CME
Expert Think Tank: New Developments in Immunotherapy-Based Management of Gastric/GEJ Cancers Across the Disease Continuum
Physicians: Maximum of 0.50 AMA PRA Category 1 Credit™
Released: June 26, 2026
Expiration: December 25, 2026

Activity
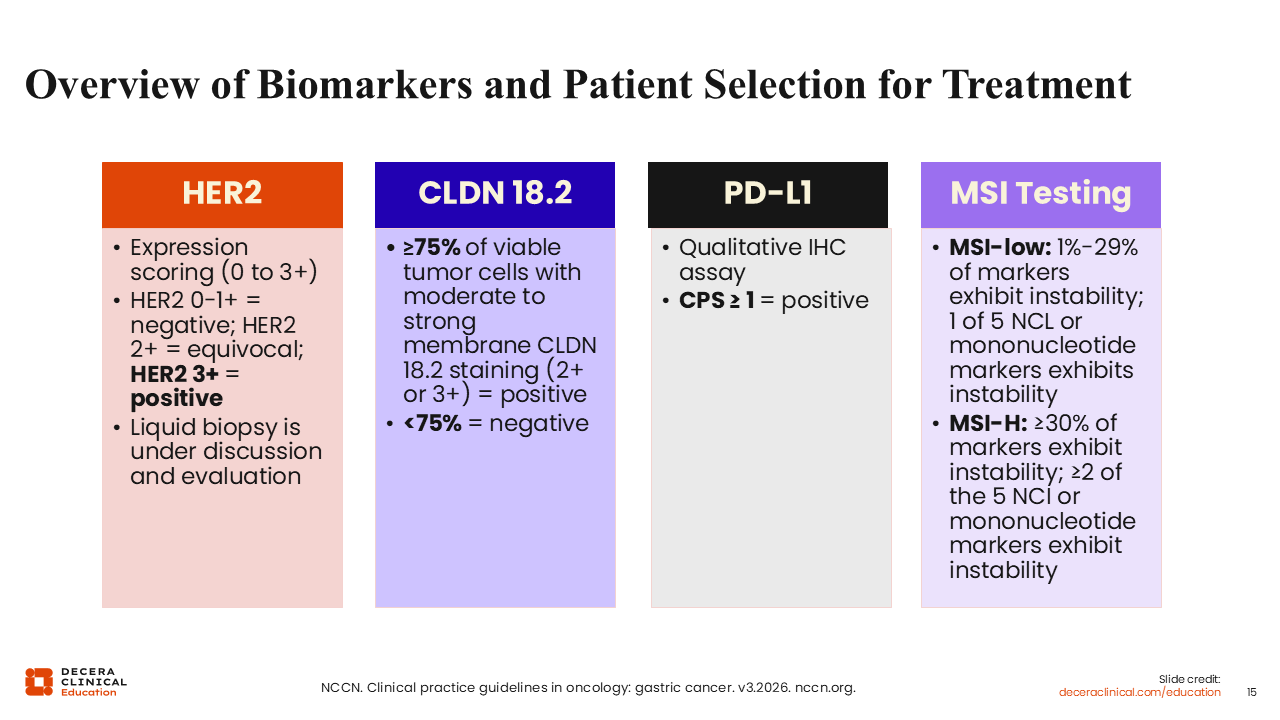
Overview of Biomarkers and Patient Selection for Treatment
There are 4 biomarkers that are recommended by all major guidelines for patients with untreated metastatic gastroesophageal adenocarcinoma. HER2 expression is currently tested by immunohistochemistry (IHC) but eventually liquid biopsy could be considered as an option in the future. Although HER2 overexpression occurs in a small percentage of gastric cancers, it can guide the selection of targeted therapies for treatment. CLDN 18.2 is a standardized IHC test, and positivity is defined as ≥75% tumor cells expressing CLDN 18.2 at 2+ or 3+ intensity. Overexpression of HER2 also guides the treatment selection with approved and emerging targeted agents. PD-L1 is tested by various antibodies and CPS is a method of scoring that is very commonly used, but there are other scoring methods that will become usable going forward. The MSI high testing to detect DNA repair defects because of dMMR can be done by IHC or polymerase chain reaction. Most institutions use IHC for the 4 DNA damage repair proteins (MLH1, PMS2, MSH2, MSH6).8
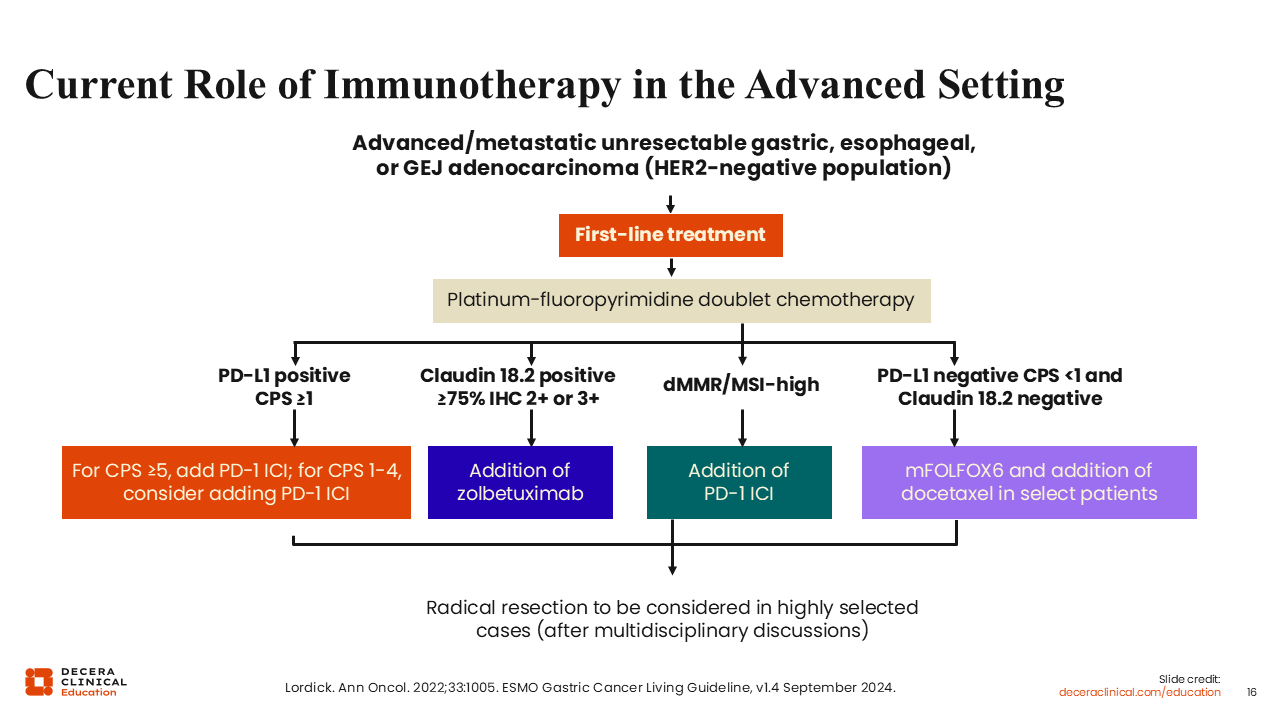
Current Role of Immunotherapy in the Advanced Setting
The standard of care in advanced/metastatic unresectable gastric cancer or GEJ carcinoma includes doublet chemotherapy unless they are MSI high. However, additional therapies can be added to the doublet chemotherapy, depending on what biomarkers are present in the tumor. Immunotherapy should be considered for first-line treatment in patients with advanced or metastatic and unresectable gastric, esophageal, or GEJ adenocarcinoma who have PD-L1–positive tumors (37%) with CPS ≥1. Patients with gastroesophageal adenocarcinoma tumors who have higher CPS scores of their PD-L1–positive tumors (CPS ≥5) have a better OS compared with those with CPS <5. Many practices administer anti–PD-1 therapy to patients with higher PD-L1 CPS.
