
CME
Expert Guidance and Clinical Resources to Improve the Care of Patients With Mantle Cell Lymphoma
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
Released: May 19, 2026
Expiration: November 18, 2026

Activity
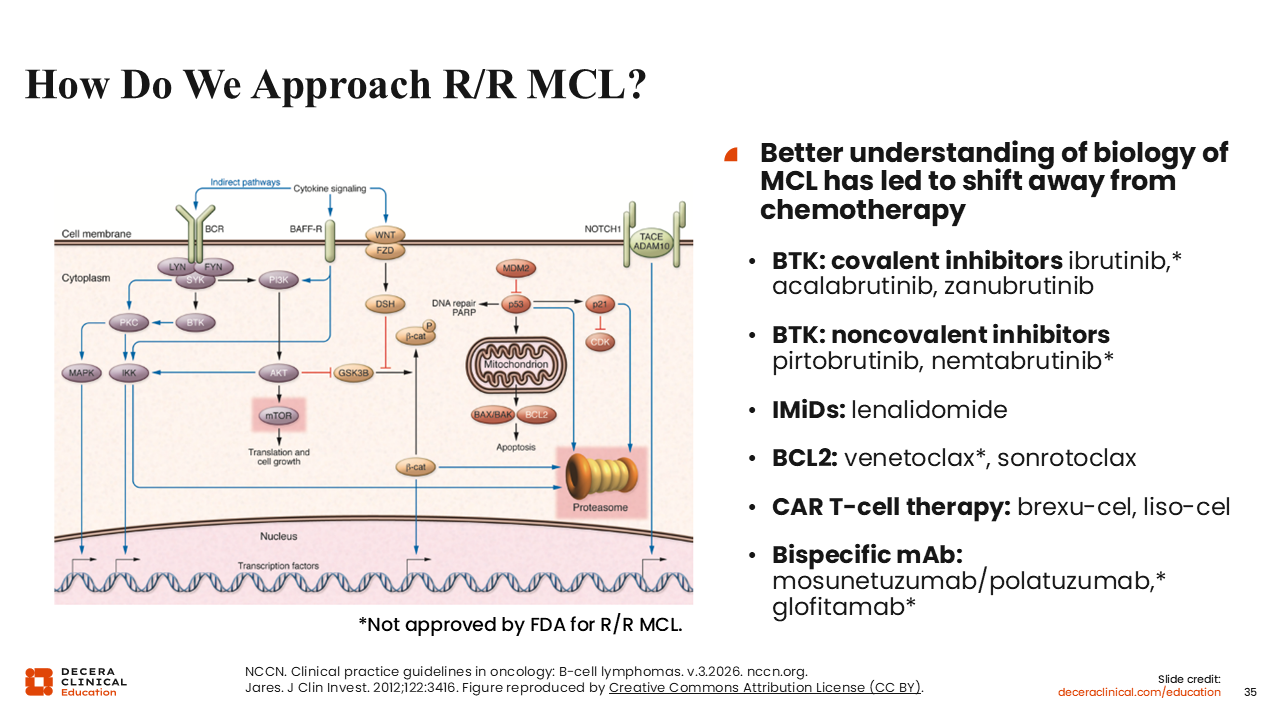
How Do We Approach R/R MCL?
Moving on to the R/R MCL setting, covalent BTK inhibitors are typically the first treatments we consider in the second-line setting for patients not previously treated with a BTK inhibitor, with acalabrutinib and zanubrutinib being the primary options. These can be followed by noncovalent BTK inhibitors, which currently include just 1 FDA-approved agent, pirtobrutinib, and 1 investigational agent, nemtabrutinib. Lenalidomide and venetoclax have smaller roles in R/R MCL, particularly in patients who relapse after BTK inhibitors.
The 2 CAR T-cell therapies, brexu-cel and liso-cel, are typically used after failure on a covalent BTK inhibitor. Among the treatment options of post covalent BTK inhibitors, they have the longest DoRs. We also have the bispecific antibodies glofitamab and mosunetuzumab plus polatuzumab vedotin; however, they are not currently approved by the FDA for MCL, so their use would need to be discussed with insurance.
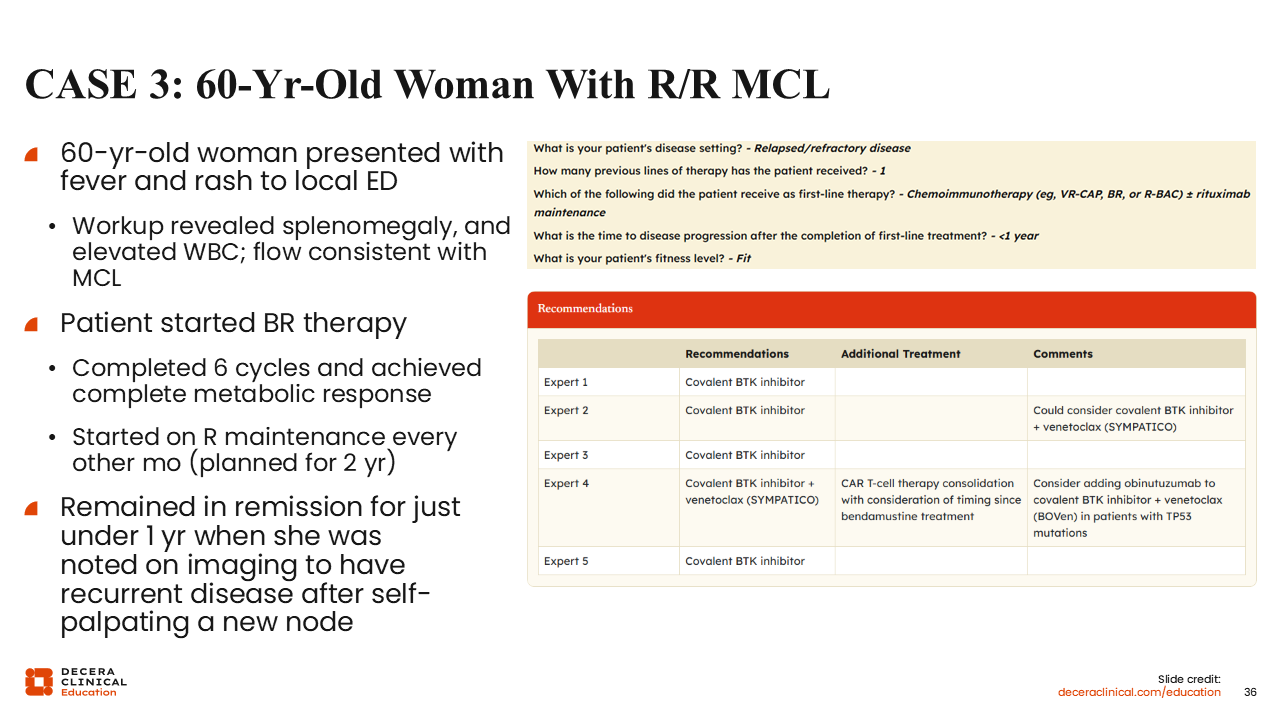
Case 3: 60-Year-Old Woman With R/R MCL
Let’s discuss how we might approach specific patient cases in R/R MCL.
A 60-year-old woman presented with fever and rash to a local emergency department. During the workup, she was found to have splenomegaly and an elevated white blood cell count, specifically an elevated lymphocyte count. Flow cytometry results of a peripheral blood sample were consistent with MCL. The patient was started on CIT with BR. She completed 6 cycles of therapy and achieved CR at the end of treatment, after which she was started on 2 years of maintenance rituximab. She remained in remission for just under 1 year, when she was noted on imaging to have recurrent disease after self-palpating a new node in the left groin.
This is a case of a patient with early relapse after what would be considered a sufficient chemotherapy backbone in the frontline. I would be concerned that this patient may have a TP53 mutation or another high-risk genetic feature. Therefore, I would treat this patient with a covalent BTK inhibitor.
When we input this case into the treatment decision tool, we can see that there is a consensus among 4 experts that optimal second-line treatment for this patient would be a covalent BTK inhibitor.
However, if a workup reveals that she has a high-risk feature, I would potentially consider an early transition to a third treatment, possibly CAR T-cell therapy. Unfortunately, BTK inhibitors have reduced duration of efficacy in most patients who have early progression after initial treatment with CIT, especially those with TP53-mutated, blastic, pleomorphic, or elevated Ki-67 disease.
Of note, 1 expert on the panel recommended a covalent BTK inhibitor with venetoclax based on the SYMPATICO trial that showed longer PFS with this combination compared with ibrutinib monotherapy.29 This is a viable option for this patient who potentially has high-risk disease and is likely at risk for a shorter DoR on a single-agent covalent BTK inhibitor.
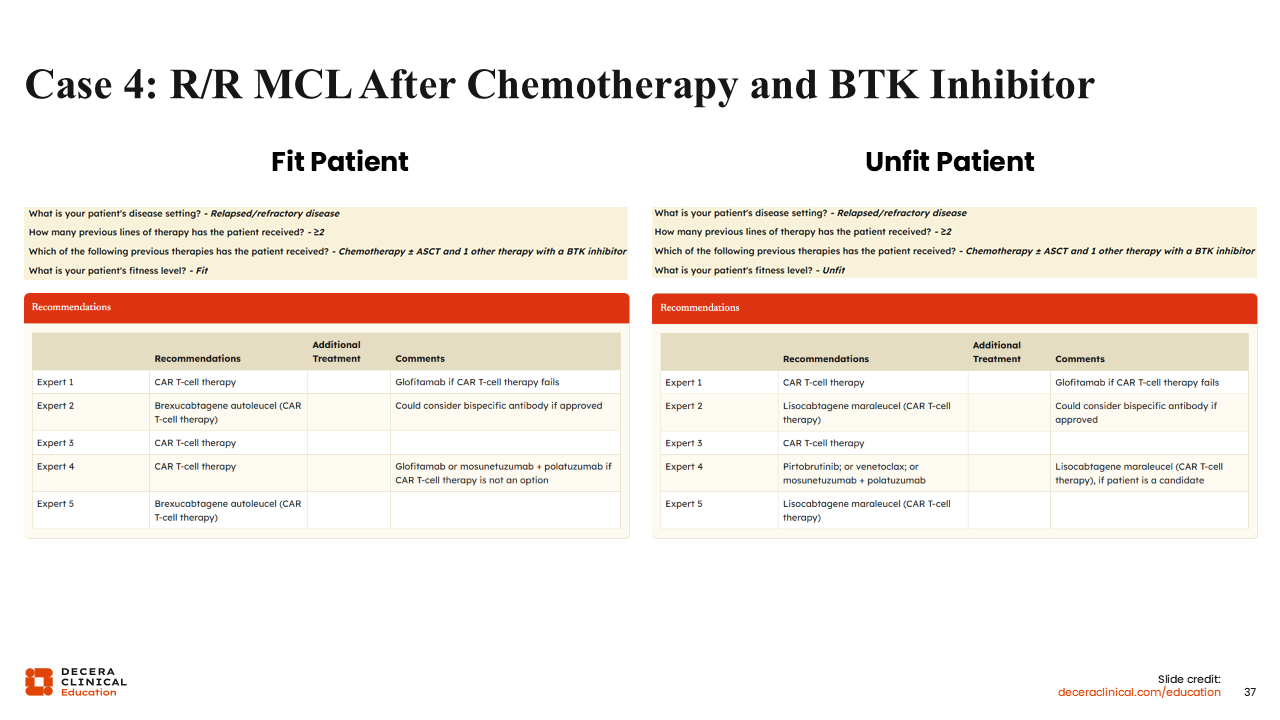
Case 4: R/R MCL After Chemotherapy and BTK Inhibitor
Now, let’s consider a patient who has undergone 2 lines of therapy, including CIT (eg, BR with rituximab maintenance) and BTK inhibitor therapy (eg, acalabrutinib). For a younger, fit patient in this situation, I would treat next with brexu-cel CAR T-cell therapy. For unfit patients, I would recommend liso-cel. As an alternative to CAR T-cell therapy, I would consider a bispecific antibody, like glofitamab or mosunetuzumab plus polatuzumab vedotin, if approved.
