CME
Expert Guidance and Clinical Resources to Improve the Care of Patients With Mantle Cell Lymphoma
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
Released: May 19, 2026
Expiration: November 18, 2026

Activity
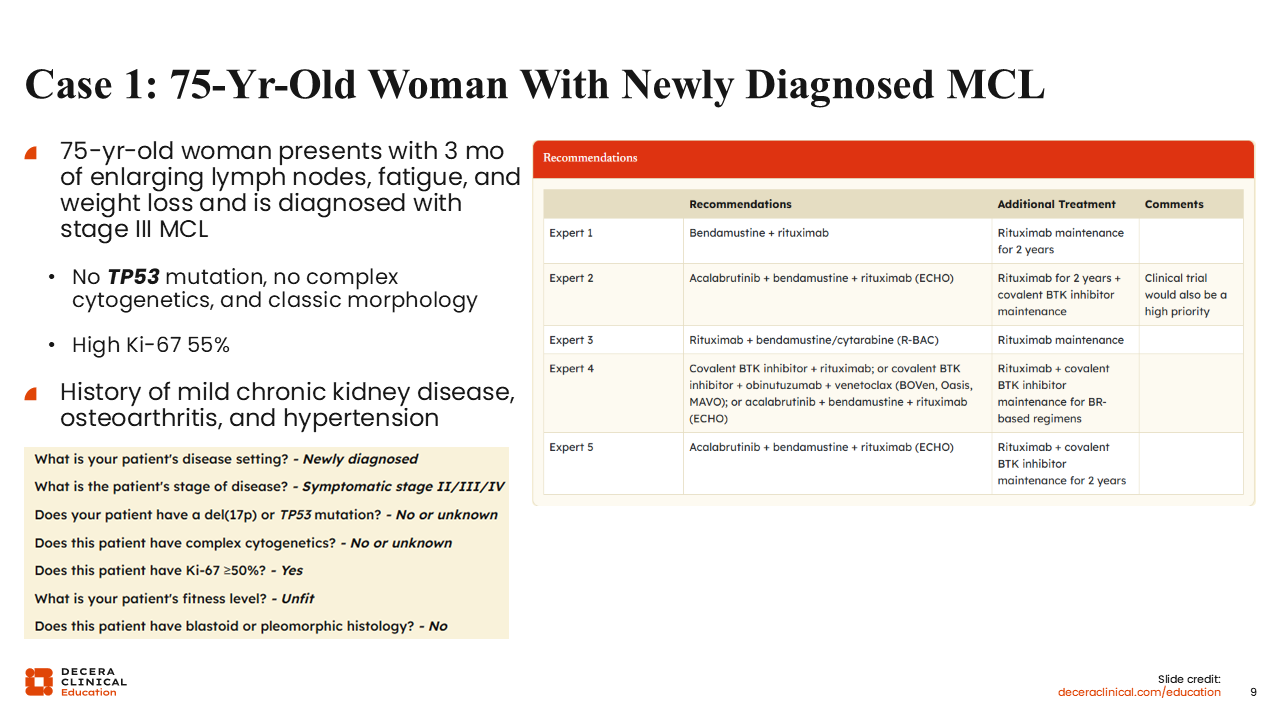
CASE 1: 75-Year-Old Woman With Newly Diagnosed MCL
A 75-year-old woman presents with 3 months of enlarging lymph nodes, fatigue, and weight loss, leading to a diagnosis of stage III MCL. The workup shows she has no TP53 mutations, no complex cytogenetics, and classic morphology, but she has high Ki-67 levels of 55%. She also has a history of mild chronic kidney disease, osteoarthritis, and hypertension.
For this patient, I would recommend the ECHO regimen of acalabrutinib plus BR, which was shown to improve PFS vs BR with rituximab maintenance in older patients with MCL. Given her elevated Ki-67 levels, which also contribute to a high MIPI score, I would further support this regimen over BR alone, as data suggest high-risk MIPI scores are associated with poor outcomes with standard chemotherapy.36
However, we can see differing expert recommendations given by the treatment decision tool. For instance, one expert recommends BR alone. Since sequential use of BR followed by a covalent BTK inhibitor likely has similar PFS to the ECHO regimen with less toxicity, you could reasonably use BR as frontline treatment for this patient. Alternatively, rituximab with bendamustine and cytarabine (R-BAC) has shown sustained efficacy in older patient populations.37 However, R-BAC had significantly lower PFS in patients with high Ki-67 levels than in those with low Ki-67 levels, so it may have limited efficacy for this patient. Another expert on the panel suggested a BOVEN-type regimen based on recent data in older patients with or without a p53 mutation.38 There is limited follow-up on this regimen as compared with ECHO or sequential BR followed by a covalent BTK inhibitor. This expert also suggested the possibility of single-agent covalent BTK inhibitor plus rituximab. Although this patient does not cleanly fit into a category, the elevated Ki-67 could potentially suggest a short PFS based on the phase II ALTAMIRA study.39
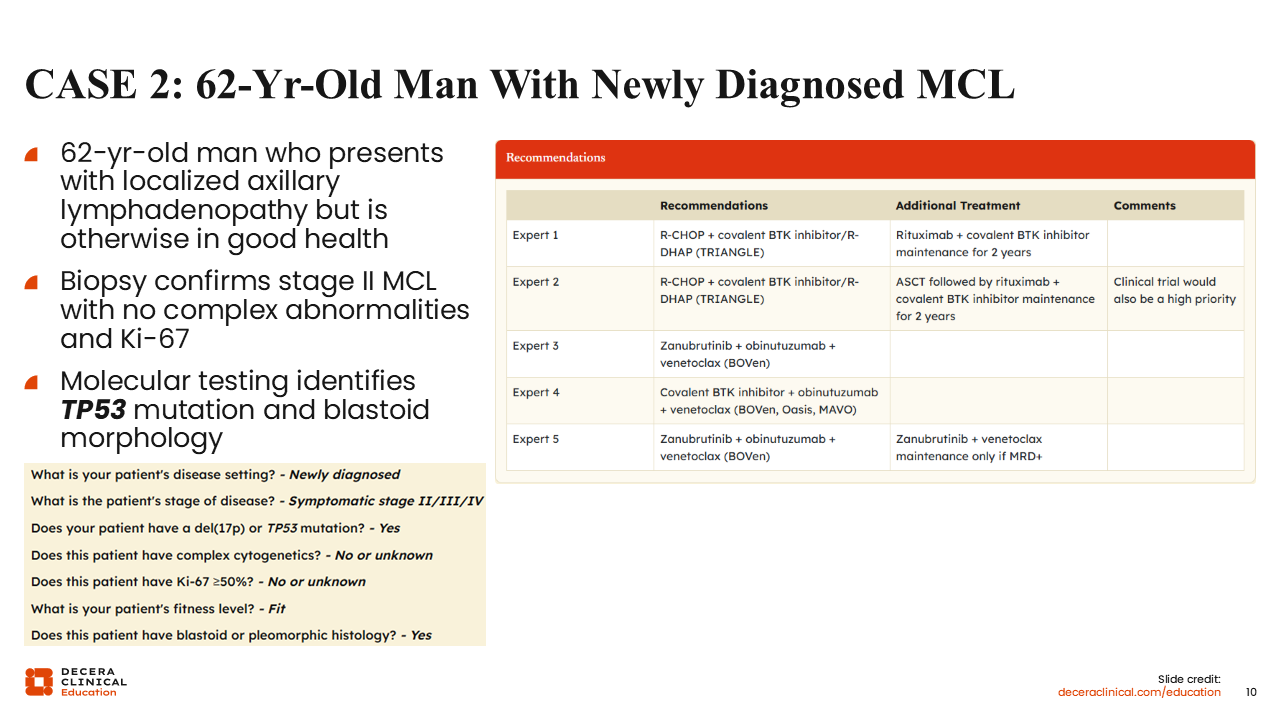
CASE 2: 62-Year-Old Man With Newly Diagnosed MCL
Here is an example of a 62-year-old man who presents with localized axillary lymphadenopathy. Biopsy confirms a diagnosis of stage II MCL with no complex abnormalities and Ki-67 of 20%. Molecular testing identifies TP53 mutation and blastoid morphology. He is in overall good health otherwise.
Patients with TP53 mutations generally have poor outcomes to CIT alone. The addition of a BTK inhibitor to CIT has been shown to improve outcomes in the TRIANGLE, BOVen, and MAVO trials.25,34-41 In addition, the ENRICH study demonstrated that although most patients benefit from ibrutinib with rituximab vs CIT (R-CHOP or BR), it did not show any benefit for patients with blastoid morphology and little benefit for those with TP53 mutations.42 So, given this patient’s high-risk factors, it would appear that a regimen with chemotherapy plus a BTK inhibitor may be more beneficial vs a nonchemotherapy-containing regimen, although there are not enough data to definitively justify a difference in this patient population.
Latest Developments in Frontline Management
In the last few years, we have seen some new developments in the frontline management of MCL. First, we have seen solid retrospective evidence supporting maintenance rituximab after BR and after R-CHOP.43,44 There has been some concern about maintenance after BR based on a prospective study in Germany, but retrospectively, data have supported the use of maintenance rituximab, which has become a standard treatment practice.45-48
As mentioned before, the ECHO trial supports the use of the covalent BTK inhibitor acalabrutinib plus BR in older patients, as this had an improvement in PFS and no detriment to OS or safety in this patient population.20 In younger patients, the first-generation BTK inhibitor ibrutinib was administered with cycles of R-CHOP alternated with R-DHAP and given for 2 years thereafter for maintenance, either after or in the absence of ASCT.25 In both situations, it was an improvement over the alternating regimen without the BTK inhibitor. Retrospective analysis of these data supports the addition of rituximab maintenance to BTK inhibitor maintenance to improve PFS; however, it was associated with a modest increase in infections during maintenance therapy.49
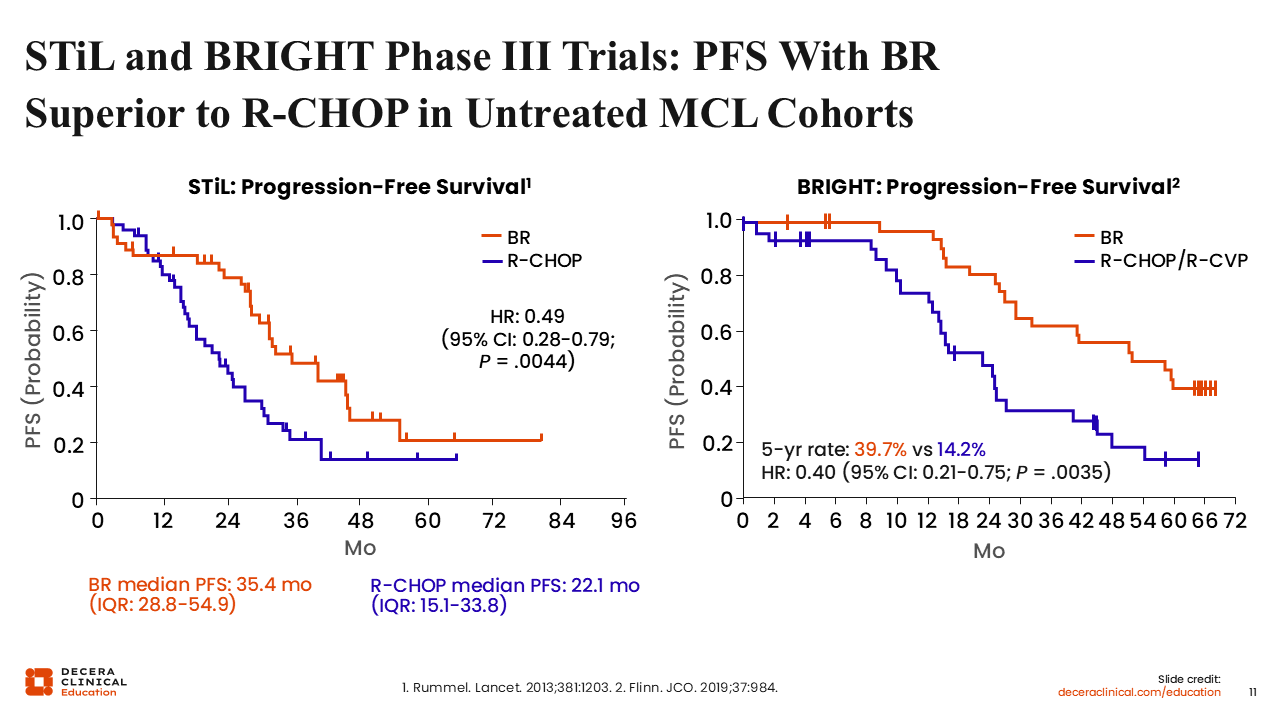
STiL and BRIGHT Phase III Trials: PFS With BR Superior to R-CHOP in Untreated MCL Cohorts
The initial study that supported the use of bendamustine for first-line treatment of MCL was the German STiL study, which showed that BR had superior PFS compared with R-CHOP in several lymphoma subsets.45 This was repeated in the United States and other countries with the phase III BRIGHT study, which confirmed that BR was a better regimen than R-CHOP/R-CVP (rituximab plus cyclophosphamide, vincristine, and prednisone) for MCL.19 These results established BR as a standard treatment backbone for MCL, especially for older patients, within the United States.
