
CME
High Suspicion, Better Outcomes: Evaluating Thrombotic Events for Underlying ET or PV
Physicians: Maximum of 0.25 AMA PRA Category 1 Credit™
Released: May 14, 2026
Expiration: November 13, 2026

Activity
Statistics: Thrombotic Events in MPN
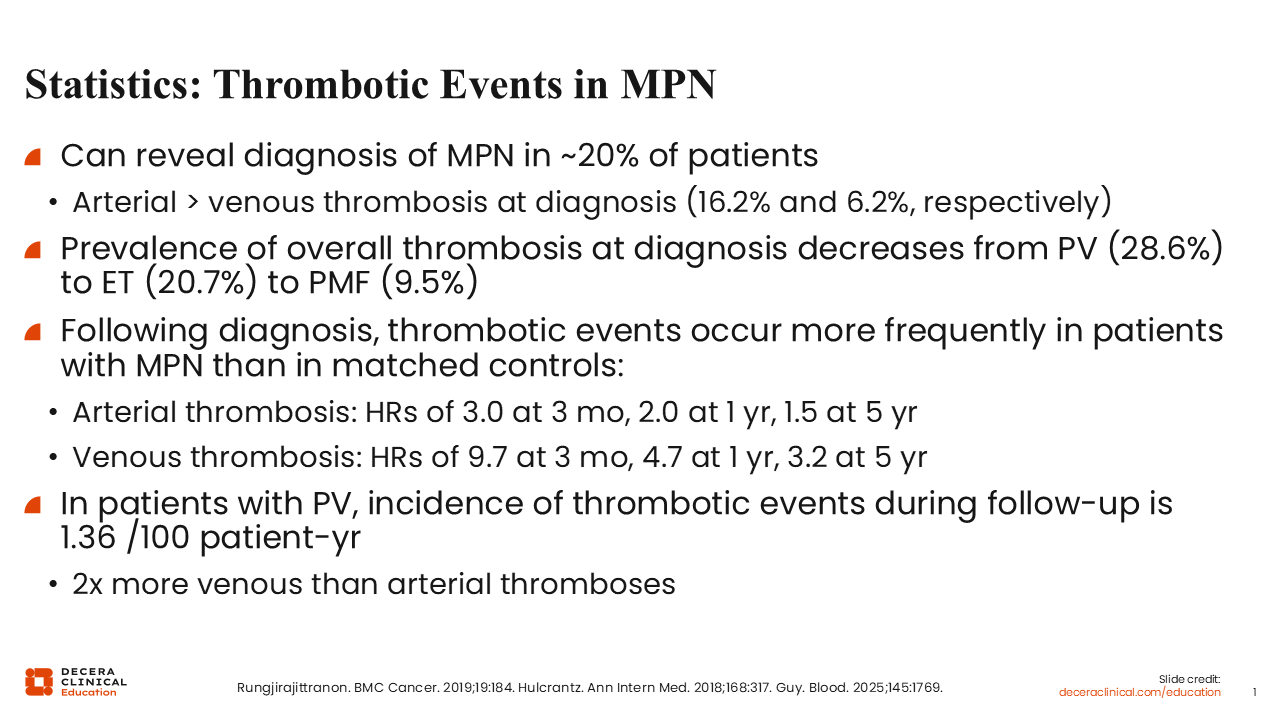
Here are some important statistics about thrombotic events in MPN.1 First, thrombotic events can reveal a diagnosis of MPNs in approximately 20% of patients.2 Patients are more likely to have an arterial thrombotic event than a venous thrombotic event at diagnosis by almost 3 to 1. The prevalence of overall thrombosis at diagnosis decreases from PV, which approaches 30%, to ET, and to primary myelofibrosis, with the lowest rate of thrombosis.
The rate of thrombotic events continues to remain high compared with the general population.3 For example, for arterial thrombosis, the HRs in patients are 3.0 at 3 months, 2.0 at 1 year, and 1.5 at 5 years. Similarly, the HRs for venous thrombosis are 9.7 at 3 months, 4.7 at 1 year, and 3.2 at 5 years. When looking specifically at PV, the incidence of thrombotic events during follow-up is 1.36/100 patient-years, and the venous thrombotic rate is higher than the arterial thrombotic rate.
