CE / CME
Improving Outcomes With Immune Checkpoint Inhibitors for Solid Tumors
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: June 18, 2026
Expiration: December 17, 2026

Activity
Practical Considerations for SC vs IV ICI Administration
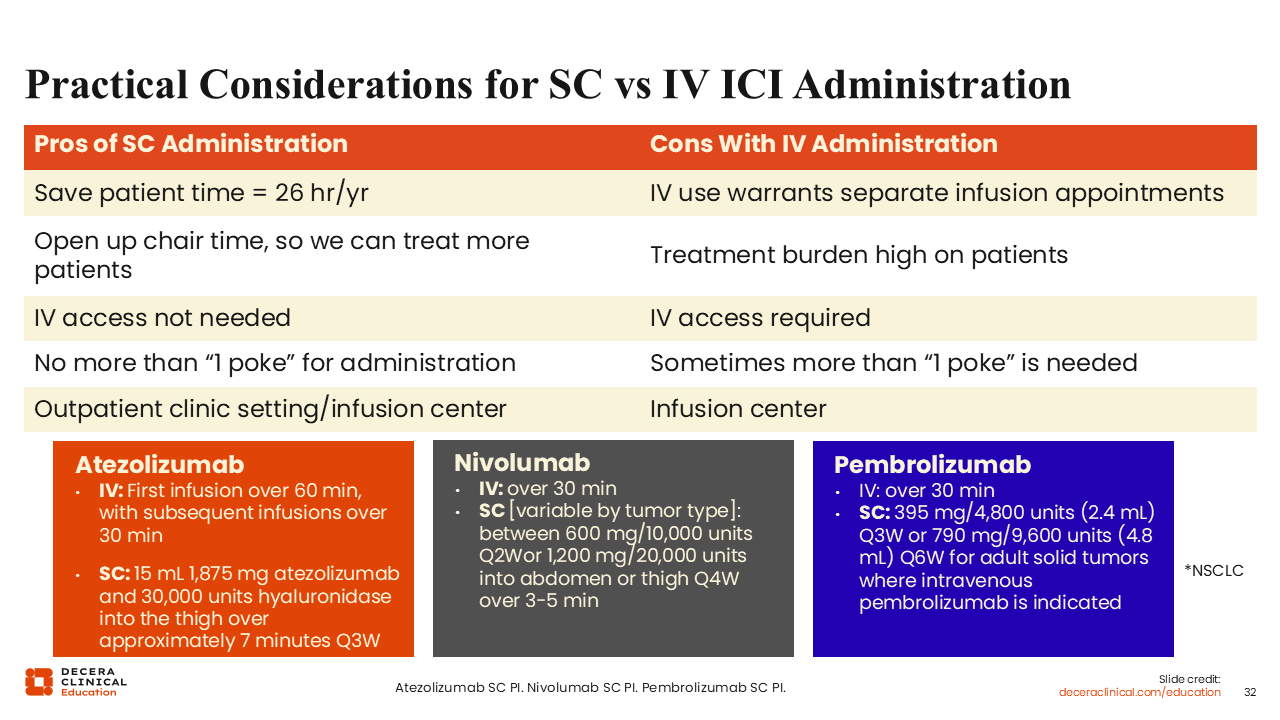
Practical considerations may favor SC administration for selected patients and practices. Compared with IV administration, SC dosing may reduce treatment burden by shortening administration time and eliminating the need for routine IV access.25-27
There is a potential time savings of approximately 26 hours per year for patients. SC administration may also open chair time and can be delivered in outpatient clinic or infusion-center settings, typically with no more than 1 poke for administration. By contrast, IV administration generally requires separate infusion appointments, IV access, and in some cases more than 1 poke.
Pricing Parity Between IV and SC
Operational and reimbursement considerations may also influence adoption of SC formulations. This slide highlights pricing parity between IV and SC administration at $15,575 per 4 weeks as of May 2025 and notes the potential for favorable bulk pricing through specialty Group Purchasing Organization contracts. It also suggests that reimbursement may be favorable, with an expectation of no financial loss, while recognizing that the route of administration could still affect practice revenue. Taken together, these factors underscore the need for practices to think strategically about acquisition, administration, billing, reimbursement, and longer-term financial sustainability.