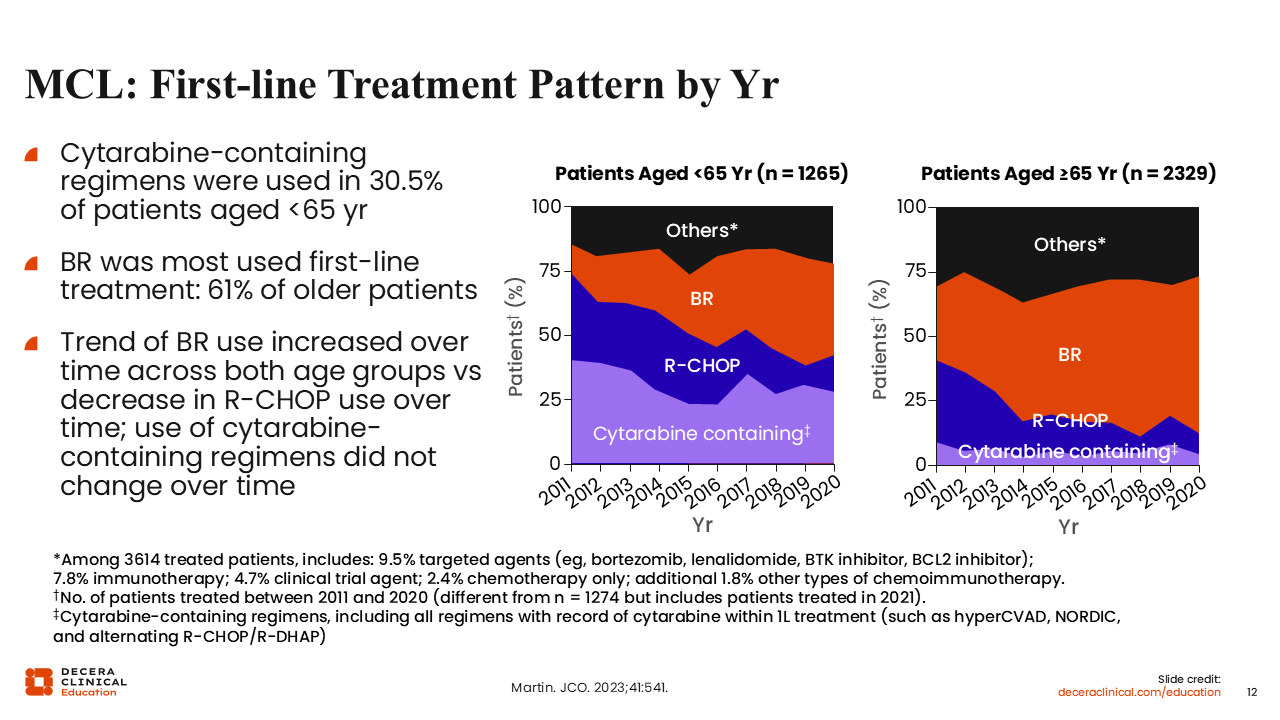
MCL: First-line Treatment Pattern by Year
Here we can see that changes in first-line treatment practices within the community setting from other chemotherapy regimens to BR have been slow, but there has been progressively greater utilization of BR and less of R-CHOP.46 BR use is approximately equal with cytarabine use for patients who are younger than 65 years of age. For older patients, there has been a marked increase in the use of BR, very little use of cytarabine, diminishing use of R-CHOP since approximately 2014, and fairly steady use of other regimens including targeted agents such as bortezomib, lenalidomide, BTK inhibitors, and BCL2 inhibitors.
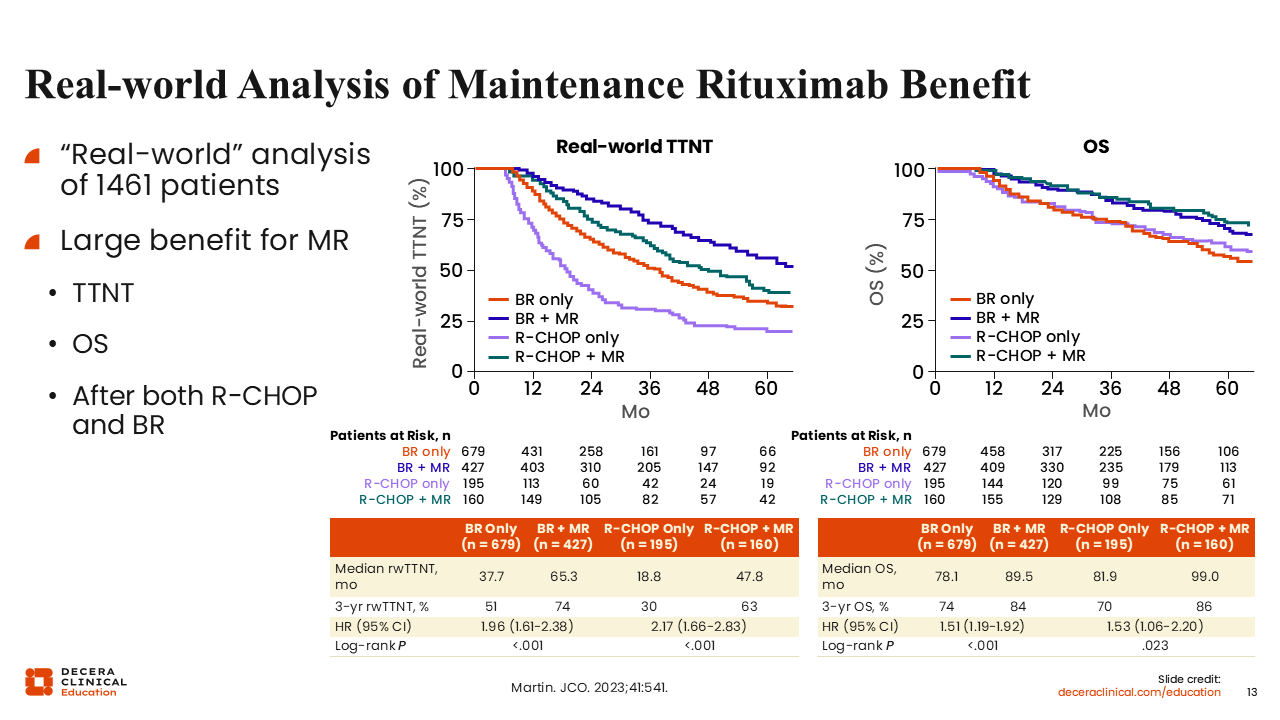
Real-world Analysis of Maintenance Rituximab Benefit
A real-world analysis of the Flatiron database confirms the benefit of BR followed by maintenance rituximab.46 R-CHOP plus maintenance did have some benefit over BR without maintenance rituximab, but the best time to next treatment was noted with BR plus maintenance rituximab. Looking at OS, the 2 maintenance arms of the analysis had the most improvement compared to the chemotherapy-alone arms.
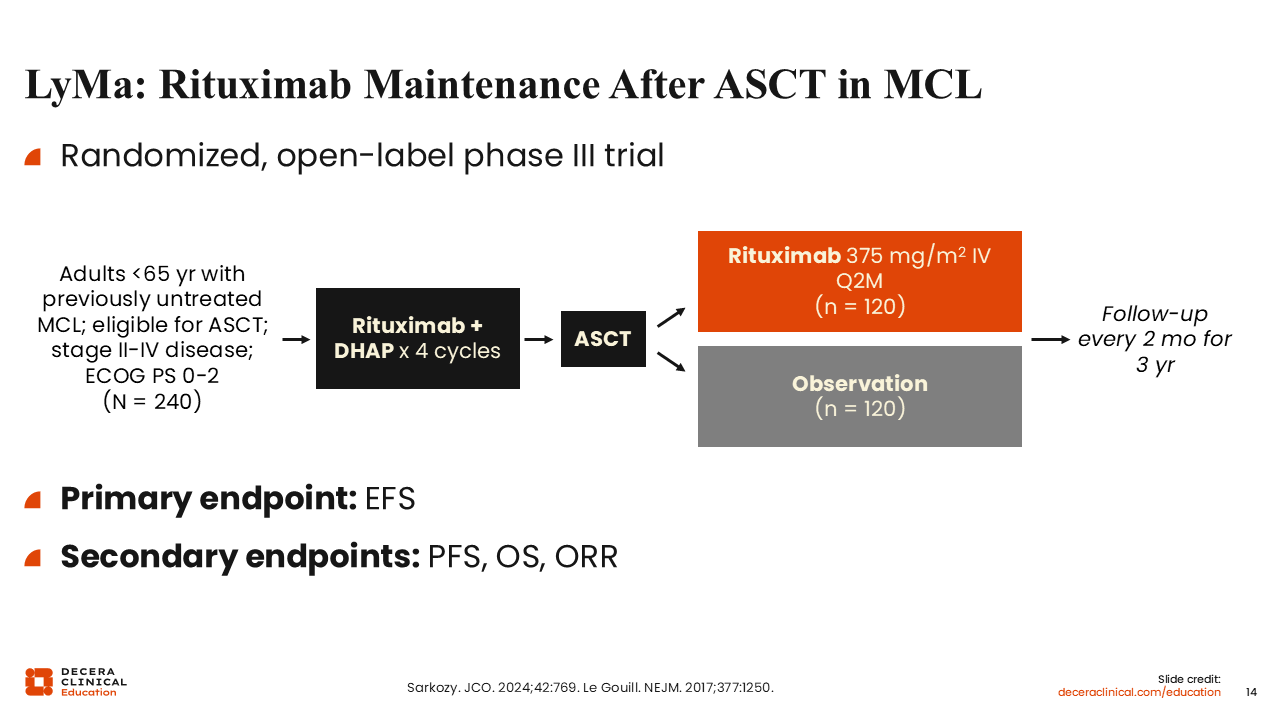
LyMa: Rituximab Maintenance After ASCT in MCL
The phase III LyMa trial treated patients younger than age 65 years of age with previously untreated MCL with R-DHAP for 4 cycles followed by ASCT. They were then randomized to maintenance rituximab or observation with no treatment.