For first-line therapy, zolbetuximab is the targeted therapy used with CLDN 18.2–positive tumors (30%). There is a movement to add immunotherapy to that group as well. In many practices, immunotherapy is not added when CLDN 18.2 is positive, but PD-L1 is low (CPS 0-4). Similarly, when CPS is ≥5 and CLDN 18.2 is positive, zolbetuximab may not be added to the double-positive groups. Currently, there is no clear evidence to combine zolbetuximab and an anti–PD-1 therapy. However, this question may be answered in the LUCERNA trial.
With the MSI-high population, these patients benefit from the addition of immunotherapy. In many of these patients, chemotherapy does not need to be given because there is no evidence that chemotherapy adds any benefit for these patients. For patients with MSI-high disease, chemotherapy can be used if immunotherapy fails, which it does in some patients. In rare patients with triple-negative disease—PD-L1 negative (<1), CLDN 18.2 negative (<75%), MSI-high negative (ie, MSI-low or 1-29% of markers exhibiting instability)—chemotherapy needs to be used. In that population, next-generation sequencing (NGS) can hopefully find new targets (such as tumor mutational burden high and tumor agnostic biomarkers). Other targets can be determined by NGS testing and are highly recommended in second or third lines.14-16
Tools to Assess Biomarkers for Gastroesophageal Cancers
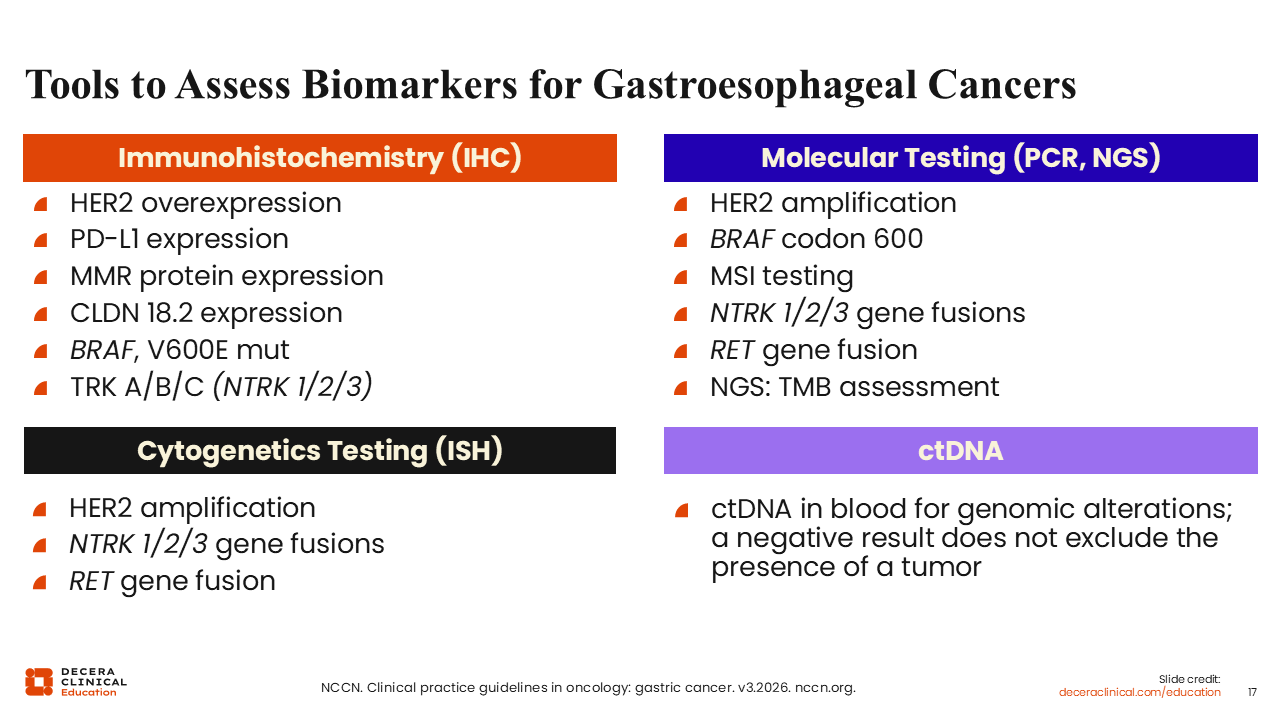
How can healthcare professionals assess gastroesophageal cancer biomarkers? This is an ongoing challenge because most of the time when there is a tumor from an endoscopic biopsy, it is a small fragment of tissue. Thus, if you have a small amount of tissue, how do you assess all of these biomarkers? IHC is the preferred method of approaching biomarker testing in the setting of gastric and gastroesophageal cancers as well as cytogenetic testing for certain genes, like HER2 and TRK.
