CME
Expert Guidance and Clinical Resources to Improve the Care of Patients With Mantle Cell Lymphoma
Physicians: Maximum of 1.00 AMA PRA Category 1 Credit™
Released: May 19, 2026
Expiration: November 18, 2026

Activity
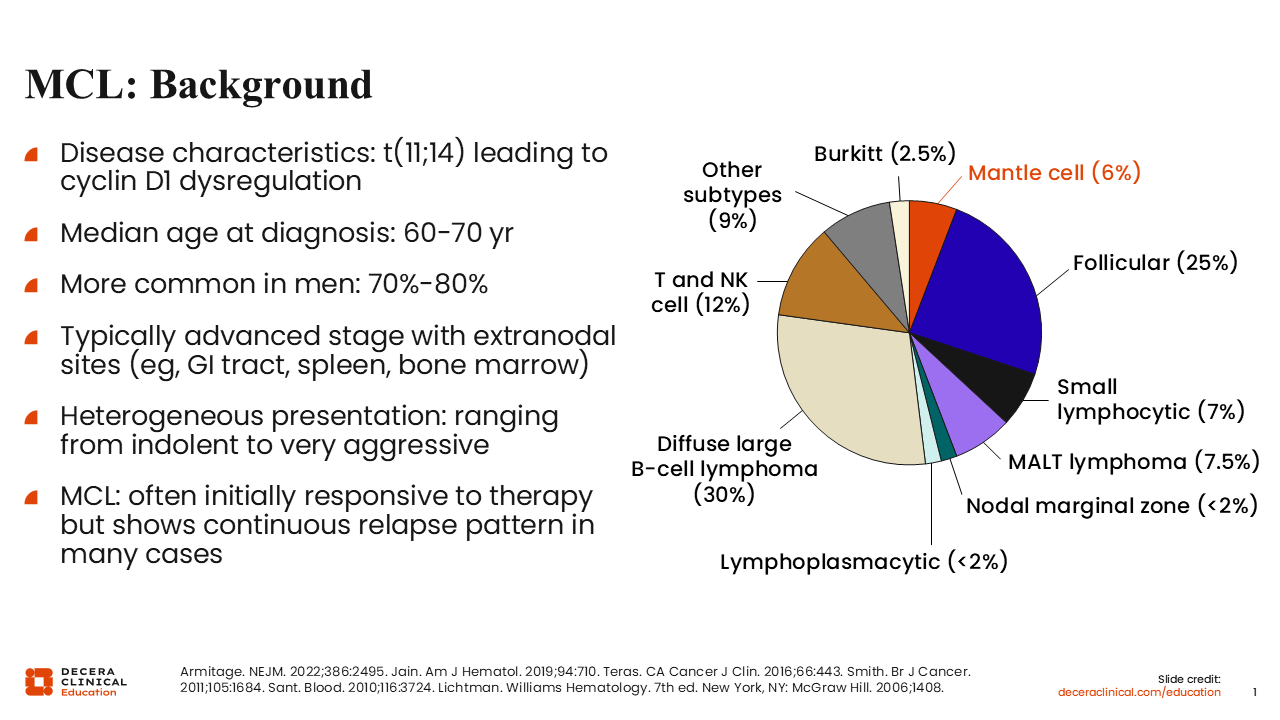
MCL: Background
MCL is a rare lymphoma, accounting for approximately 3% to 10% of B-cell non-Hodgkin lymphomas in the United States with approximately 5000 new cases per year.1-6 It is typically diagnosed by the presence of cyclin D1 and/or SOX11 by immunohistochemistry or (11;14) translocation by fluorescence in situ hybridization.1 The typical immunophenotype detected by flow cytometry is CD5-positive, CD23-negative, CD20 bright, or FMC7-positive, which helps distinguish MCL cases from chronic lymphocytic leukemia (CLL).1,3 In addition, most patients with MCL who are cyclin D1 negative will have expression of SOX11, which is also helpful for diagnosis.7
Most patients with MCL are older, with a median age of 65 years. MCL is more common in men, who represent 70% to 80% of the patient population.1-3 Patients usually present with advanced-stage disease, and it is common to have disease within the bone marrow and the gastrointestinal tract, which includes the stomach and colon.