According to the treatment decision tool, there was consensus among the 5 experts for consideration of brexu-cel or any CAR T-cell therapy for a fit patient in this setting
For an unfit patient, 4 of 5 experts recommended CAR T-cell therapy, while 1 recommended pirtobrutinib. The recommendations for pirtobrutinib come from concern over the toxicity of CAR T-cell therapy, particularly in frail patients. Although the safety profile of liso-cel suggests that it would be safe in this patient population, limited enrollment of these patients means we have little data to rely on. Pirtobrutinib has limited efficacy in patients who are refractory to covalent BTK inhibitors, but it is considered safe for unfit patients. Either after CAR T-cell therapy or as an alternative, 3 of 5 experts also suggested a bispecific antibody regimen as an option.
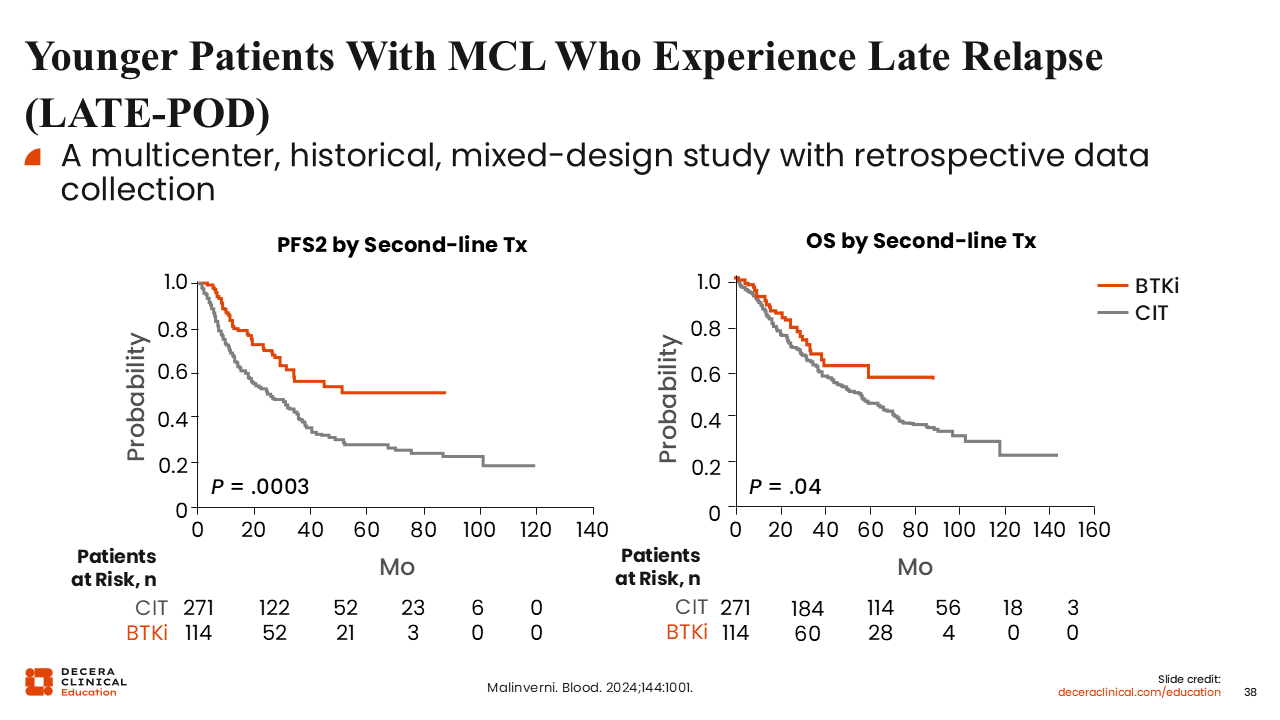
Younger Patients With MCL Who Experience Late Relapse
Retrospective data from the LATE-POD study have shown that in the second-line setting, BTK inhibitors have significantly improved outcomes compared with CIT.71 Specifically, PFS after second-line treatment (P = .0003) and OS (P = .04) were longer for patients treated with BTK inhibitors in the second line vs CIT.
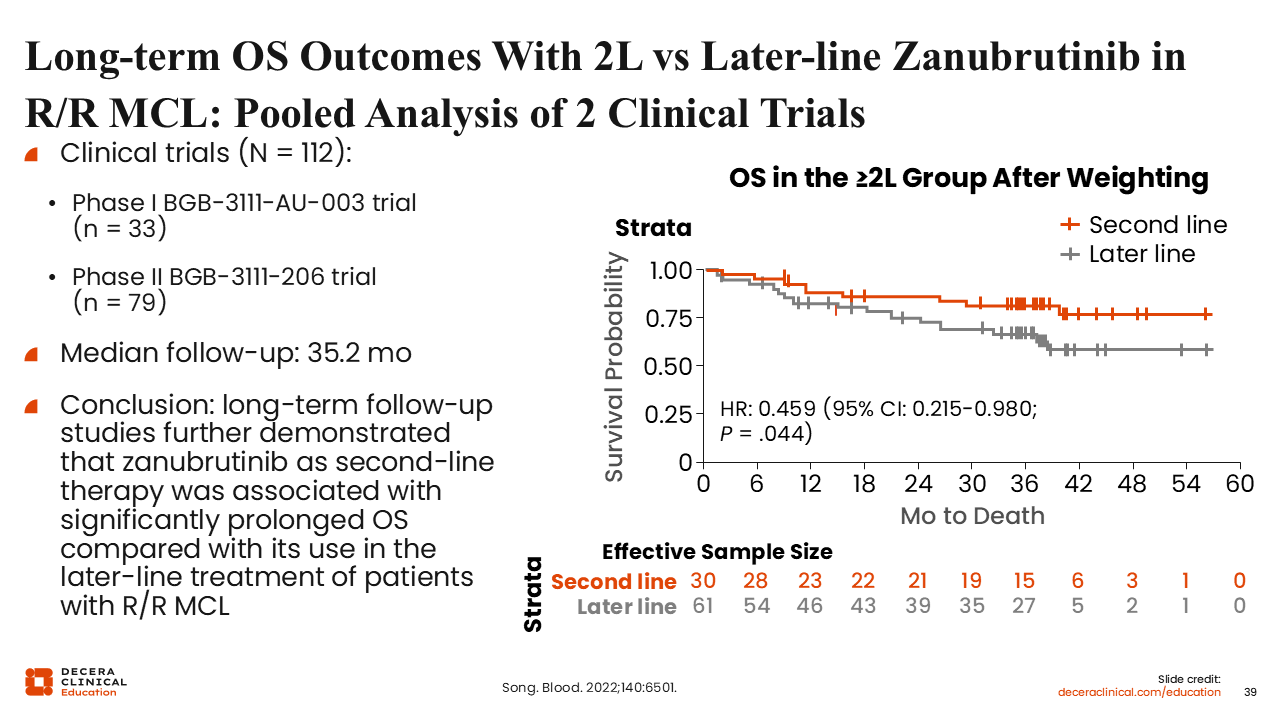
Long-term OS Outcomes With 2L vs Later-line Zanubrutinib in R/R MCL: Pooled Analysis of 2 Clinical Trials
A pooled analysis of 2 clinical trials found that OS outcomes of patients treated with zanubrutinib in the second line were longer than when given in later lines of therapy.72 Generally, patients who receive BTK inhibitors in the second line tend to have a better PFS and OS than those who receive them in the third line and beyond. This supports the strategy of using these treatments earlier in this patient population to achieve the maximum benefit.
Factors Considered by Experts When Considering Treatment With a Covalent BTK Inhibitor in R/R MCL
For patients without any comorbidities, BTK inhibitors should be the preferred regimen in the second line for R/R MCL for patients who have not previously received a BTK inhibitor. However, some comorbidities may cause hesitation before using these agents. For patients with conditions such as cardiac issues, bleeding issues, and renal insufficiency, BTK inhibitor treatment may be feasible but will require close and careful monitoring of toxicity concerns. Other toxicities, such as upper respiratory infections, are a concern with both BTK inhibitors and CIT, so they may not prevent BTK inhibitor treatment.
Overall, these BTK inhibitors are more expensive than CIT but appear to offer greater efficacy and comfort and convenience of administration. In addition, drug availability varies by country, so your choice of BTK inhibitor will depend on what is approved and available in your country. Finally, patients with high-risk features, like 17p deletion or TP53 mutations, have poorer responses and DoRs to BTK inhibitors than patients without these features. Therefore, when treating these high-risk patients, it is important to have additional treatments in mind for when they start progressing on these medications.
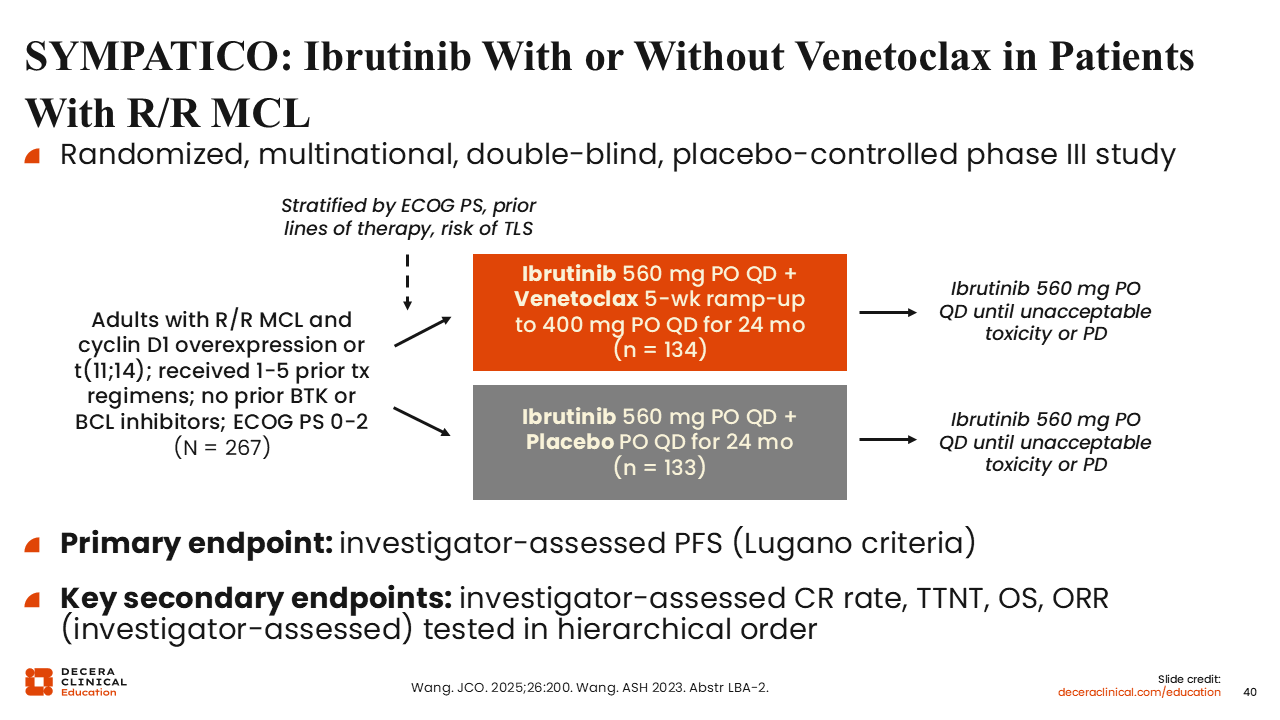
SYMPATICO: Ibrutinib With or Without Venetoclax in Patients With R/R MCL
The phase III SYMPATICO study was designed to determine whether the doublet regimen of ibrutinib plus venetoclax would be better than single-agent ibrutinib for patients with R/R MCL.29 Venetoclax was initiated with a 5-week ramp-up dosing and continued at the maximum dose of 400 mg daily for 24 months. After 24 months of treatment, patients in both arms continued ibrutinib indefinitely until disease progression or unacceptable toxicity. The primary endpoint was PFS.