Other methods for biomarker testing are polymerase chain reaction, NGS, or circulating tumor DNA. Biomarker testing will improve moving forward. In addition, it will not just be DNA but also proteins and RNA.8
First-line Therapy for Unresectable Locally Advanced, Recurrent, or Metastatic Gastroesophageal Cancers
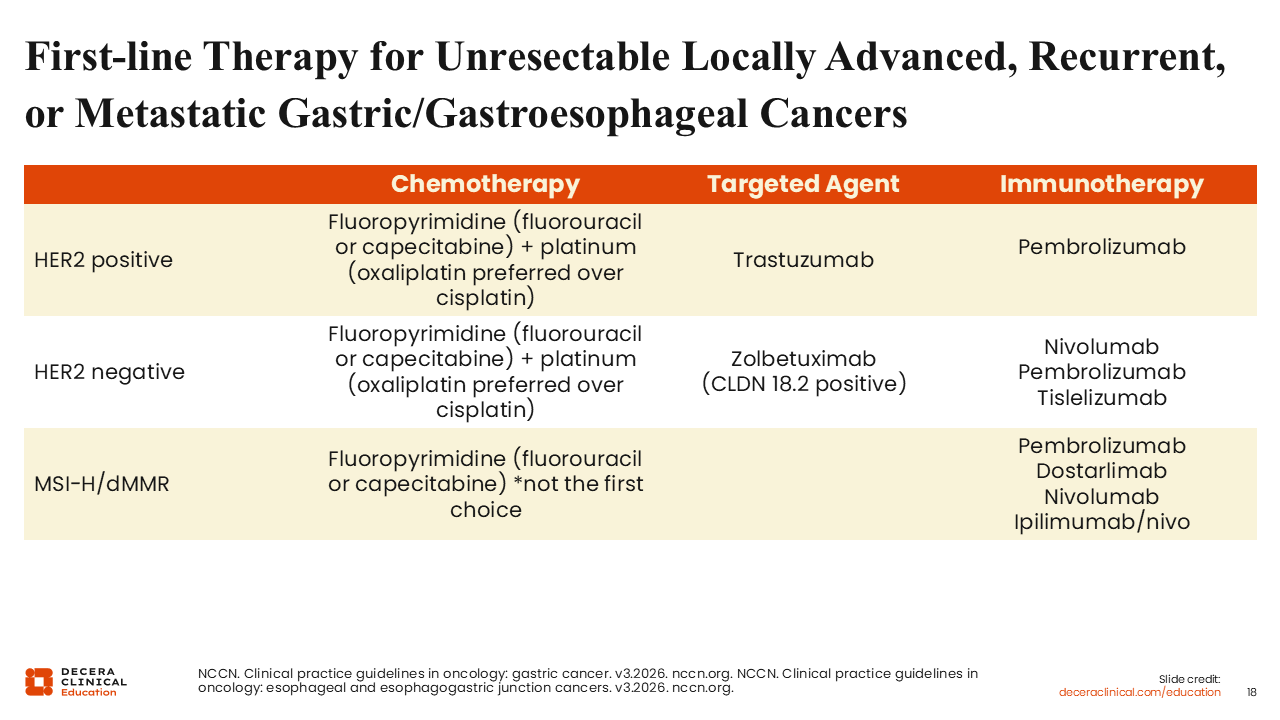
Regarding first-line therapy for unresectable and metastatic gastroesophageal cancers, therapy selection depends on the tumor biomarker. For example, if the tumor is HER2 positive (IHC 2+ or 3+), then the patient should receive trastuzumab plus chemotherapy. With equivocal IHC 2+, this must be reflexed to in situ hybridization for HER2 status and eligibility for HER2-targeted therapy. If the tumor is PD-L1 positive (CPS ≥1), pembrolizumab can be added. In HER2-negative patients (0 or 1), one can use chemotherapy with or without zolbetuximab, depending on CLDN 18.2 positivity (≥75% of viable tumor cells exhibiting moderate to strong staining), and immunotherapy with PD-L1 positivity. However, if CLDN 18.2 is negative (<75%), one can use chemotherapy plus immunotherapy with PD-L1 positivity. With MSI-high tumors (≥30% markers exhibiting instability), chemotherapy is not recommended because these patients are more responsive to immunotherapy. Therefore, healthcare professionals can start a patient with immunotherapy and then add chemotherapy later.8,17
Second-line or Subsequent Therapy for Unresectable Locally Advanced, Recurrent, or Metastatic Gastric Cancers
Unfortunately, most patients with unresectable, advanced, recurrent, and metastatic gastric or GEJ cancers will fail first-line treatment and need second-line or even third-line treatment. Combination regimens can be considered for subsequent therapy. For example, ramucirumab plus paclitaxel is recommended for the HER2-negative population. Similarly, fam-trastuzumab deruxtecan is recommended for the HER2-positive population. In addition, there are single agents like docetaxel, paclitaxel, irinotecan, or fluorouracil, and sometimes the combination of trifluridine plus tipiracil, which is an oral compound, can be considered. Other recommended treatment options are available, depending on what was used previously. For example, ramucirumab can be continued or irinotecan plus cisplatin can be given, which can have treatment-limiting AEs. Alternatively, the combination of fluorouracil and irinotecan plus ramucirumab or docetaxel plus irinotecan are options, but these also have treatment-limiting AEs.
