CE / CME
Improving Outcomes With Immune Checkpoint Inhibitors for Solid Tumors
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 18, 2026
Expiration: December 17, 2026

Activity
IMscin001 Part 1: SC Atezolizumab in Patients With Locally Advanced or Metastatic NSCLC
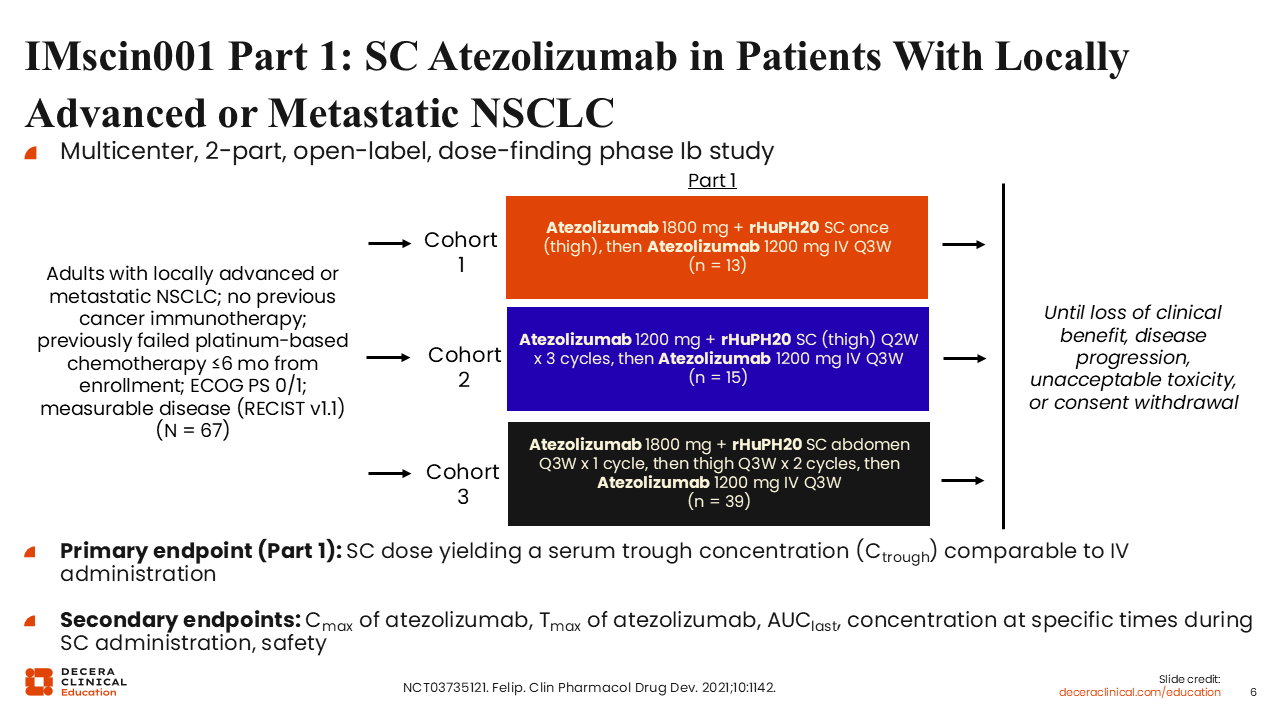
The multicenter, 2-part, open-label, dose-finding phase Ib IMSCIN001 study (NCT03735121) evaluated SC atezolizumab in adults with locally advanced or metastatic NSCLC who had not received previous cancer immunotherapy and had experienced progression following platinum-based chemotherapy within 6 months of enrollment.28
In part 1 of the study, patients were assigned to 1 of 3 SC administration cohorts designed to evaluate pharmacokinetic and pharmacodynamic characteristics of IV atezolizumab. In cohort 1, patients received atezolizumab 1800 mg plus rHuPH20 SC in the thigh once, followed by atezolizumab 1200 mg IV every 3 weeks (n = 13). In cohort 2, patients received atezolizumab 1200 mg plus rHuPH20 SC in the thigh every 2 weeks for 3 cycles, followed by atezolizumab 1200 mg IV every 3 weeks (n = 15). In cohort 3, patients received atezolizumab 1800 mg plus rHuPH20 SC in the abdomen every 3 weeks for 1 cycle, followed by thigh administration every 3 weeks for 2 cycles, and then transitioned to atezolizumab 1200 mg IV every 3 weeks (n = 39). Treatment continued until loss of clinical benefit, disease progression, unacceptable toxicity, or withdrawal of consent.
The primary endpoint for part 1 was the identification of the SC dose yielding a serum trough concentration comparable to IV administration. Secondary endpoints include atezolizumab Cmax, Tmax, AUClast, concentrations at specified time points during SC administration, and safety.
IMscin001 Part 1: Atezolizumab Serum Concentration Over Time and SC vs IV Ctrough (Primary Endpoint)
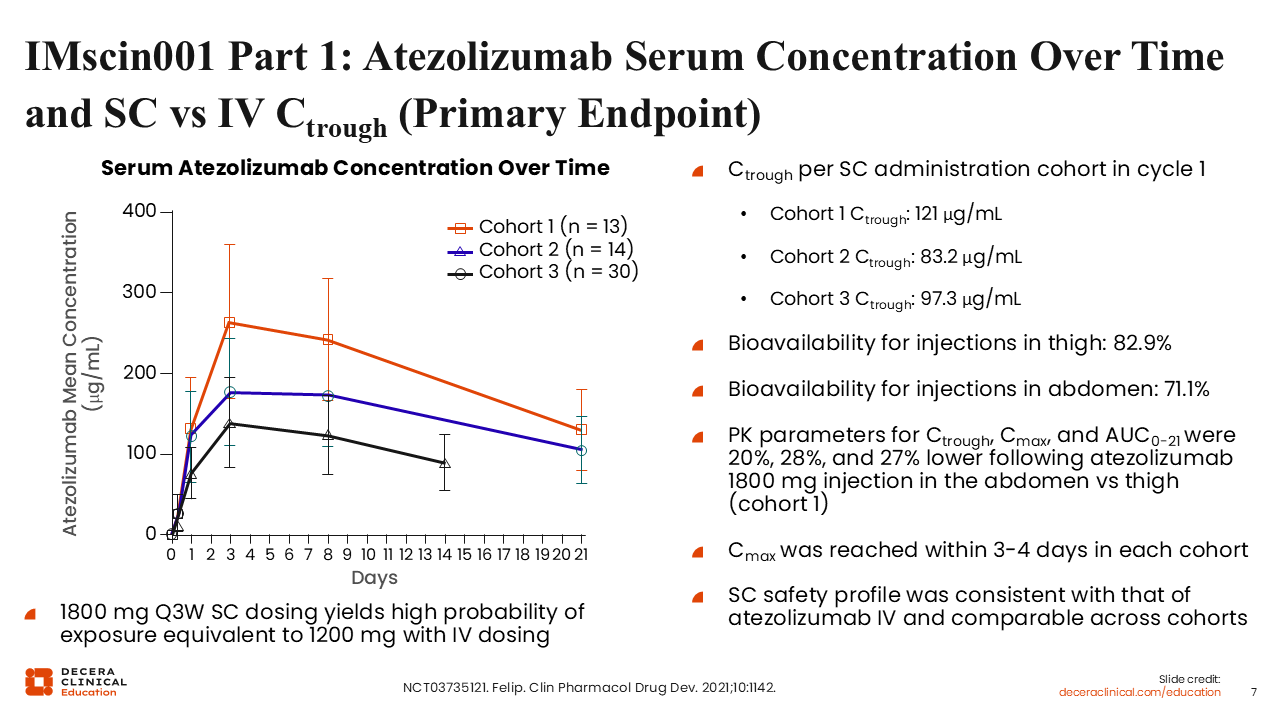
Atezolizumab serum exposure over time was generally comparable between the SC and IV formulations in IMscin001 Part 1. Across the 3 SC administration cohorts, Ctrough values in cycle 1 were in a similar range to those observed with IV atezolizumab, supporting comparable exposure. Bioavailability for thigh injections was 82.9%, and pharmacokinetic parameters for Cmax, Ctrough, AUC0-21d, and AUCinf were broadly consistent with that of atezolizumab IV. Based on these data, SC dosing provided exposure consistent with IV atezolizumab, with a high probability of exposure equivalence to 1200 mg IV every 3 weeks.
IMscin001 Part 2: SC vs IV Atezolizumab in Previously Treated LA or Metastatic NSCLC
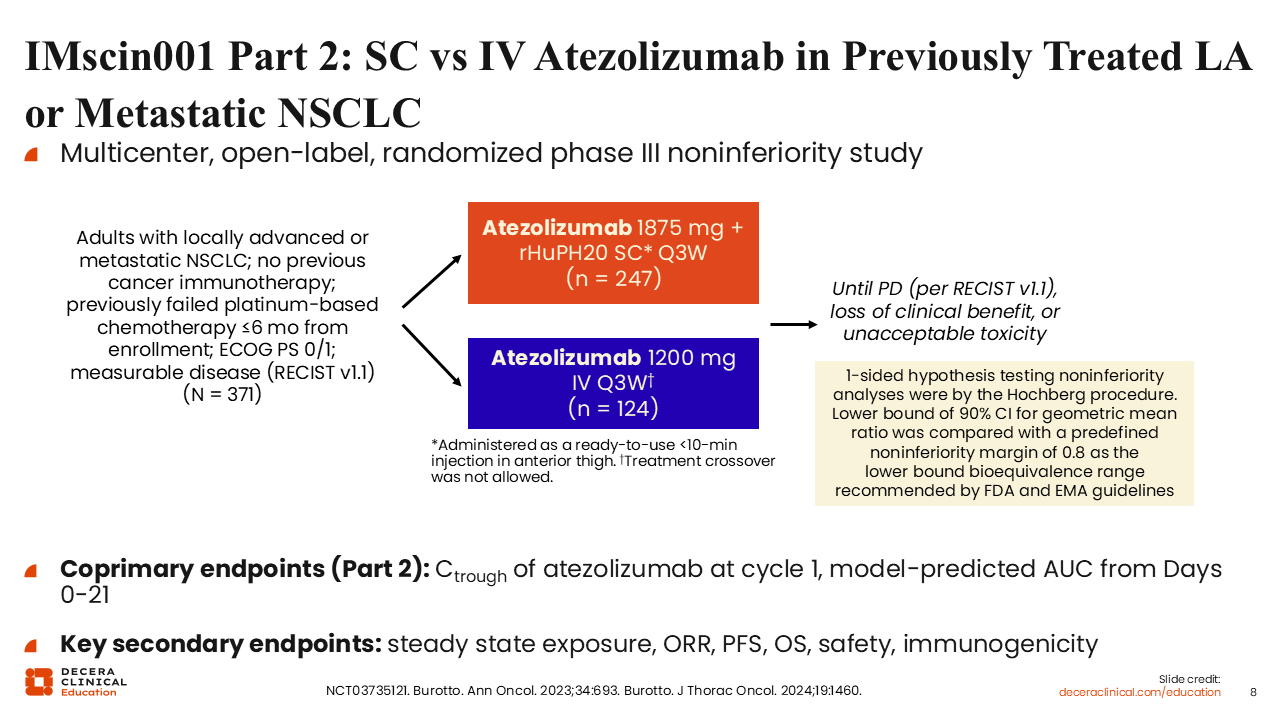
IMscin001 Part 2 was a multicenter, open-label, randomized phase III noninferiority study that compared SC with IV atezolizumab in adults with locally advanced or metastatic NSCLC (NCT03735121).29,30 Eligible patients had measurable disease per Response Evaluation Criteria in Solid Tumors (RECIST) v1.1, ECOG PS 0 or 1, no previous cancer immunotherapy, and prior failure of platinum-based chemotherapy within 6 months before enrollment. Patients were randomized to receive atezolizumab 1875 mg plus rHuPH20 SC every 3 weeks or atezolizumab 1200 mg IV every 3 weeks, with treatment continued until disease progression, loss of clinical benefit, or unacceptable toxicity; crossover was not allowed. The coprimary endpoints for part 2 were cycle 1 Ctrough and model-predicted AUC from Days 0-21 (AUC0-21), with key secondary endpoints including steady-state exposure, overall response rate (ORR), progression-free survival (PFS), overall survival (OS), safety, and immunogenicity.