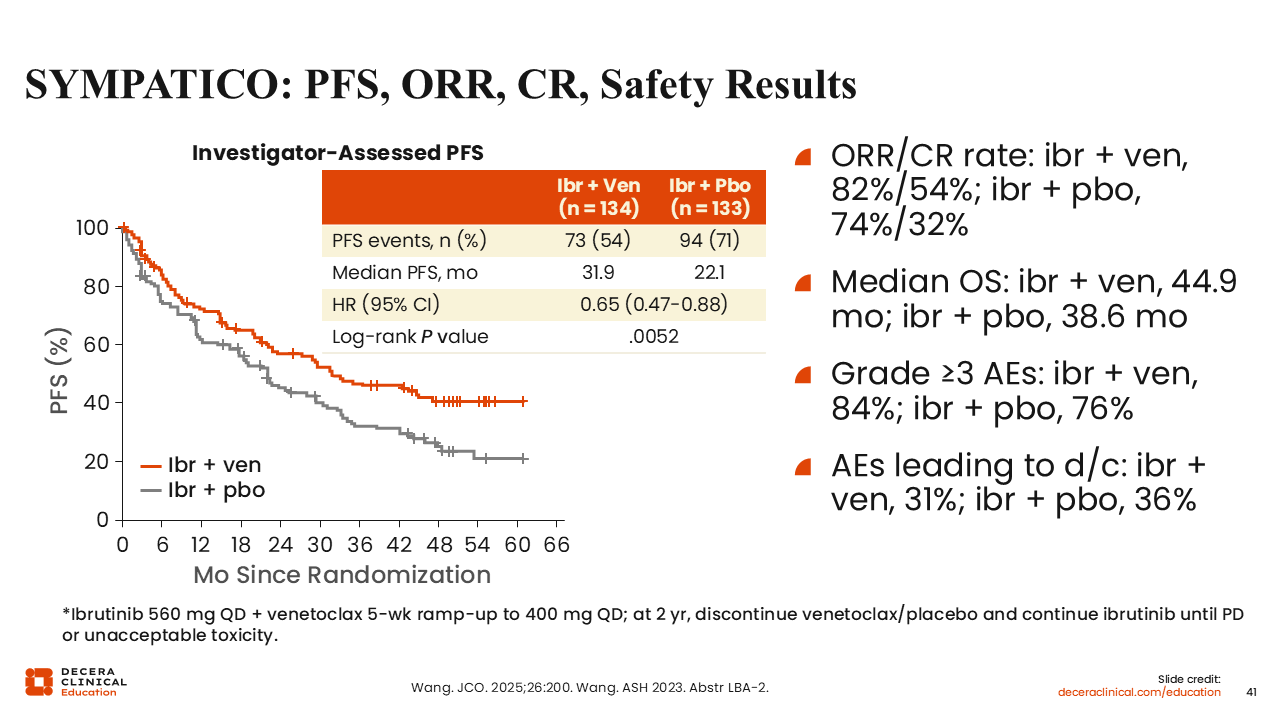
SYMPATICO: PFS, ORR, CR, Safety Results
Ibrutinib with venetoclax was shown to have superior PFS compared with ibrutinib alone, with a median PFS of 31.9 vs 22.1 months. The ORR was 82% vs 74%, and the CR rate was 54% vs 32%.29 Efficacy of the doublet combination was also promising for patients with TP53 mutations, with ORR and CR rates of 84% and 57%, respectively.73 However, some AEs occur with higher frequency with the combination of ibrutinib plus venetoclax, such as gastrointestinal toxicity and cytopenias, so it is important to be selective about the patients we treat with this regimen.29
There is also some concern about the censoring methods used in this study and how they affect long-term patient responses, potentially leading to an artificial benefit in PFS for ibrutinib plus venetoclax compared with ibrutinib plus placebo.
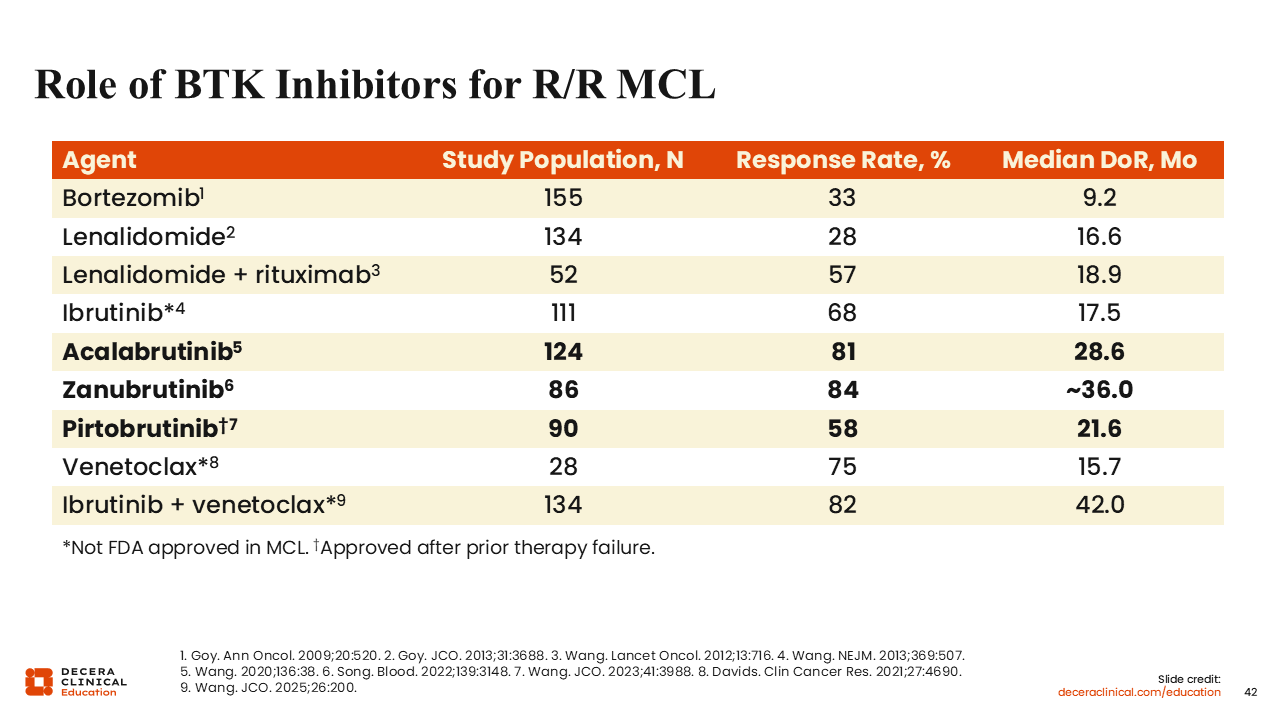
Role of BTK Inhibitors for R/R MCL
Here is a summary of some treatments we have for R/R MCL that shows higher ORRs for the BTK inhibitors. Acalabrutinib and zanubrutinib have similar efficacy (ORR: 81% and 84%, respectively), both higher than that of ibrutinib (ORR: 68%).55,72,74 Pirtobrutinib was evaluated in a post–covalent BTK inhibitor patient population, so its lower ORR (58%) is not a fair comparison to acalabrutinib and zanubrutinib, which were tested in BTK-naive patient populations.63 Nonetheless, durable responses were observed in some responding patients treated with pirtobrutinib.
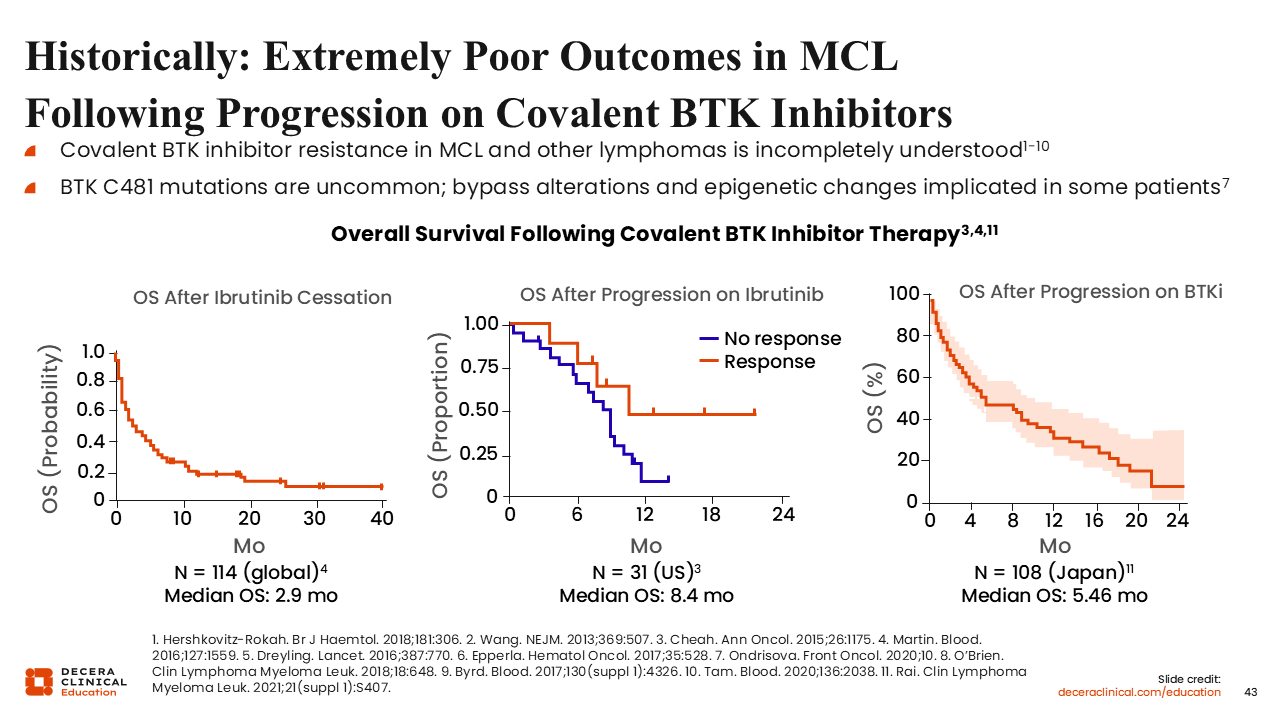
Historically: Extremely Poor Outcomes in MCL Following Progression on Covalent BTK Inhibitors
Although BTK inhibitors have been beneficial for MCL, patients who progress on covalent BTK inhibitors have very poor OS, and there are few effective drugs after progression on these agents.55,75-83 Unfortunately, we do not know why these drugs stop working. Cysteine 481 mutations in BTK are a common cause of BTK inhibitor resistance among patients with CLL but are very uncommon in MCL.76 Bypass alterations and epigenetic changes have been suggested mechanisms, but there are no definitive data pinpointing any particular mechanism of resistance in this patient population. This uncertainty makes it difficult to develop alternative strategies to overcome this resistance.