Of importance, for a patient with ET or PV, these thrombotic complications are very concerning. In the day-to-day management of MPNs, the goal is to decrease the thrombotic event rate. In the long run, the goal is to decrease the chances of progression to myelofibrosis or acute leukemia.
Pathogenesis of Thrombosis in MPNs
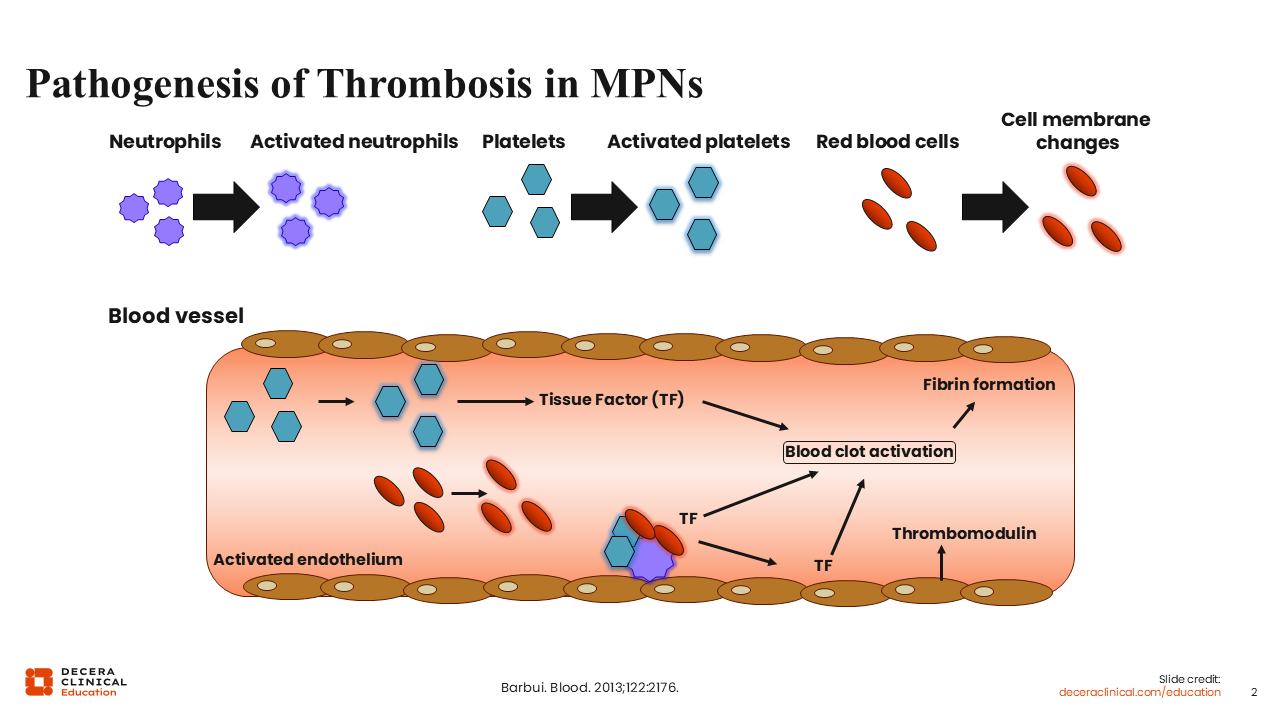
First, pathogenesis of thrombosis in MPNs is multifactorial and complex owing to numerous factors. These include age, prior history of any thrombotic event, other inflammatory conditions, and cardiovascular factors like obesity, hypertension, and hyperlipidemia. External issues like tobacco smoking also increase the chances of thrombotic events. Additional contributing factors include increased blood counts across the 3 lineages: white blood cells, red blood cells, and platelets. It is important to note that the increased risk is attributed to not only quantitative but also qualitative changes in these cells, which lead to a procoagulant state in the blood vessels.