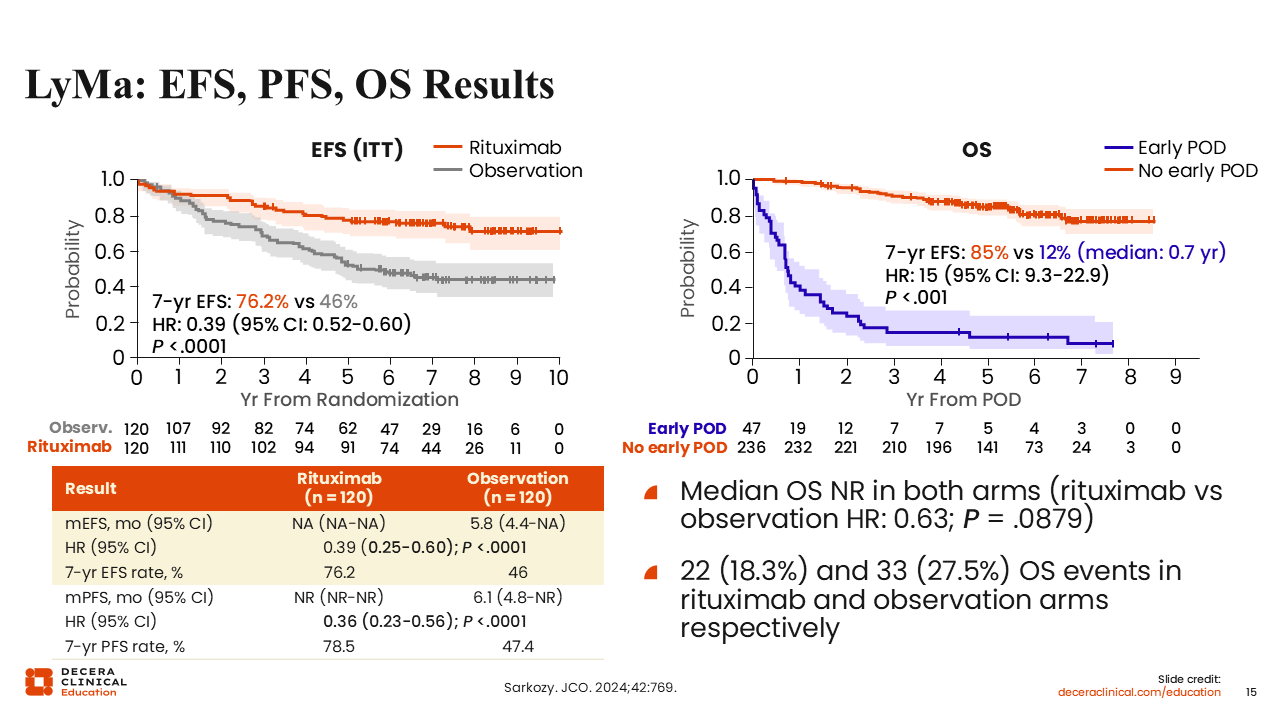
LyMa: EFS, PFS, OS Results
Here we also see that maintenance rituximab after ASCT significantly improved event-free survival and PFS vs no maintenance therapy.50 Long-term follow-up of the study no longer shows an OS benefit, but the remission duration is substantially longer, which is important when treating incurable cancer.
The overall good OS of the observation group suggests that relapses in this arm were a result of a lack of continued disease suppression and that these patients could have had continued positive outcomes with maintenance rituximab. However, relapses of patients with early disease progression (within 2 years of treatment) were more likely caused by aggressive disease, as these patients had higher baseline MIPI scores, blastoid morphology, and Ki-67 >30%.
Thoughts on Maintenance Rituximab
To conclude the discussion on maintenance rituximab, the preponderance of data suggests it has a great benefit for MCL. The PFS benefit is similar to what we see in follicular lymphoma.46,51 Although there is no longer an OS benefit noted with maintenance rituximab, its use is still supported in the majority of patients, given the incurable nature of MCL. The optimal duration is still up for debate and it has primarily been studied after R-CHOP, but currently, 2 or 3 years after induction therapy is the preferred duration. In my clinical practice, rituximab maintenance is typically used for 2 years after BR (NCCN guidelines: 2-3 years) and 2-3 years after a more intensive induction regimen (NCCN guidelines: 3 years with 2 years of covalent BTK inhibitor).18
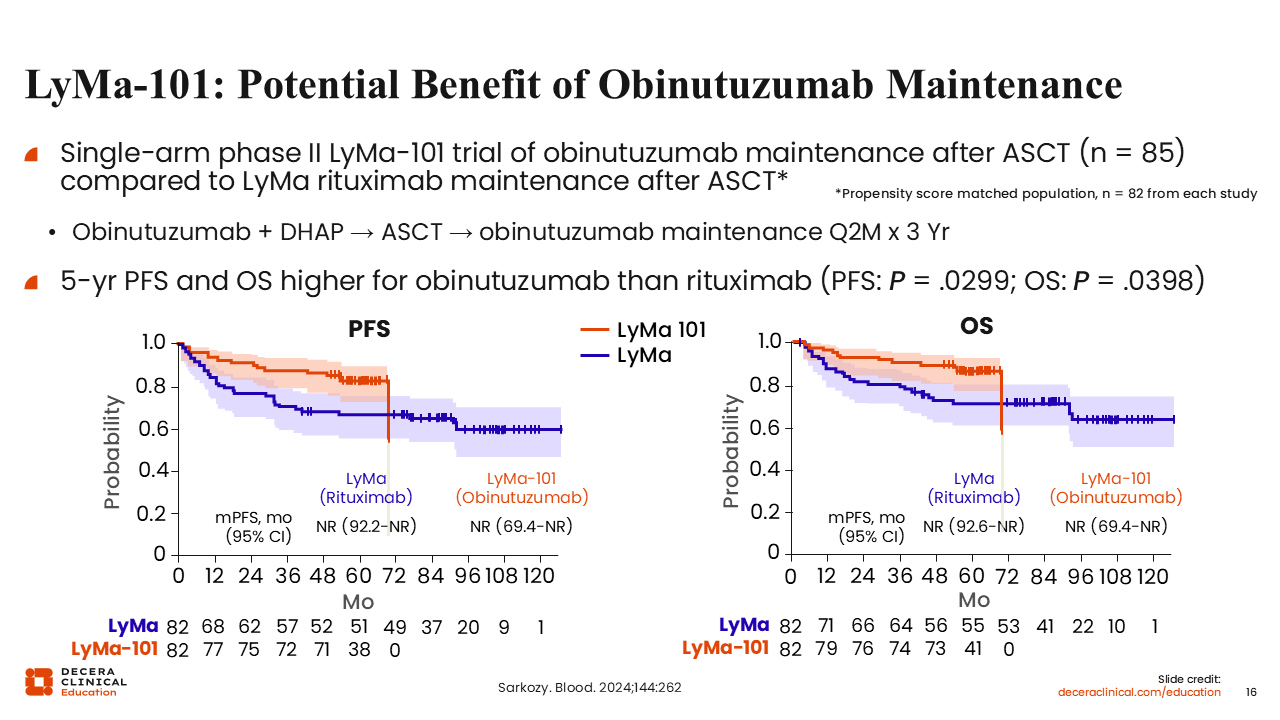
LyMa-101: Potential Benefit of Obinutuzumab Maintenance
There is also the question of whether obinutuzumab, another anti-CD20 monoclonal antibody, is a better option than rituximab in the maintenance setting. LyMa-101 is a prospective study examining maintenance obinutuzumab and was recently compared to the LyMa study.52 LyMa-101 followed the same treatment regimen as the original LyMa trial with obinutuzumab replacing rituximab: obinutuzumab with DHAP followed by ASCT and 3 years of maintenance obinutuzumab. Populations from the 2 trials were propensity score matched for comparative analysis.
These figures suggest that obinutuzumab is a better anti-CD20 antibody vs rituximab for use in MCL, with apparent improvements in 5-year PFS (82.8% vs 66.6%) and OS (86.4% vs 71.4%) but no statistical improvement overall (PFS: P = .0299; OS: P = .0398). Of note, this was not a true head-to-head study, as the R-CHOP arm is a historical comparison.
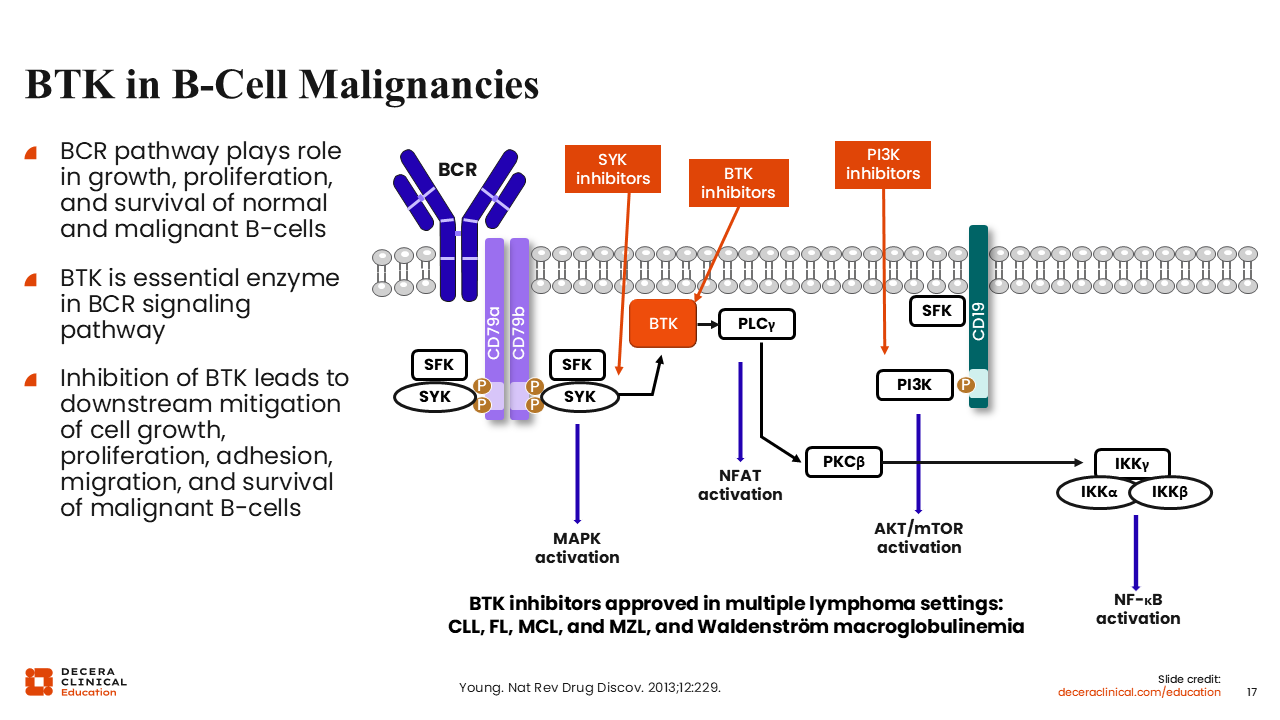
BTK in B-Cell Malignancies
Now, let’s turn our attention to one of the biggest improvements in MCL: BTK inhibitors. The B-cell receptor is a very important signaling mechanism in this disease, and BTK inhibitors, which interfere downstream, have substantial benefit in several lymphoma subtypes such as CLL, follicular lymphoma, marginal zone lymphoma, Waldenström’s macroglobulinemia, and in MCL.53
Ibrutinib: Where It All Started
Ibrutinib was the first-generation BTK inhibitor that was approved for the treatment of MCL in 2013. It was withdrawn from the US market for MCL in 2023 based on the results of the pivotal SHINE study, which tested BR with ibrutinib or placebo in patients with untreated stage II-IV MCL.54 The primary endpoint was reached, with a significant improvement in PFS with the addition of ibrutinib (80.6 vs 52.9 months; P = .01). However, there was no difference in OS (HR: 1.07) and the ibrutinib-containing arm demonstrated increased toxicity compared with the placebo arm, with incidence of grade 3/4 adverse events (AEs) of 81.5% vs 77.3%.