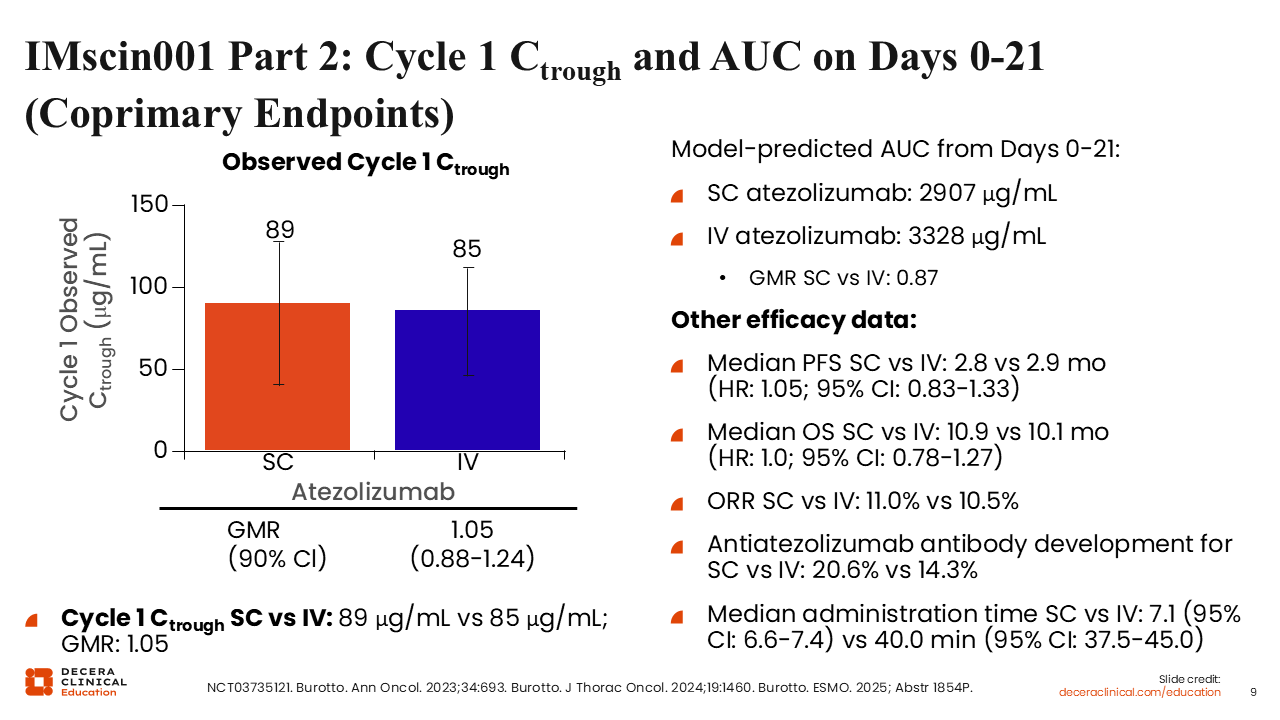
IMscin001 Part 2: Cycle 1 Ctrough and AUC on Days 0-21 (Coprimary Endpoints)
Investigators from the IMscin001 Part 2 study showed that cycle 1 atezolizumab exposure was comparable between the SC and IV formulations, with similar Ctrough and AUC0-21 values across treatment arms. Specifically, geometric mean cycle 1 Ctrough was 207 mcg/mL with SC atezolizumab vs 209 mcg/mL with IV atezolizumab, and model-predicted mean AUC0-21 was 307 vs 328 mcg/day/mL, supporting noninferior pharmacokinetic exposure with the SC formulation. Efficacy outcomes were also broadly similar for SC vs IV atezolizumab, with median PFS of 2.8 vs 2.9 months (HR: 1.05; 95% CI: 0.83-1.33), median OS of 10.9 vs 10.1 months (HR: 1.0; 95% CI: 0.78-1.27), and ORR of 11.0% vs 10.5%.
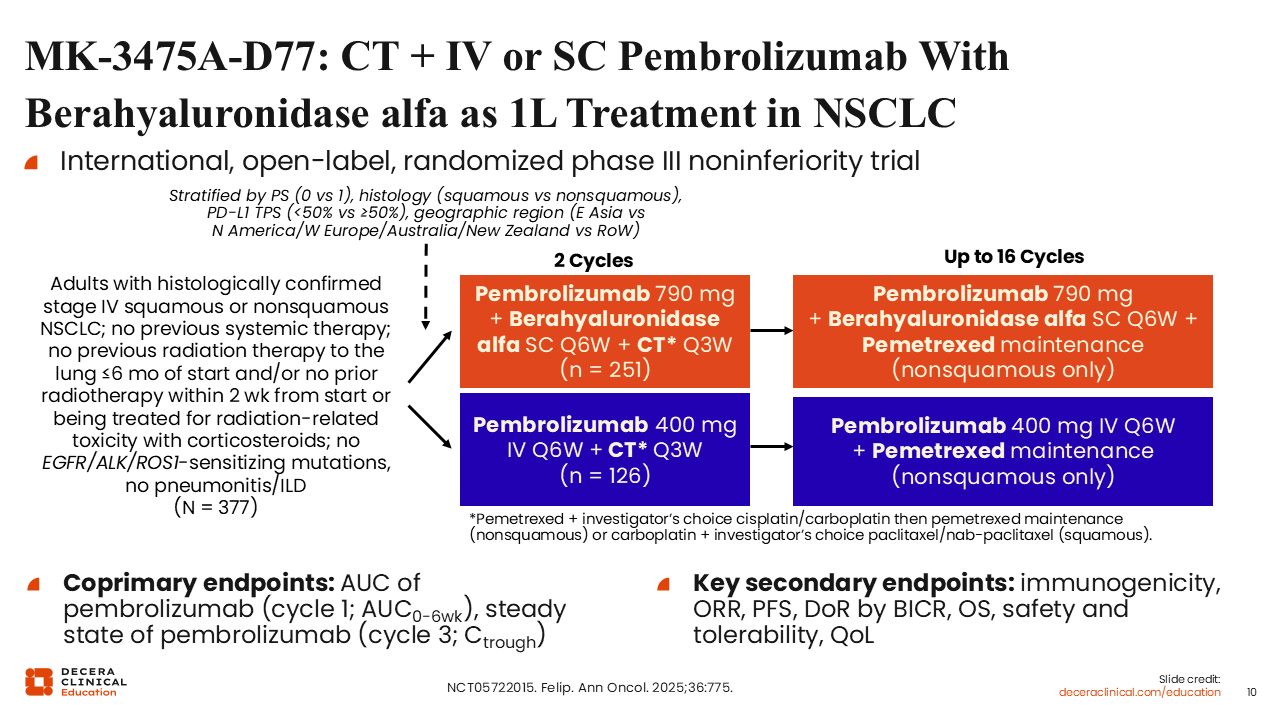
MK-3475A-D77: CT + IV or SC Pembrolizumab With Berahyaluronidase alfa as 1L Treatment in NSCLC
MK-3475A-D77 was an international, open-label, randomized phase III noninferiority trial that compared SC pembrolizumab plus berahyaluronidase alfa with IV pembrolizumab, each given with chemotherapy, as first-line treatment for advanced NSCLC.31 Eligible patients were adults with histologically confirmed stage IV squamous or nonsquamous NSCLC; no previous systemic therapy; no sensitizing EGFR, ALK, or ROS1 alterations; and no pneumonitis or ILD. Patients were randomized to receive pembrolizumab 790 mg plus berahyaluronidase alfa SC every 6 weeks or pembrolizumab 400 mg IV every 6 weeks, each with chemotherapy every 3 weeks for 2 cycles, followed by continued pembrolizumab for up to 16 cycles with pemetrexed maintenance in patients with nonsquamous disease. The coprimary endpoints were pembrolizumab AUC in cycle 1 and steady-state pembrolizumab Ctrough in cycle 3, with key secondary endpoints including immunogenicity, ORR, PFS, duration of response by blinded independent central review (BICR), OS, safety and tolerability, and quality of life.
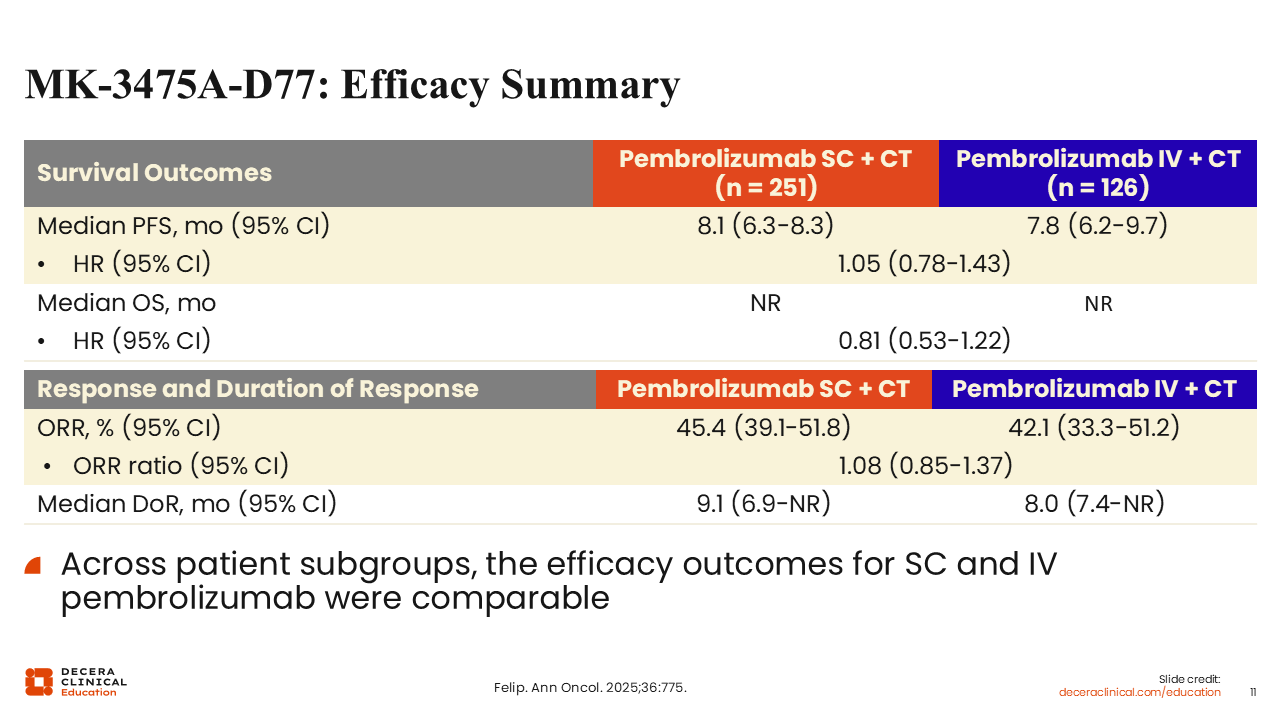
MK-3475A-D77: Efficacy Summary
Efficacy outcomes were broadly comparable between the SC and IV pembrolizumab formulations in MK-3475A-D77. Median PFS was 8.1 months with SC pembrolizumab plus chemotherapy vs 7.8 months with IV pembrolizumab plus chemotherapy (HR: 0.95; 95% CI: 0.69-1.30), and median OS was not reached in both arms (HR: 0.81; 95% CI: 0.51-1.22). ORR was also similar at 45.4% with SC pembrolizumab vs 42.1% with IV pembrolizumab, with disease control rates of 91.6% and 87.3%, respectively. Overall, these findings showed comparable efficacy across the SC and IV pembrolizumab arms.