MCL is an extremely heterogeneous disease, so there is variability in patient presentation ranging from indolent to aggressive.3 Most patients will initially have a strong response to frontline therapy, but relapses can be rapid depending on patient characteristics. MCL is incurable, so we typically would expect multiple relapses and the longest duration of responses (DoRs) with first-line therapy. However, there have been improvements with subsequent lines of therapy to help extend outpatient OS.
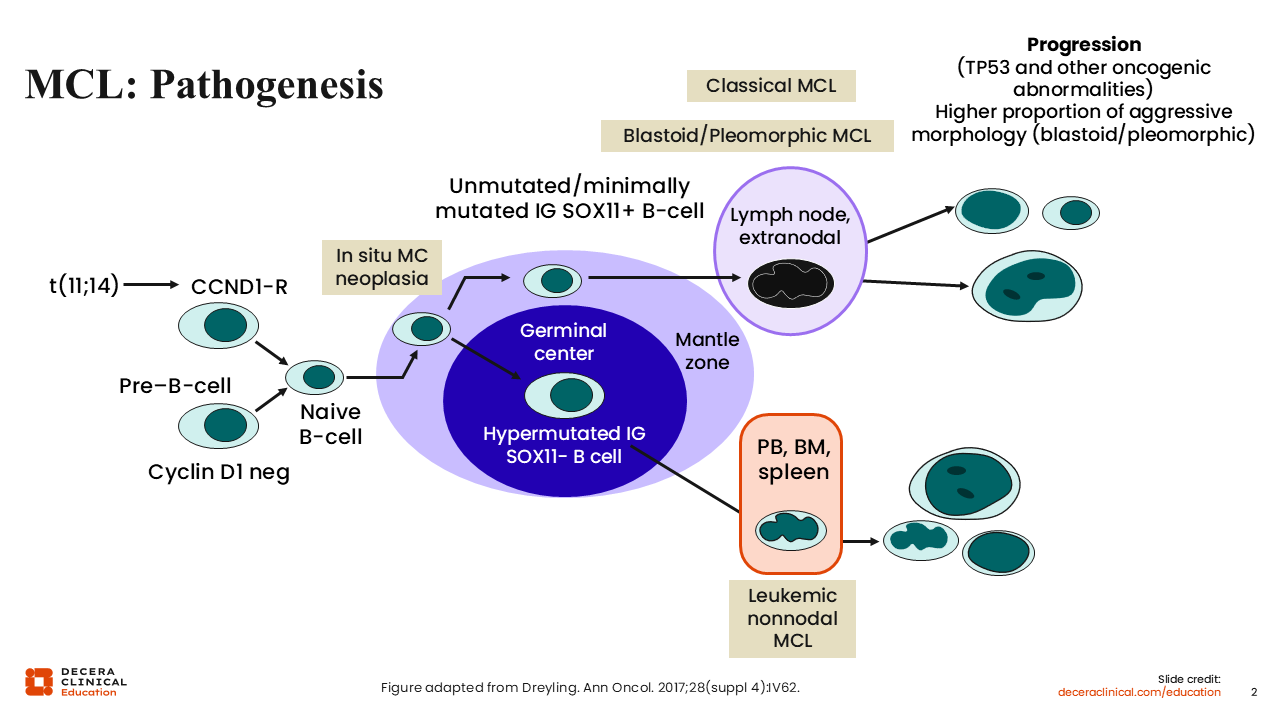
MCL: Pathogenesis
This diagram illustrates how we typically view MCL progression.8 In the ideal case, patients who have leukemic MCL are thought to have a slower clinical course than other patients with MCL.9 However, even in that patient population, we can see poor risk features such as 17p deletion or TP53 mutations. Although patients with these genetic mutations may not need immediate treatment and can have very long indolent courses, they typically have poor outcomes. In addition, during initial staging, you may see patients with classical MCL and some with aggressive features such as blastoid or pleomorphic histology. During or after disease progression, we see a higher percentage of patients with high-risk features, as these patients typically have shorter remission durations.