Assessment and Understanding of Pseudoprogression While on an ICI
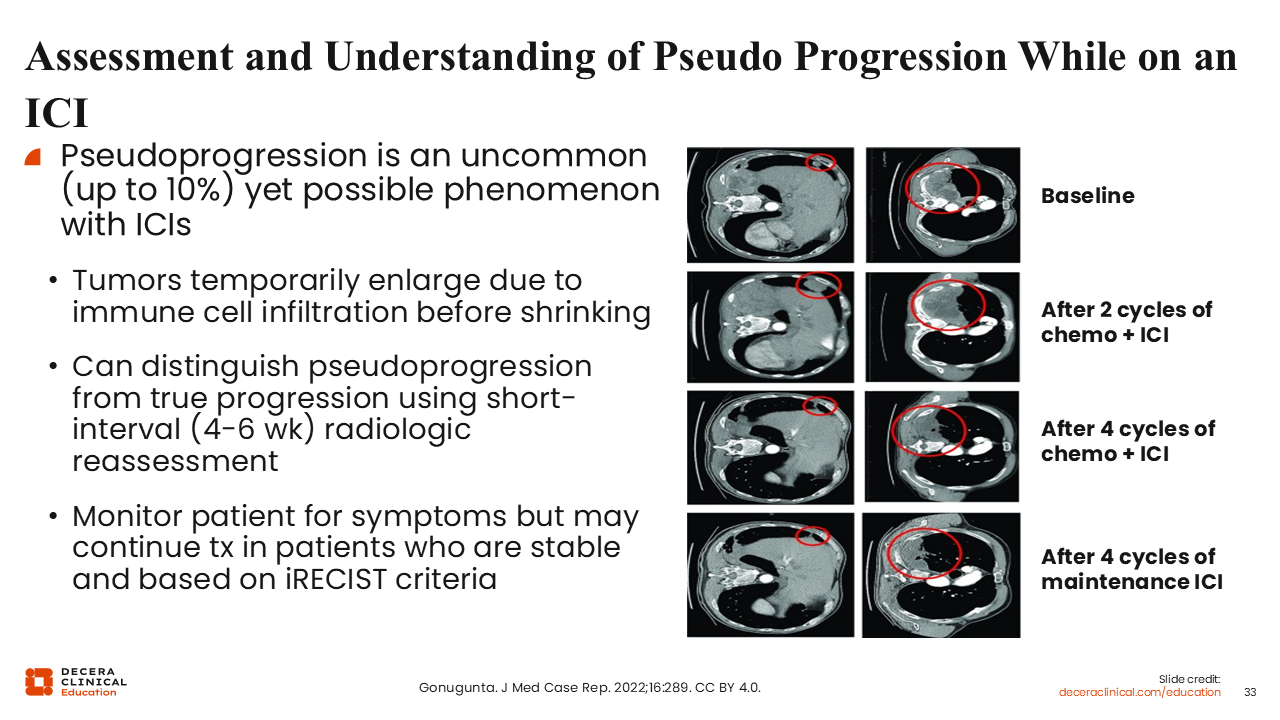
Pseudoprogression is an uncommon phenomenon, reported in up to approximately 10% of patients receiving an ICI. It refers to an initial increase in tumor burden, often thought to reflect immune cell infiltration, followed by subsequent tumor shrinkage.48 It can be distinguished from true progression because patients with pseudoprogression typically do not show rapid clinical worsening. When suspected, patients should be monitored carefully, and response should be assessed using RECIST in the context of overall clinical stability.
Pseudoprogression Examples in Skin Cancer
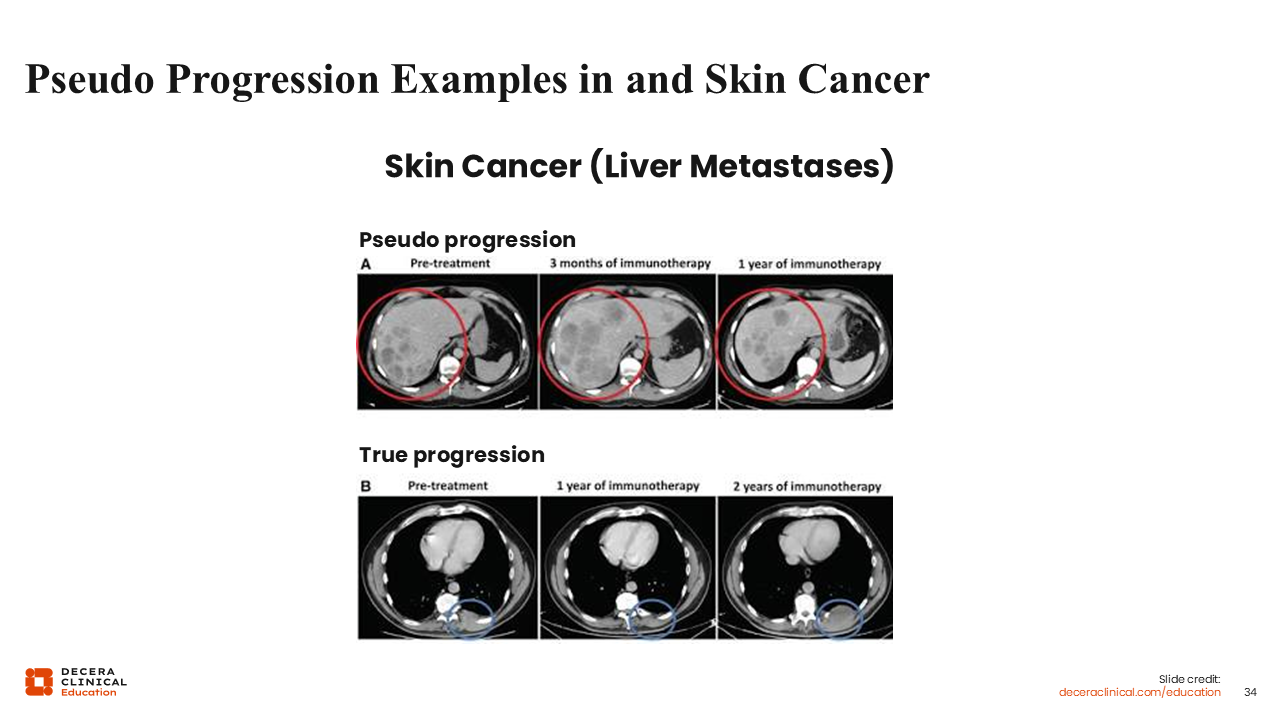
If we look at imaging examples from melanoma with liver metastases, they illustrate the difference between pseudoprogression and true progression during immunotherapy. In the top row, labeled “pseudoprogression,” the lesion appears larger at 3 months after starting immunotherapy but is smaller by 1 year, which is consistent with an initial inflammatory response followed by tumor regression. In the bottom row, labeled “true progression,” the lesion continues to enlarge over time, including at 1 year and 2 years of immunotherapy, without the later regression seen with pseudoprogression.