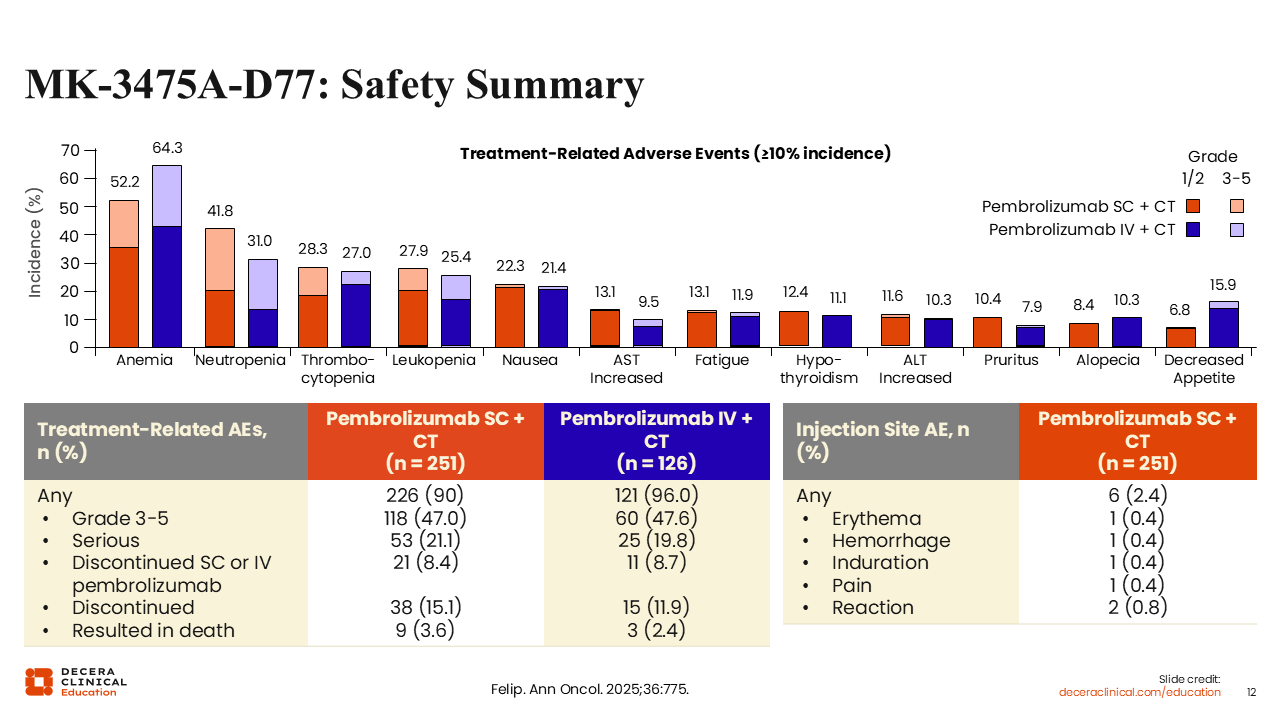
MK-3475A-D77: Safety Summary
Safety was generally comparable between the SC and IV pembrolizumab arms, with treatment-related AEs reported in 90.0% vs 96.0% of patients, grade 3-5 treatment-related AE in 47.0% vs 47.6%, and serious treatment-related AE in 21.1% vs 19.8%, respectively. Discontinuation of SC or IV pembrolizumab because of treatment-related AE occurred in 8.4% and 8.7% of patients, whereas discontinuation of any treatment occurred in 15.1% and 11.9%, and treatment-related AE resulting in death were reported in 3.6% and 2.4%, respectively.
Injection-site AEs with SC pembrolizumab were uncommon overall, occurring in 2.4% of patients, with individual events such as erythema, hemorrhage, induration, and pain each reported in 0.4% and injection-site reaction in 0.8%. Overall, these findings supported a broadly similar safety profile for the SC and IV pembrolizumab formulations.
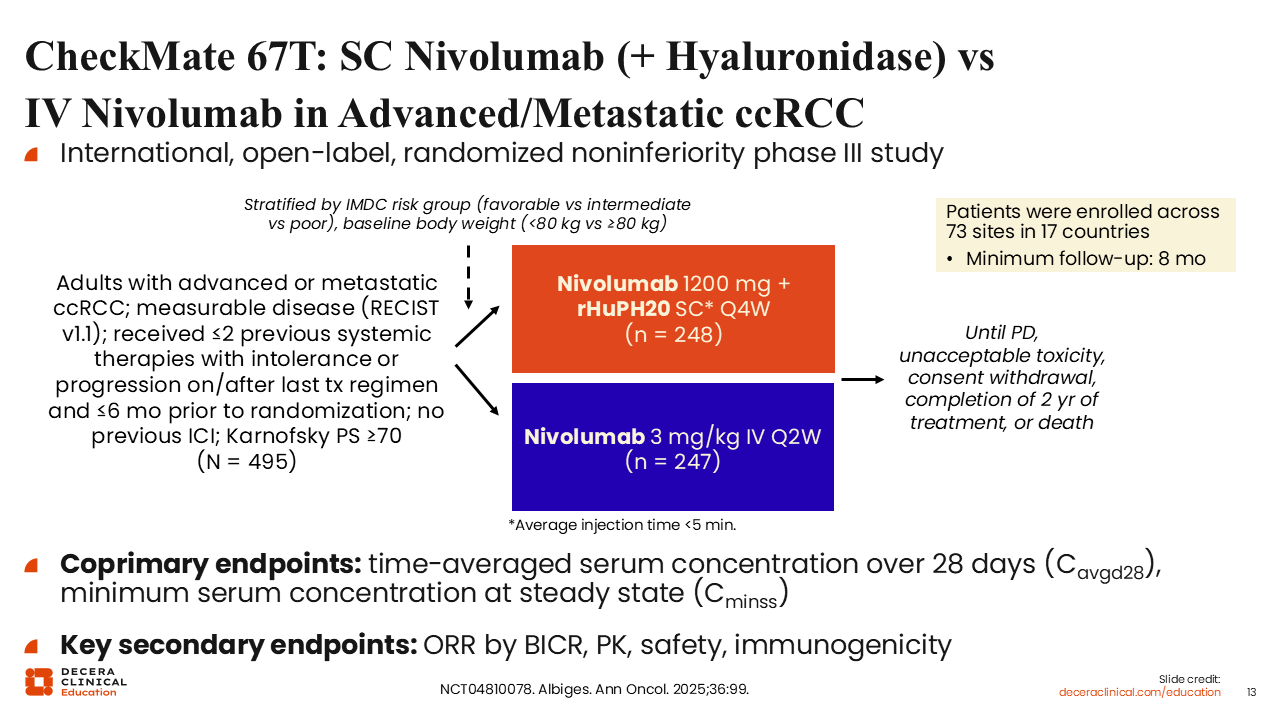
CheckMate 67T: SC Nivolumab (+ Hyaluronidase) vs IV Nivolumab in Advanced/Metastatic ccRCC
CheckMate 67T was an international, open-label, randomized noninferiority phase III study that compared SC with IV nivolumab in adults with advanced or metastatic clear cell renal cell carcinoma (NCT04810078).32 Eligible patients had measurable disease per RECIST v1.1, Karnofsky PS of at least 70, no previous ICI exposure, and up to 2 previous systemic therapies, with intolerance or progression on or after the last regimen within 6 months before randomization. Patients were stratified by International Metastatic RCC Database Consortium risk group and baseline body weight and randomized across 73 sites in 17 countries to receive nivolumab 1200 mg plus rHuPH20 SC every 4 weeks or nivolumab 3 mg/kg IV every 2 weeks. Treatment continued until disease progression, unacceptable toxicity, consent withdrawal, completion of 2 years of treatment, or death. The coprimary endpoints were time-averaged serum concentration over 28 days in cycle 1 (Cavgd28) and minimum serum concentration at steady state, with key secondary endpoints including ORR by BICR, pharmacokinetic, safety, and immunogenicity.
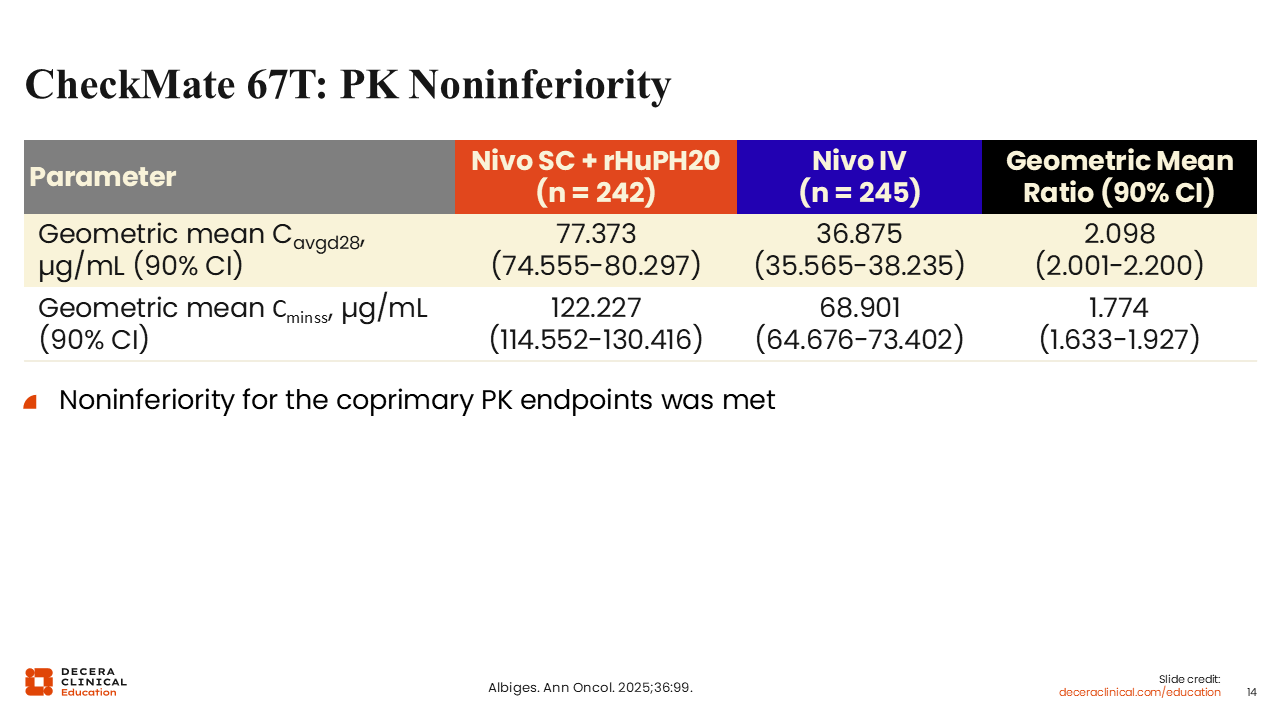
CheckMate 67T: Pharmacokinetic Noninferiority
CheckMate 67T met noninferiority for both coprimary pharmacokinetic endpoints. Geometric mean Cavgd28 was 77.373 mcg/mL with SC nivolumab plus rHuPH20 vs 36.875 mcg/mL with IV nivolumab, with a geometric mean ratio of 2.098 (90% CI: 2.001-2.200). Geometric mean Cminss was 122.227 vs 68.901 mcg/mL, respectively, with a geometric mean ratio of 1.774 (90% CI: 1.633-1.927). Overall, these data supported noninferior pharmacokinetic exposure with the SC formulation.
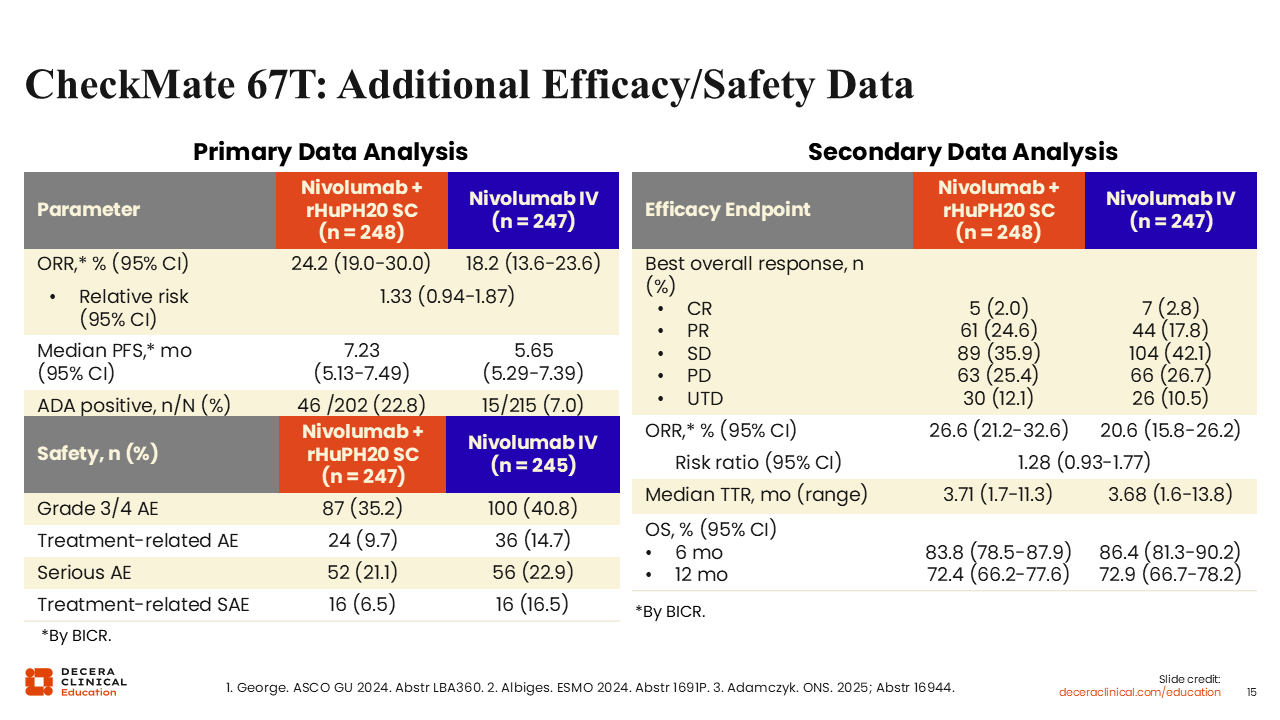
CheckMate 67T: Additional Efficacy/Safety Data
In CheckMate 67T, efficacy and safety outcomes were broadly comparable between the SC and IV nivolumab arms.33 In the primary data analysis, ORR by BICR was 24.2% vs 18.2% (relative risk: 1.33; 95% CI: 0.94-1.87), and median PFS was 7.23 vs 5.65 months (95% CI: 5.13-7.49 vs 5.29-7.39) for SC vs IV nivolumab, respectively. In the secondary data analysis, ORR was 26.6% vs 20.6%, median time to response was 3.71 vs 3.68 months, and OS rates at 6 months were 83.8% vs 86.4% and at 12 months were 72.4% vs 72.9%, respectively. Safety was also generally comparable, with grade 3/4 AEs reported in 35.2% vs 40.8%, treatment-related AEs in 9.7% vs 14.7%, and serious AEs in 21.1% vs 22.9%.
