CME
Expert Think Tank: New Developments in Immunotherapy-Based Management of Gastric/GEJ Cancers Across the Disease Continuum
Physicians: Maximum of 0.50 AMA PRA Category 1 Credit™
Released: June 26, 2026
Expiration: December 25, 2026

Activity
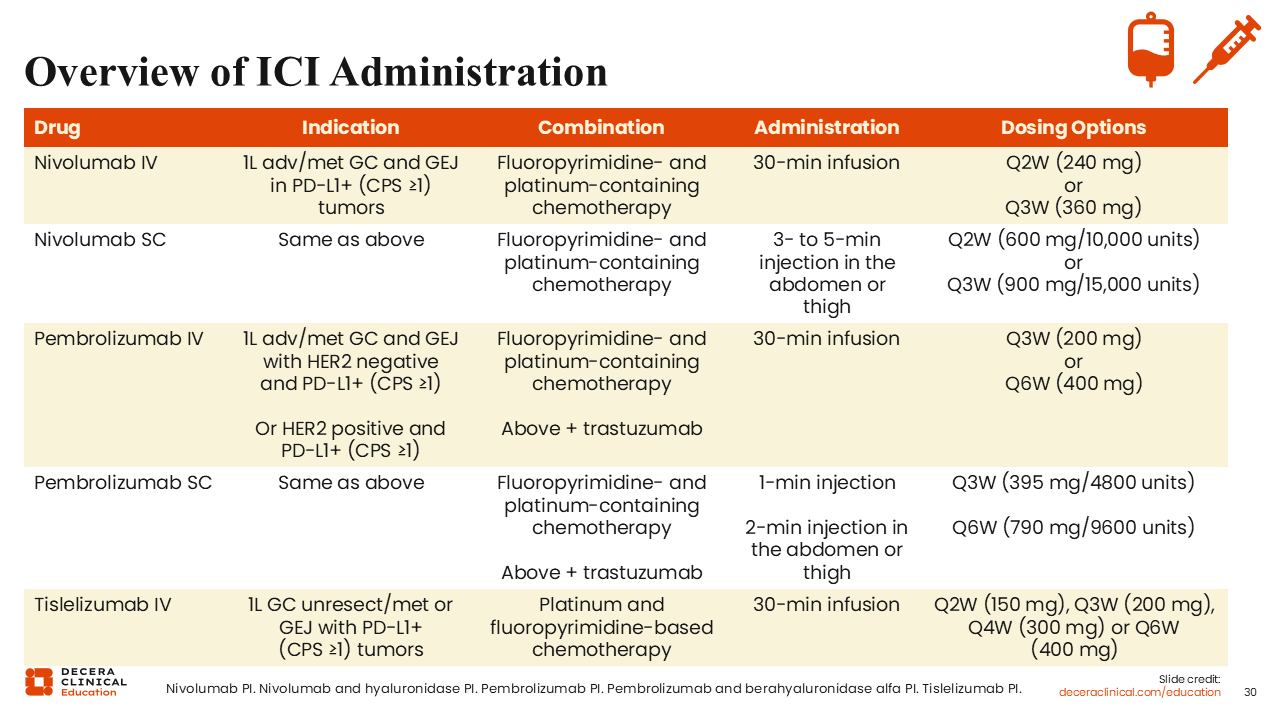
Overview of ICI Administration
Another important dimension of immunotherapy in gastrointestinal tumors is the SC administration of immune checkpoint inhibitor drugs. Both nivolumab and pembrolizumab can be given subcutaneously,32,33 which can produce a lot of advantages for the patient in the future. Using SC injection provides a clear benefit for the patient regarding time as they will not have to sit in the chemotherapy area and wait for the nurse, wait for the infusion, and sometimes wait for observation after administration. Tislelizumab is approved as an IV formulation in this indication and is under evaluation in clinical trials for a SC formulation for non-small-cell lung cancer.18-20,34
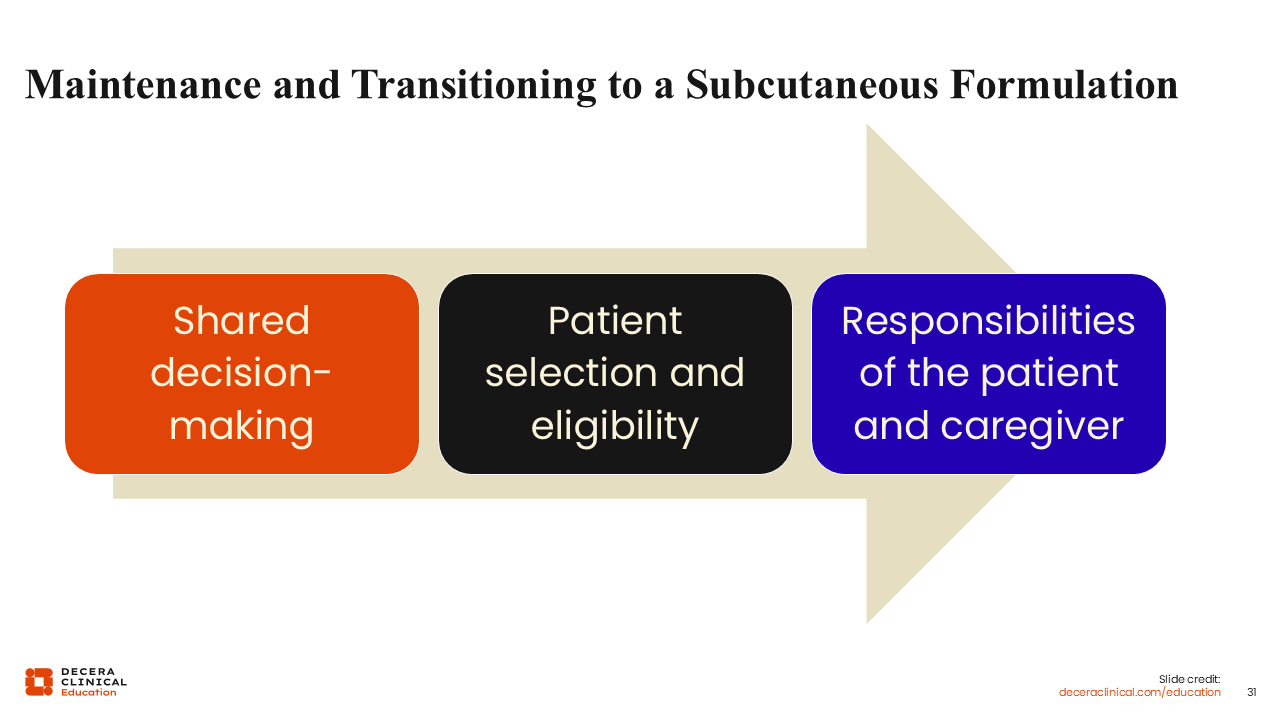
Maintenance and Transitioning to a Subcutaneous Formulation