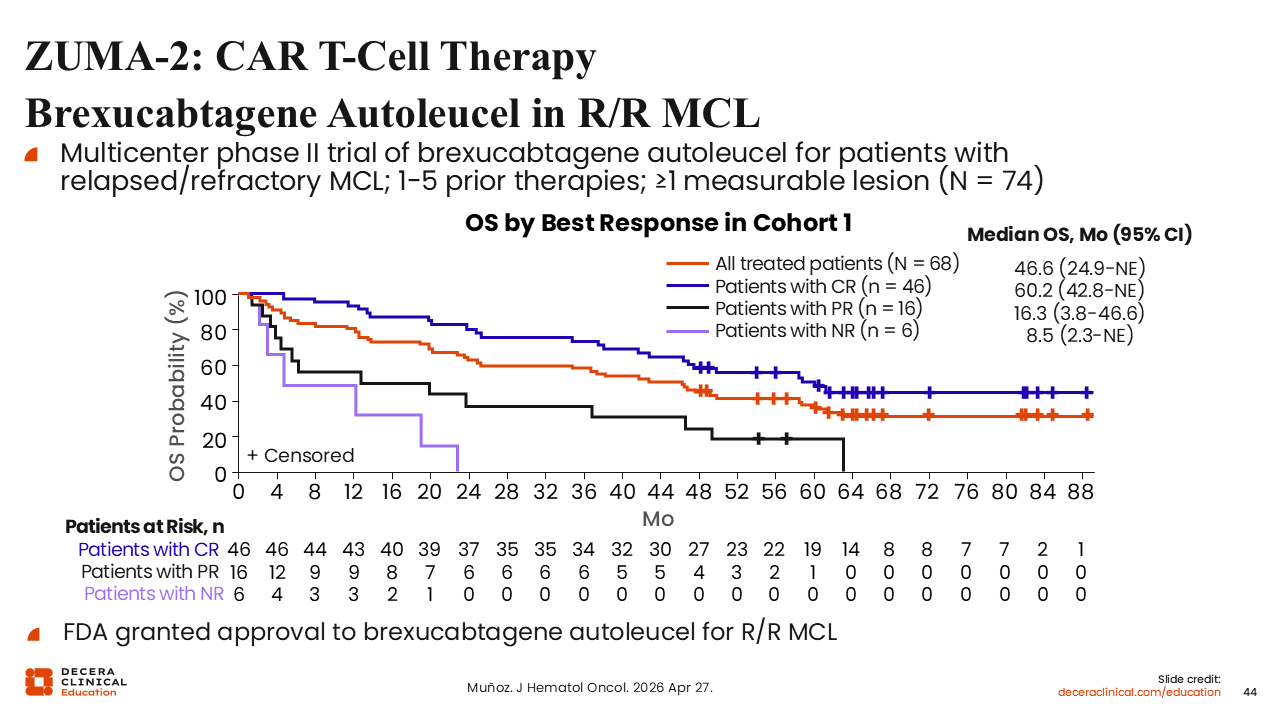
ZUMA-2: CAR T-Cell Therapy Brexucabtagene Autoleucel in R/R MCL
One effective non-BTK inhibitor therapy in this patient population has been CAR T-cell therapy. The phase II ZUMA-2 trial evaluated brexu-cel in patients previously treated with 1-5 therapies including a covalent BTK inhibitor, ibrutinib or acalabrutinib.84,85 The study demonstrated a high ORR and DoR in those who had responses, especially compared with typical outcomes in this patient population. Real-world data show similar response rates, with an ORR of 90% and a CR rate of 82%.86 Unfortunately, unlike in aggressive large T-cell lymphomas, CAR T-cell therapy does not appear to be curative in MCL.87 The 5-year long-term follow-up of ZUMA-2 shows that many patients relapse after CAR T-cell therapy, with 83% of patients achieving a CR or partial response and only 25% with ongoing responses (median follow-up: 67.8 months).85
In the primary analysis of ZUMA-2 Cohort 3, brexu-cel demonstrated high efficacy in patients with R/R MCL who were BTK inhibitor naive.88 Among 86 treated patients, the ORR was 91%, including a 73% CR rate and a 17% partial response rate. At a median follow-up of 15.5 months, responses were durable, with estimated 12-month PFS, DoR, and OS rates of 75%, 80%, and 90%, respectively. These results highlight strong activity of brexu-cel earlier in the treatment pathway and supported its recent full approval for patients with R/R MCL.
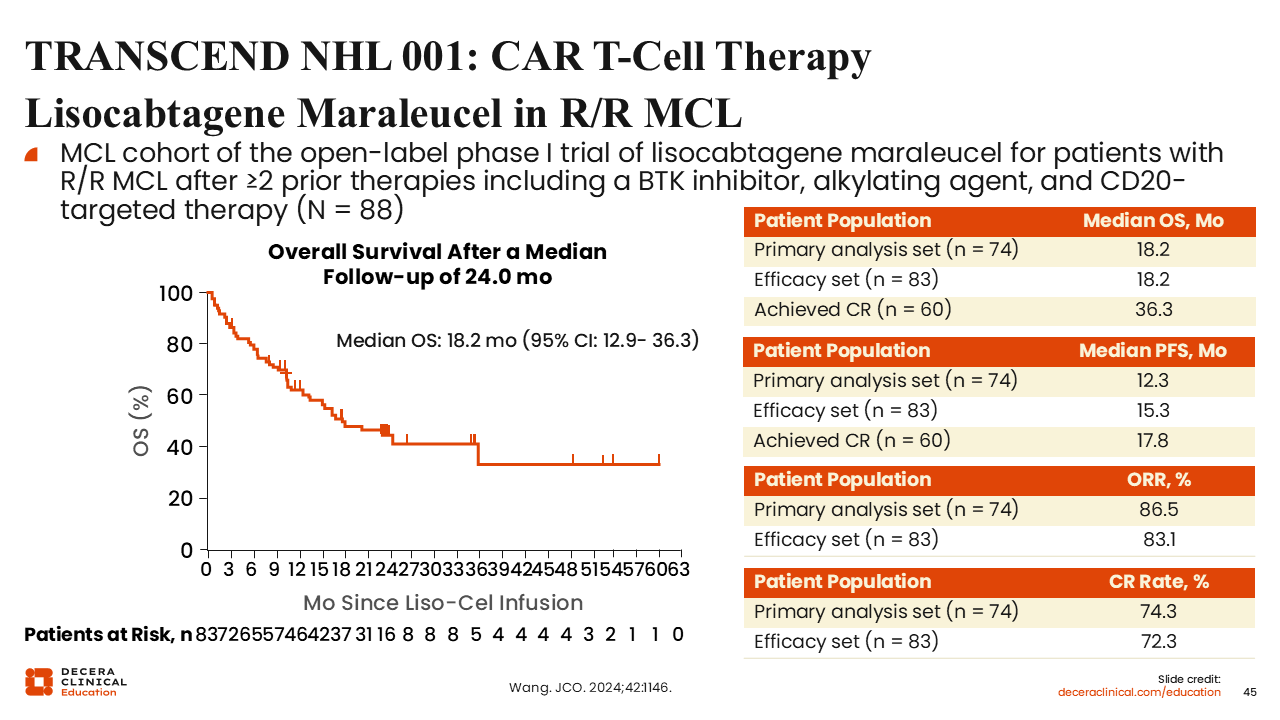
TRANSCEND NHL 001: CAR T-Cell Therapy
Lisocabtagene Maraleucel in R/R MCL
The other CAR T-cell therapy approved for R/R MCL is liso-cel, which was tested in the phase I TRANSCEND NHL 001 study.89 The MCL cohort of the trial tested liso-cel in patients with R/R MCL after at least 2 prior lines of therapy including a BTK inhibitor, a CD20-targeted therapy, and an alkylating agent. The ORR was similar to that reported for brexu-cel—86.5% in the primary analysis set—with a higher CR rate of 74.3%. However, median OS after a median follow-up of 24 months was lower at 18.2 months (36.3 months for patients who achieved CR).
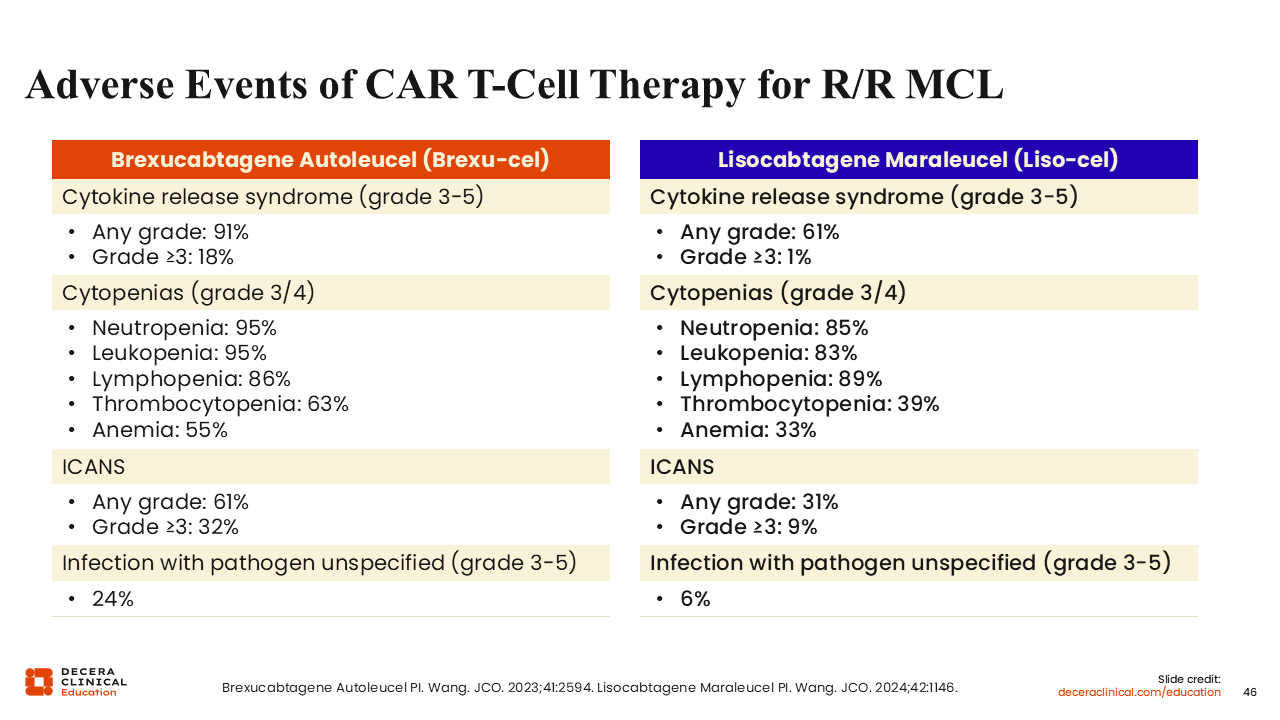
Adverse Events of CAR T-Cell Therapy for R/R MCL
Toxicities to be aware of with CAR T-cell therapies include cytokine-release syndrome (CRS), neurologic AEs, immune effector cell–associated neurotoxicity syndrome (ICANS), cytopenias, and infections. These 2 CAR T-cell products were not compared head to head, but we can see that liso-cel had lower rates of grade 3-5 CRS (1% for liso-cel; 18% for brexu-cel) and neurologic toxicities (eg, encephalopathy: 9% for liso-cel; 24% for brexu-cel).73,89-91 However, the incidences of cytopenias are high for both agents (eg, neutropenia: 85% for liso-cel; 95% for brexu-cel).