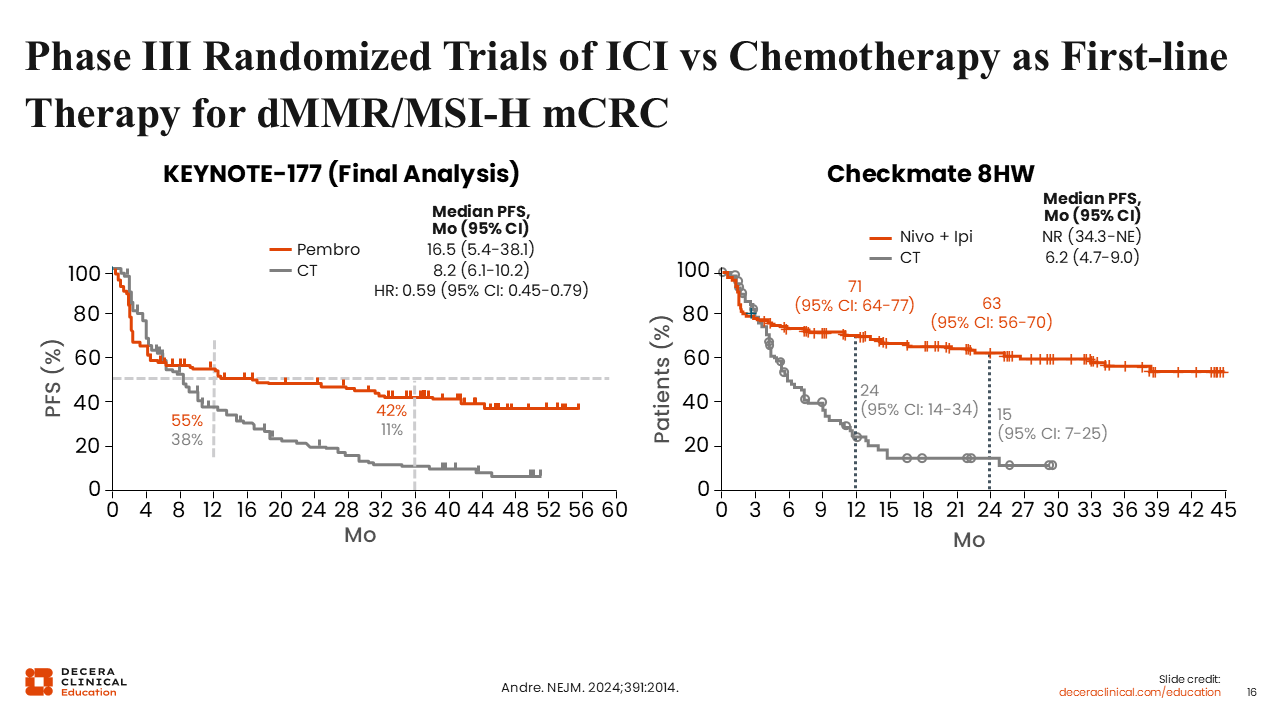
Phase III Randomized Trials of ICI vs Chemotherapy as First-line Therapy for dMMR/MSI-H mCRC
Phase III randomized trials have shown durable PFS benefit with first-line ICI therapy compared with chemotherapy in patients with mismatch repair–deficient (dMMR)/microsatellite instability–high (MSI-H) metastatic CRC. In the final analysis of KEYNOTE-177, pembrolizumab improved median PFS to 16.5 months (95% CI: 5.4-38.1) vs 8.2 months (95% CI: 6.1-10.2) with chemotherapy (HR: 0.59; 95% CI: 0.45-0.79); PFS rates at 12 months were 55% vs 38% and at 36 months were 42% vs 11%.34 In CheckMate 8HW, nivolumab plus ipilimumab further demonstrated sustained benefit, with median PFS not reached (95% CI: 34.3-not estimable) vs 6.2 months (95% CI: 4.7-9.0) with chemotherapy; PFS rates at 12 months were 71% (95% CI: 64%-77%) vs 24% (95% CI: 14%-34%) and at 24 months were 63% (95% CI: 56%-70%) vs 15% (95% CI: 7%-25%).35 Overall, these data support durable disease control with first-line ICI-based therapy in dMMR/MSI-H mCRC.
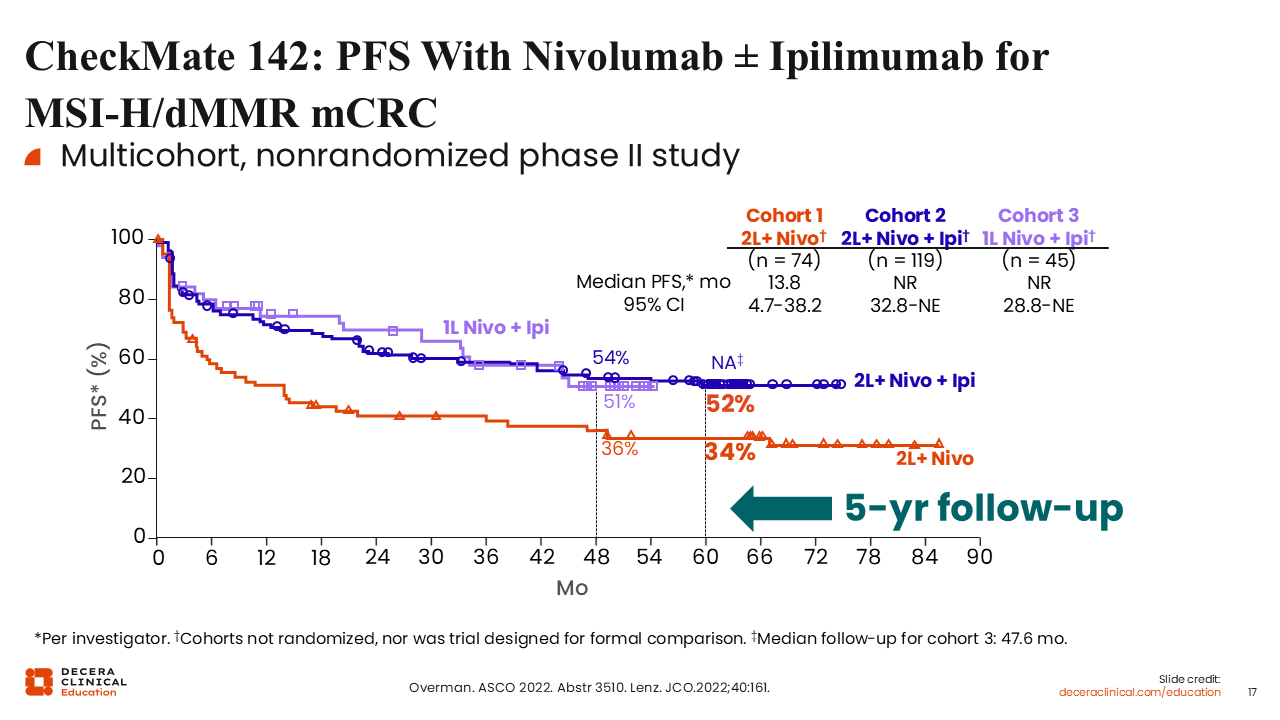
CheckMate 142: PFS With Nivolumab ± Ipilimumab for MSI-H/dMMR mCRC
CheckMate 142 was a multicohort, nonrandomized phase II study evaluating nivolumab with or without ipilimumab in MSI-H/dMMR metastatic CRC.36,37 Investigators from that trial reported a median PFS of 13.8 months with second-line or later nivolumab alone (95% CI: 4.7-38.2). By contrast, median PFS was not reached with nivolumab plus ipilimumab in both the second-line or later cohort (95% CI: 32.8-not estimable) and the first-line cohort (95% CI: 28.8-not estimable). At 48 months, PFS rates were 36% with second-line or later nivolumab alone, 54% with second-line or later nivolumab plus ipilimumab, and 51% with first-line nivolumab plus ipilimumab. At 60 months, the PFS rates were 34% and 52%, respectively, for nivolumab alone and second-line or later nivolumab plus ipilimumab.
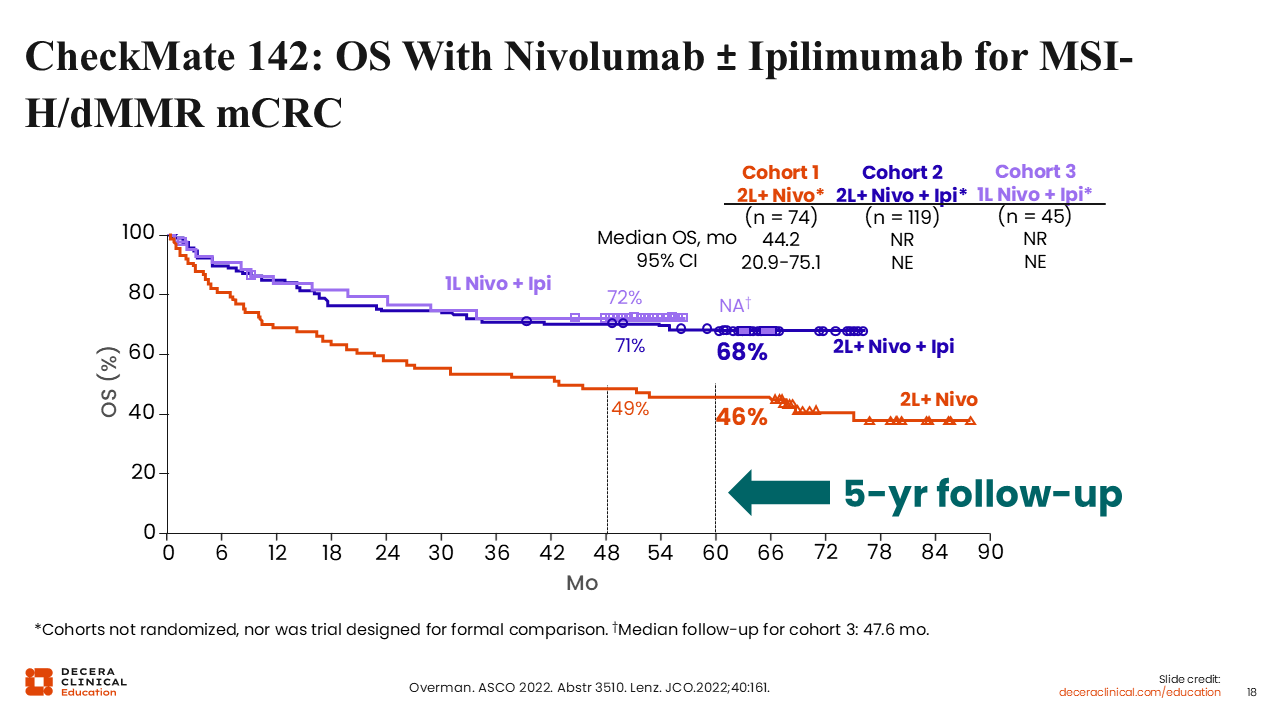
CheckMate 142: OS With Nivolumab ± Ipilimumab for MSI-H/dMMR mCRC
Similarly, the OS results showed durable benefit, although the cohorts were not randomized and were not intended for formal comparison.36,37 Investigators reported a median OS of 44.2 months with second-line or later nivolumab alone (95% CI: 20.9-75.1). By contrast, median OS was not reached with nivolumab plus ipilimumab in both the second-line or later and first-line cohorts, and the 95% CIs were not estimable. At 48 months, OS rates were 49% with second-line or later nivolumab alone, 71% with second-line or later nivolumab plus ipilimumab, and 72% with first-line nivolumab plus ipilimumab. At 60 months, OS rates were 46% and 68%, respectively, for nivolumab alone and second-line or later nivolumab plus ipilimumab. The 60-month OS rate for the first-line nivolumab plus ipilimumab cohort was not available because follow-up was shorter, with a median duration of 47.6 months.