Finally, there are tumor agnostic recommendations that require biomarker testing on the tumor sample. For example, NGS testing will resolve whether the tumor has an NTRK gene fusion, and if it does, that determines the most appropriate, targeted therapy (eg, entrectinib, larotrectinib, or repotrectinib) for a patient with an NTRK 1/2/3 gene fusion. A similar scenario is also applicable for a BRAF mutation (dabrafenib plus trametinib) or high tumor mutational burden (pembrolizumab).8,17

FDA Decisions in 1L Advanced Gastric/GEJ: Restrict Anti–PD-1 Class to HER2-/PD-L1 CPS ≥1 in MSS Disease
In 2024, an issue arose regarding whether patients who have PD-L1–negative tumors (CPS <1) should be treated with PD-L1 ICI immunotherapy given the benefits vs risks. The FDA congregated a group of ODAC members and requested data submitted by manufacturers regarding immunotherapy. After reviewing the documents, the ODAC members suggested that patients who have PD-L1–negative tumors (<1) should not receive anti–PD-1 agents, such as pembrolizumab, nivolumab, or tislelizumab, because those patients do not seem to benefit and they experience AEs. All prescribing labels were changed to reflect that these immunotherapy drugs should be used for PD-L1–positive (CPS ≥1) tumors. Tislelizumab, which is the third anti–PD-1 molecule, was approved by the FDA only for patients with PD-L1–positive (≥1) tumors.18-20
Phase III CheckMate 649: 5-Year Follow-up With Nivolumab
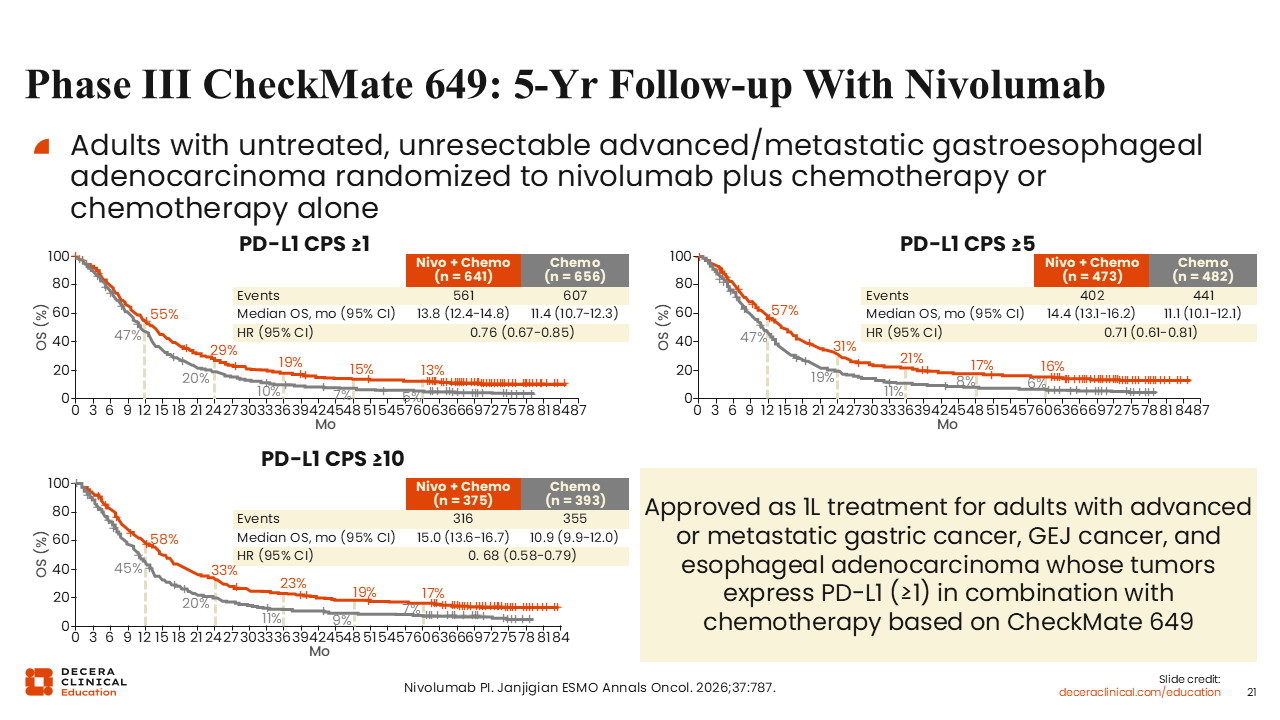
CheckMate-649 was a pivotal phase III trial with a 5-year follow-up. In this study, adults with previously untreated, unresectable, advanced or metastatic gastroesophageal adenocarcinoma were randomized to receive either nivolumab plus chemotherapy (n = 789) or chemotherapy alone (n = 792). The primary endpoints were OS and PFS. After a minimum follow-up of 60.1 months, the OS benefit (HR: 0.71, P <.0001) with nivolumab plus chemotherapy vs chemotherapy (mOS: 14.4 vs 11.1 months, respectively) in patients with PD-L1 CPS ≥5 was sustained. The OS primary endpoint was met in a previous interval (2-3 years) as nivolumab plus chemotherapy demonstrated superior OS. The OS graphs for cohorts