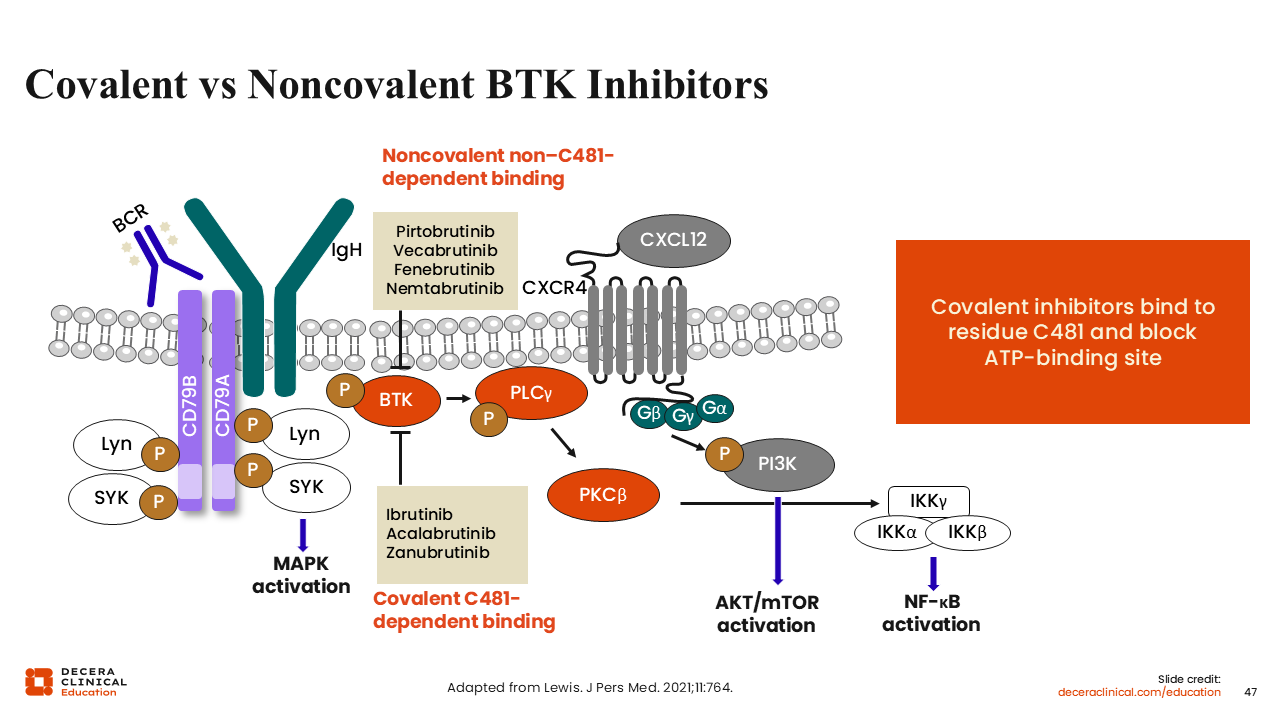
Covalent vs Noncovalent BTK Inhibitors
Whereas covalent BTK inhibitors permanently bind to the BTK receptor, noncovalent BTK inhibitors exhibit allosteric inhibition, allowing them to move in and out of the binding pocket.92 This means they are less affected by binding site mutations and potential resistance, although these mechanisms of resistance are rare in MCL.
Pirtobrutinib
Pirtobrutinib is a noncovalent BTK inhibitor approved in 2023 for adult patients with R/R MCL after 2 or more lines of systemic therapy, including a BTK inhibitor.93 The ORR for pirtobrutinib in this setting is 57.8%, and the median DoR in covalent BTK inhibitor–pretreated patients is 21.6 months.63
An important characteristic of pirtobrutinib is that it is fairly well tolerated, with lower incidences of AEs compared with covalent BTK inhibitors. It also has the convenience of once-daily dosing with 200 mg.
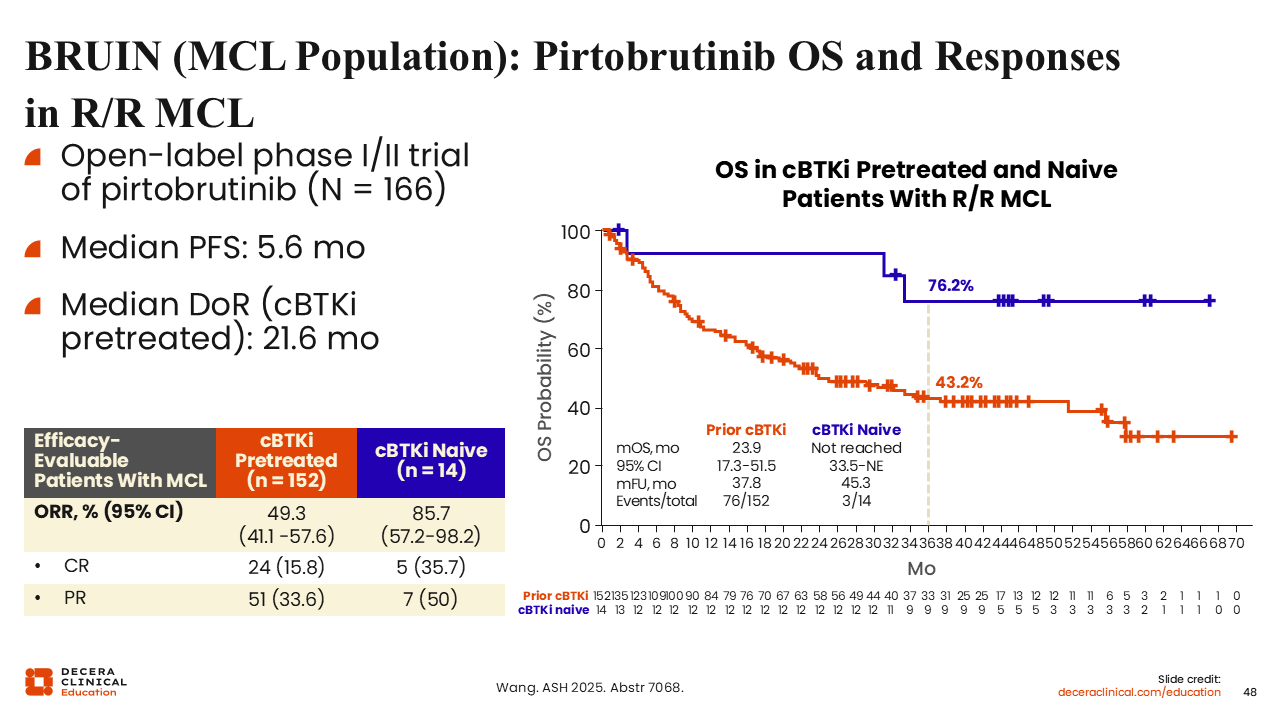
BRUIN (MCL Population): Pirtobrutinib OS and Responses in R/R MCL
The phase I/II BRUIN trial investigated pirtobrutinib for patients with R/R MCL.63 Most of these patients had previous exposure to a covalent BTK inhibitor (152 of 166 patients).
Although the ORR (49.3%) is fairly impressive in this post–covalent BTK inhibitor setting, the DoR of 21.6 months and PFS of 5.6 months show that the response is not very durable. However, the median OS at the median follow-up of 37.8 months was 23.9 months. These data together suggest that pirtobrutinib may be best suited as a bridge treatment instead of a definitive treatment in R/R MCL.