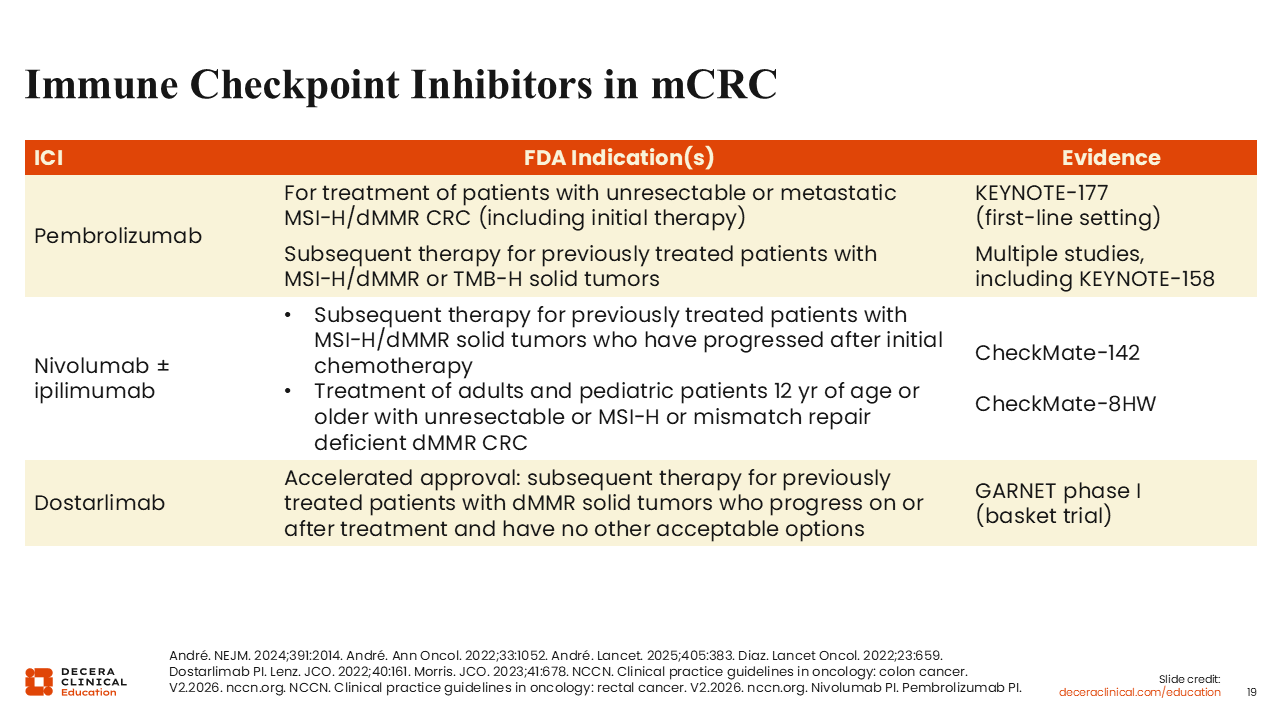
Immune Checkpoint Inhibitors in mCRC
Durable survival signal comes from the nonrandomized, multicohort phase II CheckMate 142 study (NCT02060188), so these cohorts should be interpreted descriptively rather than as formal head-to-head comparisons.36,37 Median OS was 44.2 months with second-line or later nivolumab alone (95% CI: 20.9-75.1) and was not reached in either nivolumab plus ipilimumab cohort. At 48 months, OS rates were 49%, 71%, and 72% for cohort 1 (second-line nivolumab), cohort 2 (second-line nivolumab plus ipilimumab), and cohort 3 (first-line nivolumab plus ipilimumab), respectively. The 60-month OS rates of 46% with second-line or later nivolumab alone and 68% with second-line or later nivolumab plus ipilimumab.
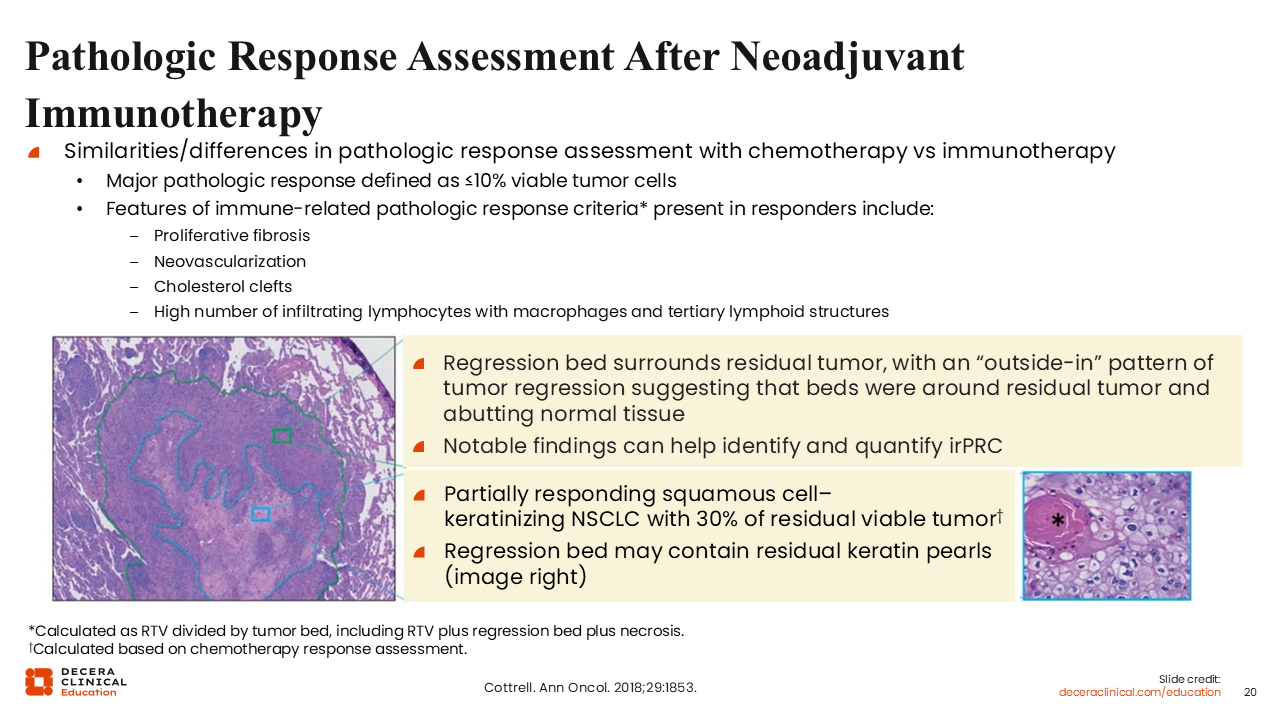
Pathologic Response Assessment After Neoadjuvant Immunotherapy
We have had now 4 different phase III studies for either neoadjuvant or perioperative chemoimmunotherapy for NSCLC, initially with CheckMate 816, then KEYNOTE-671 for pembrolizumab, AEGEAN of durvalumab,38-40 and more recently, CheckMate 77T41 of perioperative nivolumab response after neoadjuvant component of treatment. It appears there is a difference between pathologic complete response (pCR) for immunotherapy and the traditional responses we see with chemotherapy. For the purpose of this review, we define major pathologic response as 10% or less residual viable cancer cells in the specimen.
KEYNOTE-671: Pembro or Pbo + Plt-Based Neoadj CT Followed by Resection and Adj Pembro or Pbo in Early-Stage NSCLC
A recent area that has risen out of ICI advances is the fairly dramatic shift over the last 2-3 years from patients having upfront surgery for stage II and III lung cancer and instead having neoadjuvant chemotherapy with ICIs. This has given rise to the phenomenon of pCR being considered as a potential surrogate endpoint. We know about this from breast cancer because there were relatively high rates of pCR in some subtypes of breast cancer. Historically, with chemotherapy alone, we did not see much with regard to pCR rates in NSCLC.
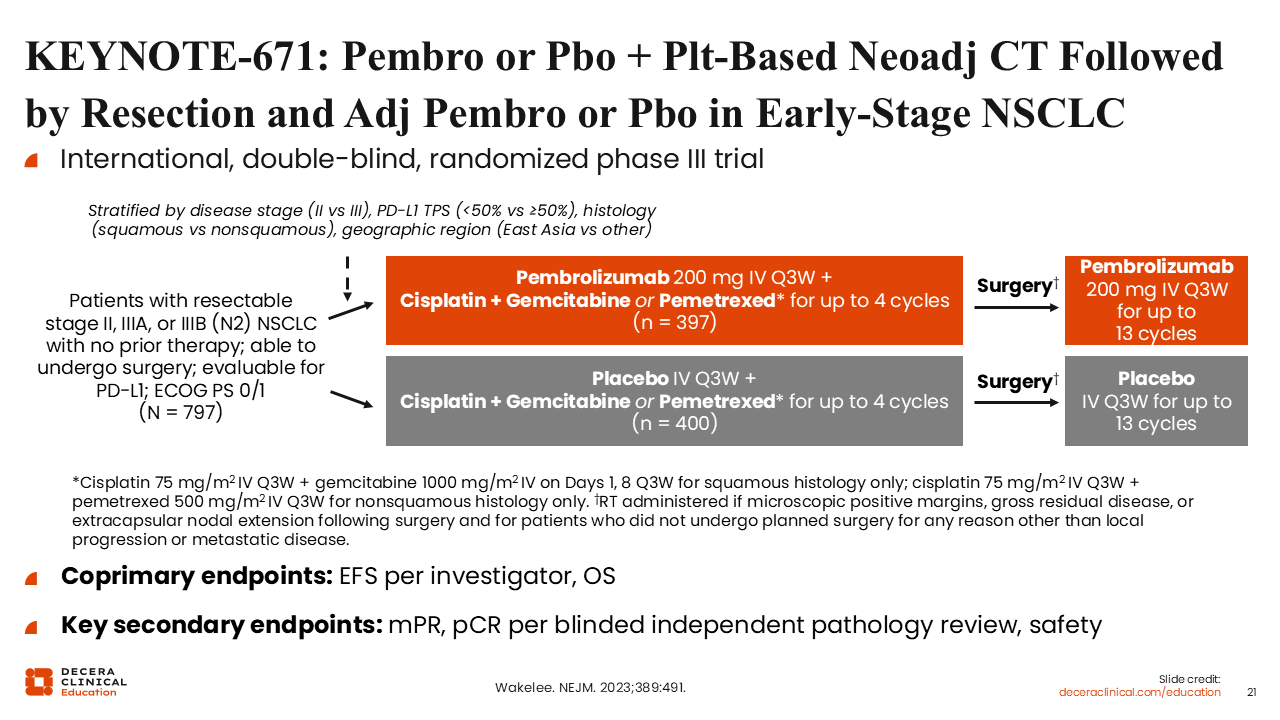
KEYNOTE-671 was an international, double-blind, randomized phase III trial that evaluated perioperative pembrolizumab plus platinum-based chemotherapy vs placebo plus platinum-based chemotherapy in patients with resectable stage II, IIIA, or IIIB (N2) NSCLC.39 Eligible patients had no prior therapy, were able to undergo surgery, were evaluable for PD-L1 expression, and had ECOG PS 0/1. Patients were stratified by disease stage, PD-L1 tumor proportion score, histology, and geographic region, and then randomized to receive pembrolizumab 200 mg IV every 3 weeks or placebo with cisplatin plus gemcitabine for squamous disease or cisplatin plus pemetrexed for nonsquamous disease for up to 4 cycles before surgery, followed by adjuvant pembrolizumab or placebo every 3 weeks for up to 13 cycles. The coprimary endpoints were event-free survival per the investigator and overall survival, with key secondary endpoints including major pathologic response, pCR per blinded independent pathology review (BIPR), and safety.