with PD-L1–positive CPS ≥1 (HR: 0.76), CPS ≥5 (HR: 0.71), and CPS ≥10 (0.68) are shown in the slide. Results show with higher CPS, a better outcome is achieved from nivolumab. The survival curve for CPS ≥5 has a tail of approximately 15% to 18%, which is remarkable. But looking at this smaller population with CPS ≥10, one sees a higher tail at 17% to 20%. Therefore, if a tumor has high CPS, one can discuss the possibility of very long-term benefit or even cure with the patient. Based on the outcome of this trial, nivolumab plus chemotherapy received approval as first-line therapy for unresectable advanced, HER2-negative gastric cancer, GEJ cancer, and esophageal adenocarcinoma. No new safety concerns were observed, with grade 3/4 treatment-related AEs occurring in 60% of patients receiving nivolumab plus chemotherapy (95% any grade) and 45% of patients receiving chemotherapy (89% any grade).19,21
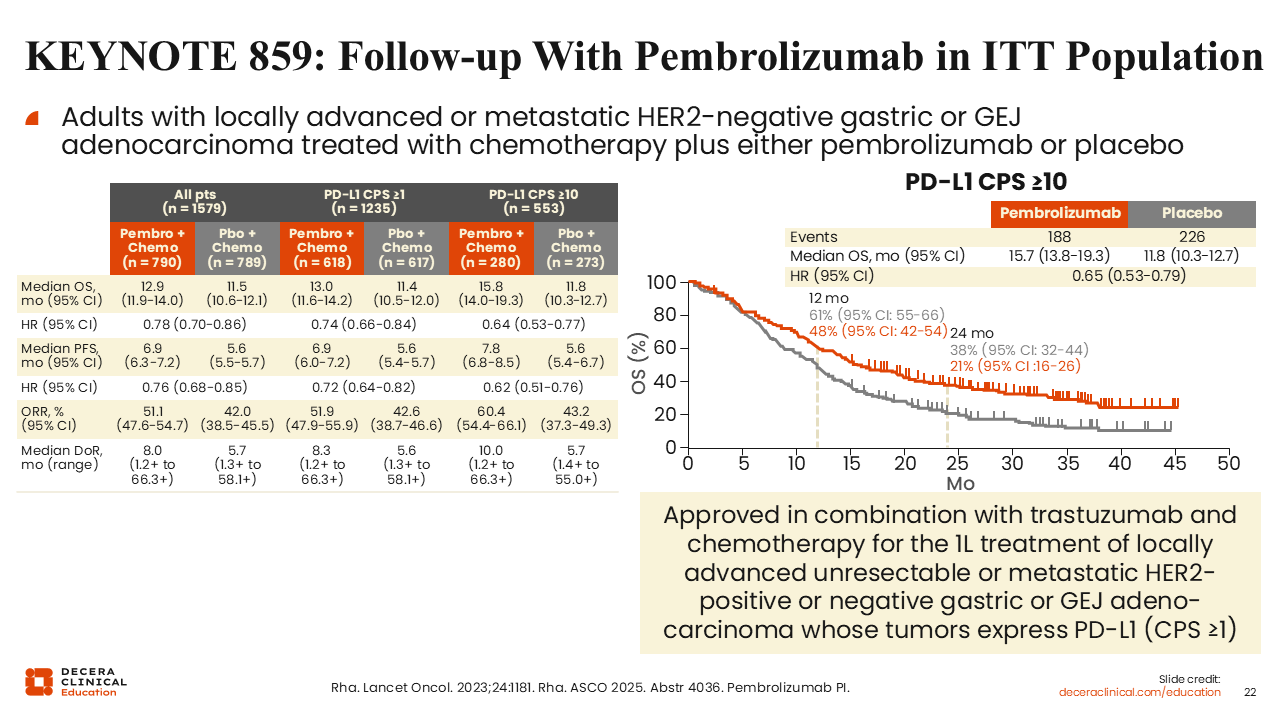
KEYNOTE 859: Follow-up With Pembrolizumab in ITT Population
Similar results are seen with KEYNOTE 859. This randomized, double-blind phase III clinical study evaluated the efficacy of pembrolizumab plus chemotherapy (cisplatin combined with 5-fluorouracil or oxaliplatin combined with capecitabine) vs placebo in combination with chemotherapy for the treatment of HER2-negative advanced gastric or GEJ adenocarcinoma in adult participants. The primary endpoint of the study was OS among all participants and then cohorts with positive PD-L1 (CPS ≥1 and CPS ≥10). The mOS for all patients treated with pembrolizumab plus chemotherapy was 12.9 months (range: 11.9-14.0) vs placebo plus chemotherapy at 11.5 months (range: 10.6-12.1) (HR: 0.78). For patients with CPS ≥1, the mOS was 13.0 months (range: 11.6-14.2) vs 11.4 months (range: 10.5-12.0) (HR: 0.74), and for patients with CPS ≥10, the mOS was 15.8 months (range: 14.0-19.3) vs 11.8 months (range: 10.3-12.7) (HR: 0.64). Trends for overall response rate (ORR) and PFS mimicked the results of OS. In conclusion, patients with CPS ≥10 have a remarkable tail lasting beyond 3 years. Grade 3-5 treatment-related AEs occurred in 59.4% of patients receiving pembrolizumab plus chemotherapy (95.7% any grade) and 51.3% of patients receiving placebo plus chemotherapy (93.5% any grade). Patients receiving pembrolizumab reported a higher incidence of hypothyroidism.18,22,23