Ibrutinib was considered effective in the original phase II study with a response rate of 68% and median DoR of 17.5 months.55 The ORR is likely higher than that of other BTK inhibitors; however, the study responses were based on CT scans where the other second-generation BTK inhibitors were evaluated with PET scans. In addition, ibrutinib is typically dosed at 560 mg per day for MCL, which is higher than what we used for patients with CLL.56
Some AEs with ibrutinib can be long-term, chronic issues, such as arthralgias or myalgias, which are joint and muscle aches, as well as rash and skin issues.54-56 Over time, we see increasing risk of hypertension, especially with long-term use, although a lot of this evidence is from patients with CLL. There are also varying reports of atrial fibrillation, particularly in older male patients, and ventricular arrhythmia leading to sudden death. In addition, because of off-target effects on platelets, we can see bleeding issues with ibrutinib, so it will need to be held for surgery. This also means it has a contraindication for use with anticoagulants like warfarin.57
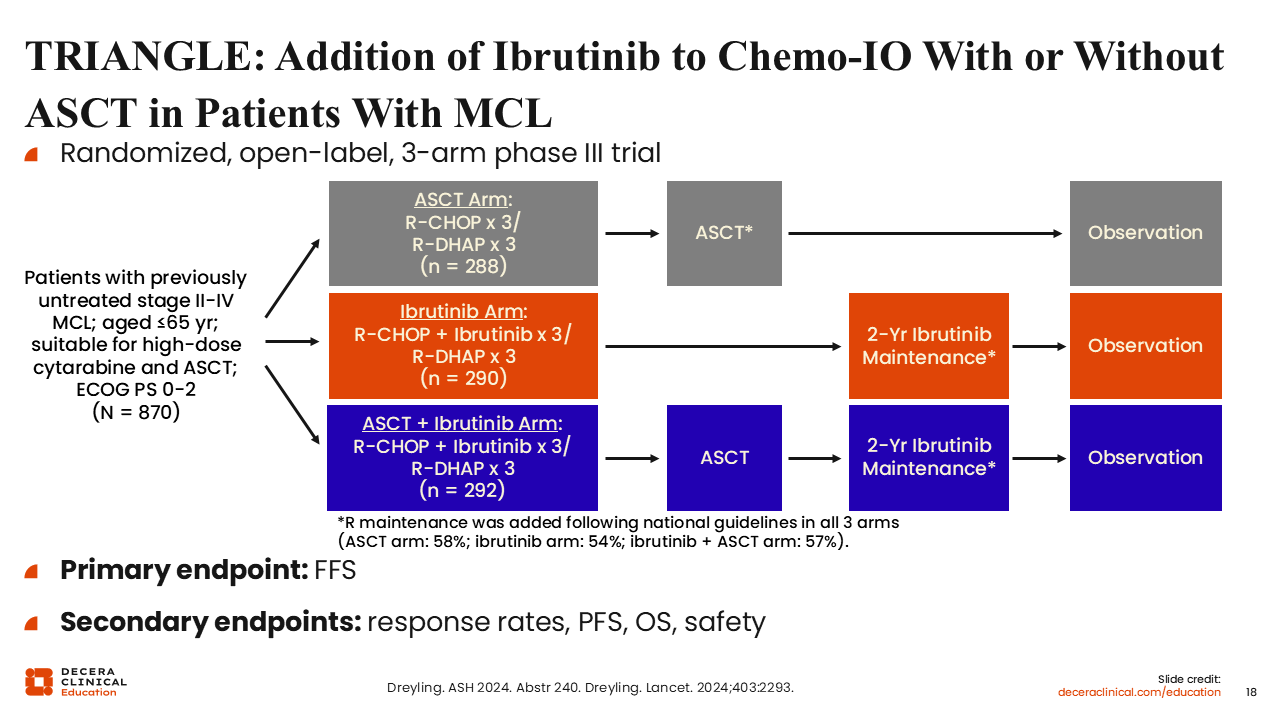
TRIANGLE: Addition of Ibrutinib to Chemo-IO With or Without ASCT in Patients With MCL
As mentioned earlier, ibrutinib was studied in the TRIANGLE trial in younger patients (65 years of age or younger) with untreated MCL.25,58 This was a 3-arm phase III study with the standard-of-care arm consisting of 3 cycles of R-CHOP alternated with 3 cycles of R-DHAP followed by ASCT (A arm). The 2 experimental arms added ibrutinib to the R-CHOP/R-DHAP arm, with or without subsequent ASCT (I and A + I arms), plus 2 years of ibrutinib maintenance and then observation. An important caveat is that the standard-of-care arm did not include any maintenance therapy. Later on in the study, approximately one half of patients in each arm were eventually given rituximab maintenance based on its approval in certain countries at that time.
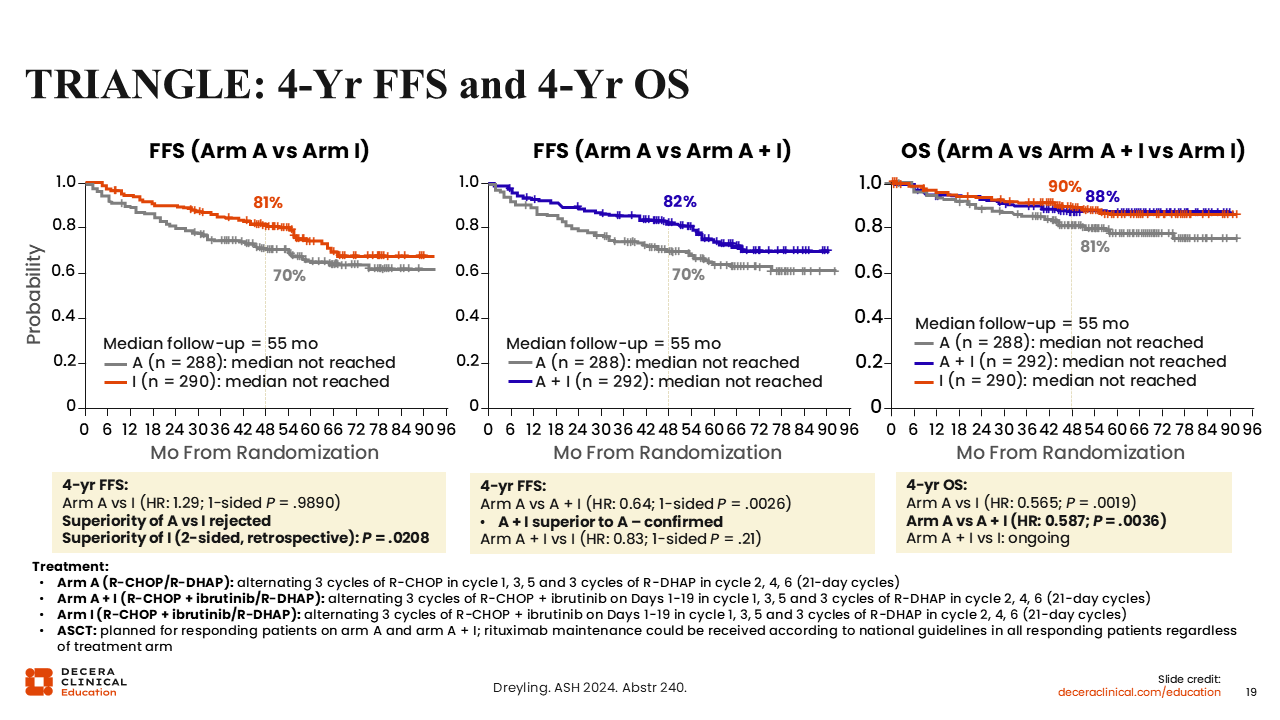
TRIANGLE: 4-Year FFS and 4-Year OS Results
As can be seen with the most recent update, the 2 experimental arms including ibrutinib had a failure-free survival (FFS) benefit and an OS benefit over the standard-of-care arm.25 Of note, we did see a very early separation in the FFS curves, suggesting that some high-risk patients, especially with TP53 alterations, were included in the standard-of-care arm, which is a bit different than what we would have done in the United States. Even with the inclusion of rituximab maintenance, it appears that the FFS benefit maintains an OS benefit in this patient population.
Regarding safety, ASCT with ibrutinib was associated with more grade ≥3 blood and lymphatic system disorders (A + I: 54%; I: 28%; A: 23%) and infections (A + I: 34%; I: 26%; A: 15%) than both the standard-of-care arm and ibrutinib without ASCT arm.
BTK Inhibitor Comparisons
Since the introduction of ibrutinib, we have seen 2 second-generation BTK inhibitors approved in the United States: the covalent BTK inhibitors acalabrutinib and zanubrutinib. These have never been directly compared with ibrutinib in MCL, but there are some data comparing them in other lymphoma subtypes, suggesting that these second-generation BTK inhibitors may have improved efficacy and certainly improved safety in this setting.59-61 Part of the efficacy benefit may be simply because of the better tolerability, which allows patients to stay on these medications for longer periods of time compared to ibrutinib.
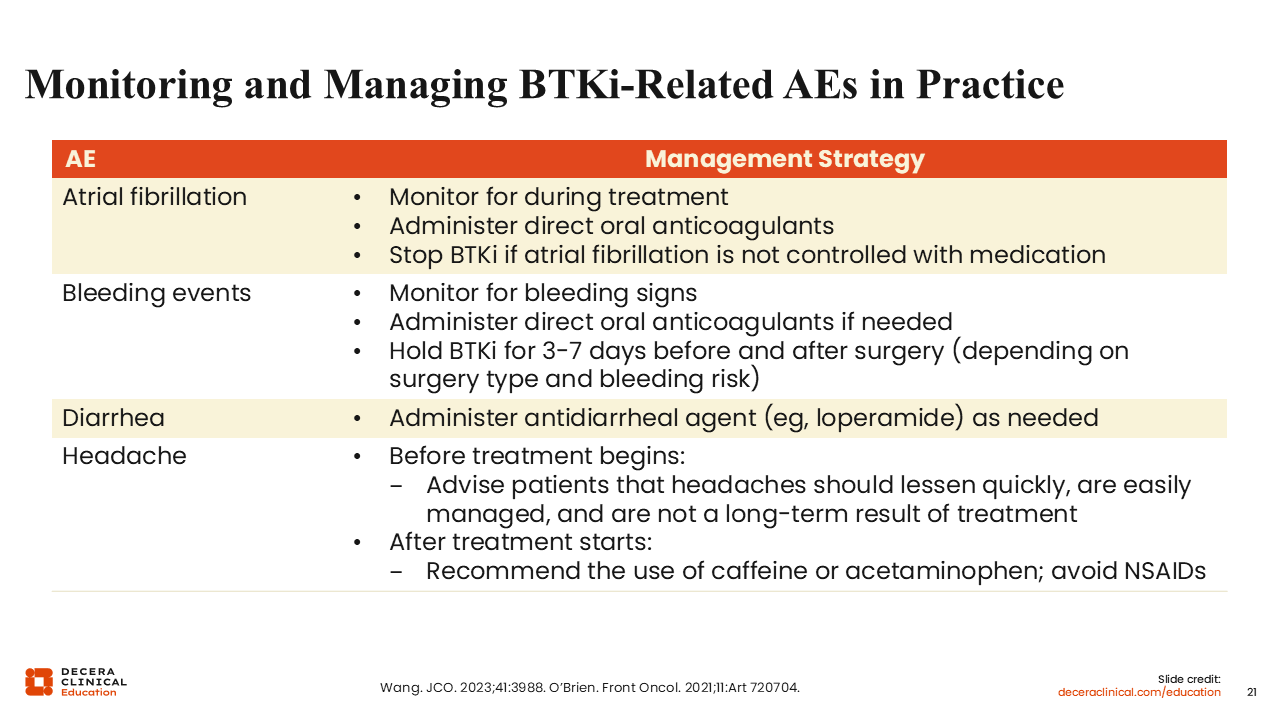
Monitoring and Managing BTK Inhibitor–Related AEs in Practice
Listed here are some of the major AEs of BTK inhibitors, and it appears that some of these are class effects.62,63 Atrial fibrillation can occur, although there are lower rates of atrial fibrillation with acalabrutinib and zanubrutinib. Much of this is related to the higher specificity of these drugs in targeting the BTK receptor, as they affect fewer off-target kinases compared with ibrutinib. Similarly, although all 3 covalent BTK inhibitors are associated with bleeding events, there is less severity with the 2 second-generation drugs.