The transition to an SC formulation includes making a shared decision with the patient and family. Patient selection and eligibility are important because not all patients will be able to self-administer an SC agent, they may not have a family member to do it, or they may not have a local resource like a nurse coming to their homes to inject the agent. Then comes the responsibility of the patient and caregiver with tasks like reporting of toxicity early or having somebody available to take the patient to the emergency department if needed. Therefore, SC formulations may not be suitable for every patient.
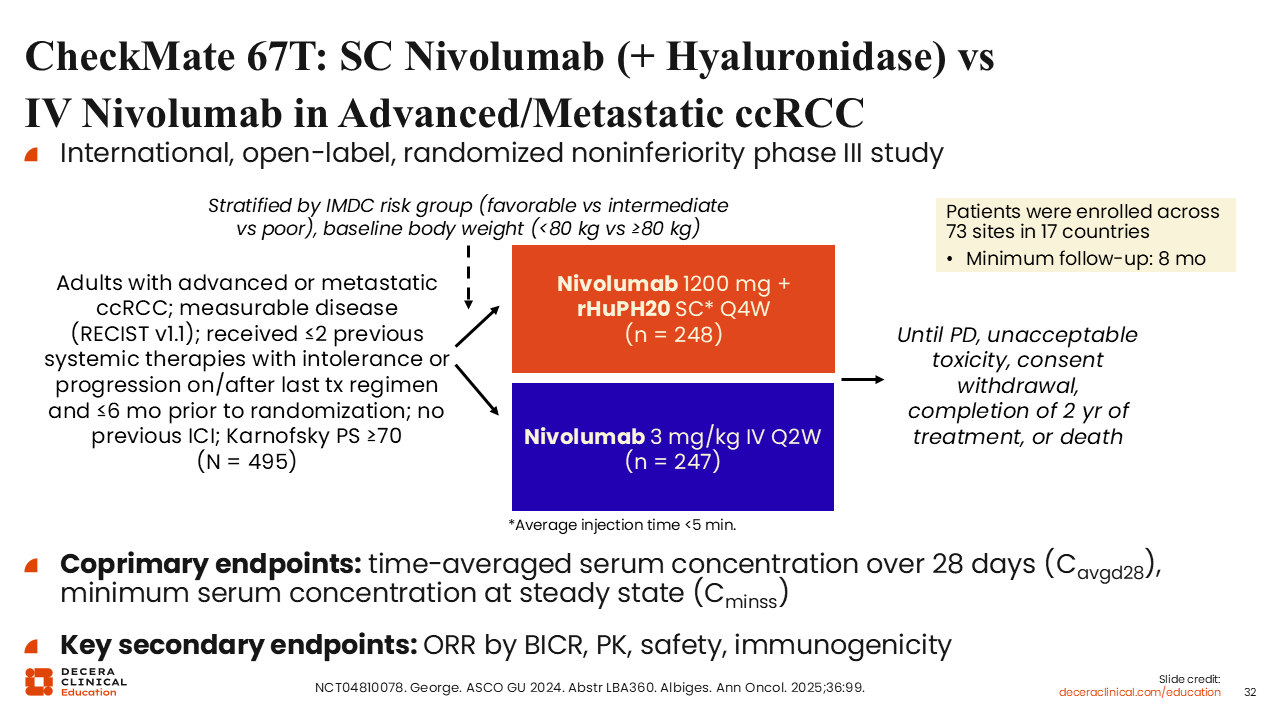
CheckMate 67T: SC Nivolumab (+ Hyaluronidase) vs IV Nivolumab in Advanced/Metastatic ccRCC
CheckMate 67T is one of the pivotal trials that led to the approval of SC nivolumab. CheckMate 67T is an international, open-label, randomized, noninferiority phase III study. The study enrolled 495 adults with advanced or metastatic clear cell renal cell carcinoma and measurable disease by Response Evaluation Criteria in Solid Tumors v1.1 who had received ≤2 previous systemic therapies with intolerance or progression on or after their last treatment regimen and ≤6 months prior to randomization. They