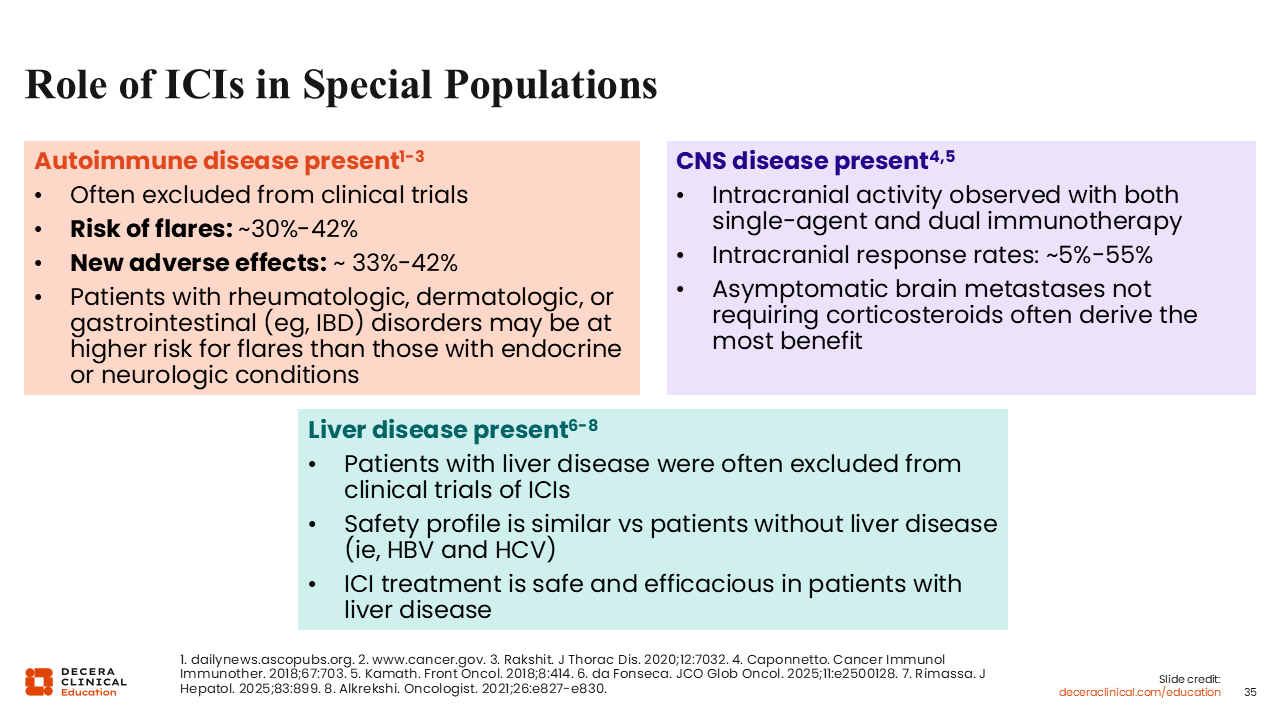
Autoimmune Disease Present
Patients with autoimmune disease often were excluded from the original ICI trials, but we now have growing data to help guide treatment in this setting.49,50 ICIs can be used in selected patients with preexisting autoimmune disease, although the risk of autoimmune flare is meaningful, at approximately 30% to 42%, and new AEs occur in approximately 33% to 42% of patients. Flare risk may be higher in patients with rheumatologic, dermatologic, or gastrointestinal disorders such as inflammatory bowel disease than in those with endocrine or neurologic autoimmune conditions.