Diarrhea can be noted with most oral medications given to treat cancers. These instances are generally mild and can be managed with over-the-counter loperamide. Headache is the most common AE associated with acalabrutinib. This is a self-limiting AE that will typically resolve on its own but can be managed with caffeine and does not typically require over-the-counter analgesics.62
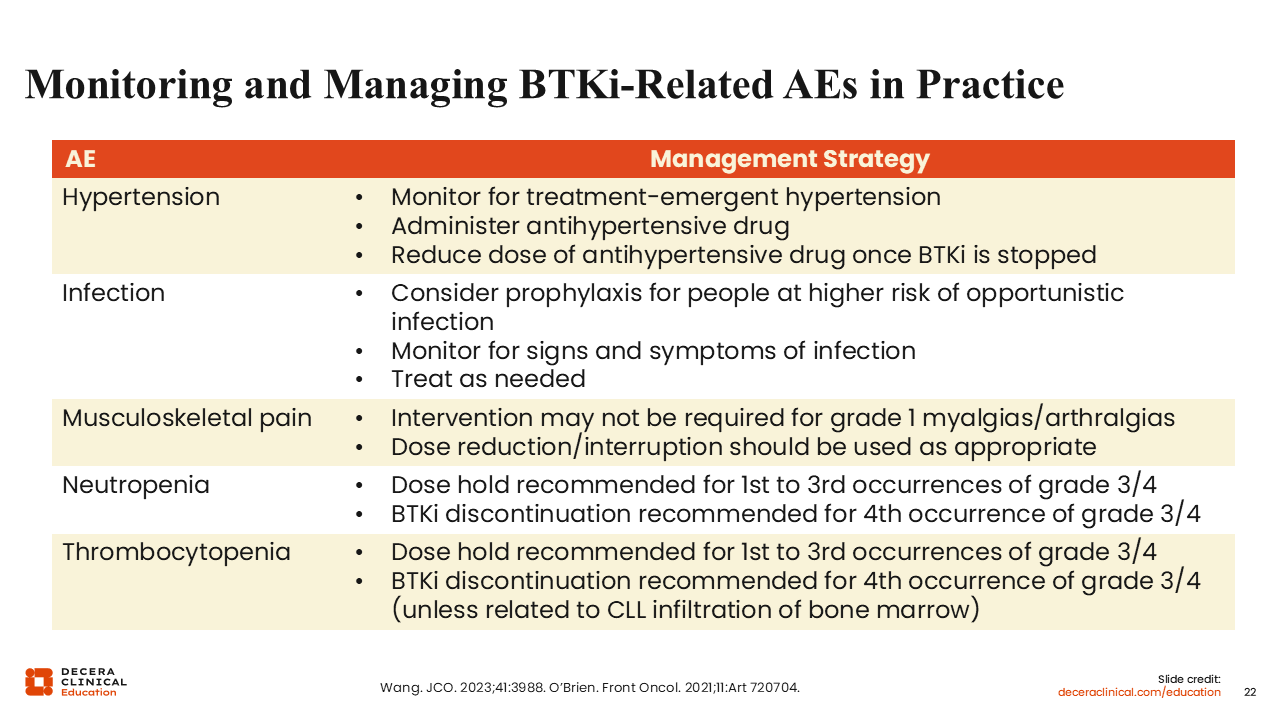
Monitoring and Managing BTK Inhibitor–Related AEs in Practice
Hypertension is a concern with these drugs; it seems to be a long-term AE, as we often see increasing elevation in blood pressure with extended BTK inhibitor use.62,63 There is also a higher incidence of viral infections because these medications suppress the B-cell receptor, which can affect all B-cell activities. There are some reports of neutropenia with zanubrutinib, so there can be some concern for bacterial infections with this agent. In addition, musculoskeletal and joint pain can be long-term, chronic AEs in this patient population. Finally, thrombocytopenia can be seen, but generally most of these drugs will not affect the platelet count. They can cause platelets to be less sticky, however, which increases the risk of bleeding.
Again, most of the AEs noted with these drugs are typically extrapolated from the CLL patient population and long-term use of BTK inhibitors is less common in MCL. So, although we tend not to see many of these long-term AEs, they can be noted if patients with MCL are on these drugs for 3 or more years.
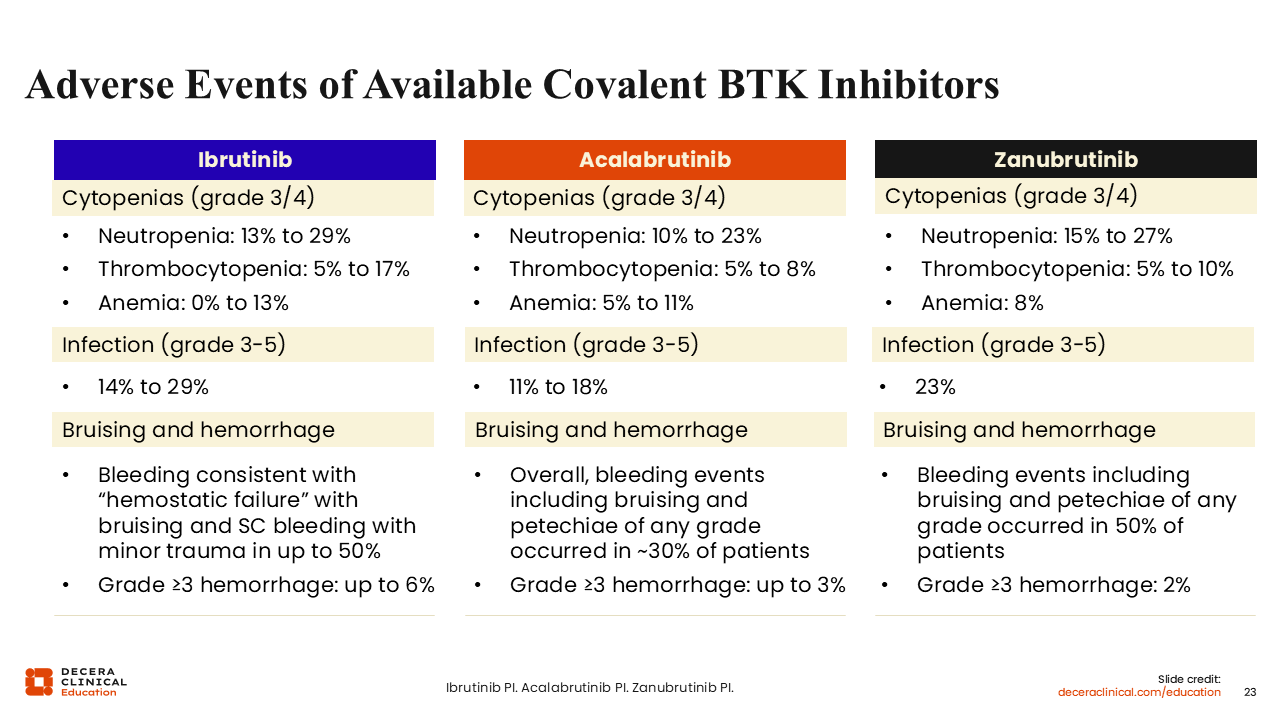
AEs of Available Covalent BTK Inhibitors
Here is a breakdown of AEs by specific covalent BTK inhibitor, with the caveat that ibrutinib is no longer approved for MCL in the United States. As you can see, there are variable rates of neutropenia, thrombocytopenia, and anemia among the different agents.21,57,64 Thrombocytopenia rates are highest with ibrutinib (5%-17%), likely because of having more off-target AEs in general. Infection risks can range from 11% to 29% based on the agent being used, and bruising and bleeding can be noted because of platelet dysfunction.
Decera Clinical Education has updated an interactive decision support tool to help with guidance for the management of AEs associated with covalent and noncovalent BTK inhibitors that are used for patients with MCL. HCPs can enter the details in the tool, such as whether patients have a planned invasive procedure, whether they are receiving a BTK inhibitor as part of a combination regimen, and what specific AE and severity of that event they are experiencing, to view recommendations from experts based on those specific presenting characteristics.
Acalabrutinib
Now we will further discuss acalabrutinib, the first second-generation BTK inhibitor, approved by the FDA for MCL in 2017. It is a more selective BTK inhibitor than ibrutinib, so it is associated with fewer AEs in the CLL patient population.59 Acalabrutinib causes fewer instances of arthralgias, myalgias, hypertension, atrial fibrillation, and bleeding, but it also causes more headaches than the other BTK inhibitors. In addition, the dosage for MCL is 100 mg orally twice daily, whereas ibrutinib is a once-daily medication.21,56
However, acalabrutinib is very effective, with a high ORR of 81.5% and a median DoR of 28.6 months.65 When comparing this agent with the first-generation BTK inhibitor, it is key to consider that the ORR was calculated using PET scans with acalabrutinib vs CT scans with ibrutinib. Also, because acalabrutinib has primarily been tested in the second line, the patient populations in studies were less heavily pretreated before acalabrutinib than before ibrutinib, which was tested in the third-line setting and beyond.
ECHO (ACE-LY-308): Acalabrutinib + BR vs Placebo + BR in Older Patients With Untreated MCL
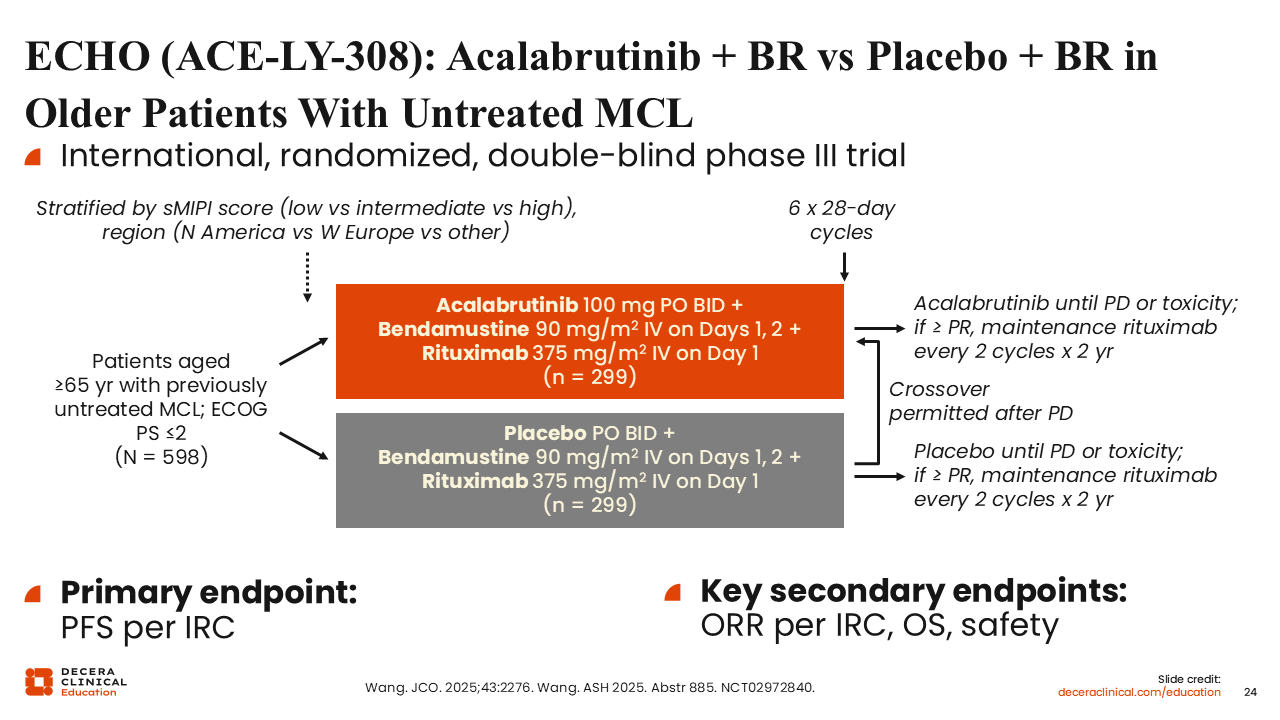
The phase III ECHO study examined acalabrutinib combined with BR vs placebo plus BR.20,66 This patient population was older (65 years of age or older) and considered to be ineligible for an ASCT. They received BR over 6 cycles and acalabrutinib was administered daily. After completing 6 cycles of BR, patients continued acalabrutinib until intolerance or progression. In both arms, if partial response was achieved, patients also continued on maintenance rituximab for 2 years. The primary endpoint was PFS by an independent review committee.