also had not received any previous ICIs and had a Karnofsky PS ≥70. The patients were randomized 1:1 to either SC nivolumab (1200 mg + rHuPH20; n = 248) or IV nivolumab (3 mg/kg; n = 247) and administered until progressive disease, unacceptable toxicity, consent withdrawal, 2 years of treatment, or death. The coprimary endpoints were the time-averaged serum concentration over 28 days and the minimum serum concentration at steady state. The goals were to assess pharmacokinetics (PK) and verify that PK and safety are similar. In addition, immunogenicity and ORR of the SC injection were other key secondary endpoints (NCT04810078).35,36
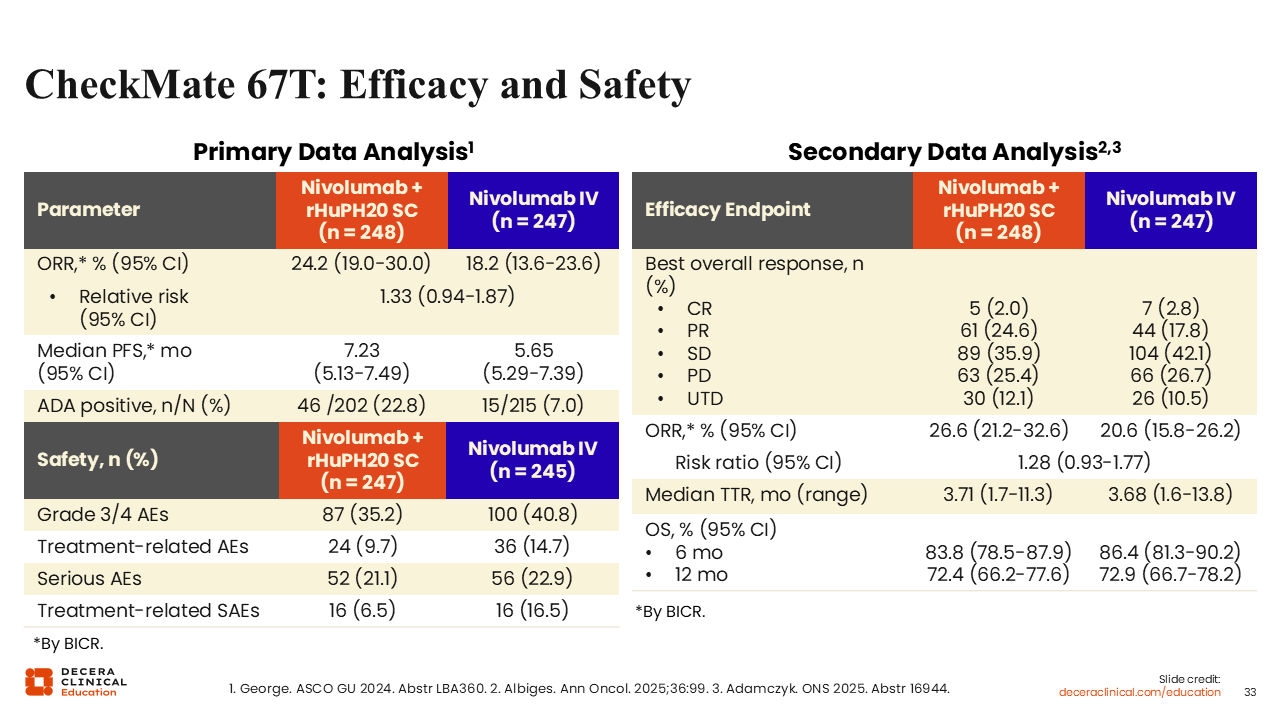
CheckMate 67T: Efficacy and Safety
CheckMate 67T results from the primary data analysis show the ORR of SC nivolumab was 24.2% and IV nivolumab was 18.2% (Relative Risk: 1.33). The median PFS was 7.23 months for SC nivolumab and 5.65 months for IV nivolumab with ADA positive of 22.8% and 7.0%, respectively. The secondary data analysis shows that the CR was 2.0% with SC nivolumab and 2.8% for IV nivolumab. The ORRs were 26.6% and 20.6%, respectively (Relative Risk: 1.28).