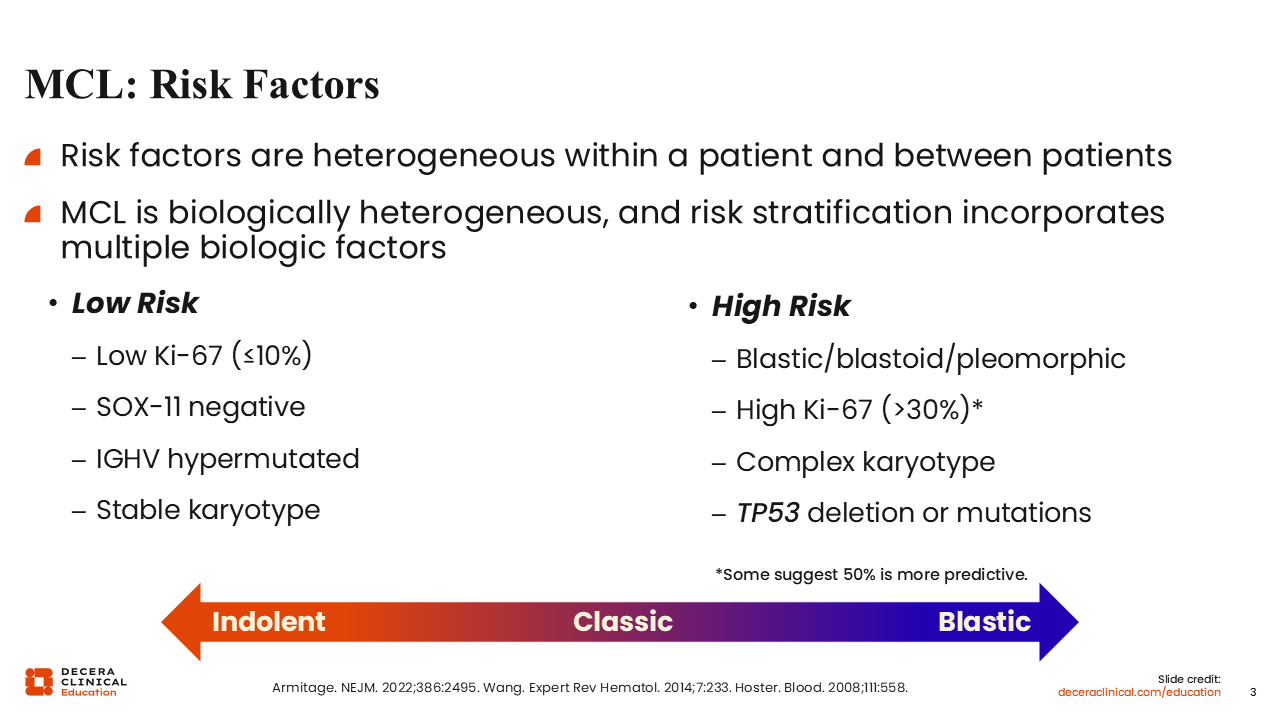
MCL: Risk Factors
Low-risk features typically include low Ki-67 and SOX11 negative as well as mutation of immunoglobulin heavy chain variability region and having a stable karyotype.1,3,10 High-risk features include high-risk blastoid and pleomorphic morphology and elevated Ki-67.11,12 The defining threshold for high Ki-67 varies from >30% to >50% or higher in this patient population. Complex karyotype is also a high-risk factor; it is the presence of at least 3 cytogenetic abnormalities in addition to (11;14) translocation.13,14 Patients with TP53 mutations, located on chromosome 17, tend to have worse outcomes than patients with a TP53 deletion. There