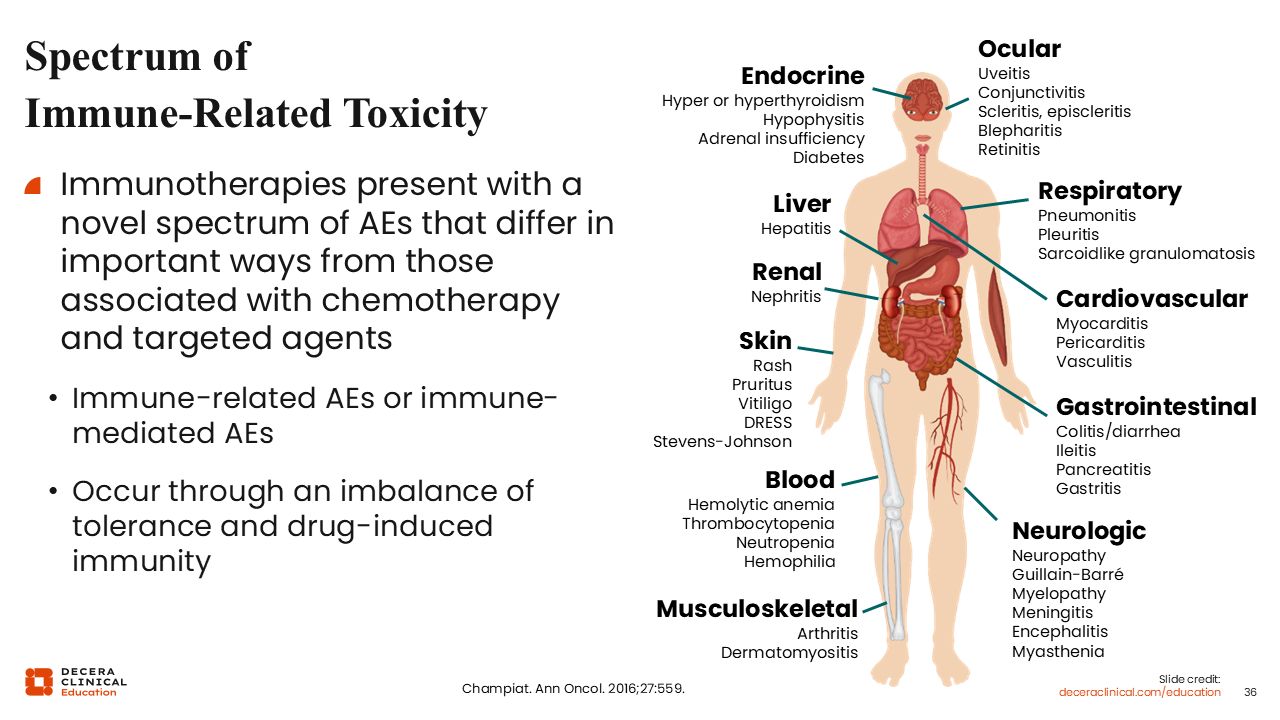
Spectrum of Immune-Related Toxicity
Immune-related AEs span multiple organ systems (eg, liver, endocrine, ocular, respiratory, cardiovascular) and require early recognition. We have to keep this in mind while not disturbing patients too much when we have to explain that many patients go through these treatments with very few, if any, AEs. Awareness is very important, as is reporting potential new symptoms as soon as they occur.
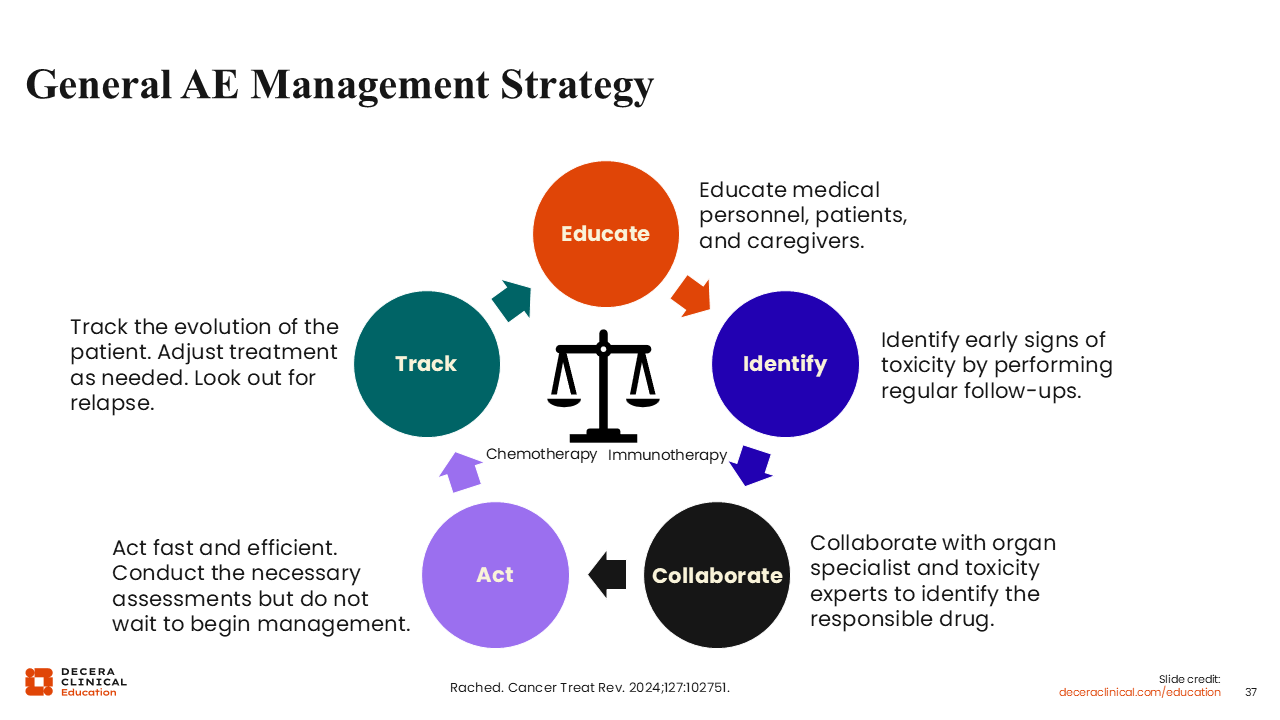
General AE Management Strategy
Early education and prompt reporting are central to immune-related AE management. Both caregivers and patients should be alerted to notify the clinic if patients develop any new, unusual symptoms. Sometimes we, as healthcare professionals, have to work with toxicity experts and organ specialists (eg, pulmonologists, rheumatologists) and also must move quickly. It is not a situation where we let the patient fester for some time because that is the situation, particularly with conditions like pneumonitis, where they can get sick very quickly.