Thus, the response rate is similar between SC and IV formulations of nivolumab. Technically, the response was a little higher in SC arm, but I don't think we can say that SC is better for response rate. The data is very similar. The OS for SC nivolumab was 72.4% at 12 months and 72.9% at 12 months for IV nivolumab. Serious AEs, grade 3, and grade 4 AEs were also similar. The median time to response was also very similar in both arms. Therefore, these data are reassuring in the fact that you can use nivolumab subcutaneously and don't have to be concerned whether you are receiving sufficient levels of the drug to be efficacious.35-37
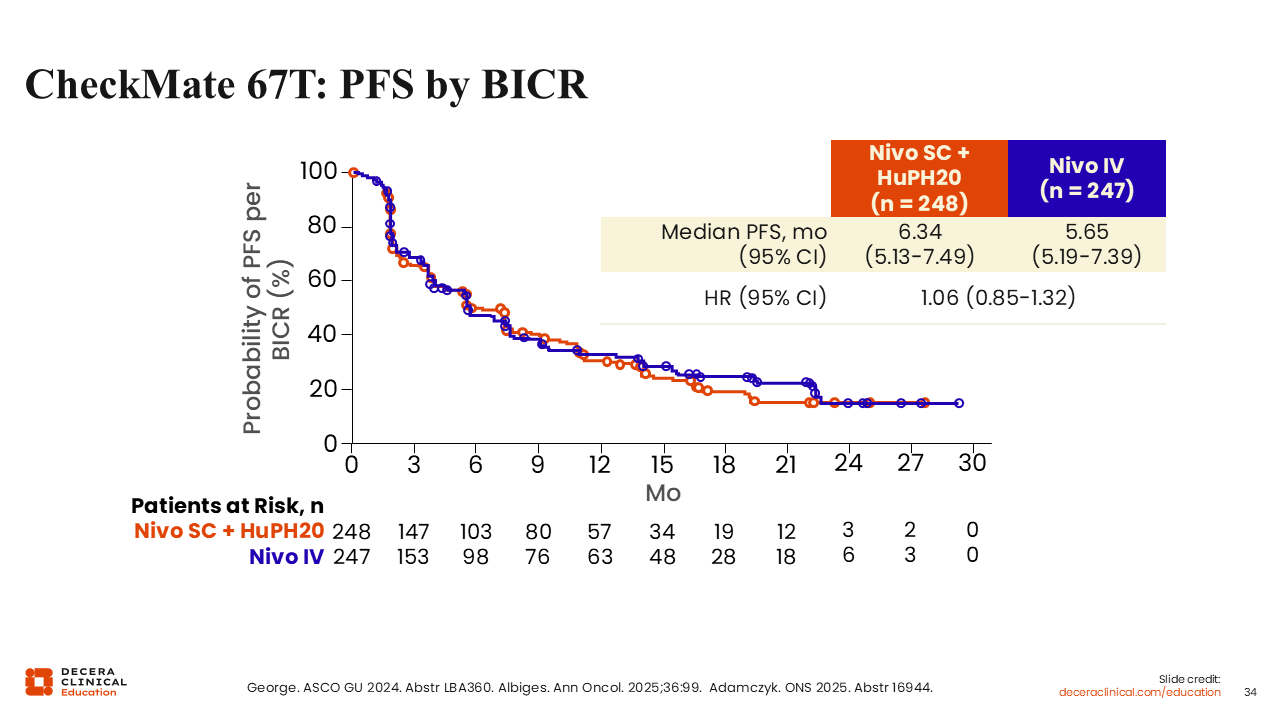
CheckMate 67T: PFS by BICR
Assessing the PFS results measured and interpreted per blinded independent central review, the probability curves are crossing each other multiple times. The median PFS for SC nivolumab is 6.34 months and the median PFS for IV nivolumab is 5.65 months (HR: 1.06). This is reassuring that whether patients receive the drug IV or SC, they will obtain the same PFS advantage.35-37
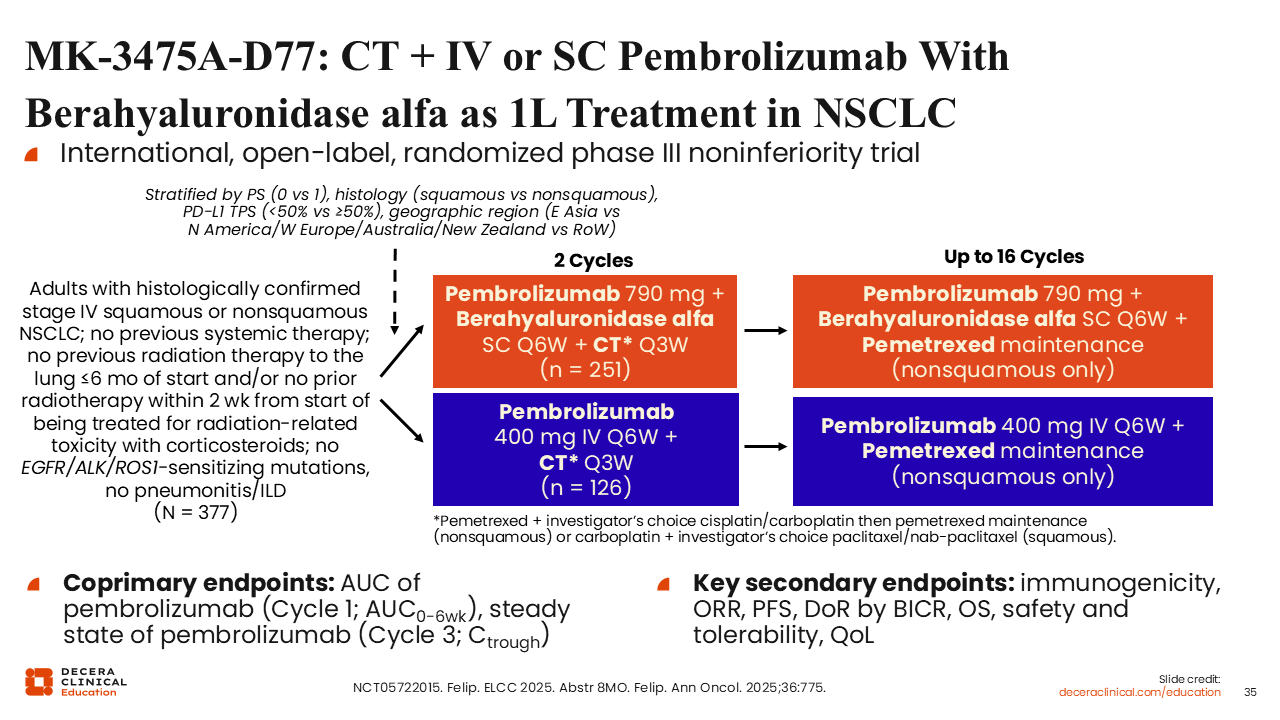
MK-3475A-D77: CT + IV or SC Pembrolizumab With Berahyaluronidase alfa as 1L Treatment in NSCLC