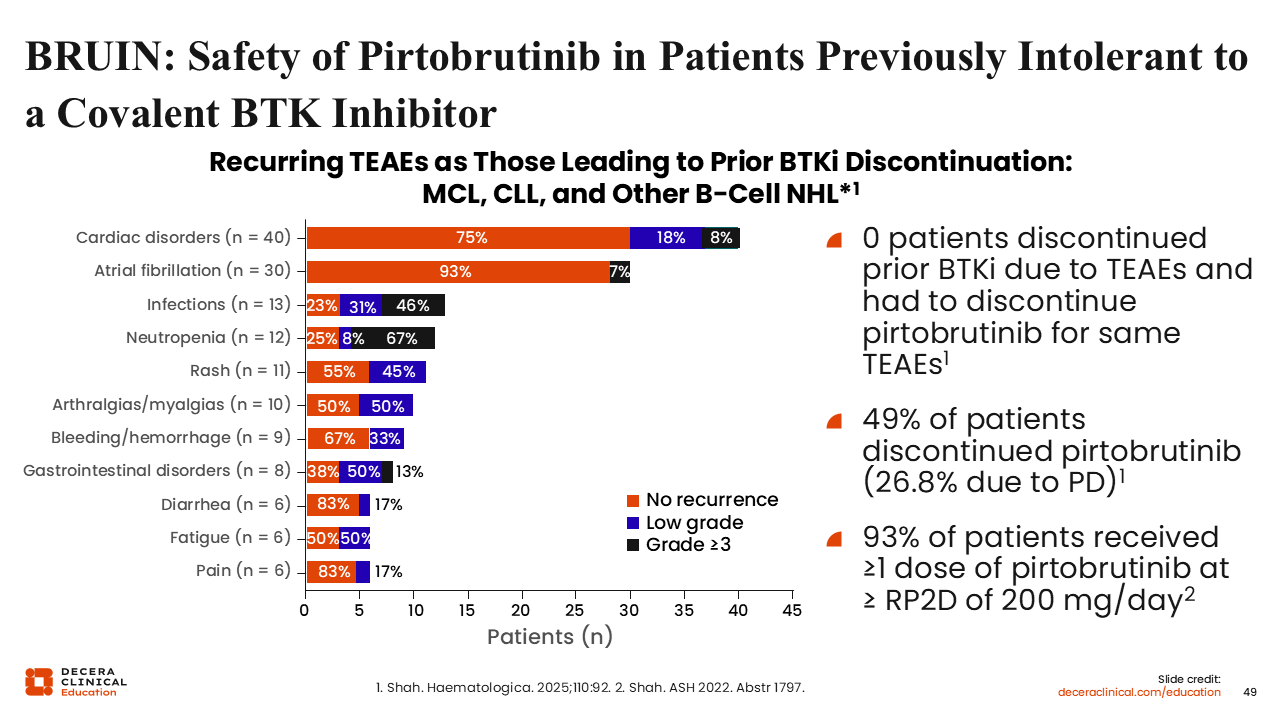
BRUIN: Safety of Pirtobrutinib in Patients Previously Intolerant to a Covalent BTK Inhibitor
Pirtobrutinib is associated with AEs expected for the BTK inhibitor class, such as cardiac disorders, atrial fibrillation, infection, neutropenia, rash, diarrhea, and fatigue.63,94 However, the incidence of these AEs appears lower. In addition, among patients who discontinued prior BTK inhibitors because of AEs, few had recurrence of those same AEs.94
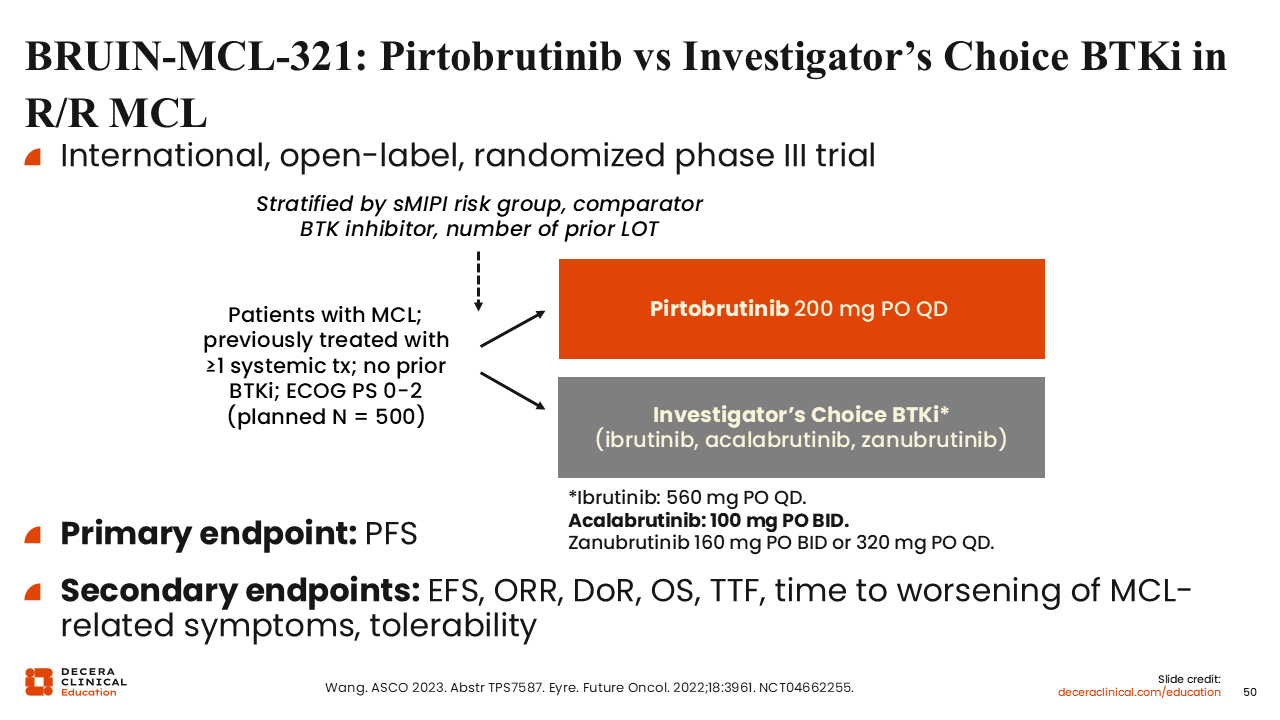
BRUIN-MCL-321: Pirtobrutinib vs Investigator’s Choice BTKi in R/R MCL
Pirtobrutinib is being further evaluated in the R/R MCL setting in a pivotal phase III study, BRUIN-MCL-321, against the investigator's choice.95,96 This will offer us data on the efficacy of pirtobrutinib in an earlier line of therapy in BTK-naive patients.
Sonrotoclax
Sonrotoclax is a novel BCL2 inhibitor that was approved by the FDA in May 2026 for patients with R/R MCL after at least 2 lines of systemic therapy, including a BTK inhibitor.97 From a pharmacologic perspective, sonrotoclax is a more selective and potent oral inhibitor of BCL2 than venetoclax, with a shorter half-life that may reduce drug accumulation and consequently lower the risk of tumor lysis syndrome (TLS).98
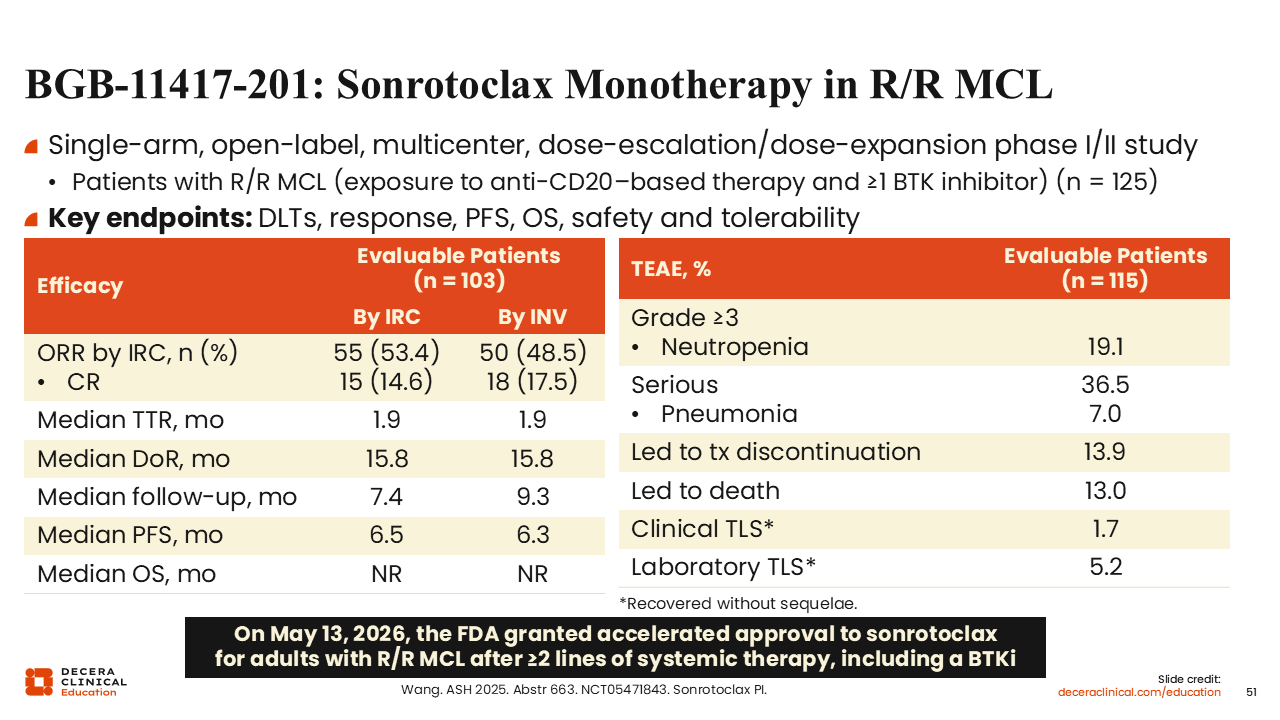
BGB-11417-201: Sonrotoclax Monotherapy in R/R in MCL
The approval of sonrotoclax is based on the BGB-11417-201 single-arm phase I/II trial for adult patients with R/R mantle cell lymphoma who had previously received anti-CD20–based therapy and a BTK inhibitor.99 Sonrotoclax was administered with a 4-week ramp-up phase to a target dose of 320 mg once daily until disease progression or intolerance. The ORR was 53.4% and the CR rate was 14.6%, making it very similar to the activity seen with pirtobrutinib. The median DoR was 15.8 months.
The most common grade ≥3 treatment-emergent AE was neutropenia (19.1%). Approximately 1 of 3 patients had a serious treatment-emergent AE, with pneumonia (7.0%) being the most common. Treatment-emergent AEs led to treatment discontinuation in 16 patients (13.9%) and death in 15 patients (13.0%). Clinical TLS occurred in 2 patients (1.7%) and laboratory TLS in 6 (5.2%). All recovered without sequelae.
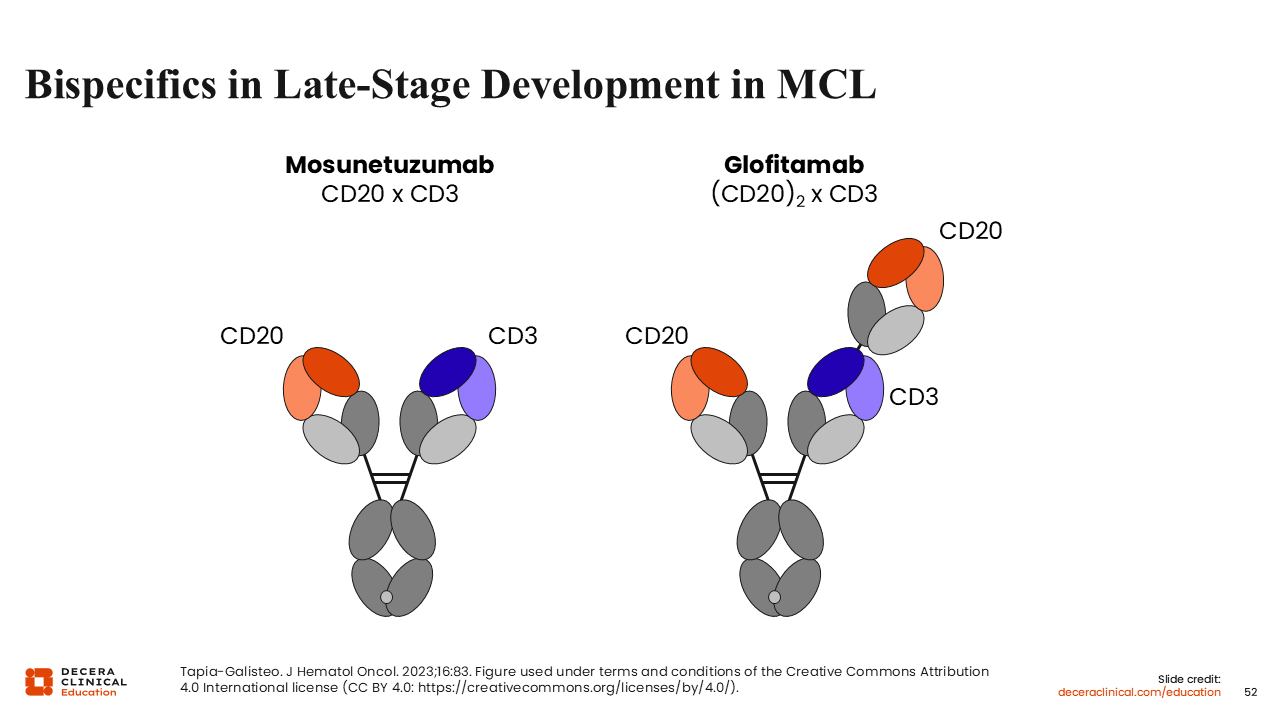
Bispecifics in Late-Stage Development in MCL
The last class of agents we will discuss in the R/R MCL setting is bispecific antibodies. These antibodies bind to CD20 on B-cells and CD3 on T-cells and, in effect, pull T-cells to malignant tumor cells. There are currently 2 bispecific antibody regimens with evidence of efficacy in R/R MCL: glofitamab as a single agent and mosunetuzumab given in combination with polatuzumab vedotin.