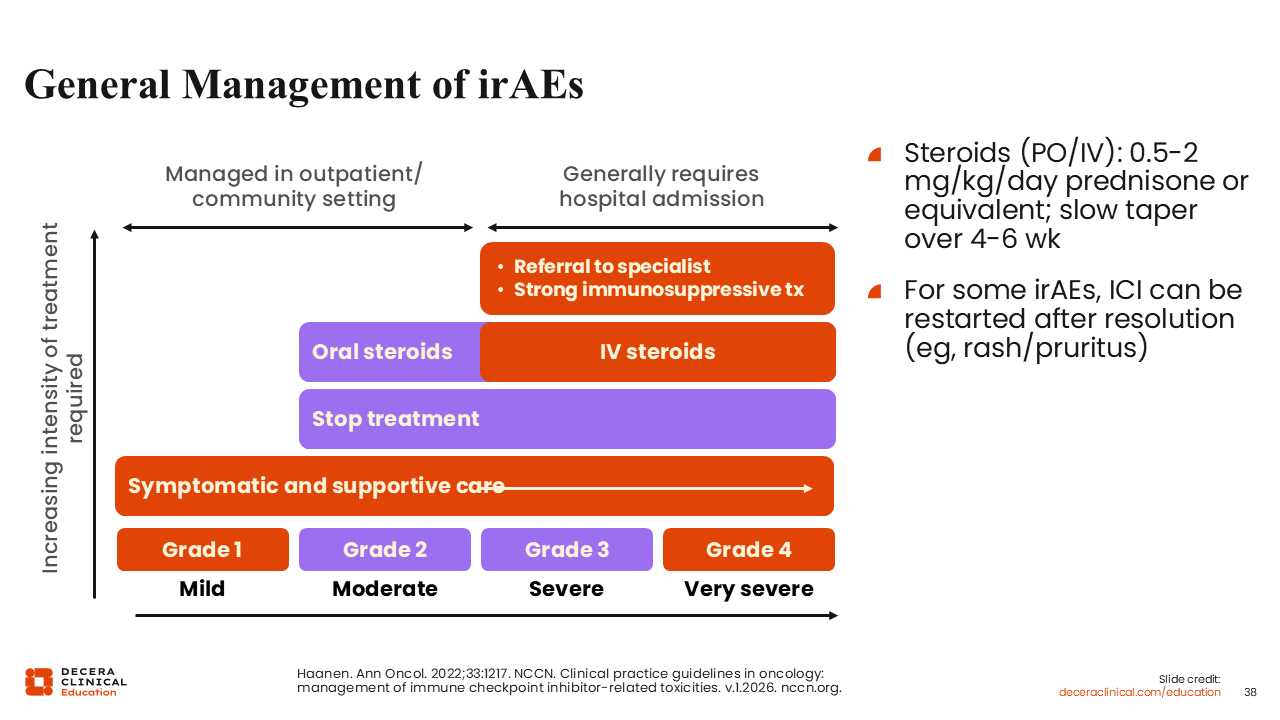
General Management of Immune-Related AEs
In general, management of immune-related AEs is guided by toxicity grade, with treatment intensity increasing from grade 1 to grade 4.49 Mild grade 1 AEs are often managed with symptomatic and supportive care in the outpatient setting. For grade 2 AEs, treatment is commonly held and oral steroids may be started. For grade 3/4 AEs, patients more often require hospital-based care, IV steroids, referral to the appropriate specialist, and in some cases, stronger immunosuppressive therapy. The steroids are typically given at 0.5-2.0 mg/kg/day of prednisone or equivalent, followed by a slow taper over 4-6 weeks, and for some AEs such as with rash or pruritus, ICI therapy can be restarted after resolution.
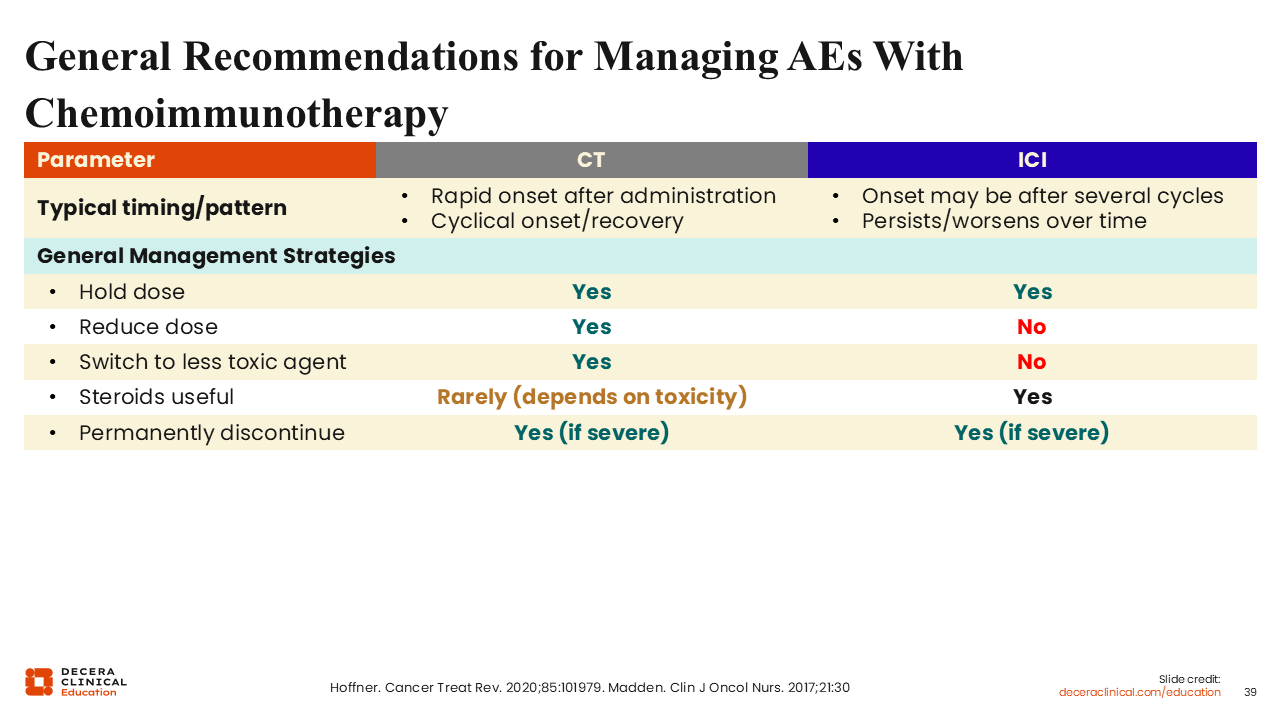
General Recommendations for Managing AEs With Chemoimmunotherapy
When patients are receiving chemoimmunotherapy, it can be challenging to determine whether an AE is more consistent with chemotherapy or with ICI, and the timing can be a useful clue.50 Chemotherapy-related AEs usually have a rapid onset after treatment and tend to follow a cyclical pattern of onset and recovery, whereas immune-related AEs may not appear until after several cycles and can persist or worsen over time.50,51 That distinction matters for management: Holding treatment can be appropriate in either setting, but chemotherapy AEs may also be managed by dose reduction or switching to a less toxic agent, whereas those strategies do not apply to immune-related AEs. Steroids are rarely useful for chemotherapy AEs, depending on the specific event, but they are a standard tool for immune-related AEs. In severe cases, either chemotherapy or immunotherapy may need to be permanently discontinued.