KEYNOTE-671 pCR/MPR
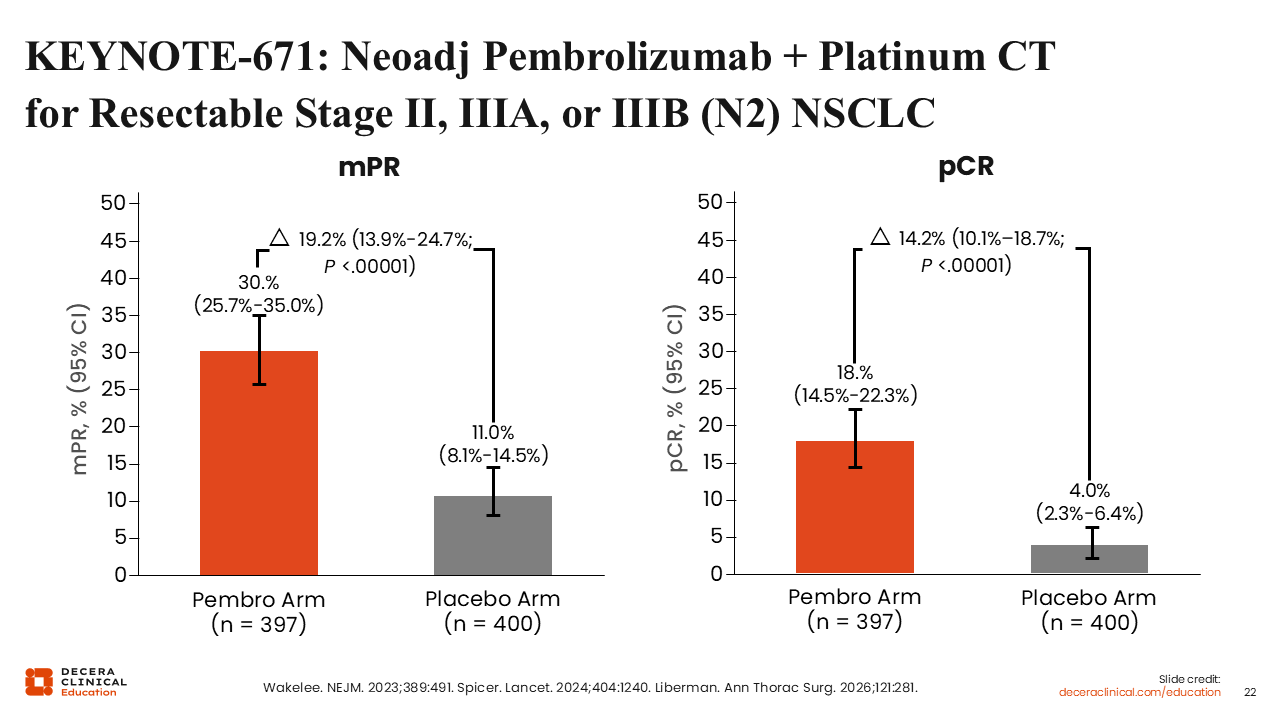
We see some of the improvement seen with pembrolizumab. We have some major pathologic response.42,43 Again, 10% or less residual cancer went from 11% with placebo plus chemotherapy to 30% for chemotherapy plus pembrolizumab. Then pCR was also increased more than fourfold by the addition of pembrolizumab to chemotherapy. Moreover, we see that more patients in the chemoimmunotherapy arm had a pCR (18% vs 4%).
KEYNOTE-671: EFS and OS (Coprimary Endpoints)
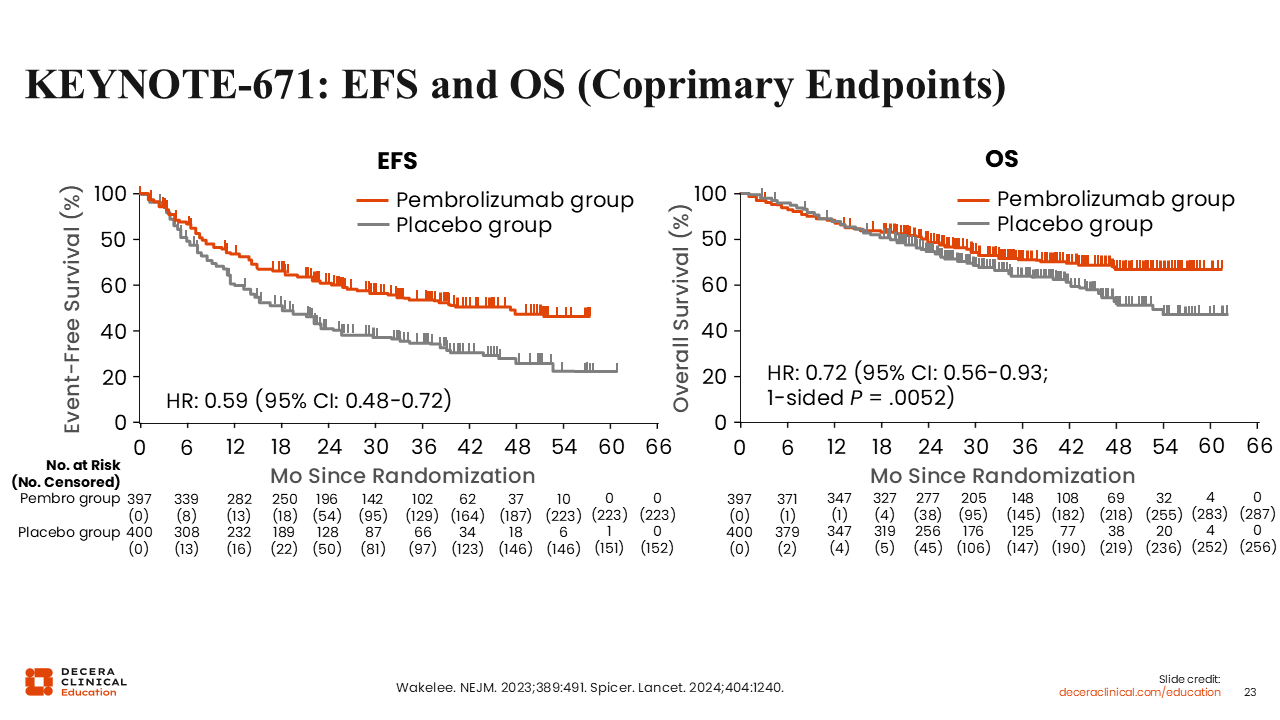
Investigators from KEYNOTE-671 reported significant improvement in both coprimary endpoints with perioperative pembrolizumab plus platinum-based chemotherapy vs placebo plus chemotherapy. Event-free survival was improved with an HR of 0.59 (95% CI: 0.48-0.72), and OS was also improved with an HR of 0.72 (95% CI: 0.56-0.93; 1-sided P = .0052), both favoring the pembrolizumab-containing arm vs chemotherapy plus placebo.42 These findings showed benefit for pembrolizumab in the neoadjuvant and adjuvant setting in patients with resectable stage II-IIIB (N2) NSCLC.
KEYNOTE-671: Immune-Mediated AEs and Infusion Reactions Across Treatment Phases
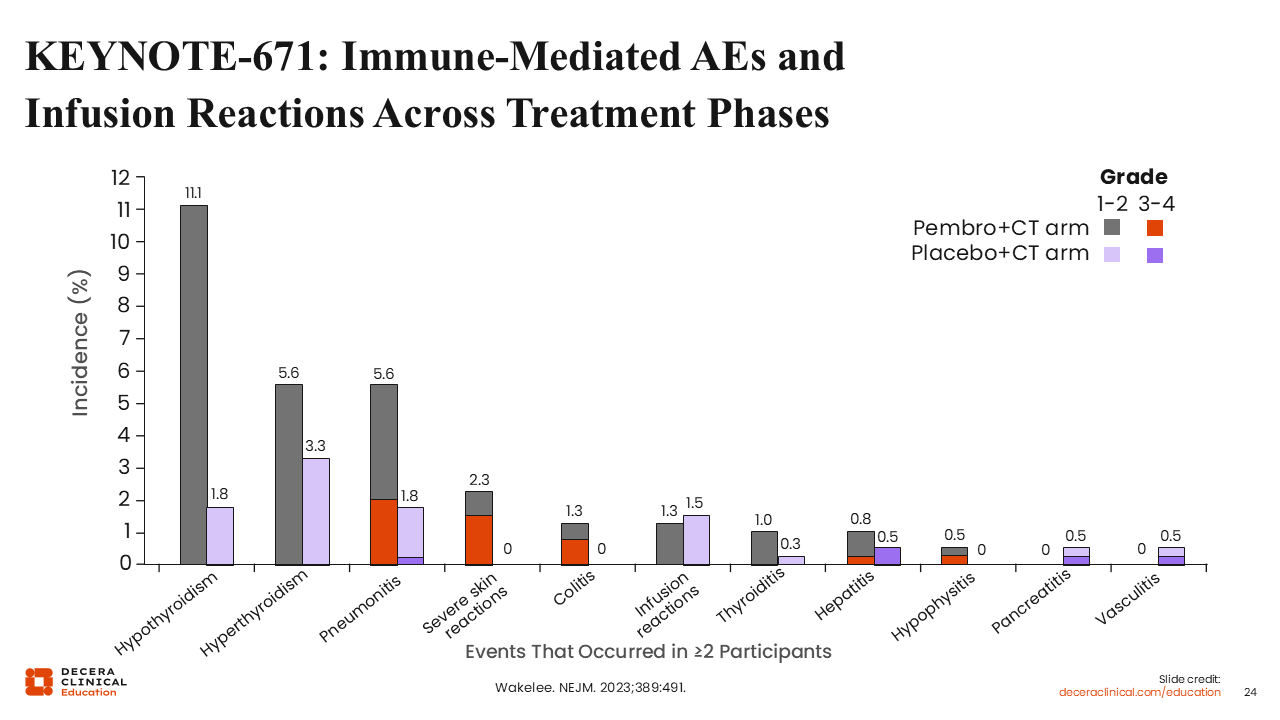
Immune-mediated AEs and infusion reactions were more common with pembrolizumab plus chemotherapy than with placebo plus chemotherapy in KEYNOTE-671, although most were low grade. The most frequent grade 1/2 immune-mediated AE was hypothyroidism, reported in 11.1% vs 1.8% of patients, followed by hyperthyroidism in 5.6% vs 3.3%. Selected higher-grade AEs remained relatively uncommon but occurred more often in the pembrolizumab arm for some AEs, including pneumonitis (grade 3/4: 2.0% vs 0.2%), severe skin reactions (1.5% vs 0%), and colitis (0.8% vs 0%). Infusion reactions were infrequent overall, reported in 1.3% vs 1.5% of patients.
Overall, these findings suggest that immune-mediated AE increased with pembrolizumab, but most were low grade and generally manageable with appropriate monitoring and management.