ECHO (ACE-LY-308): PFS, ORR, OS Results
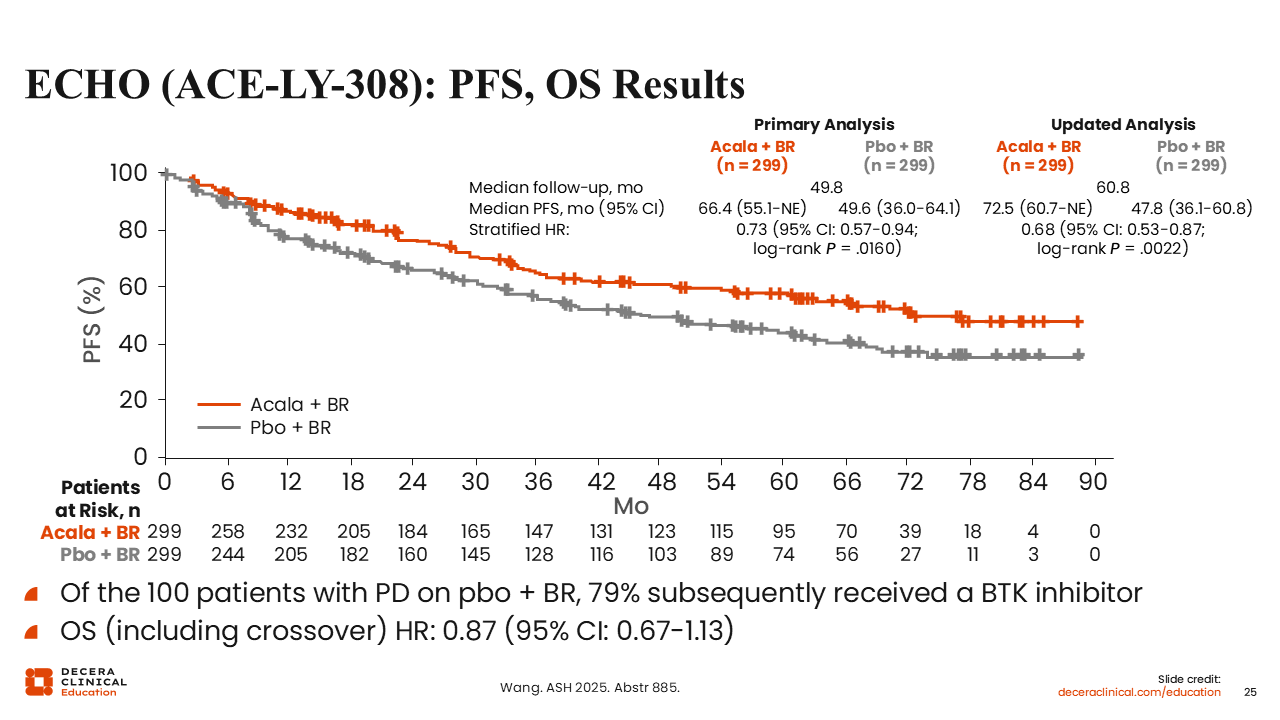
ECHO showed a PFS benefit for acalabrutinib plus BR vs placebo plus BR (median PFS: 72.5 vs 47.8 months; HR: 0.68; P = .0022).66 Of note, patients in the experimental arm were on indefinite therapy, which may account for the PFS difference seen in this patient population. However, we can see a separation of the curves fairly early, at approximately 12 months, where patients in both arms would still be receiving maintenance rituximab.
Median OS was not reached in either arm, although there was a positive trend in OS for acalabrutinib plus BR vs placebo plus BR (HR: 0.87), particularly when censoring COVID-19 deaths (HR: 0.78).
In addition, the incidences of grade ≥3 AEs (89.2% vs 88.6%) and serious AEs (70.4% vs 63.0%) were similar with vs without acalabrutinib.20
EA4181: BR + Cytarabine ± Acalabrutinib vs BR + Acalabrutinib in Previously Untreated Older MCL
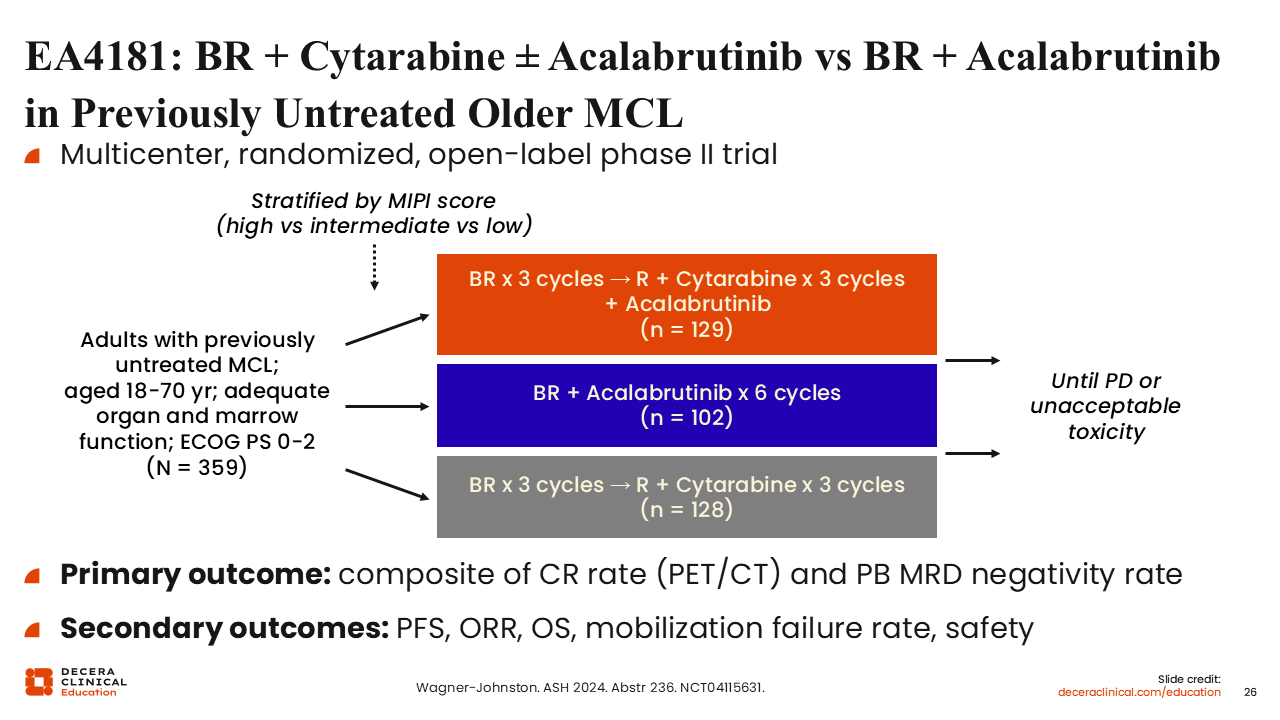
Now we will discuss other regimens using acalabrutinib that are currently being tested. The phase II EA4181 trial evaluated acalabrutinib with 3 arms: BR with acalabrutinib, BR alternated with high-dose cytarabine plus acalabrutinib, and the standard-of-care arm of BR alternated with high-dose cytarabine.67 The primary endpoint was CR rate and the rate of undetectable measurable residual disease (MRD) in the peripheral blood. The goal of this study was to identify the regimen that would provide the highest CR rate and, therefore, could be used as a bridge to either ASCT or maintenance therapy or as consolidation at the initial induction therapy. This study was not designed to evaluate these regimens for long-term benefit.
EA4181: MRD, ORR, CR Results
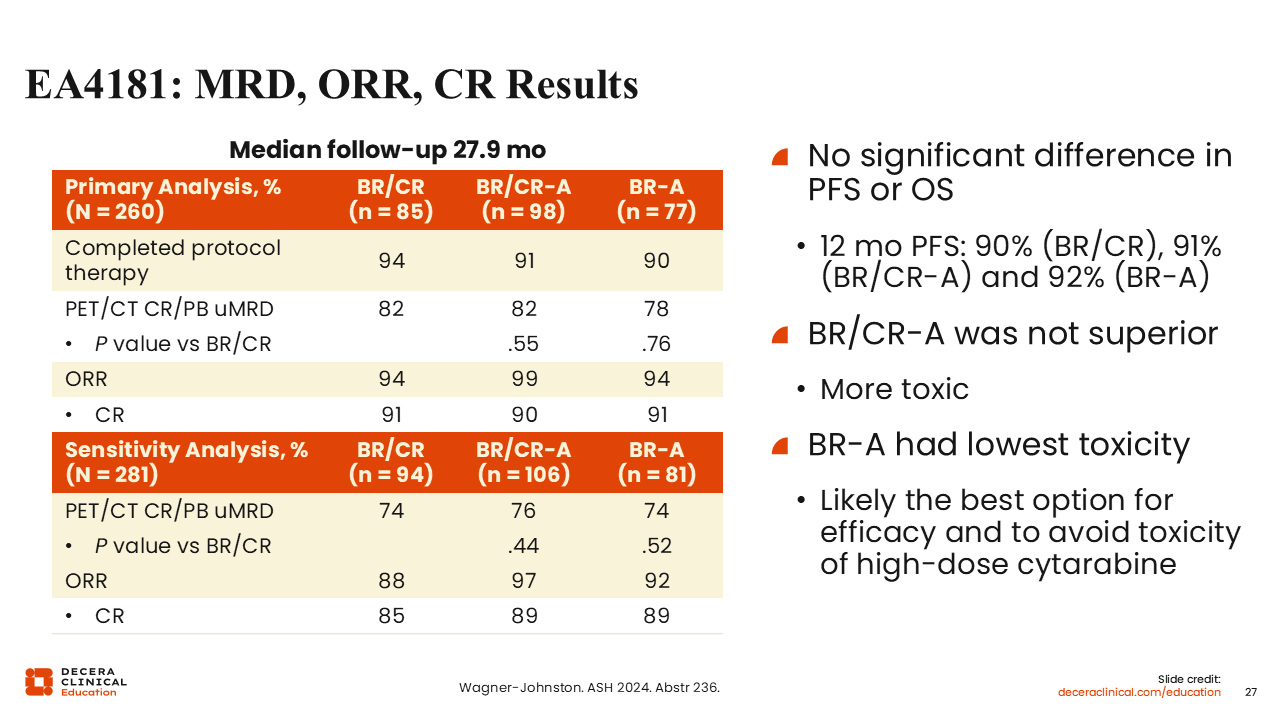
Here we see that there was no significant difference between any of the 3 arms regarding ORR or CR rate.67 All 3 regimens were effective, with high rates of complete metabolic remission (94%-99%) and similar rates of undetectable MRD in the peripheral blood (78%-82%). BR plus acalabrutinib was the arm with the lowest toxicity, so moving forward, this is likely to be the regimen chosen as a backbone for any future studies using bendamustine and acalabrutinib.