Combination Anti-VEGF(R) + Anti–PD-1/PD-L1 Therapy
Combination anti-VEGF(R) plus anti–PD-1/PD-L1 therapy has demonstrated clinical benefit across multiple ICI-naive tumor types and has supported several FDA approvals.52-54 Examples include renal cell carcinoma with pembrolizumab plus axitinib and avelumab plus axitinib, endometrial carcinoma with lenvatinib plus pembrolizumab, and hepatocellular carcinoma with atezolizumab plus bevacizumab.
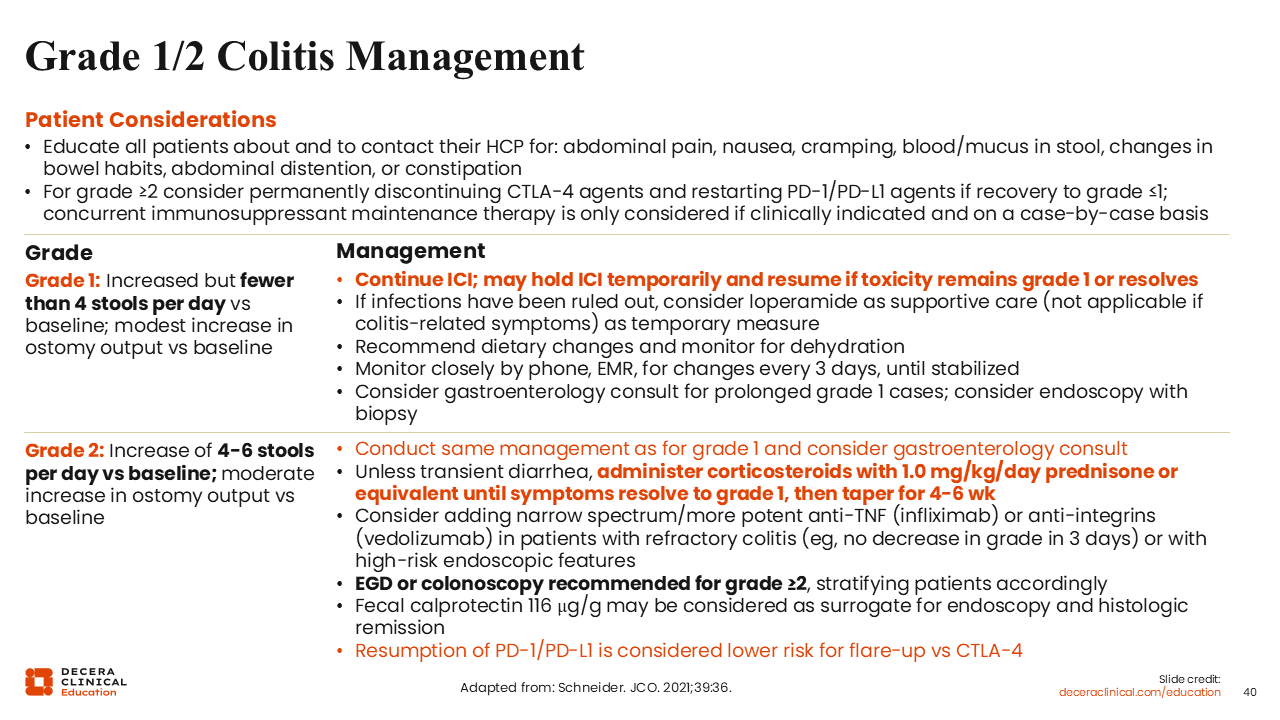
Grade 1/2 Colitis Management
For grade 1/2 immune-related colitis, management depends on symptom severity, whether symptoms are improving, and the clinical context.55 For grade 1 diarrhea, defined as fewer than 4 stools per day over baseline, ICI therapy may be continued with close monitoring, supportive care such as antidiarrheals and hydration, and a stool workup when appropriate. If grade 1 symptoms persist beyond approximately 2 weeks or if there is concern for progression, low-dose prednisone at 1 mg/kg may be started. For grade 2 diarrhea, defined as 4-6 stools per day over baseline, ICI therapy is generally held, supportive measures are continued, and prednisone at 1-2 mg/kg/day is recommended; colonoscopy can also be considered after stool studies. If symptoms improve to grade 1 or resolve, steroids can be tapered over at least 4-6 weeks, and treatment may be resumed in selected cases.