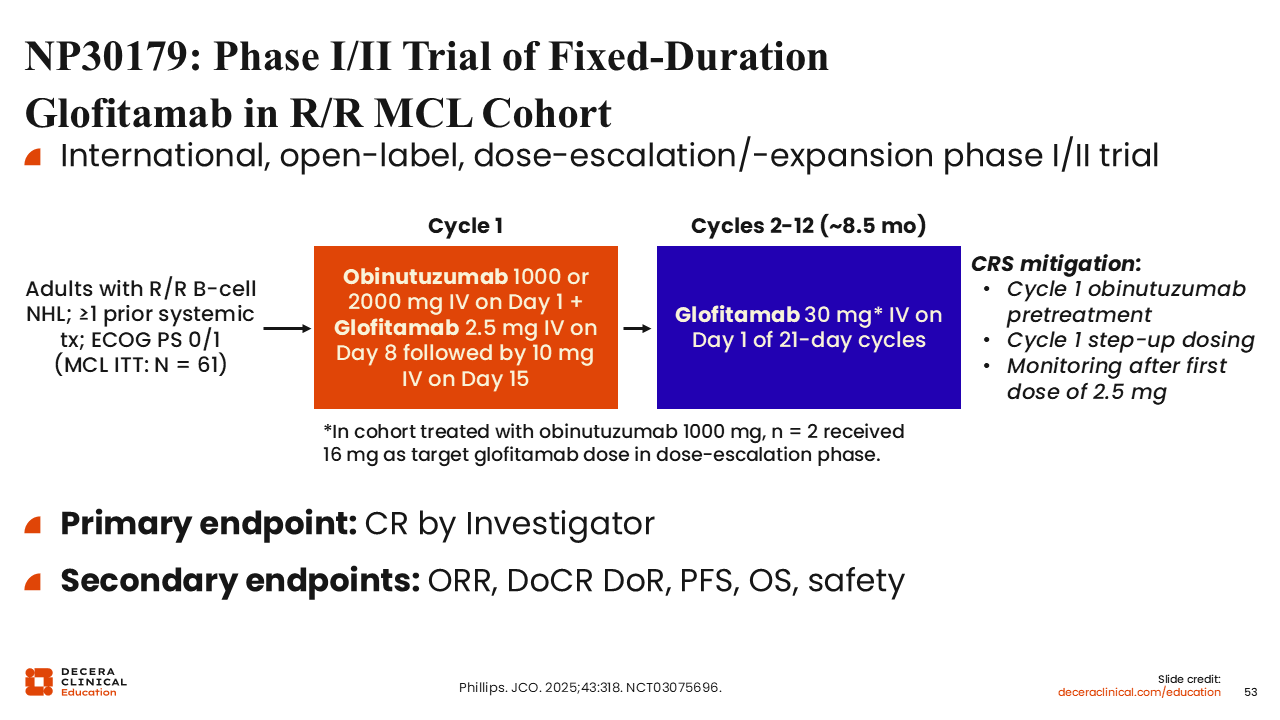
NP30179: Phase I/II Trial of Fixed-Duration Glofitamab in R/R MCL Cohort
The phase I/II dose-escalation/dose-expansion study NP30179 enrolled 61 patients with R/R MCL, approximately one half of whom were previously exposed to BTK inhibitors (51.7%).100 Patients were treated with glofitamab for 12 cycles with step-up dosing and obinutuzumab pretreatment in cycle 1 to mitigate CRS. The primary endpoint was CR rate by investigator.
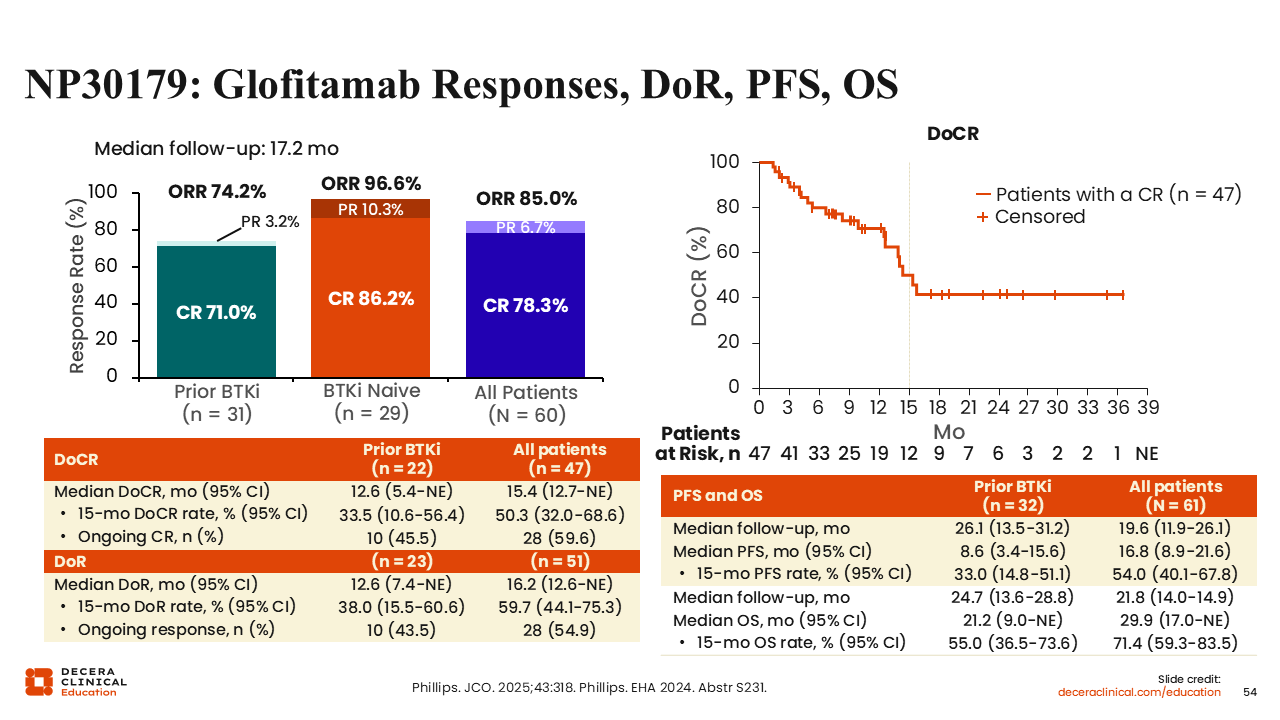
NP30179: Glofitamab Responses, DoR, PFS, OS
The ORR and CR rate were high for both BTK inhibitor–exposed (ORR: 74.2%; CR: 71.0%) and BTK inhibitor–naive patients (ORR: 96.6%; CR: 86.2%).100 The DoR curve also appears stable, especially in those with CR; however, the current follow-up is short compared with data for CAR T-cell therapy. The median PFS of 16.8 months is longer than that of pirtobrutinib (5.6 months) but less than that of brexu-cel (25.3 months).63,84,100
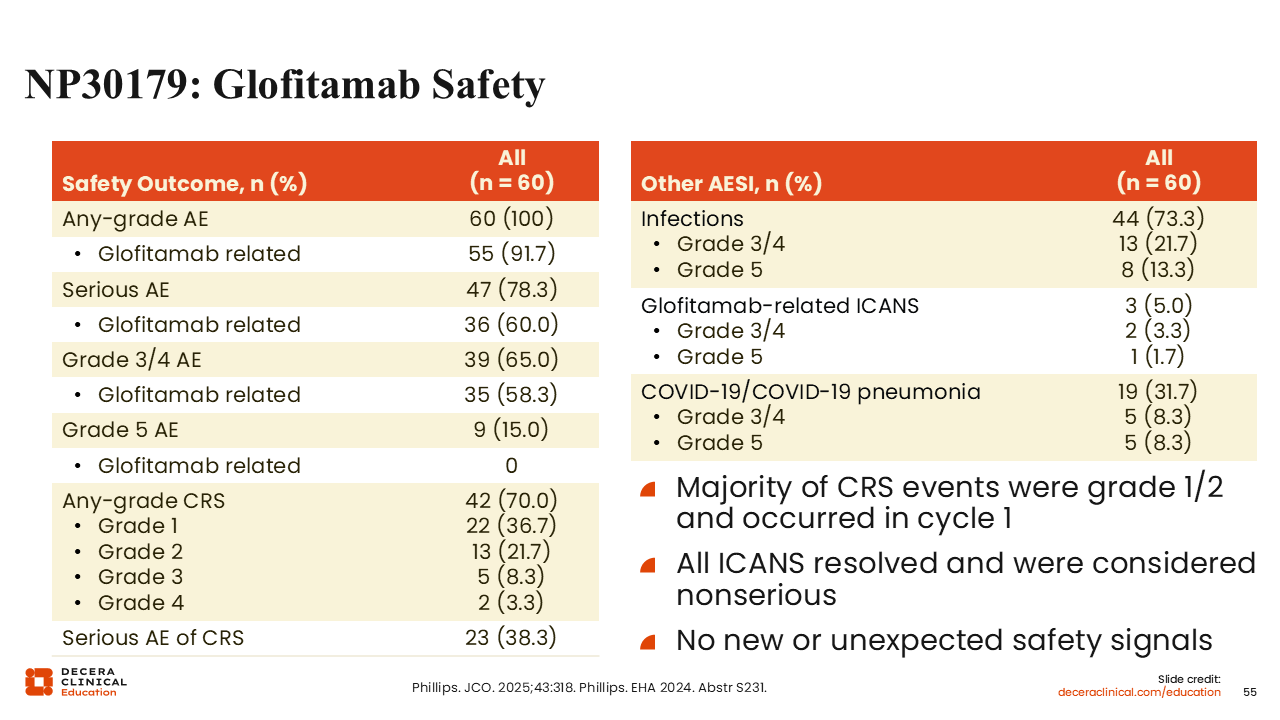
NP30179: Glofitamab Safety
The major AE of glofitamab is CRS (any grade incidence: 70%; grade 3/4: 11.6%).100 However, compared with CAR T-cell therapy, rates of neurologic complications like ICANS (glofitamab: 11.7%; brexu-cel: 61%; liso-cel: 31%) were low.86,89,100 Incidence of other AEs was also low, but infection was a concern, especially during the COVID-19 pandemic, and there were some cases of COVID-19 fatalities in patients previously treated with BTK inhibitors (n = 7).