are other mutational factors, such as NOTCH mutations, which may also lead to worse outcomes.12 However, TP53 mutations appear to be one of the most significant prognostic factors affecting DoR and OS in frontline therapy.12,15
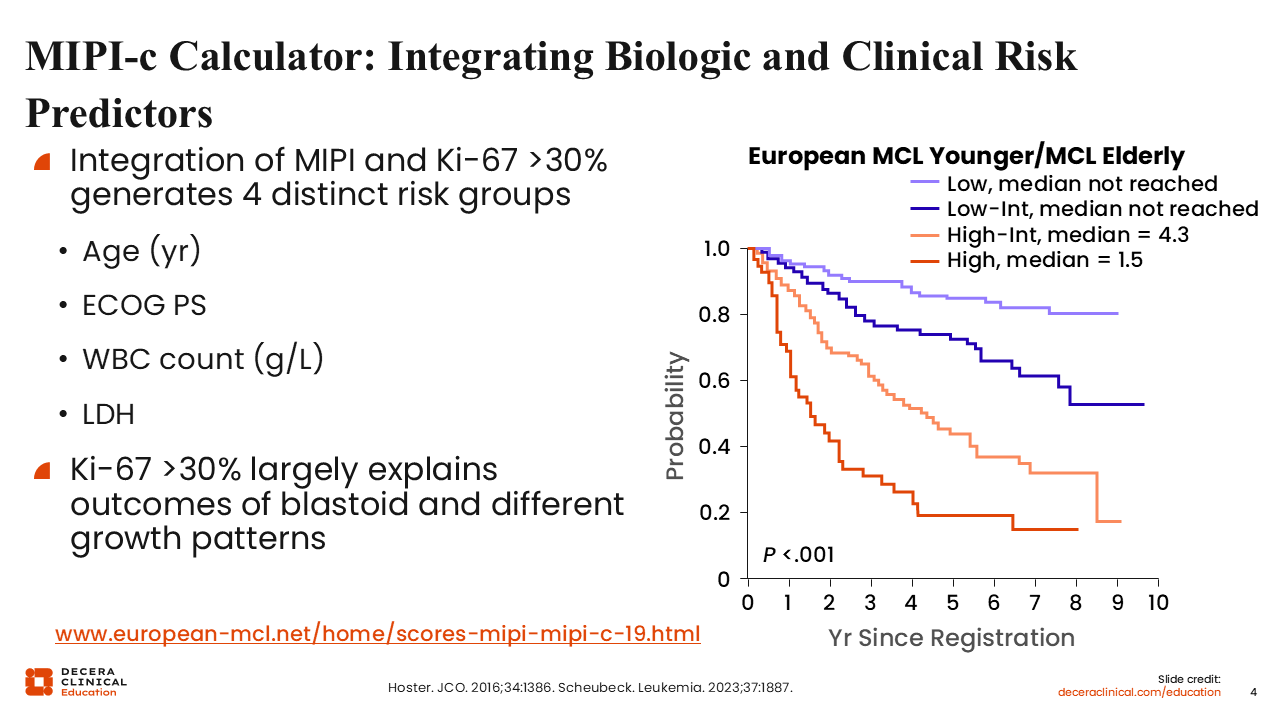
MIPI-c Calculator: Integrating Biologic and Clinical Risk Predictors
The MIPI-c score stratifies patients into 4 distinct risk groups and takes into account various risk factors such as age, performance status, white blood cell count, lactate dehydrogenase, and Ki-67.16 We see that patients with high-risk MIPI-c tend to have worse outcomes seemingly regardless of age.17 MIPI-c can be helpful to identify clinically high-risk patients.