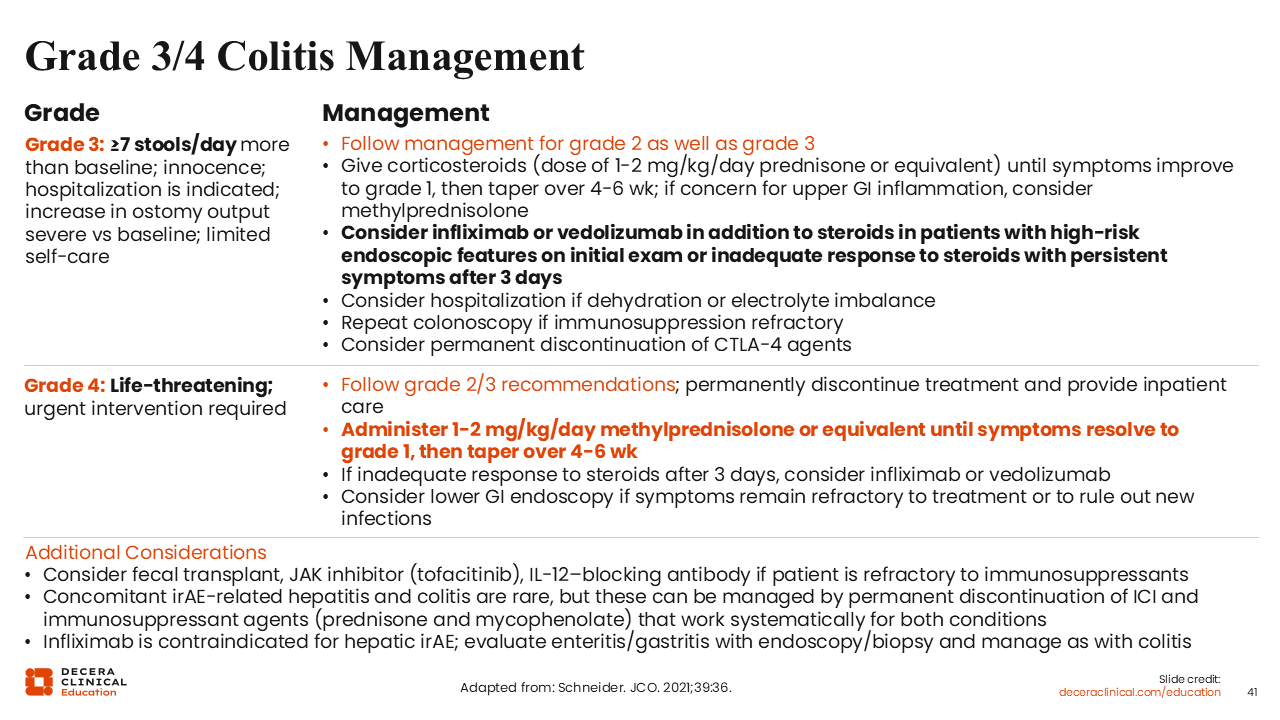
Grade 3/4 Colitis Management
For grade 3 immune-related colitis, defined as 7 or more stools per day above baseline or symptoms severe enough to limit self-care and often require hospitalization, management builds on the grade 2 approach but with more intensive treatment.55 Corticosteroids at 1-2 mg/kg/day of prednisone or equivalent are recommended until symptoms improve to grade 1, followed by a 4- to 6-week taper. In patients with high-risk endoscopic features on initial evaluation or an inadequate response to steroids after 3 days, infliximab or vedolizumab should be considered. Hospitalization may also be needed, particularly when dehydration or electrolyte abnormalities are present, and repeat colonoscopy can be considered in immunosuppression-refractory cases. Permanent discontinuation of CTLA-4 therapy may also be appropriate.
For grade 4 colitis, which is life-threatening and requires urgent intervention, treatment should be permanently discontinued, and the patient should be managed with inpatient care. Methylprednisolone 1-2 mg/kg/day or an equivalent regimen is recommended until symptoms improve to grade 1, followed by a 4- to 6-week taper. If there is still an inadequate response after 3 days of steroids, infliximab or vedolizumab should be considered, and lower gastrointestinal endoscopy may help evaluate refractory symptoms or exclude new infection. Additional refractory options include fecal transplant, tofacitinib, or an IL-12–blocking antibody. Concomitant hepatitis and colitis are uncommon but, when present, may require permanent ICI discontinuation and systemic immunosuppression such as prednisone plus mycophenolate; infliximab is contraindicated for hepatic immune-related AEs.