RATIONALE-305: Tislelizumab in Advanced Unresectable or Metastatic Gastric or GEJ Adenocarcinoma
The RATIONALE-305 study was an international, double-blind, placebo-controlled, randomized phase III trial that enrolled treatment-naive adults (N = 997) with locally advanced, unresectable, or metastatic gastric or GEJ carcinoma, no HER2+ disease, and ECOG PS 0/1. They were randomized to receive either tislelizumab 200 mg IV plus chemotherapy (capecitabine and oxaliplatin or 5-fluorouracil and cisplatin) (n = 501) or placebo plus chemotherapy (n = 496) for up to 6 cycles. Then participants would receive either tislelizumab or placebo with optional capecitabine in either regimen until progressive disease or unacceptable toxicity. Patients were continued on immunotherapy for up to 2 years. The primary endpoint was OS in a very selective population of high PD-L1 (≥5). Here the PD-L1 was scored by another method, tumor-associated positivity (TAP). TAP is a visual method for assessing the tumor, which was designed to simplify PD-L1 positivity and has a high level of concordance with CPS in gastric cancer and GEJ adenocarcinoma. The secondary endpoints were PFS, ORR, duration of response, and safety (NCT03777657).24

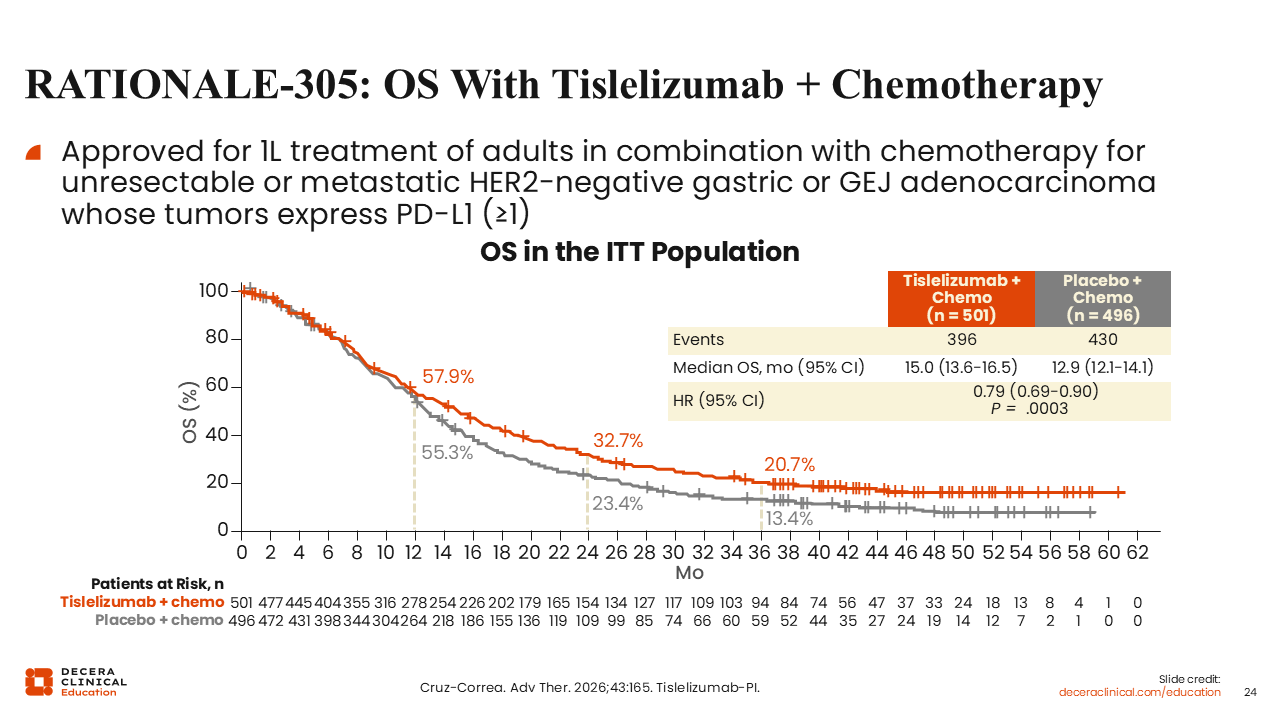
RATIONALE-305: OS With Tislelizumab + Chemotherapy
Trial results from RATIONALE-305 demonstrated superior OS (HR: 0.79; P = .0003) in the intention-to-treat population of tislelizumab plus chemotherapy vs placebo plus chemotherapy (15.0 vs 12.9 months, respectively), showing a clear advantage of the addition of tislelizumab. Based on the results of this trial, tislelizumab was approved for first-line treatment of adults in combination with chemotherapy for unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumors express PD-L1 (CPS ≥1). All 3 ICIs, nivolumab, pembrolizumab, and tislelizumab, seem to produce very similar results, and here there is a tail of patients who are living beyond 3 years, which is highly desirable. Treatment-related AEs occurred in patients receiving tislelizumab plus chemotherapy (97.0%) and placebo plus chemotherapy (96.4%), with some at grade ≥3 AEs (54.0% and 49.8%, respectively). Among the most common AEs was a decrease in neutrophil and platelet counts.20,24