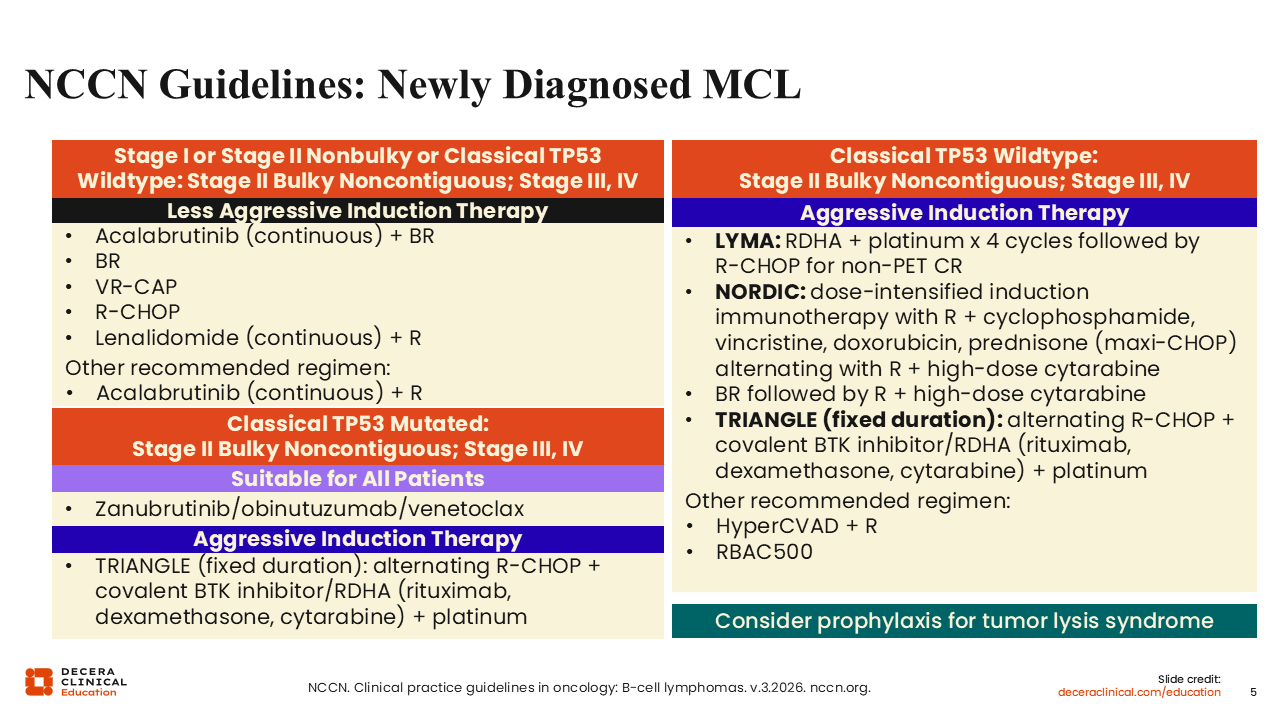
NCCN Guidelines: Newly Diagnosed MCL
The NCCN guidelines for patients with newly diagnosed MCL have recommendations for less aggressive and aggressive induction regimens.18 Many of the less aggressive options primarily use CIT, for instance, BR. VR-CAP is an option that substitutes bortezomib in for vincristine in patients treated with R-CHOP. R-CHOP itself is less preferred, with more data suggesting that it is inferior compared with bendamustine.19 In addition, continuous lenalidomide and rituximab is a nonchemotherapy option. From the ECHO trial, we have the FDA and European Medicines Agency approvals of the combination regimen of continuous acalabrutinib plus BR for adults with previously untreated MCL who are not eligible for autologous stem cell transplantation (ASCT).20-22 Other studies that have been investigating acalabrutinib with rituximab suggest a promising efficacy and safety profile with this second-generation BTK inhibitor.23
For patients with TP53 mutations, the BOVen study demonstrated the efficacy of the covalent BTK inhibitor zanubrutinib with the CD20 antibody obinutuzumab and the BCL2 inhibitor venetoclax.24
For younger, fitter patients, we can use more aggressive regimens, often alternating chemotherapy such as R-CHOP or BR with high-dose cytarabine.18 Many of these regimens have been followed by ASCT, but as we discuss later, there seems to be less and less utilization of ASCT in this patient population.
More recently, the TRIANGLE study evaluated the use of R-CHOP with the covalent BTK inhibitor ibrutinib alternated with rituximab plus dexamethasone, cytarabine, and cisplatin (R-DHAP). This fixed-duration regimen with and without ASCT consolidation was more effective with ibrutinib than without, so it has become another useful regimen.25 Given that FDA approval of ibrutinib for the treatment of MCL was withdrawn in 2023, we typically substitute one of the approved second-generation BTK inhibitors for ibrutinib in this regimen.
Other regimens are hyperCVAD with rituximab, which has some toxicity concerns, and RBAC500, which is an Italian regimen of rituximab, bendamustine, and cytarabine, typically desired for older patients.