Some prothrombotic features include increased expression of procoagulant and proteolytic enzymes by blood cells; release of inflammatory cytokines by blood cells, especially white blood cells; and expression of adhesion molecules. In response to inflammatory cytokines, hyperviscosity, and leukocyte-derived proteases, prothrombotic changes occur in the normal endothelium. In particular, the upregulation of endothelial adhesion receptors, which favors the attachment of platelets, red blood cells, and white blood cells to the vascular endothelium, leads to localization of clotting reactions and fibrin deposition.4
Finally, both in vitro and in vivo experiments suggest that JAK2 V617F–mutated cells are found in the vascular endothelium and not restricted to the hematopoietic lineage.5-7
Effect of Elevated Hematocrit in PV/ET
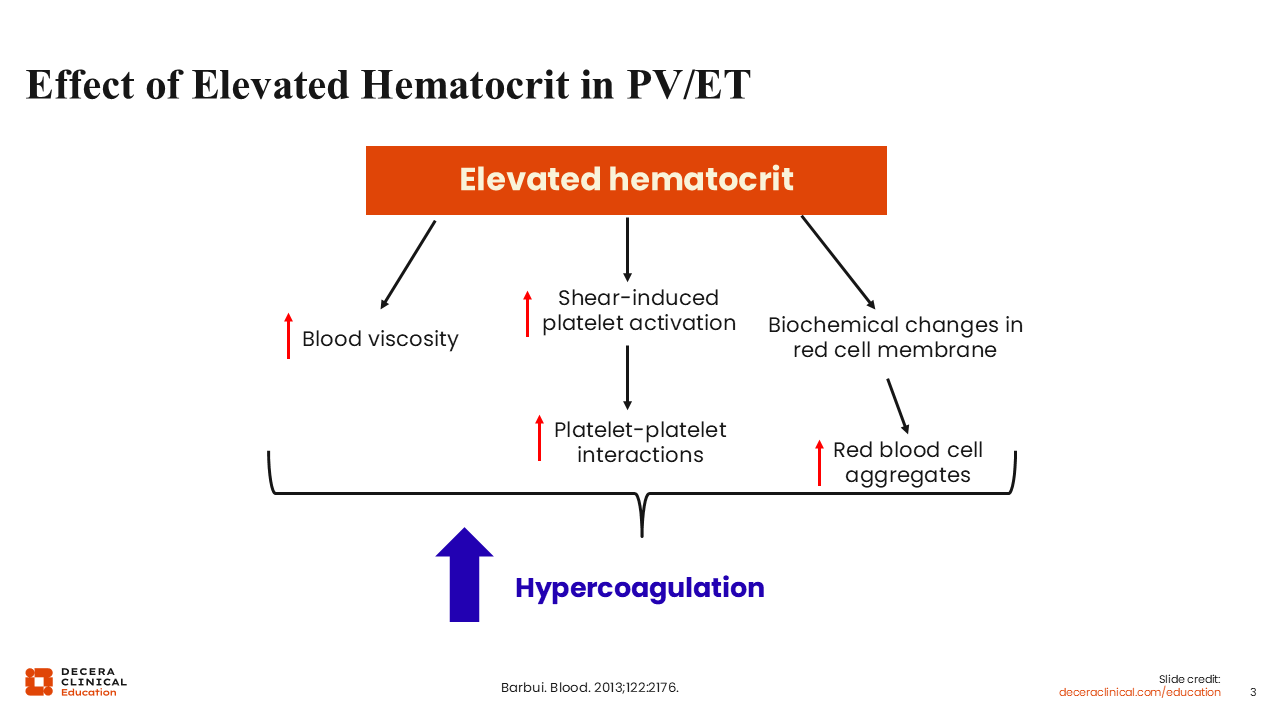
In addition to the factors previously described, an elevated hematocrit, one of the key and defining features of PV, also increases thrombotic risk via several different mechanisms.