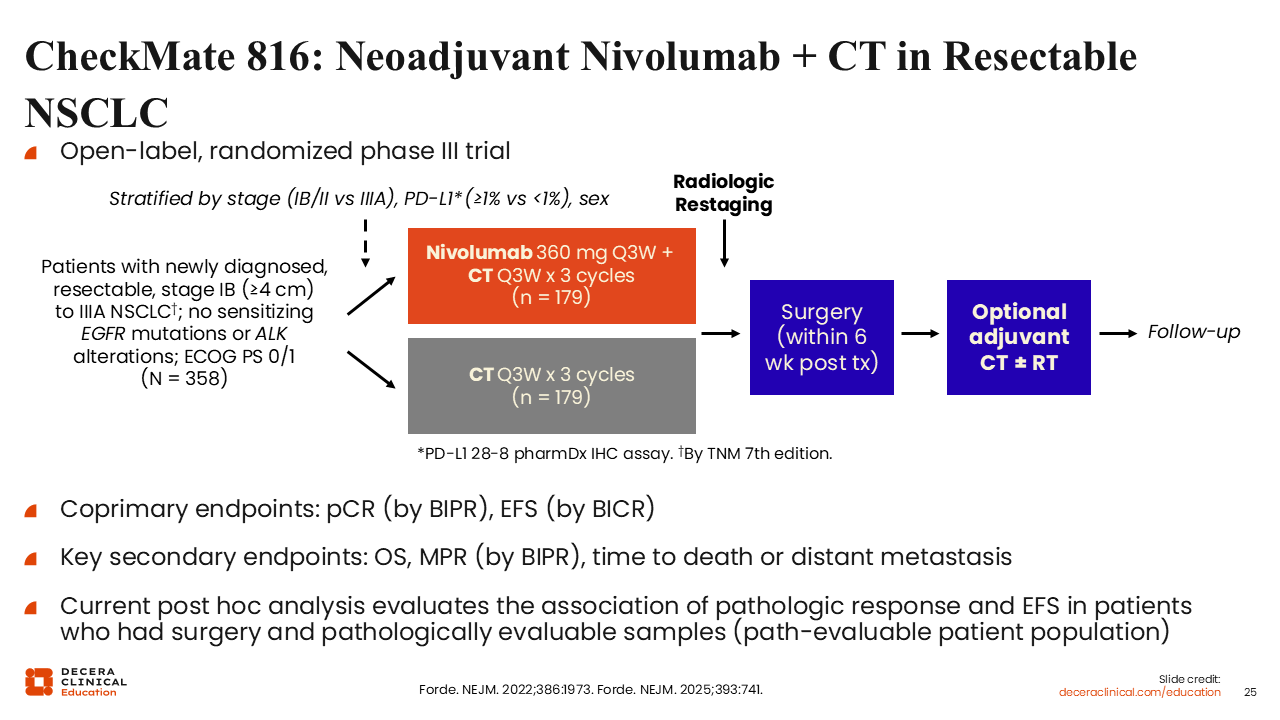
CheckMate 816: Neoadjuvant Nivolumab + CT in Resectable NSCLC
CheckMate 816 was an open-label, randomized phase III trial that evaluated neoadjuvant nivolumab plus chemotherapy vs chemotherapy alone in patients with newly diagnosed, resectable stage IB (≥4 cm) to IIIA NSCLC. Eligible patients had ECOG PS 0/1 and no sensitizing EGFR mutations or ALK alterations.44,45 Patients were stratified by stage, PD-L1 expression, and sex, and then randomized to receive nivolumab 360 mg every 3 weeks plus chemotherapy every 3 weeks for 3 cycles or chemotherapy alone for 3 cycles, followed by radiologic restaging and surgery within 6 weeks after treatment, with optional adjuvant chemotherapy and/or radiotherapy. The coprimary endpoints were pCR by BIPR and event-free survival by BICR, with key secondary endpoints including overall survival, major pathologic response by BIPR, and time to death or distant metastasis.
CheckMate 816: Neoadj Nivolumab + Platinum CT
for Resectable Stage IB-IIIA NSCLC
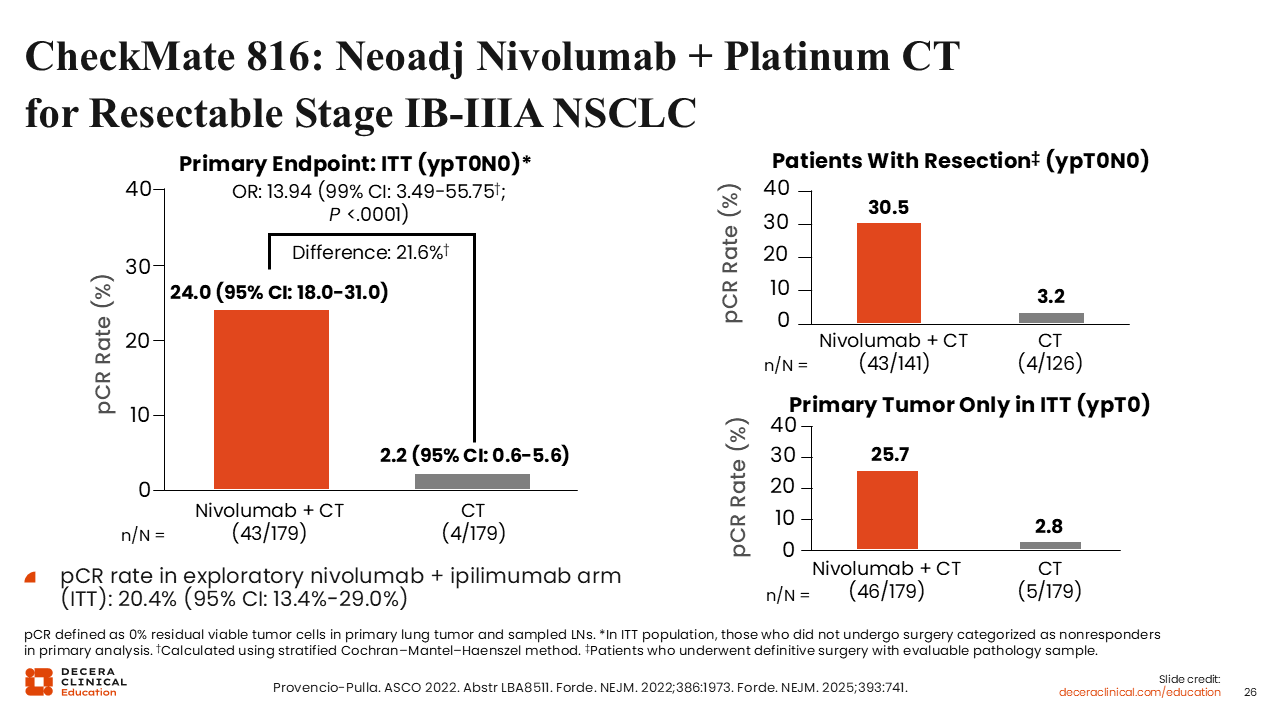
Investigators from CheckMate 816 showed a substantially higher pCR rate with neoadjuvant nivolumab plus chemotherapy vs chemotherapy alone. In the intention-to-treat population, pCR was 24.0% with nivolumab plus chemotherapy vs 2.2% with chemotherapy alone, corresponding to an absolute difference of 21.6% and an odds ratio of 13.94 (99% CI: 3.49-55.75; P <.0001). Among patients who underwent resection, pCR rates were 30.5% vs 3.2%, and in the intention-to-treat analysis of primary tumor only, pCR rates were 25.7% vs 2.8% for nivolumab plus chemotherapy vs chemotherapy alone, respectively. a pCR rate of 20.4% (95% CI: 13.4%-29.0%) was also noted in the exploratory nivolumab plus ipilimumab arm.
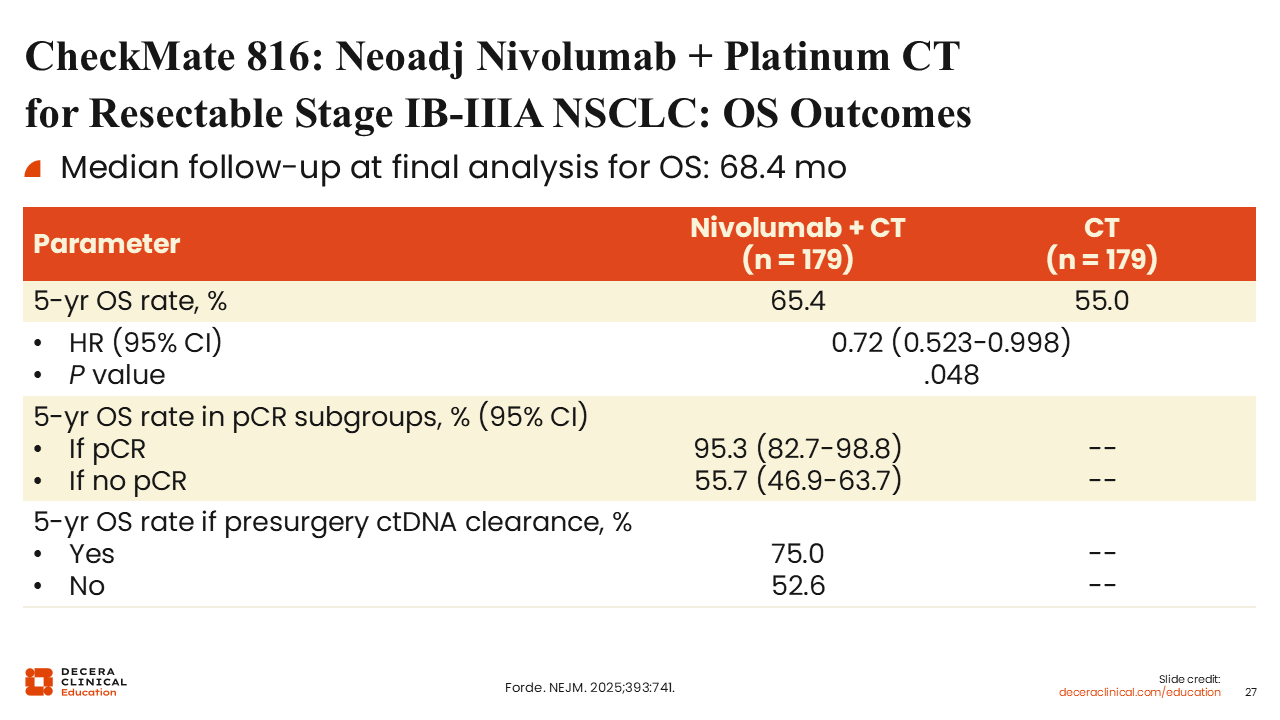
CheckMate 816: Neoadj Nivolumab + Platinum CT for Resectable Stage IB-IIIA NSCLC: OS Outcomes
We also observe a significant improvement in both OS and event-free survival. The 5-year OS is approximately 65% in the nivolumab plus chemotherapy arm compared with 55% in the chemotherapy alone arm (HR: 0.72), favoring the nivolumab plus ipilimumab arm. An important point here is that if patients had a pCR (24% of patients in the trial), they had a 5-year survival of 95% vs 55% if they did not have a pCR.
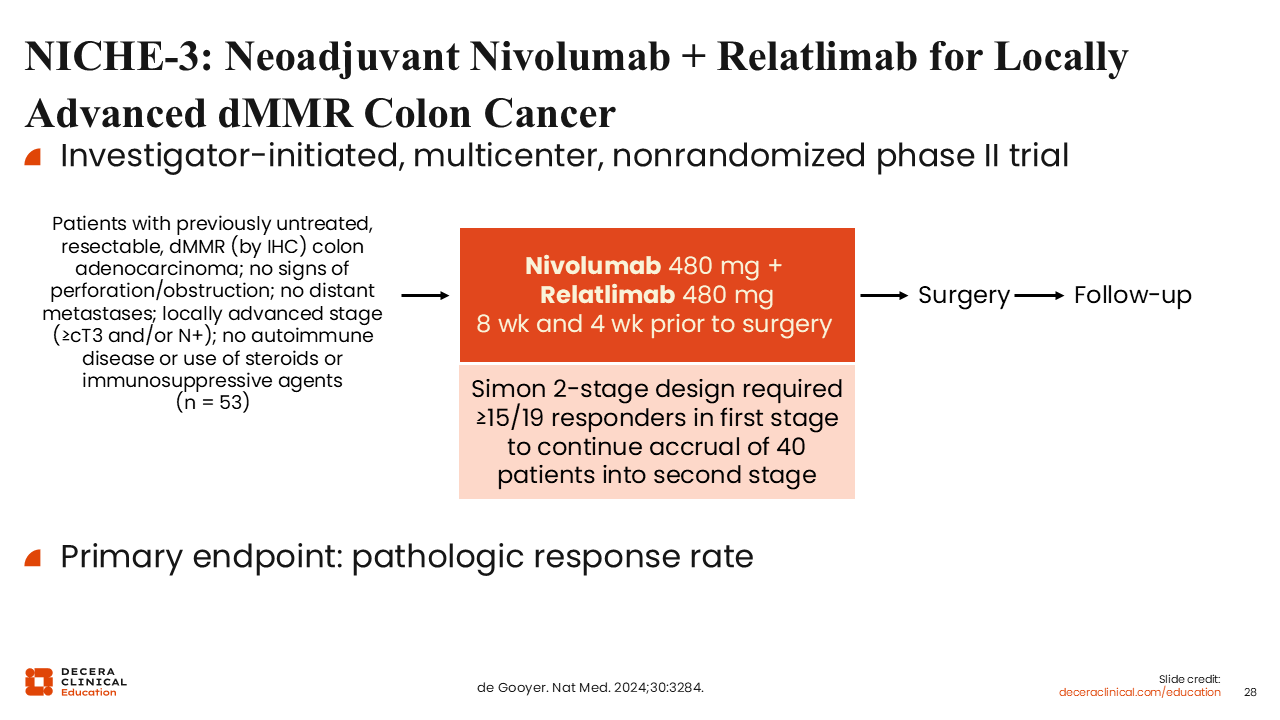
NICHE-3: Neoadjuvant Nivolumab + Relatlimab for Locally Advanced dMMR Colon Cancer
The NICHE-3 trial was an investigator-initiated, multicenter, nonrandomized phase II trial that evaluated neoadjuvant nivolumab plus relatlimab in patients with locally advanced dMMR colon cancer.46 Eligible patients had previously untreated, resectable colon adenocarcinoma with dMMR by immunohistochemistry, no signs of perforation or obstruction, no distant metastases, and locally advanced disease defined as at least cT3 and/or node-positive disease; patients with autoimmune disease or use of steroids or other immunosuppressive agents were excluded. Patients received nivolumab 480 mg plus relatlimab 480 mg at 8 weeks and 4 weeks before surgery, followed by surgery and follow-up. The primary endpoint was pathologic response rate, and the trial used a Simon 2-stage design requiring at least 15 responses among the first 19 patients to continue accrual into the second stage.