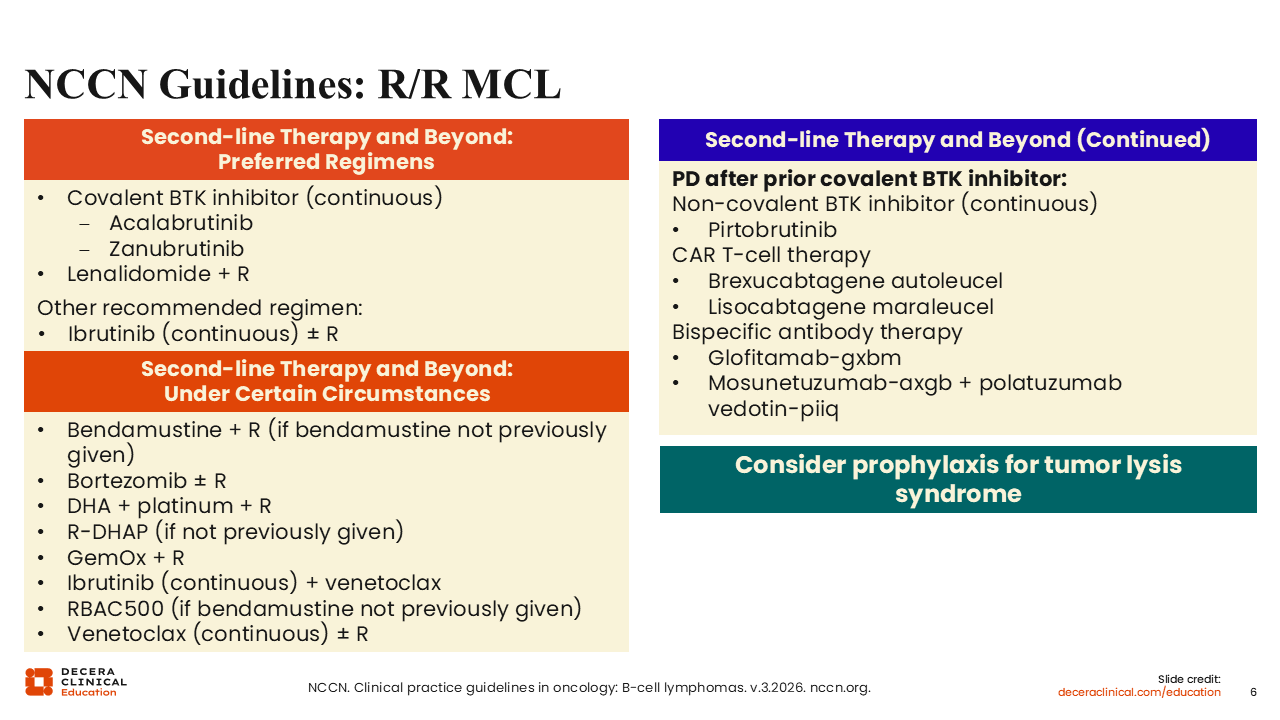
NCCN Guidelines: R/R MCL
Moving on to R/R MCL, we have the 2 second-generation BTK inhibitors, acalabrutinib and zanubrutinib.18 In my clinical practice, I have not noticed a substantial difference between these agents. We also have lenalidomide plus rituximab and other regimens that include ibrutinib and/or rituximab. Although ibrutinib is no longer approved by the FDA for MCL, it can still be used in select cases where central nervous system (CNS) involvement is a concern, as it is one of the only BTK inhibitors that we know crosses over into the CNS.26 There are some CNS data with zanubrutinib in diffuse large B-cell lymphoma, which we can extrapolate to MCL, and we have limited data for acalabrutinib regarding CNS penetration.27,28
Other options for R/R disease include CIT, but these are generally less preferred unless patients have a contraindication to or otherwise do not have access to BTK inhibitors. In addition, we have the ibrutinib and venetoclax combination from the SYMPATICO study, as well as venetoclax and rituximab.29,30 Although venetoclax after a BTK inhibitor has not been shown to be very efficacious, in BTK inhibitor–naive patients, it is a consideration based on data from the initial phase I study.30 After covalent BTK inhibitor treatment, we have the noncovalent BTK inhibitor pirtobrutinib, and, of more importance, the 2 CAR T-cell therapies brexu-cel and lisocabtagene maraleucel (liso-cel), which both have shown significant efficacy in this patient population. Finally, 2 bispecific antibody therapies—glofitamab and mosunetuzumab plus polatuzumab vedotin—are also second-line treatment options in guidelines. Both are approved as single agents for other B-cell lymphoma subtypes but not for patients with MCL.