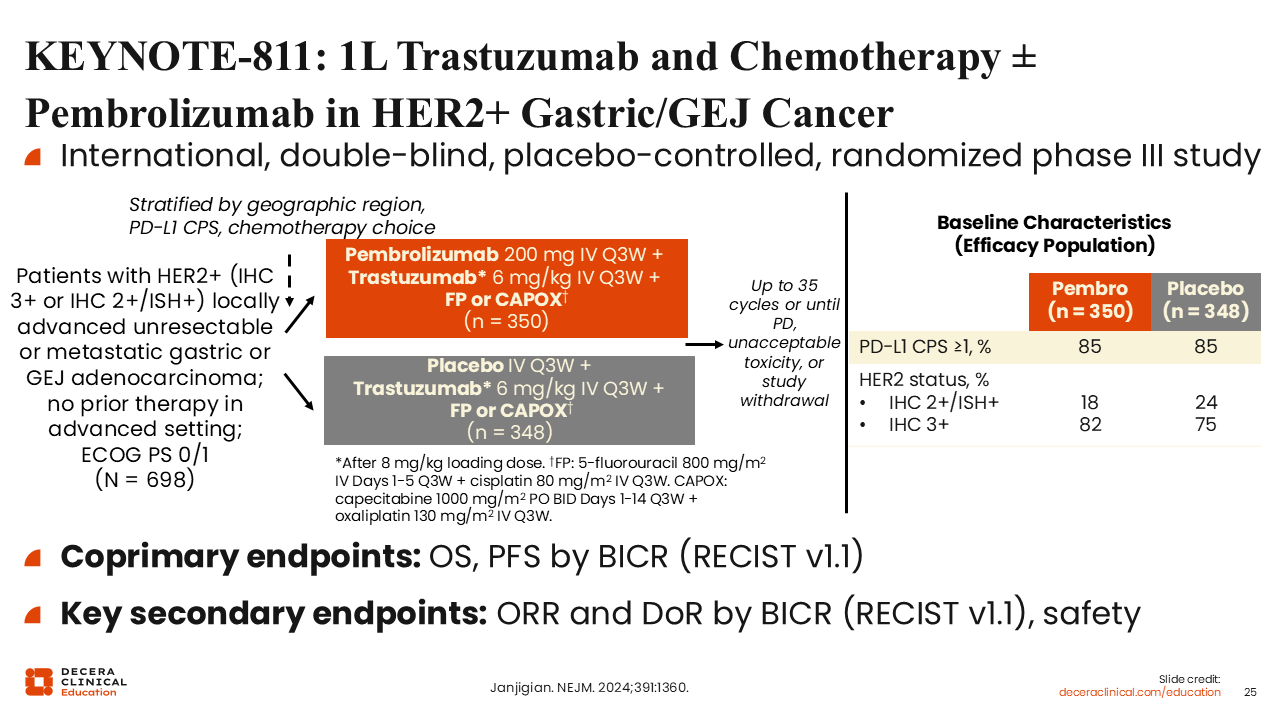
KEYNOTE-811: 1L Trastuzumab and Chemotherapy ± Pembrolizumab in HER2+ Gastric/GEJ Cancer
KEYNOTE-811 was an international, double-blind, placebo-controlled, randomized phase III study of 698 patients with HER2-positive tumors (IHC/in situ hybridization 2+ or 3+) with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma who were evaluated for treatment with chemotherapy (5-fluorouracil plus cisplatin or capecitabine plus oxaliplatin) plus trastuzumab with either a placebo (n = 348) or pembrolizumab (n = 350). Treatment was planned for up to 35 cycles or until progressive disease, study withdrawal, or unacceptable toxicity. Initially, there was no discrimination between patients with PD-L1–positive and PD-L1–negative disease. Approximately 85% of these patients had positive PD-L1 testing and most HER2 results were 3+, which indicates a favorable result for the patient. The coprimary endpoints were OS and PFS.25
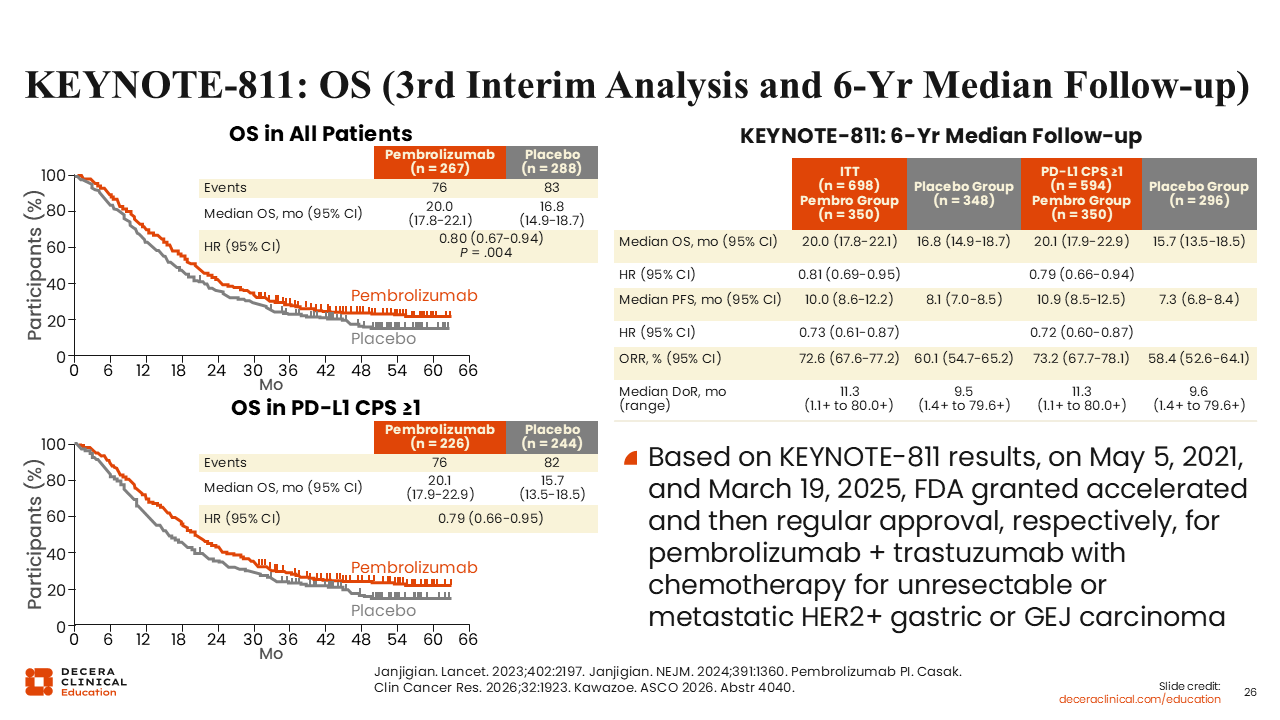
KEYNOTE-811: OS (3rd Interim Analysis)
In the intention-to-treat population, the results show a mOS of 20.0 months in the cohort treated with pembrolizumab and 16.8 months with the placebo (HR: 0.80). When positive PD-L1 is used (CPS ≥1) to stratify the patient cohorts, then the mOS is 20.1 months and 15.7 months, respectively (HR: 0.79). In addition, the area between the curves suggests the experimental agent produces benefit for patients, but there is a statistically significant borderline advantage. Thus, for all patients, there is an advantage to add pembrolizumab (P = .004). However, with tumors that have CPS ≥1, there is a greater advantage. When these data were reviewed by the FDA, it became clear with a HER2-positive but PD-L1 negative tumor, providers should not use pembrolizumab because patients actually do worse.