MK-3475A-D77 is an international, open-label, randomized phase III noninferiority trial that evaluated pembrolizumab IV vs SC in adults (N = 377) with histologically confirmed stage IV squamous or nonsquamous non-small-cell lung cancer, no previous systemic therapy, no previous radiation therapy to the lung ≤6 months of start and/or no prior radiotherapy within 2 weeks from the start of being treated for radiation-related toxicity with corticosteroids, no EGFR/ALK/ROS1-sensitizing mutations, and no pneumonitis/interstitial lung disease. For 2 cycles, patients were randomized 2:1 to receive either SC pembrolizumab (790 mg + berahyaluronidase alfa) plus chemotherapy (n = 251) or IV pembrolizumab (400 mg) plus chemotherapy (n = 126). The first 2 cycles included chemotherapy that was either pemetrexed plus the investigator’s choice of cisplatin or carboplatin. For cycles 3 up to 16, the IV or SC pembrolizumab remained the same, but the chemotherapy was switched to pemetrexed maintenance (nonsquamous) or carboplatin plus the investigator’s choice of paclitaxel or nab-paclitaxel (squamous). The coprimary endpoints were the area under the curve for pembrolizumab (cycle 1) and the steady state (cycle 3). The coprimary endpoints were required by the FDA to document PK, and then look at immunogenicity, ORR, PFS, duration of response, OS, tolerability, quality of life, and safety.38
