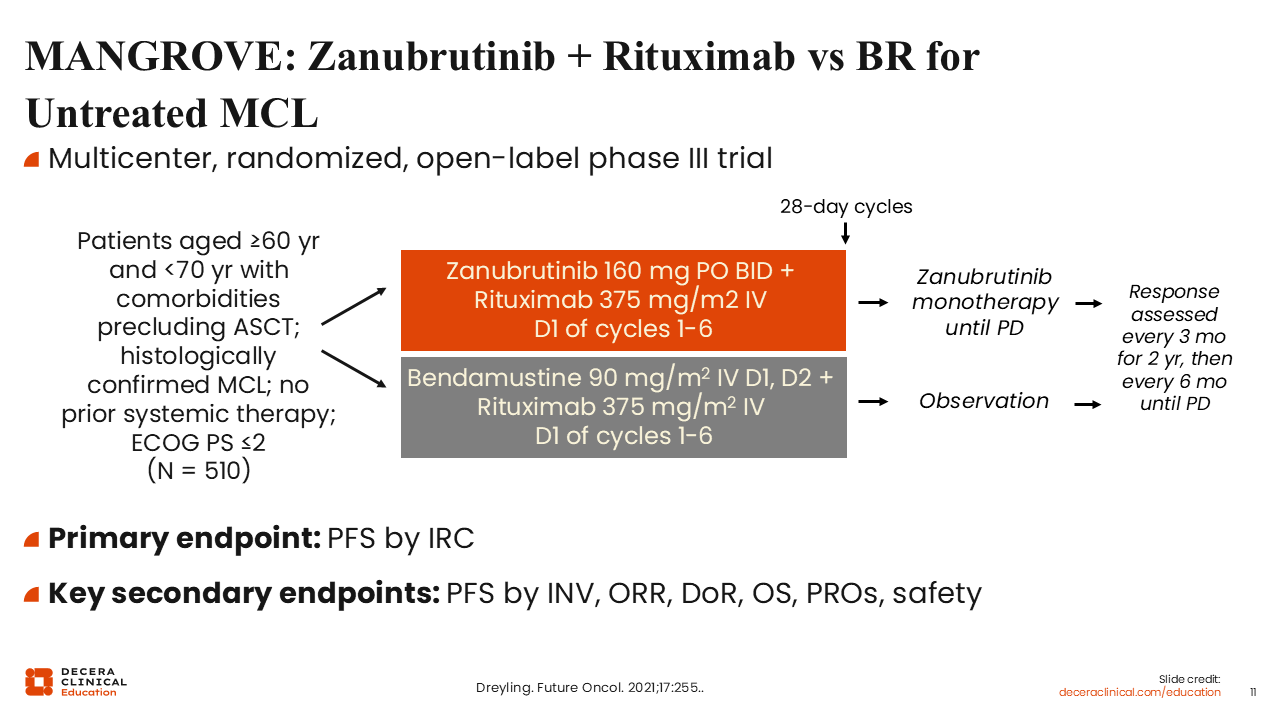
MANGROVE: Zanubrutinib + Rituximab vs BR for Untreated MCL
It is important to note that the ongoing randomized phase III MANGROVE trial is comparing the efficacy and safety of another covalent BTK inhibitor, zanubrutinib, in combination with rituximab vs BR for patients aged 60 years or older but younger than 70 years of age with MCL (NCT04002297). Patients must have preexisting comorbidities precluding ASCT.9 In total, 510 patients have been accrued on this trial. On the zanubrutinib-containing induction arm, patients will receive zanubrutinib monotherapy until disease progression.
The primary endpoint is PFS by IRC, and the secondary endpoints include investigator-assessed PFS, ORR, OS, and safety. We are awaiting the readout of this trial and hope the results will soon become available. The readouts from this trial are eagerly anticipated.
Other Investigational Combinations in Untreated MCL
Early results from the phase II TrAVeRse trial investigating the combination of acalabrutinib with venetoclax and rituximab in treatment-naive MCL showed encouraging activity and a manageable safety profile (NCT05951959).10 Alternating BR and rituximab/high-dose cytarabine is a regimen that was developed through a collaboration between Dana-Farber Cancer Institute and Washington University in St Louis as induction therapy prior to ASCT for transplant-eligible patients with MCL. This regimen led to high response rates and durable remissions (NCT01661881, NCT02728531).11 The ongoing, single-arm phase I/II MAVO trial is investigating the efficacy and safety of acalabrutinib plus venetoclax and obinutuzumab for patients with untreated or relapsed/refractory (R/R) MCL (NCT04855695). Early results from this trial demonstrated that the regimen is well tolerated and effective in R/R MCL, treatment-naive MCL, and those with TP53 mutation–positive disease.12 In addition, the single-arm OAsis trial examined ibrutinib in combination with venetoclax and obinutuzumab in patients with MCL, and the combination was well tolerated, yielding high response rates among patients with previously untreated and R/R MCL.13 Finally, the phase II BOVen trial is investigating zanubrutinib plus venetoclax and obinutuzumab in previously untreated patients with MCL. Among 25 patients with untreated MCL and a TP53 mutation, the best overall response rate was 96%, including a CR rate of 88%. More than 80% of the patients achieved undetectable measurable residual disease, and the PFS and OS rates at 2 years were 72% and 76%, respectively.14