Based on the KEYNOTE-811 results, the FDA granted approval for pembrolizumab plus trastuzumab with chemotherapy for unresectable or metastatic HER2-positive gastric or GEJ carcinoma. Treatment-related AEs occurred in patients in the pembrolizumab group with some at grade ≥3 AEs (58%) as well as in the placebo group (51%). In each cohort, treatment-related AEs leading to death occurred in 1% of patients. The most common AEs in the pembrolizumab group vs placebo, respectively, were diarrhea (47% vs 42%), nausea (44% vs 44%), and anemia (31% vs 33%).18,25-28
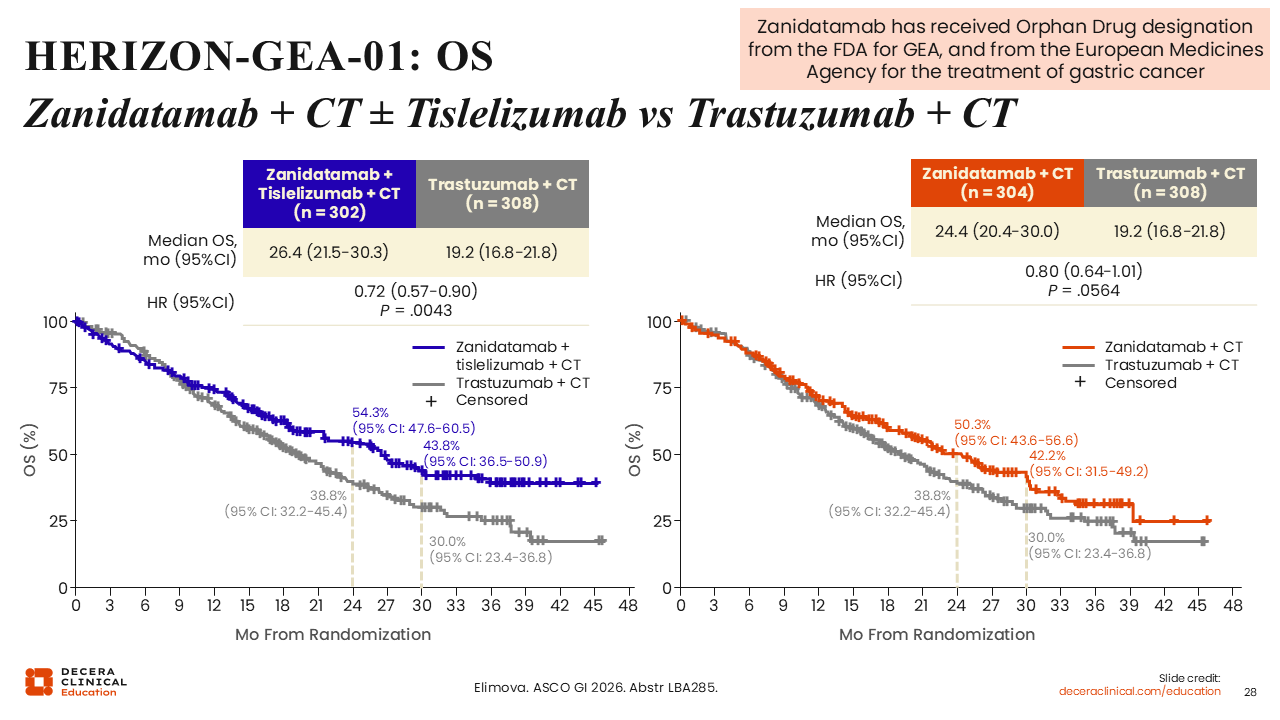
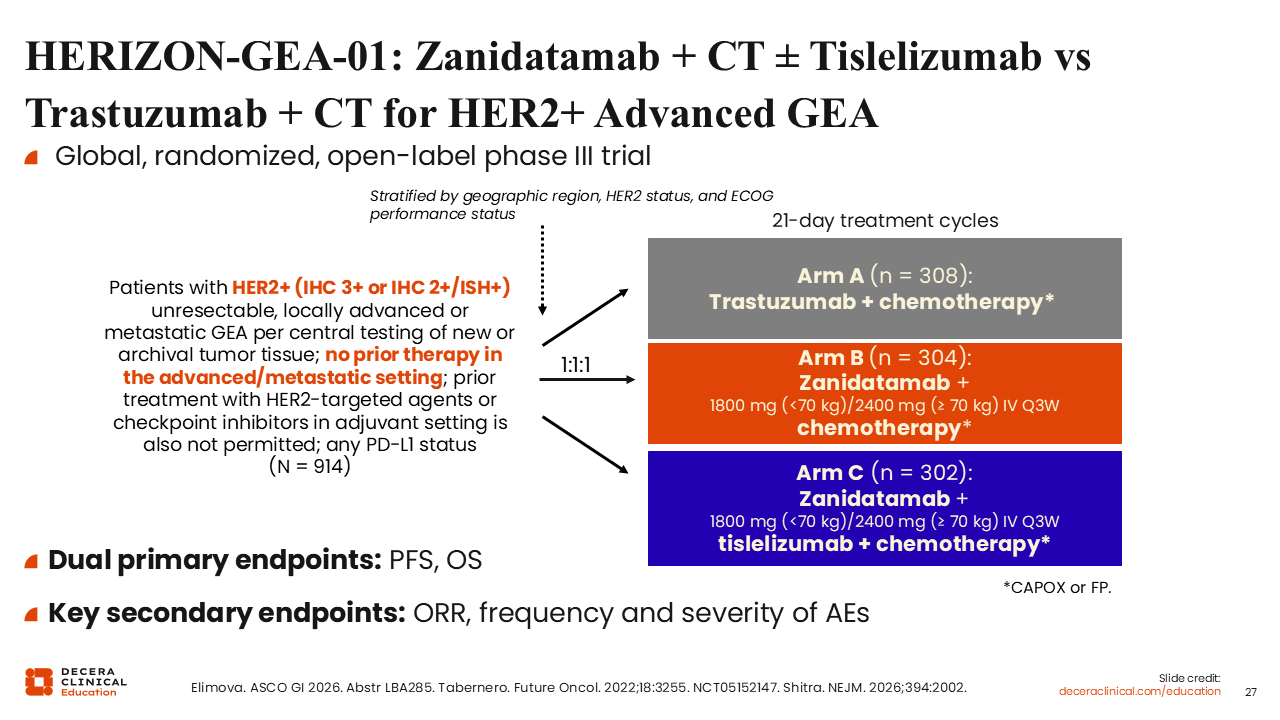
HERIZON-GEA-01: Zanidatamab + CT ± Tislelizumab vs Trastuzumab + CT for HER2+ Advanced GEA
The phase III HERIZON-GEA-01 trial is a global, randomized, open-label trial of the investigational agent zanidatamab that enrolled 914 treatment-naive participants with HER2-positive, unresectable, locally advanced or metastatic gastroesophageal adenocarcinoma per central testing of new or archival tumor tissue. The participants were randomized 1:1:1 to either trastuzumab plus chemotherapy (n = 308), zanidatamab plus chemotherapy (n = 304), or zanidatamab plus tislelizumab and chemotherapy (n = 302). The 2 primary endpoints assessed were OS and PFS (NCT05152147).29-31
HERIZON-GEA-01: OS—Zanidatamab + CT ± Tislelizumab vs Trastuzumab + CT
Among participants with HER2-positive advanced gastroesophageal adenocarcinoma, HERIZON-GEA-01 results demonstrated that the OS was longer with zanidatamab plus tislelizumab and chemotherapy than with trastuzumab and chemotherapy (mOS: 26.4 vs 19.2 months; HR: 0.72; P = .0043). Additional analyses are planned to assess zanidatamab plus chemotherapy, which showed mOS of 24.4 months compared with 19.2 months with trastuzumab plus chemotherapy (HR: 0.80; P = .0564). Rates of grade ≥3 treatment-related AEs were 83.3% with zanidatamab plus tislelizumab and chemotherapy, 73.8% with zanidatamab plus chemotherapy, and 74.5% with trastuzumab plus chemotherapy. The most commonly reported treatment-related AE was diarrhea at 24.8%, 20.0%, and 12.9%, respectively. As a result of HERIZON-GEA-01, the FDA is evaluating and reviewing the data of zanidatamab for gastric/GEJ cancer with a decision expected later in 2026.29