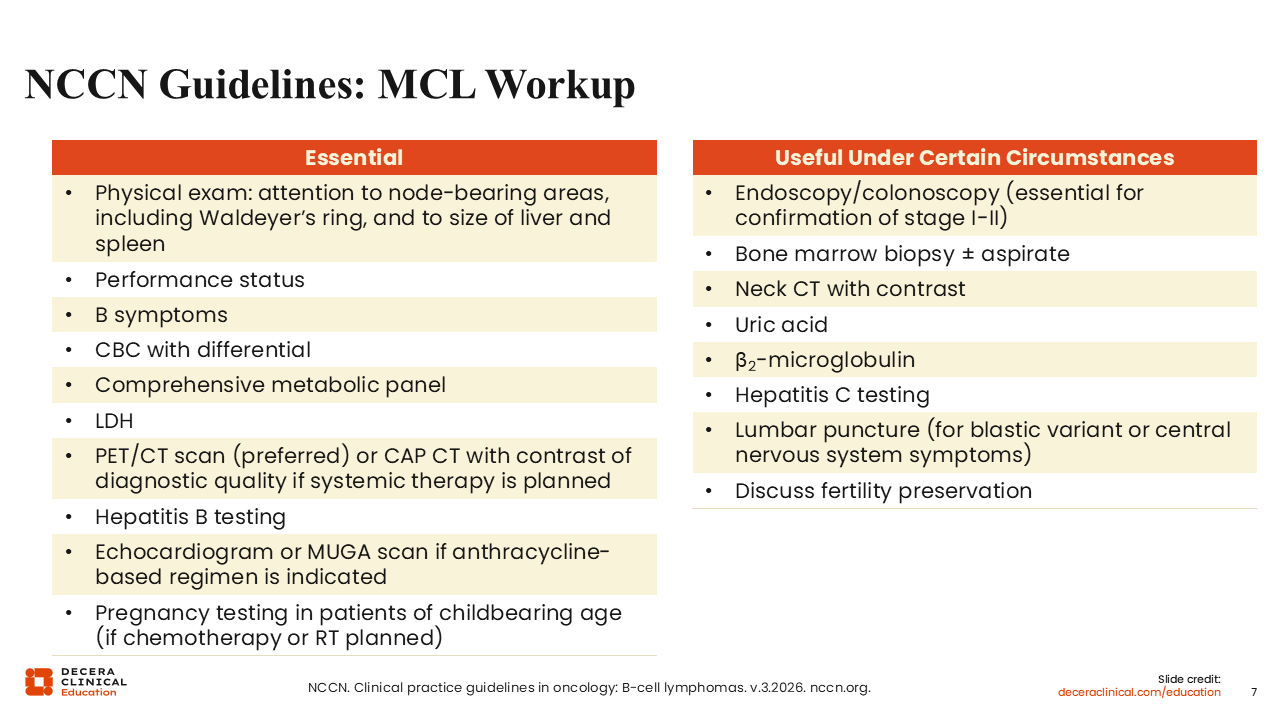
NCCN Guidelines: MCL Workup
For the MCL workup, we typically begin with a physical exam, complete blood count, comprehensive metabolic panel, and lactate dehydrogenase test.18 PET scan is generally preferred for this patient population, as well as hepatitis B testing because of the use of CD20 antibodies. Echocardiograms are not needed as much anymore, given the reduction in the use of R-CHOP, but patients do need one before using an anthracycline. Pregnancy tests are also necessary for women of childbearing potential.
In addition, endoscopy, colonoscopy, and bone marrow biopsy should be considered for complete staging, unless the patient has circulating disease because many biomarker tests can be performed using peripheral blood. Uric acid levels are usually tested at baseline to gauge the need for allopurinol to reduce uric acid. Hepatitis C testing can be considered for some patients if they are high risk. For patients with aggressive morphology or CNS disease symptoms, we can consider lumbar puncture.