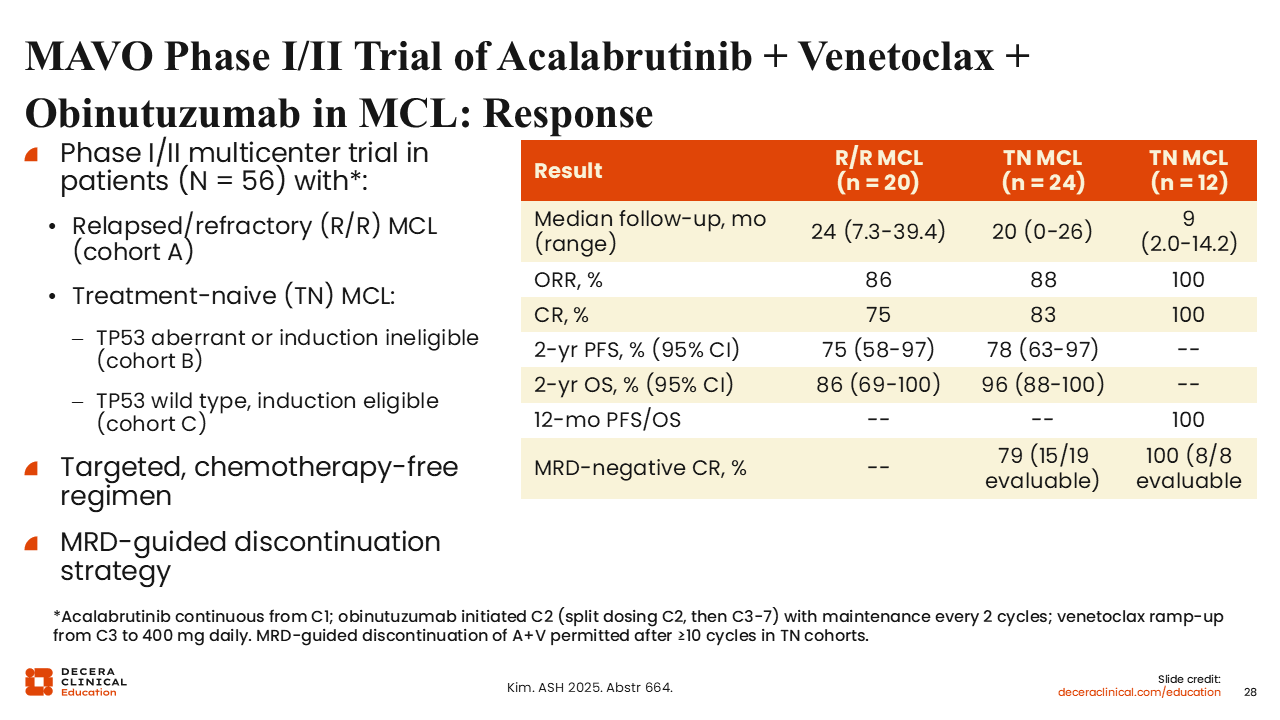
Phase I/II Trial MAVO of Acalabrutinib + Venetoclax + Obinutuzumab in MCL: Response
Here is the phase I/II MAVO study evaluating a chemotherapy-free triplet regimen of acalabrutinib, venetoclax, and obinutuzumab in patients with R/R and treatment-naive MCL.41
Fifty-six patients were enrolled across 3 cohorts, including R/R disease and treatment-naive patients with both TP53-aberrant and TP53 wild-type disease. Treatment consisted of continuous acalabrutinib with obinutuzumab and venetoclax added sequentially, with an MRD-guided strategy allowing treatment discontinuation after sustained MRD-negative CR.
In the R/R cohort, the ORR was 86% with a CR rate of 75%. In treatment-naive patients with TP53-aberrant disease, the ORR was 88% with a CR rate of 83%, and 79% of evaluable patients achieved MRD-negative CR. In the TP53 wild-type cohort, responses were particularly deep, with 100% ORR and CR rates and universal MRD negativity among evaluable patients. These results suggest that the acalabrutinib, venetoclax, and obinutuzumab regimen is highly active across biologically high-risk subgroups and supports the feasibility of MRD-guided, time-limited therapy in MCL.
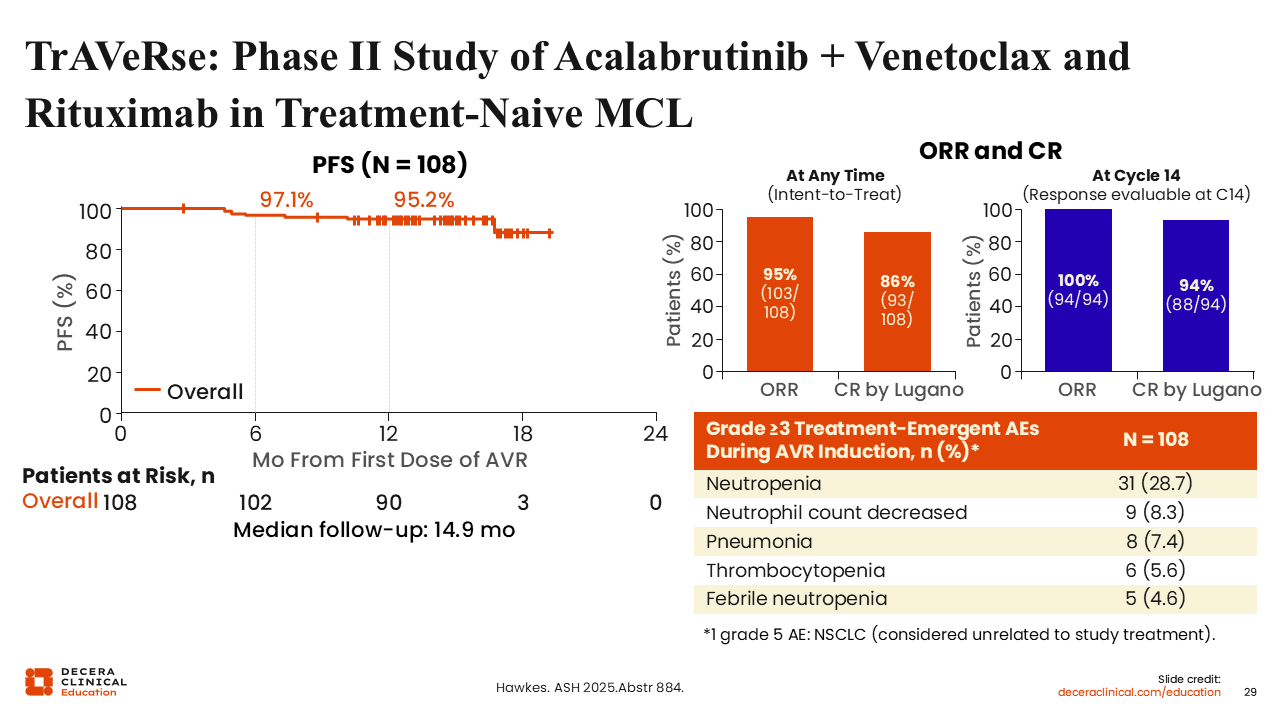
TrAVeRse: Phase II Study of Acalabrutinib + Venetoclax and Rituximab in Treatment-Naive MCL
The phase II TrAVeRse study evaluated the combination of acalabrutinib, venetoclax, and rituximab in 108 treatment-naive patients with MCL.68
Early efficacy results demonstrated a high ORR of 95.4%, with CR rates of 86% by Lugano criteria.
Preliminary PFS rates at 6 and 12 months were 97.1% and 95.2%, respectively, indicating promising early durability. The regimen demonstrated a manageable safety profile, with neutropenia and infections among the most common grade ≥3 AEs.
The TrAVeRse study has completed enrollment and remains ongoing, with longer follow-up needed to confirm durability of responses and long-term safety.
Zanubrutinib
Zanubrutinib is another second-generation BTK inhibitor approved for MCL in the United States. Although it has not been tested against ibrutinib for MCL in a head-to-head trial, it is considered a more selective kinase inhibitor than ibrutinib, with fewer AEs and a high ORR and DoR in patients with R/R CLL.60 Zanubrutinib’s improved efficacy is likely driven by the improved safety and subsequent higher compliance and ability of patients to stay on the medication. Zanubrutinib provides some flexibility with dosing, as these patients can take 160 mg twice daily or 320 mg once daily.64
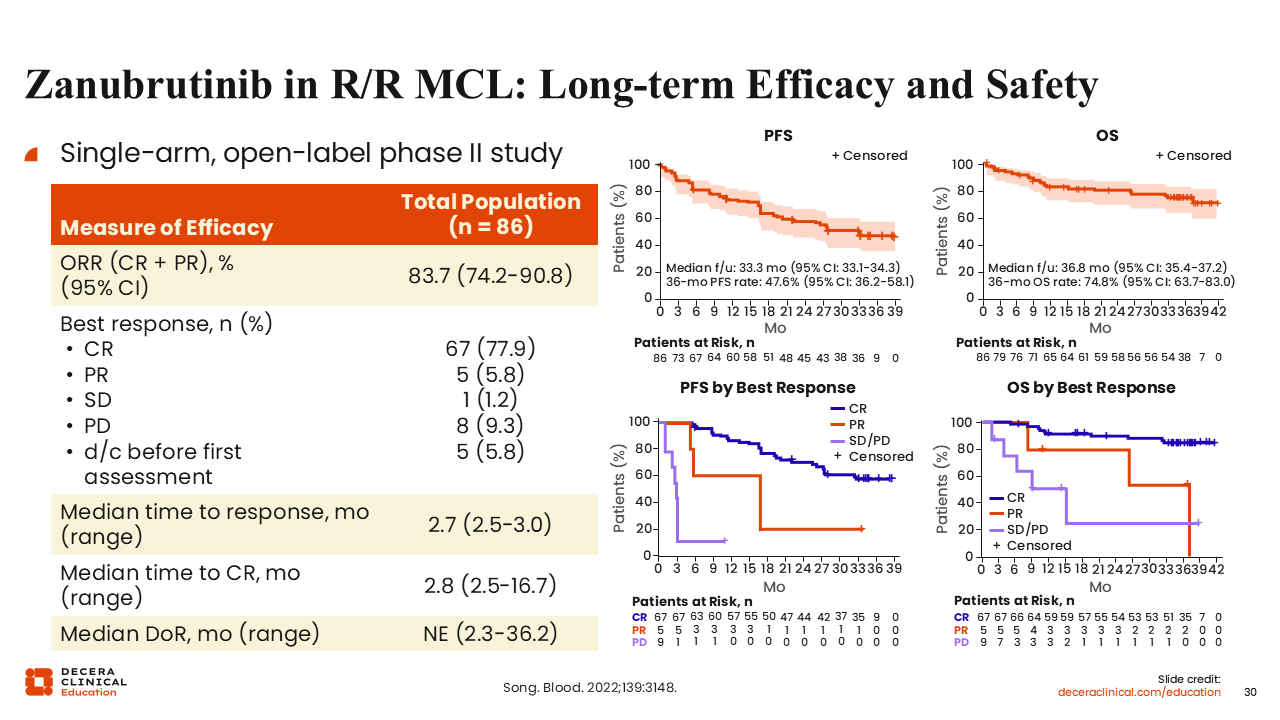
Zanubrutinib in R/R MCL: Long-term Efficacy and Safety
Regarding the long-term efficacy of zanubrutinib in MCL, the results demonstrate efficacy comparable to that observed with acalabrutinib. Also, similar to long-term follow-up results of ibrutinib, patients who achieved CR with zanubrutinib had higher OS than those who did not respond to treatment and long and durable PFS, with some remissions in this phase II study approaching up to 3 years.69
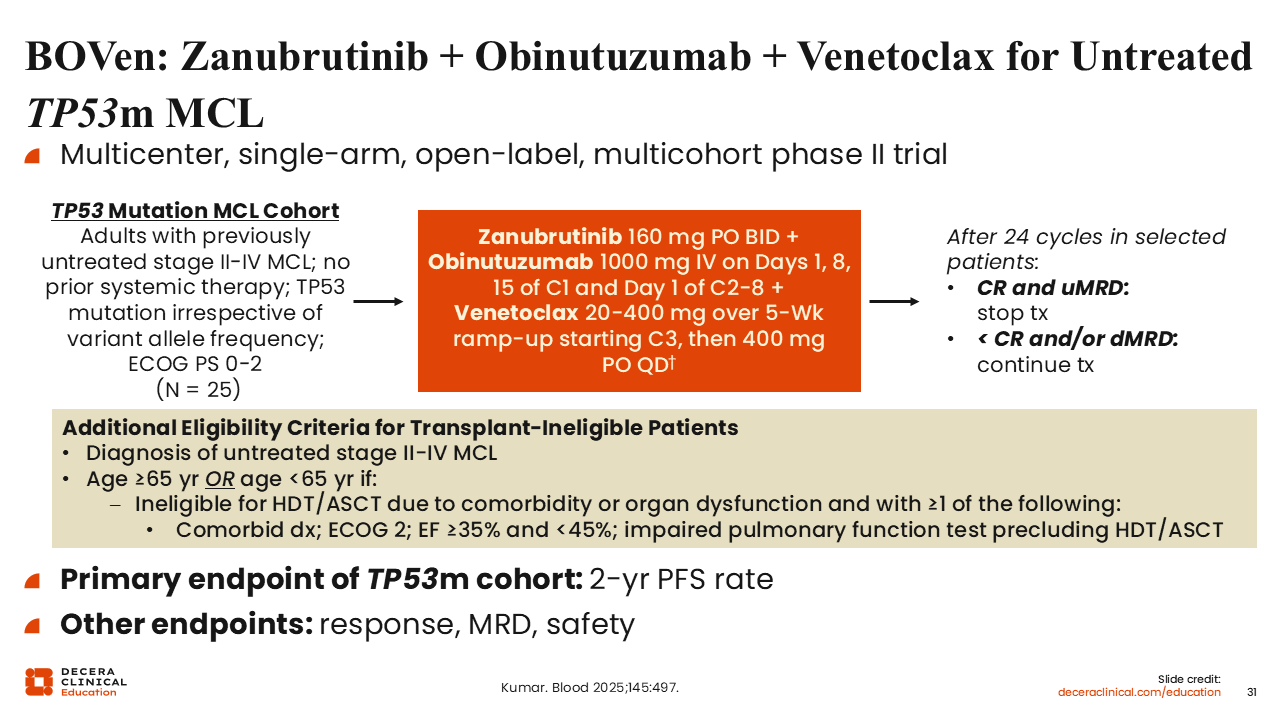