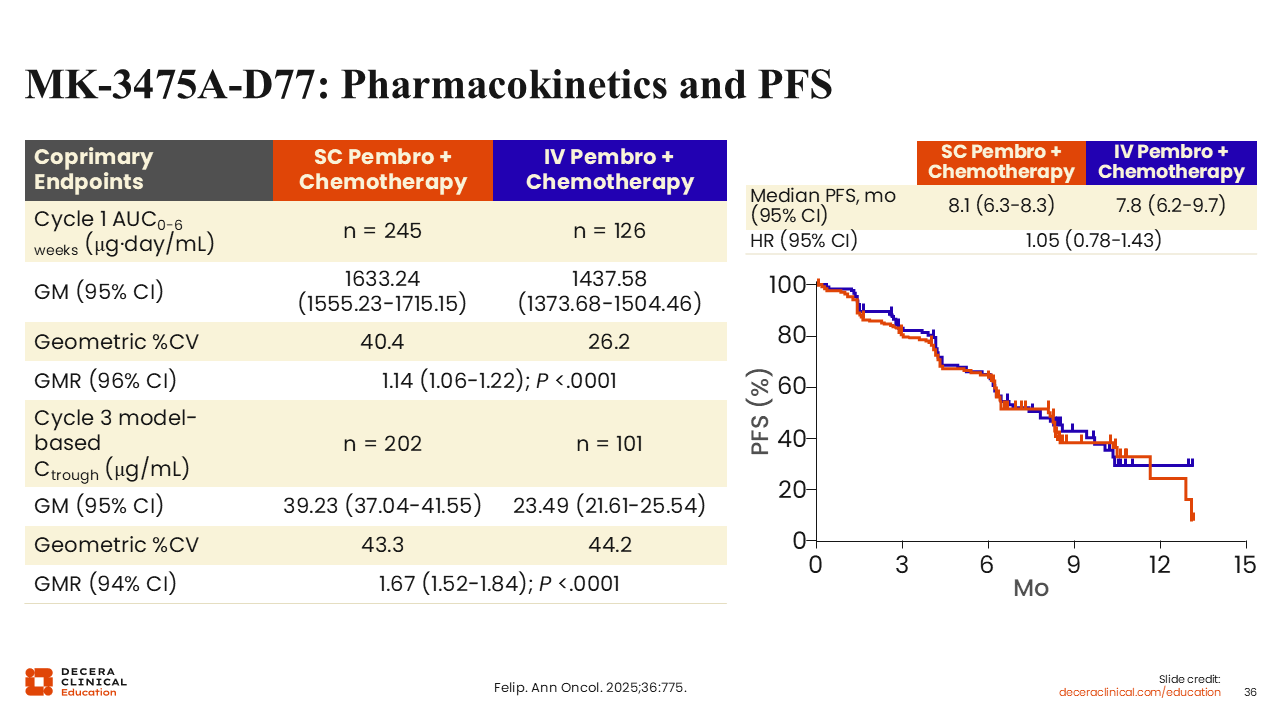
MK-3475A-D77: Pharmacokinetics and PFS
Results of the study demonstrated median PFS of 8.1 months with SC pembrolizumab plus chemotherapy and 7.8 months with IV pembrolizumab plus chemotherapy (HR: 1.05). Similar to results in the previous trial, the PFS curves are overlapping. Therefore, there should not be a concern that if you give pembrolizumab SC, you're going to have inferior results. No such evidence for this concern exists. The other parameters were shown as area under the concentration curves (1633.24 with SC and 1437.58 with IV; Geometric Mean Ratio: 1.14; P < .0001), and the steady state of pembrolizumab (Geometric Mean: 39.23 vs 23.49; Geometric Mean Ratio: 1.67; P <.0001). This study assessing the PK and PFS clearly documents that the SC administration of pembrolizumab is acceptable.38
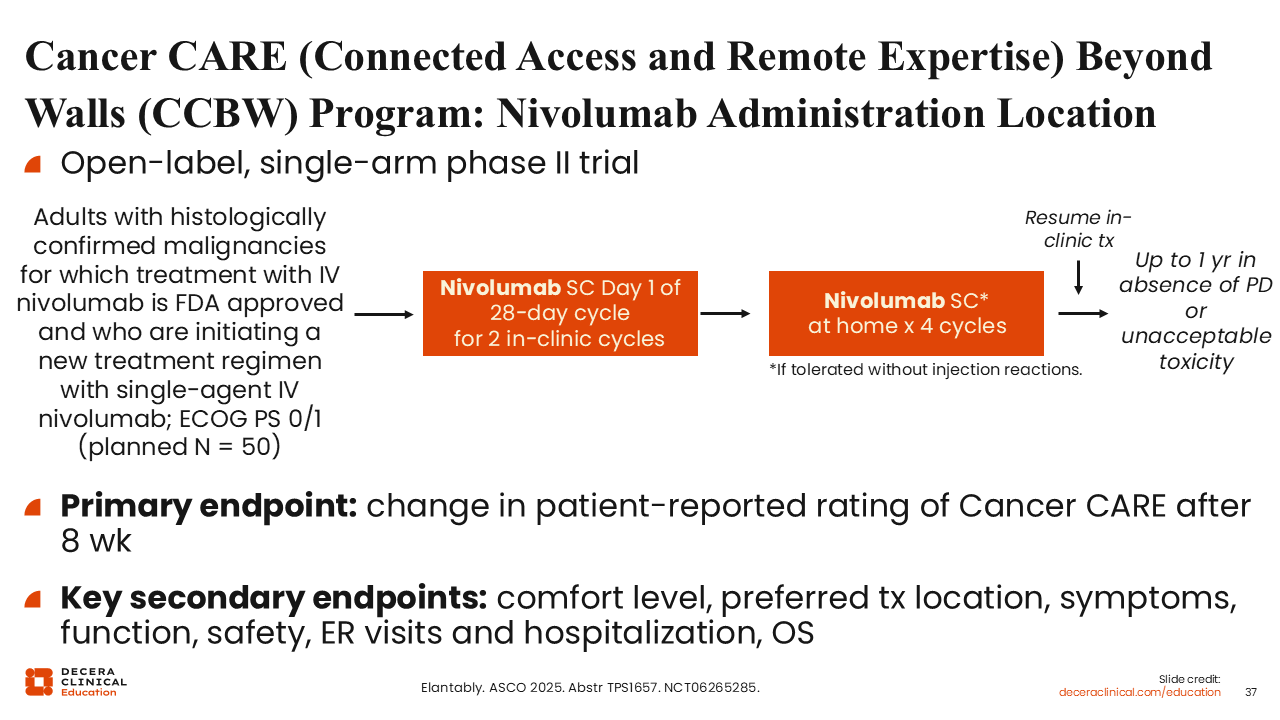
Cancer CARE (Connected Access and Remote Expertise) Beyond Walls (CCBW) Program: Nivolumab Administration Location
The Cancer CARE Beyond the Walls program is an open-label, single-arm phase II trial, where SC nivolumab was given. Participants are adults (planned N = 50) with histologically confirmed malignancies for which treatment with IV nivolumab is FDA approved and who are initiating