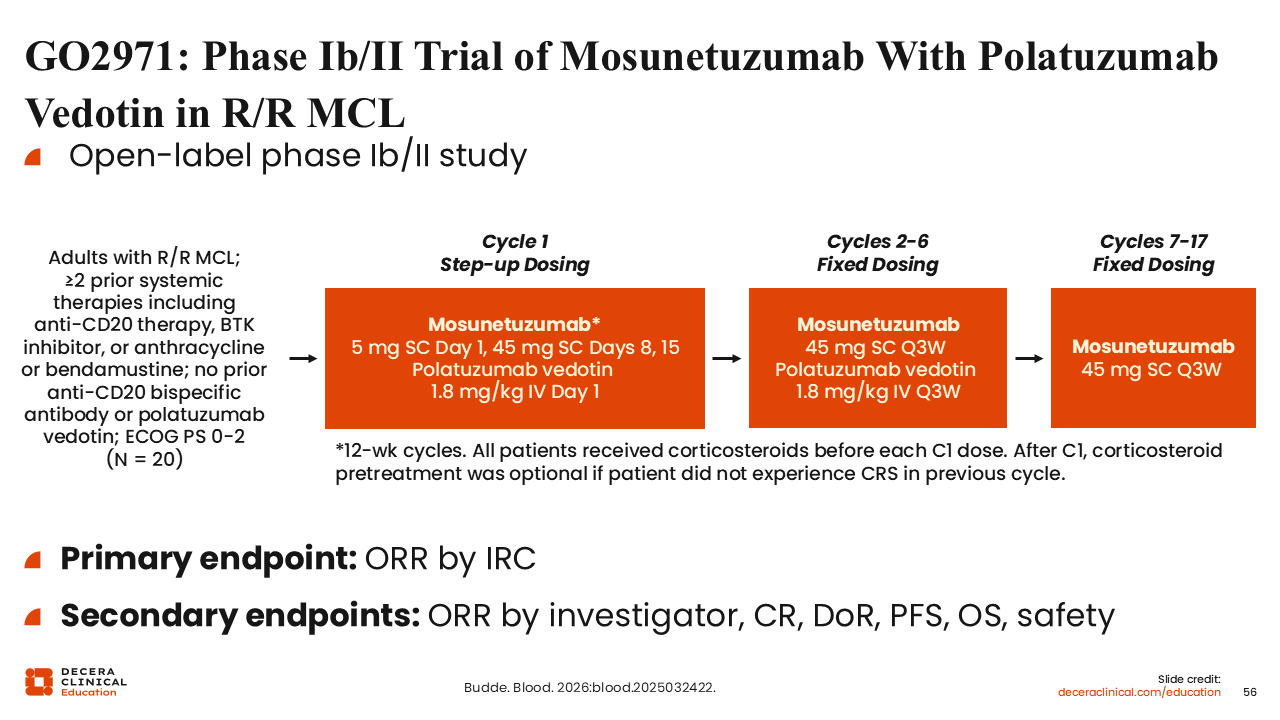
GO2971: Phase Ib/II Trial of Mosunetuzumab With Polatuzumab Vedotin in R/R MCL
Next we will discuss the phase Ib/II study of mosunetuzumab, a CD20/CD3 bispecific antibody, with polatuzumab vedotin in patients with R/R MCL and at least 2 prior systemic therapies (including anti-CD20 therapy, BTK inhibitors, or anthracycline or bendamustine).101 Patients were treated with 17 cycles of mosunetuzumab with initial step-up dosing in cycle 1 and polatuzumab vedotin during the first 6 cycles.
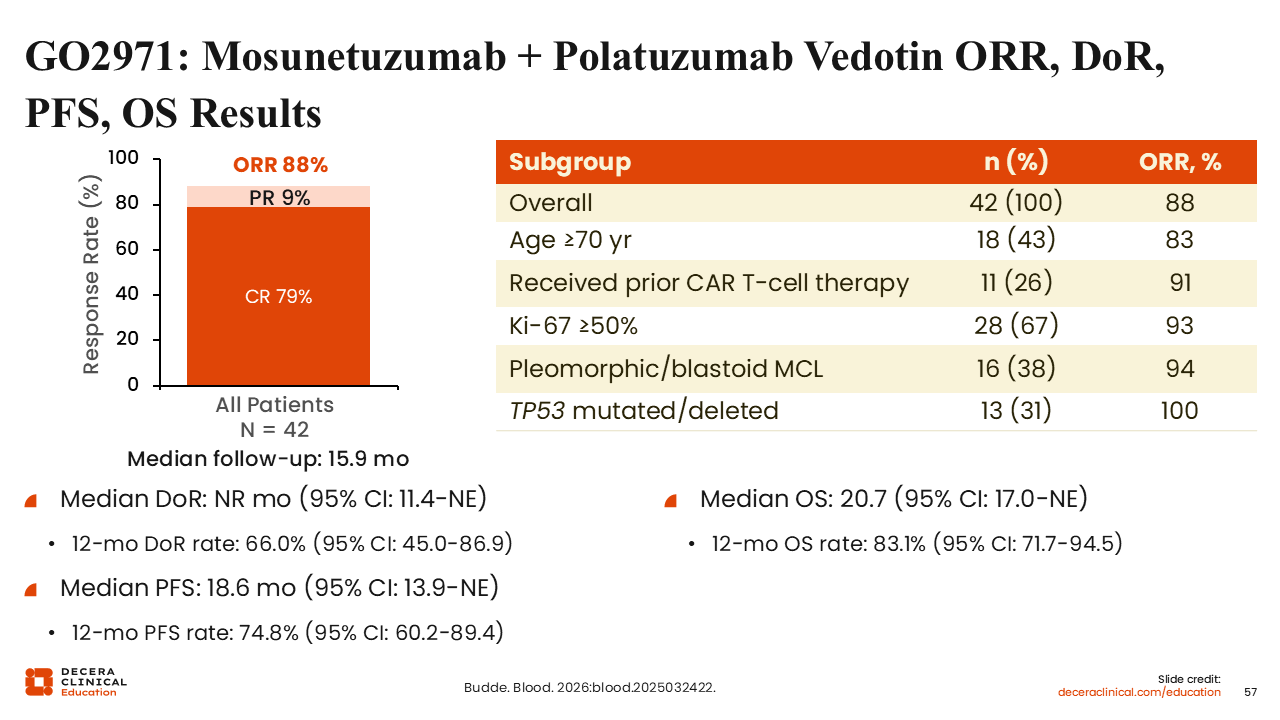
GO2971: Mosunetuzumab + Polatuzumab Vedotin ORR, DoR, PFS, OS Results
In this small patient population of 42 individuals, mosunetuzumab plus polatuzumab vedotin resulted in a high ORR of 88% and CR rate of 79%.101 Subgroup analysis further shows efficacy in some high-risk patient populations, including patients with a TP53 mutation and those with Ki-67 ≥50%.
With short-term follow-up (median: 15.9 months), the median DoR was not reached, median PFS was 18.6 months, and median OS was 20.7 months. The 12-month PFS rate was 74.8%, suggesting mosunetuzumab with polatuzumab vedotin may have some response durability.
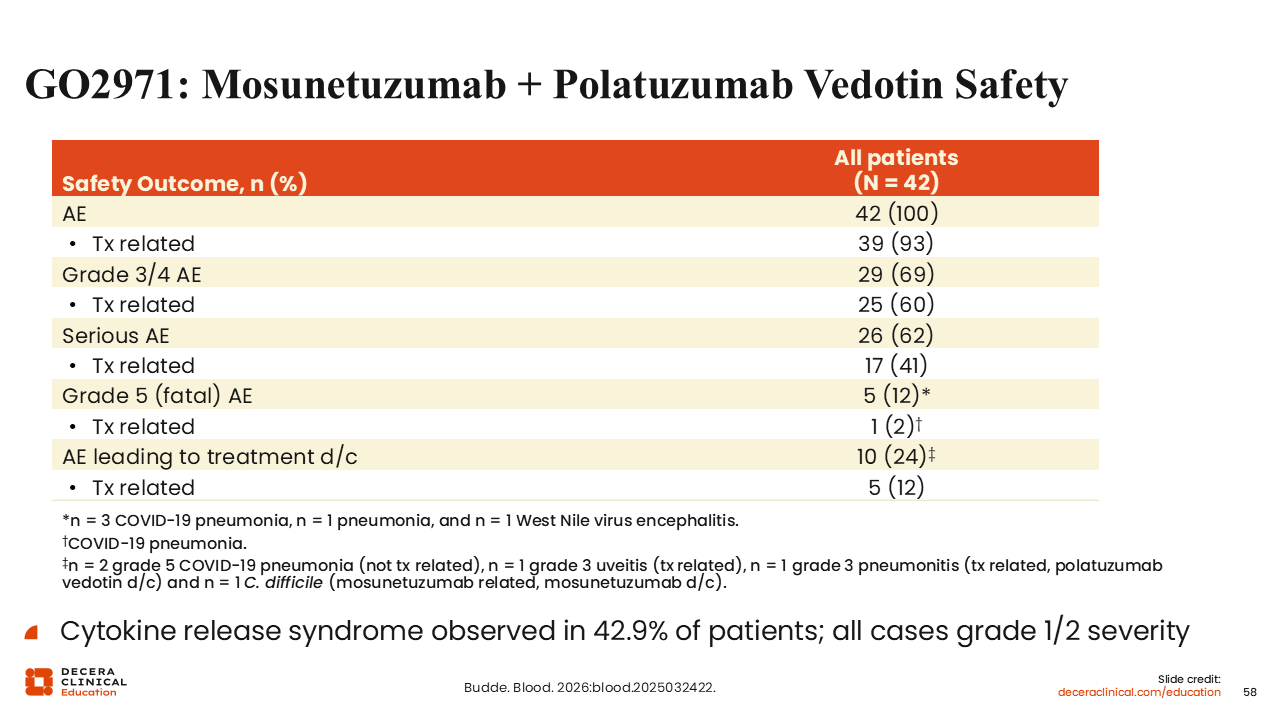
GO2971: Mosunetuzumab + Polatuzumab Vedotin Safety
Of importance, this regimen exhibited low rates of CRS, especially as compared with glofitamab (43% vs 70%), and all were grade 1/2 in severity.100 These preliminary data suggest that mosunetuzumab plus polatuzumab vedotin may have a better safety profile and potentially similar efficacy compared with glofitamab, but currently long-term durability is not clear for patients with R/R MCL.
Summary
MCL is a complex disease with various risk factors and many treatment options in the first-line and R/R settings. Traditionally, chemotherapy combination regimens have been used, but more recently, studies like TRIANGLE and ECHO have demonstrated the efficacy of combining covalent BTK inhibitors with chemotherapy in the first-line setting. In addition, a combination regimen with covalent BTK inhibitors with obinutuzumab and venetoclax is an induction therapy option in patients with TP53 mutations that also has early but encouraging data in older patients. If covalent BTK inhibitors are not used in the frontline setting, covalent BTK inhibitor monotherapy should be the treatment of choice for most patients at relapse, with consideration for combination with venetoclax in select patients. For those who relapse or are refractory to a covalent BTK inhibitor, the noncovalent BTK inhibitor, pirtobrutinib, and CAR T-cell therapy can be used. Between these 2 options, CAR T-cell therapy has the highest and most durable efficacy, especially in patients who are truly resistant to covalent BTK inhibition. Finally, there are recent data for the use of bispecific antibodies in this patient population.
Given the expanding treatment landscape available for patients with MCL, choosing optimal therapy for these patients based on their specific presentation has become more complex. We hope that you find the interactive treatment decision tool with recommendations from 5 experts for many different presentations of MCL that we have illustrated in this module to be a convenient and effective resource to help you with treatment recommendations for your patients with MCL.