MCL: Unique Clinical Features
Most patients have advanced-stage MCL with disease in the blood, bone marrow, or gastrointestinal tract.31,32 Sometimes we see an elevated lactate dehydrogenase level, especially in patients with very aggressive disease.16 Depending on the time from disease development to diagnosis, we can see a variation in the presence of symptoms, with 25% having B symptoms at diagnosis.33 Thankfully, CNS involvement is rare, but it is slightly more common in patients with R/R MCL who generally have more aggressive disease.34 Again, MCL is generally considered to be incurable, except with ASCT. However, up to 30% of patients will have indolent disease, which means they can be watched and monitored and do not require treatment or diagnosis.35
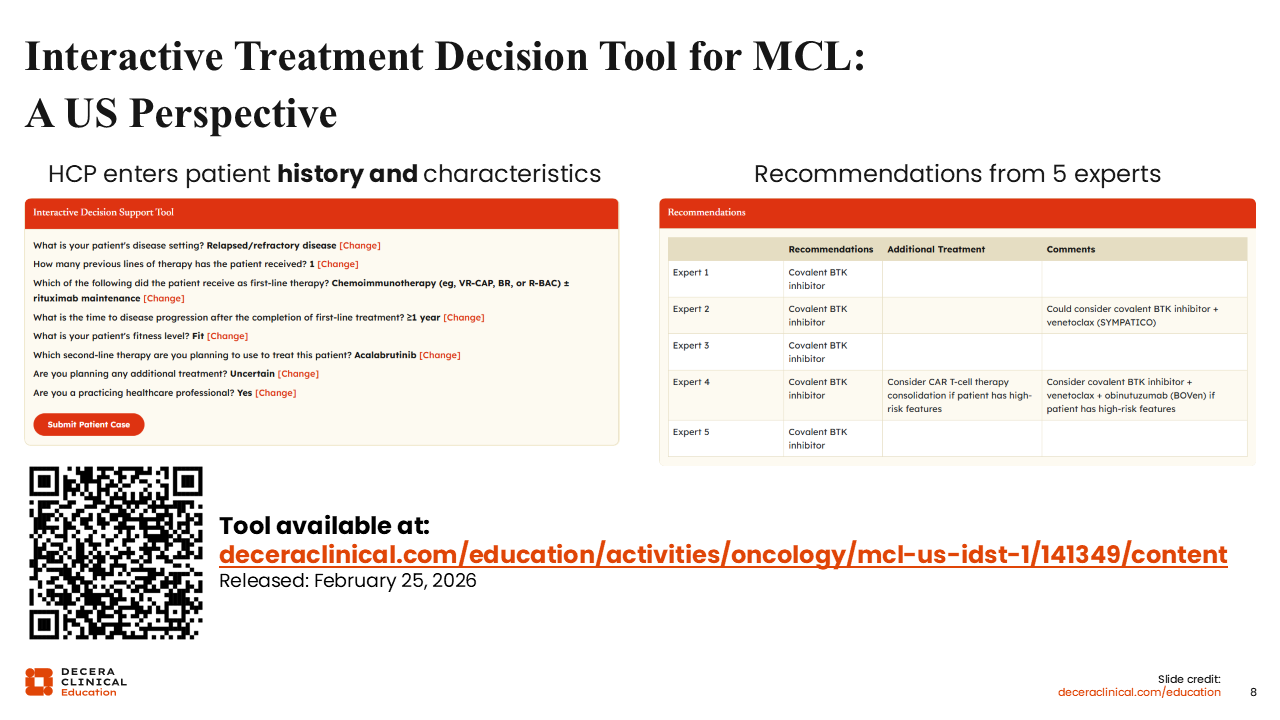
Interactive Treatment Decision Tool for MCL: A US Perspective
Decera Clinical Education has updated an interactive decision support tool to help healthcare professionals (HCPs) choose treatments for their patients with MCL. HCPs can enter the details of a patient case in the tool to view recommendations from 5 experts based on those specific presenting characteristics. Recommendations for first-line treatment consider the stage of disease and various risk factors, including del(17p)/TP53 mutation status, complex cytogenetics status, Ki-67 level, blastoid/pleiomorphic histology, and patient fitness status. Recommendations for later-line treatments consider previous therapies, time to progression after first-line therapy (when choosing second-line treatment), and patient fitness.