a new treatment regimen with single-agent IV nivolumab and have an ECOG PS 0/1. Patients will receive 2 cycles of SC nivolumab in clinic and then switch to at home care for 4 cycles. At that point, some participants will resume with their treatment back in the clinic. The primary endpoint is a change in the patient-reported rating of outcomes after 8 weeks. The secondary endpoints assessed comfort level, preferred treatment location, symptoms, safety, and other parameters such as emergency department visits and hospitalization (NCT06265285).39
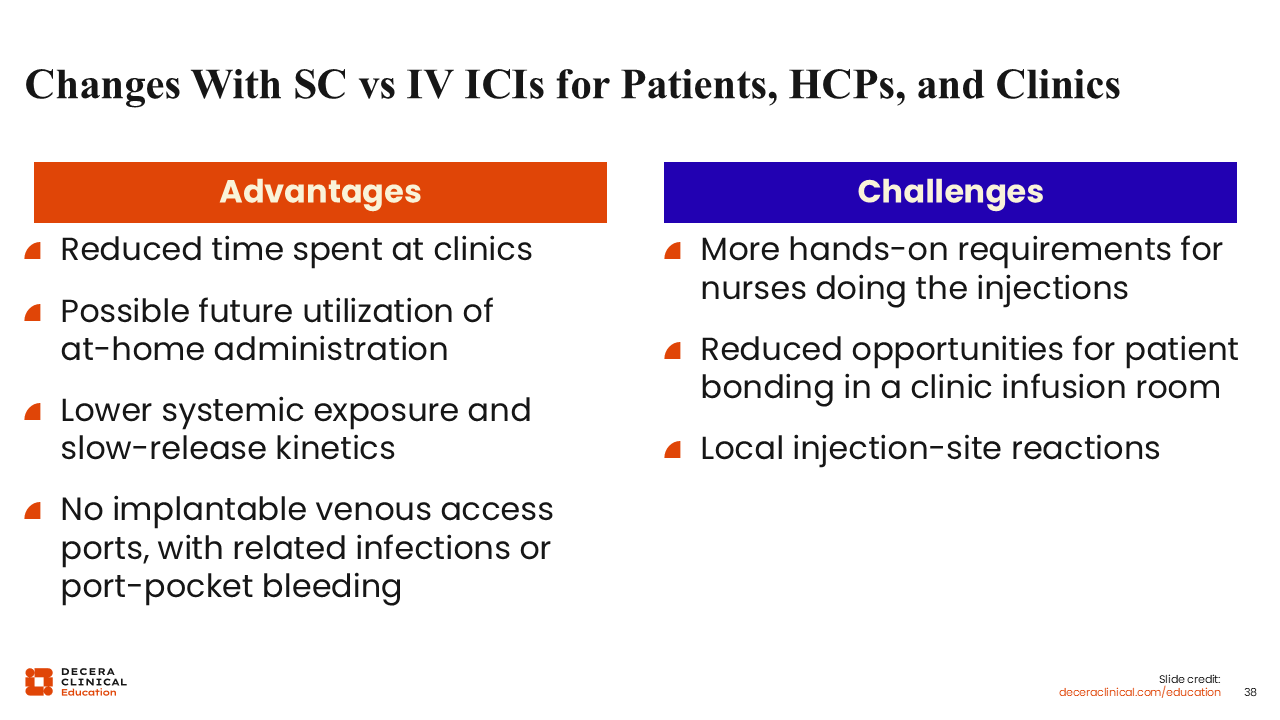
Changes With SC vs IV ICIs for Patients, HCPs, and Clinics
The advantage of giving these agents subcutaneously includes a reduction in the time spent at the clinics and particularly in maintenance phase. Patients can get SC injections at home; they do not have to go anywhere. They can have their blood drawn and come home and get the injection, which can improve quality of life. In addition, it may be that lower systemic exposure with SC administration will produce some advantages. For example, the port may be removed: If that patient starts with chemotherapy and immunotherapy and then chemotherapy is stopped, it may be possible to remove the port and continue SC injection of the immunotherapy.