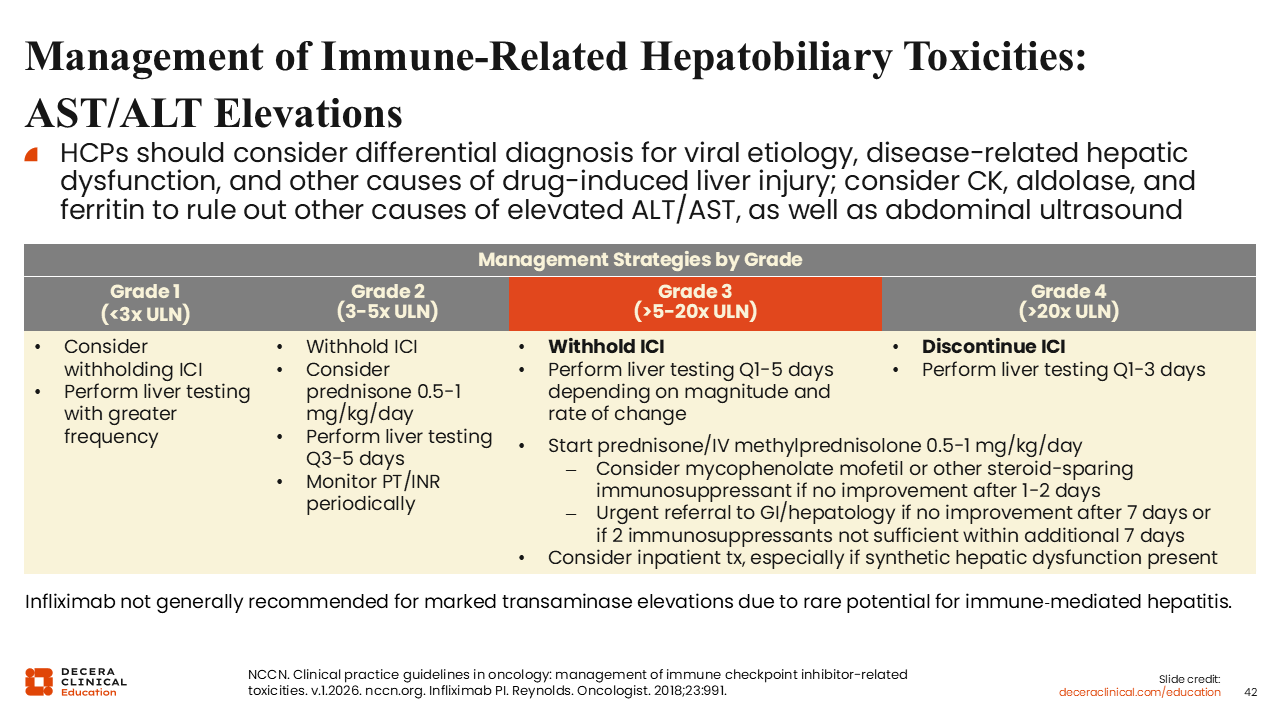
Management of Immune-Related Hepatobiliary Toxicities: AST/ALT Elevations
Immune-related hepatobiliary toxicity should be managed by grade after ruling out other causes of aspartate aminotransferase/alanine aminotransferase elevation, such as viral hepatitis, disease-related liver dysfunction, other drug-induced injury, or muscle-related sources. For grade 1 elevations, defined as less than 3 times the upper limit of normal, treatment may continue with more frequent liver testing. For grade 2 elevations, at 3-5 times the upper limit of normal, the ICI should be withheld, prednisone 0.5-1.0 mg/kg/day can be considered, and liver tests should be repeated every 3-5 days. For grade 3 elevations, 6 to 20 times the upper limit of normal, the ICI should be withheld and prednisone or IV methylprednisolone started, with added immunosuppression or hepatology referral if there is no improvement. For grade 4 elevations, more than 20 times the upper limit of normal, the ICI should be discontinued and inpatient care considered. Infliximab is generally avoided in this setting.
Counseling Patients and Caregivers
Patients and caregivers should be counseled to have realistic expectations for immunotherapy, including that responses may take longer to emerge than with chemotherapy or targeted therapy. They should also be prepared to promptly report new symptoms, carry an immunotherapy wallet card, and understand that appropriate management of immune-related AEs, including treatment interruption or steroids when needed, does not appear to compromise outcomes.
Patient Resources
There are some additional resources that are available,56-58 if you want to explore further any of these discussions we have had today. In terms of counselling patients and caregivers, it is important to set evidence-based expectations for treatment benefit. The benefits from immunotherapy can take longer to emerge than with targeted therapy or even chemotherapy. It is very important to emphasize that patients report symptoms rapidly.
Counseling for patients and caregivers should set evidence-based expectations for immunotherapy, including that benefits may take longer to emerge than with chemotherapy or targeted therapy and may not be appropriate to wait for in patients with high tumor burden or rapidly progressive disease. Patients and caregivers should be told to monitor closely for new symptoms, contact the oncology team promptly, and report any emergency department visits or care from other healthcare professionals. They should also carry an immunotherapy wallet card at all times and receive clear education on immune-related AE management, including that stopping ICIs because of AEs does not worsen survival and that treating immune-related AEs with steroids does not appear to compromise response or survival.