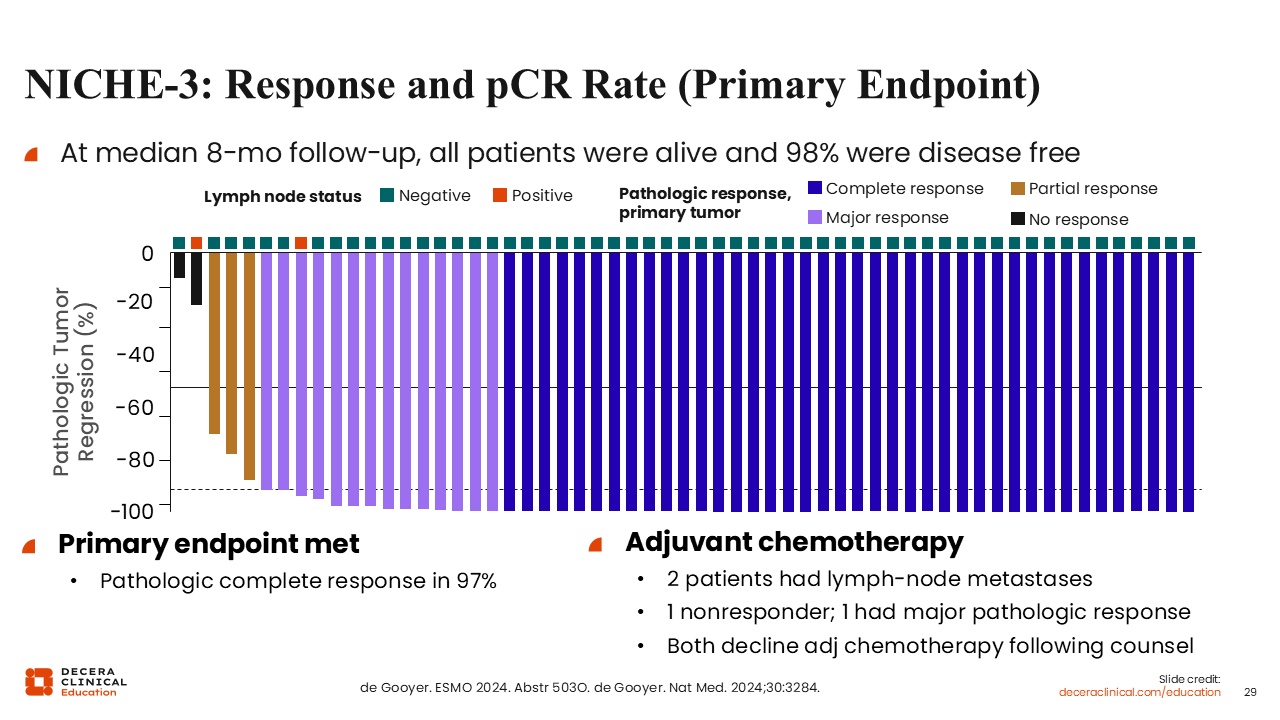
NICHE-3: Response and pCR Rate (Primary Endpoint)
Investigators reported that the NICHE-3 met its primary endpoint, with pCR in 97% of patients. At a median follow-up of 8 months, all patients were alive and 98% were disease free. We see that nearly all patients achieved deep pathologic regression, with most experiencing complete response and only rare cases of partial response or no response. Two patients had lymph node metastases and were considered for adjuvant chemotherapy; one was a nonresponder, one had a major pathologic response, and both declined adjuvant chemotherapy after counseling.
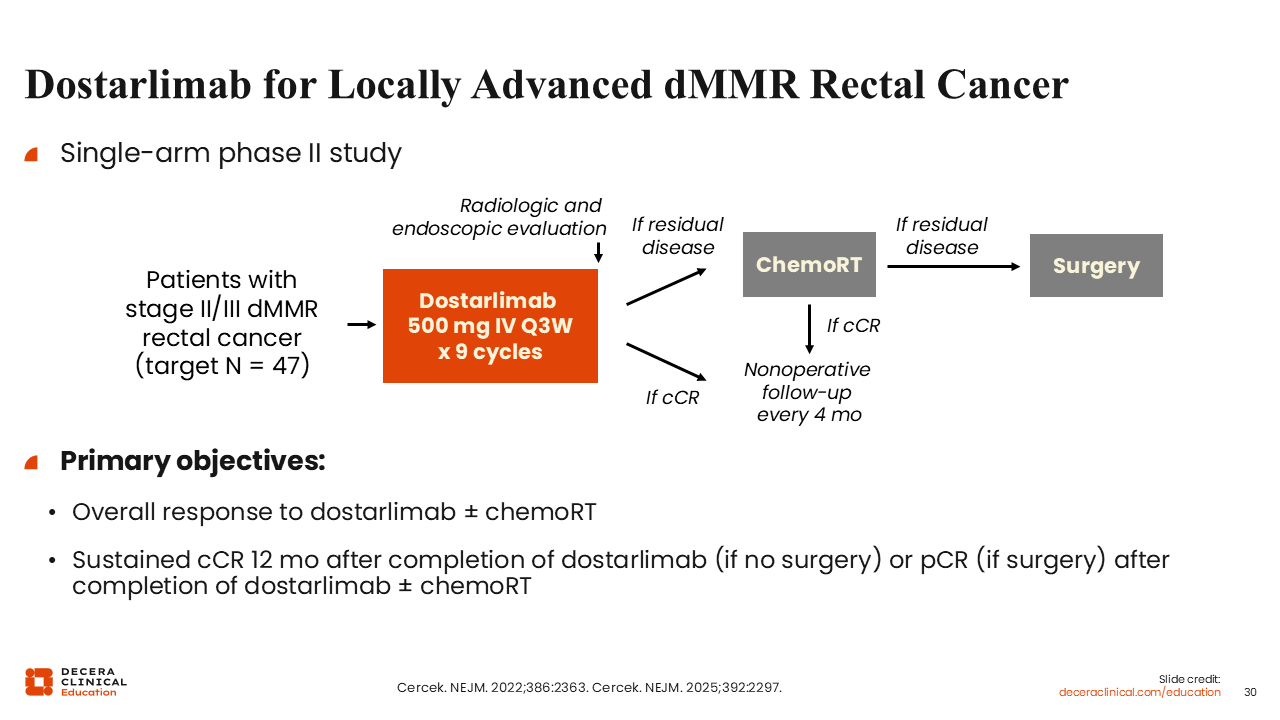
Dostarlimab for Locally Advanced dMMR Rectal Cancer
This has led to other studies for other immunotherapy agents in development.
Dostarlimab for locally advanced dMMR rectal cancer was evaluated in a single-arm phase II study in patients with stage II/III dMMR rectal cancer, with a target enrollment of 47 patients.47 Patients received dostarlimab 500 mg IV every 3 weeks for 9 cycles, followed by radiologic and endoscopic evaluation. If residual disease was present, patients proceeded to chemoradiotherapy and then surgery if residual disease persisted; if a clinical complete response was achieved, patients entered nonoperative follow-up every 4 months. The primary objectives were overall response to dostarlimab with or without chemoradiotherapy and sustained clinical complete response 12 months after completion of dostarlimab in patients who did not undergo surgery or pCR in those who did undergo surgery.
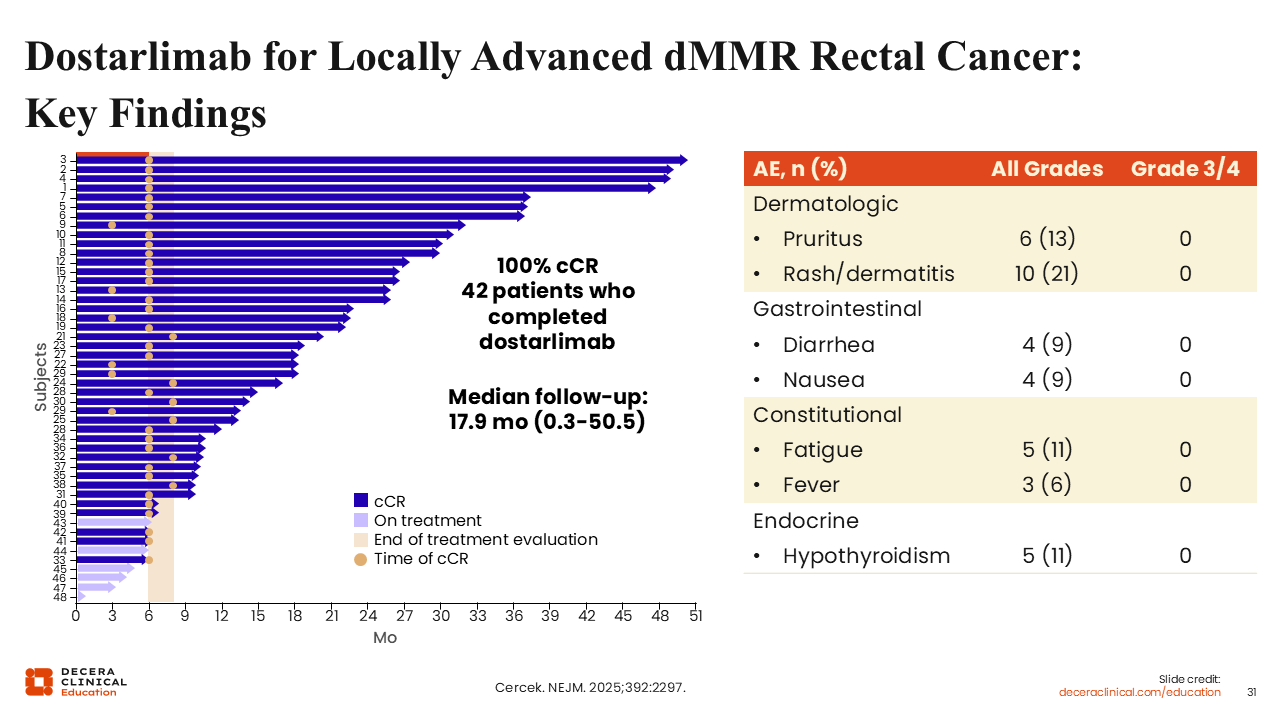
Dostarlimab for Locally Advanced dMMR Rectal Cancer: Key Findings
Dostarlimab produced a clinical complete response in 100% of the 42 patients who completed treatment, supporting a nonoperative management approach in this cohort of locally advanced dMMR rectal cancer. At the time of this analysis, median follow-up was 17.9 months (range: 0.3-50.5), indicating that some patients had remained in clinical complete response for more than 4 years without surgery. Treatment was also generally well tolerated, with the most common all-grade AEs including rash/dermatitis in 21%, pruritus in 13%, fatigue in 11%, hypothyroidism in 11%, diarrhea in 9%, and nausea in 9%; no grade 3/4 AEs were reported for the AEs listed on the slide. Overall, these findings support the potential for organ-preserving management in selected patients with dMMR rectal cancer treated with dostarlimab.