By contrast, the challenges that emerge with transitioning from IV to SC includes a requirement for more individuals to assist the patient at home, especially if the patient is unable to self-administer. Then patients may need a nurse to come to their homes, which can be challenging for some circumstances. Home administration also reduces opportunities for patients to bond with one another in person, but perhaps they can connect with online patient support communities. Finally, the SC injection can produce a local reaction because the immune milieu of skin is different than when given via IV.
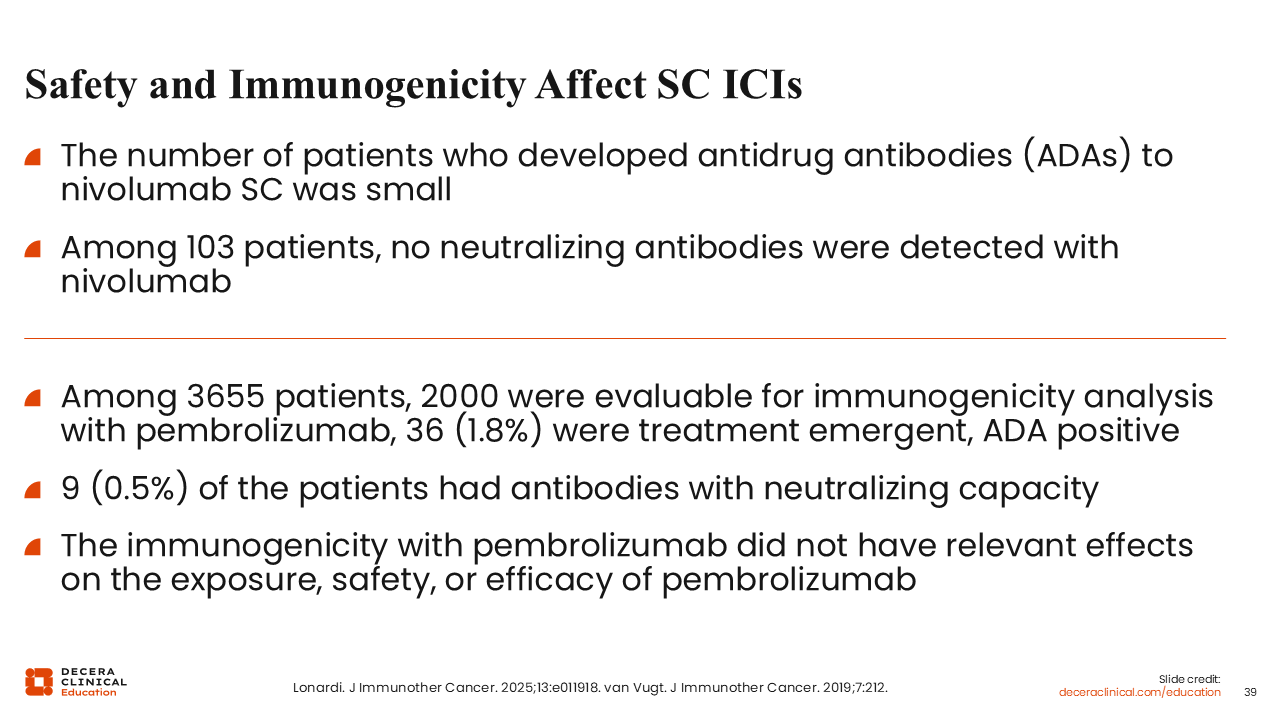
Safety and Immunogenicity Affect SC ICIs
Other safety concerns include the immune response of the host, and the host can form ADAs. There is a slightly higher chance of that happening with SC injection because the immune environment of the skin is different. No ADAs were detected, which is ideal. Otherwise, ADAs can neutralize the drug. This is the reason why it is important to look for these ADAs. In this case, the results were favorable.
Biomarkers like TAP and CPS assessment of PD-L1 expression, HER2 positivity, MSI high, and CLDN 18.2 positivity, coupled with drug treatment approvals for gastric cancer and GEJ adenocarcinoma are emerging. In addition, SC options for drug administration are also evolving, reducing the requirements for patients to repeatedly return to a clinic setting for IV infusions of immunotherapy. SC drug formulations allow additional flexibility to patients and their healthcare professionals, increasing options and potentially translating to quality-of-life measures.40,41