BOVen: Zanubrutinib + Obinutuzumab + Venetoclax for Untreated TP53m MCL
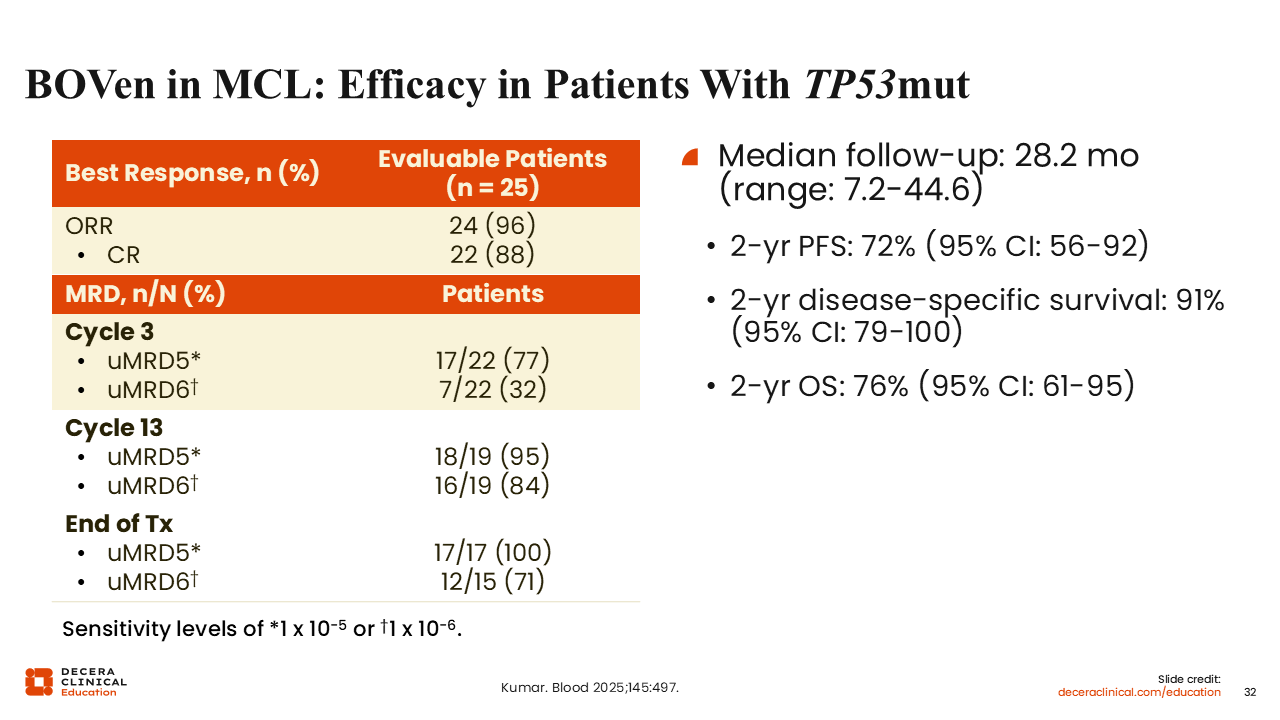
The phase II BOVen study was designed to investigate patients with untreated CLL, small lymphocytic lymphoma, or MCL.24,40 Here, we will focus on the cohort of patients with MCL and TP53 mutations who initially received obinutuzumab and zanubrutinib and received venetoclax with step-up dosing starting on cycle 3 to reduce the risk of tumor lysis syndrome. Patients continued this regimen for 24 months if tolerated, at which point select patients with CR and MRD undetectability could discontinue therapy and be monitored. Others had the option of continuing the therapy indefinitely.
BOVen in MCL: Efficacy in Patients With TP53mut
This regimen resulted in high ORR (96%) and CR (88%) rates as well as high rates of undetectable MRD (uMRD5 at the end of treatment: 100%) in patients with TP53-mutated MCL.40 The TP53-mutated MCL cohort met its primary endpoint of a significant 2-year PFS rate (72%). This was markedly higher than what we observe in younger patients with TP53-mutated MCL treated with CIT, where the median PFS is less than 1 year.70 Neither the Ki-67 or MIPI risk score were significantly associated with PFS or OS. Blastoid or pleomorphic variant morphology was associated with inferior PFS and OS.
The response rates were similar in the older patient population (with MCL, with or without TP53 mutations), but the available data were collected during an early follow-up, so later data will determine the durability of this response.24 Of importance, there was minimal toxicity that led to treatment discontinuation in this patient population (1 discontinuation due to a treatment-related AE), supporting the long-term viability of this regimen in older patients.
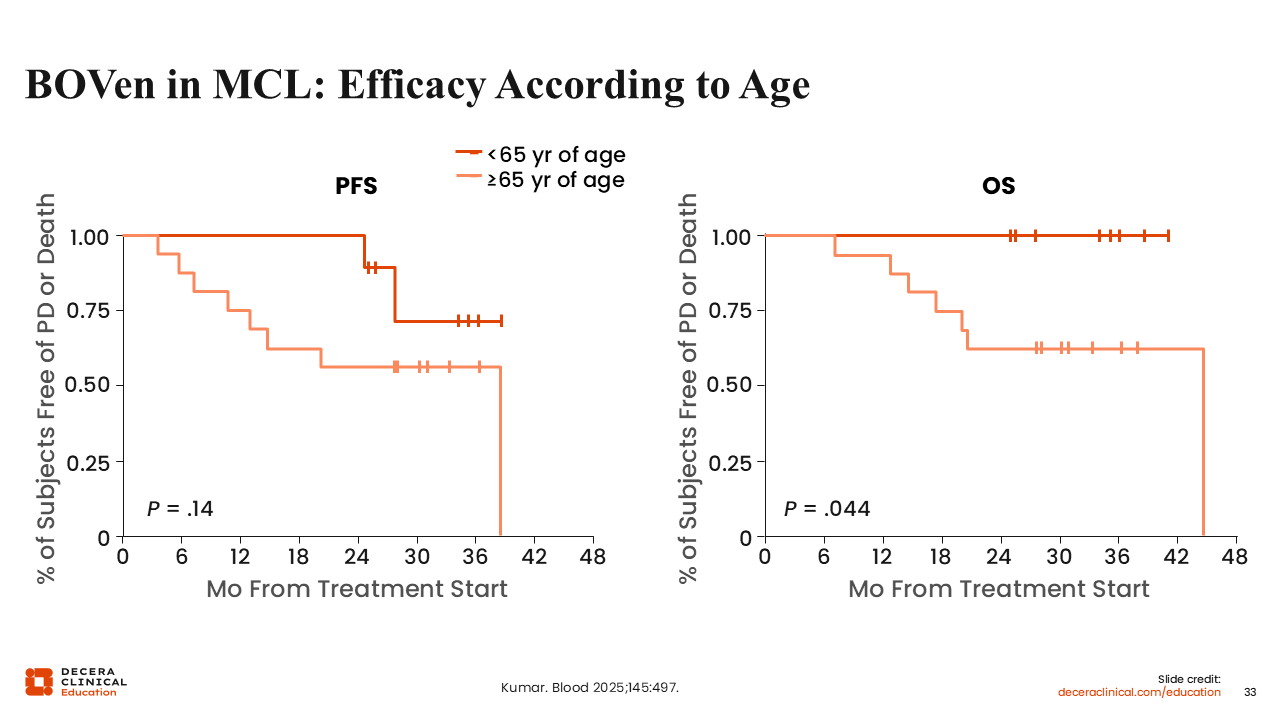
BOVen in MCL: Efficacy According to Age
When stratified by age, no statistically significant difference in PFS was observed between younger and older patients (P = .14), suggesting comparable disease control regardless of age. However, OS appeared inferior in patients 65 years of age or older, with a statistically significant difference (P = .044), indicating worse OS outcomes in older patients.
This difference could be influenced by nondisease-related factors, as several deaths were unrelated to MCL (eg, COVID-19 and other comorbid conditions).
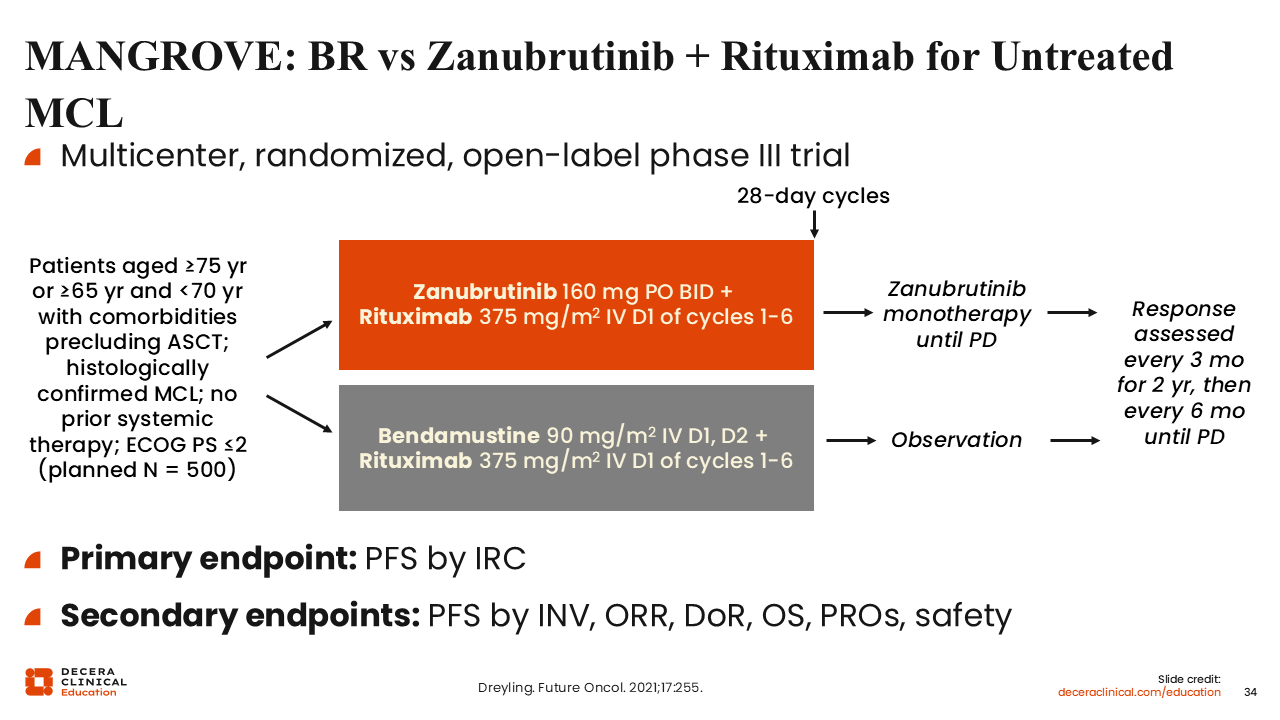
MANGROVE: BR vs Zanubrutinib + Rituximab for Untreated MCL
Another key trial of zanubrutinib that is underway in previously untreated MCL is the phase III MANGROVE study (NCT04002297). We are awaiting results from this trial, which is no longer recruiting and has randomized patients who are ASCT ineligible to zanubrutinib with rituximab or BR.
A key aspect of this trial is that patients in the zanubrutinib plus rituximab arm will continue zanubrutinib monotherapy until disease progression or intolerance, whereas the BR arm does not include maintenance therapy. As we previously discussed, BR followed by maintenance therapy has a substantial benefit compared with BR alone, which somewhat disadvantages the standard-of-care arm in this study.