One is through increased blood viscosity. The second is through high shear stress that occurs because red blood cells displace platelets toward the vessel wall, which leads to shear-induced platelet activation and enhances platelet–platelet interactions, thus cascading down the blood clot pathway. Even under low shear rates, as in the venous bed, hyperviscosity can increase thrombotic risk by causing major disturbances to blood flow. Finally, biochemical changes in the cell membrane and the intracellular content of red blood cells can increase thrombotic risk.4
Predictive Scores for Thrombosis in MPN
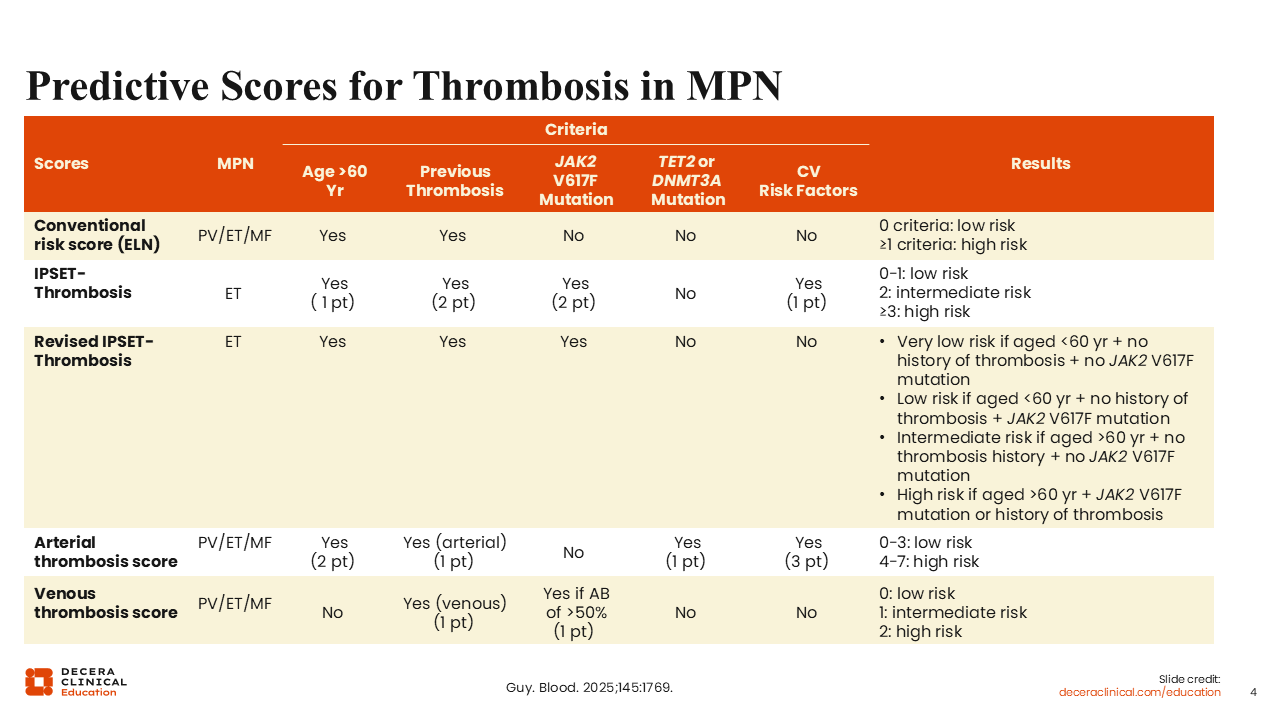
The risk scoring systems typically used for MPNs are shown in the table; I will focus on the first 3. The conventional risk score (European LeukemiaNet) is used for PV and takes into account 2 factors: age older than 60 years and history of thrombotic events. If patients have either of these attributes, they have high-risk PV.
For ET, the International Prognosis Score in Essential Thrombocythemia (IPSET)-thrombosis score, which takes into account 4 risk factors, and the revised IPSET-thrombosis score, which takes into account 3 factors (ie, age older than 60 years, prior history of thrombosis, and the presence or absence of JAK2 V617F mutation), are used. The presence or absence of JAK2 V617F mutation is important because patients with ET or myelofibrosis who lack this mutation have only a moderate risk of thrombosis. By the revised IPSET-thrombosis score, there are 4 risk categories of ET: very low risk, low risk, intermediate risk, and high risk.1
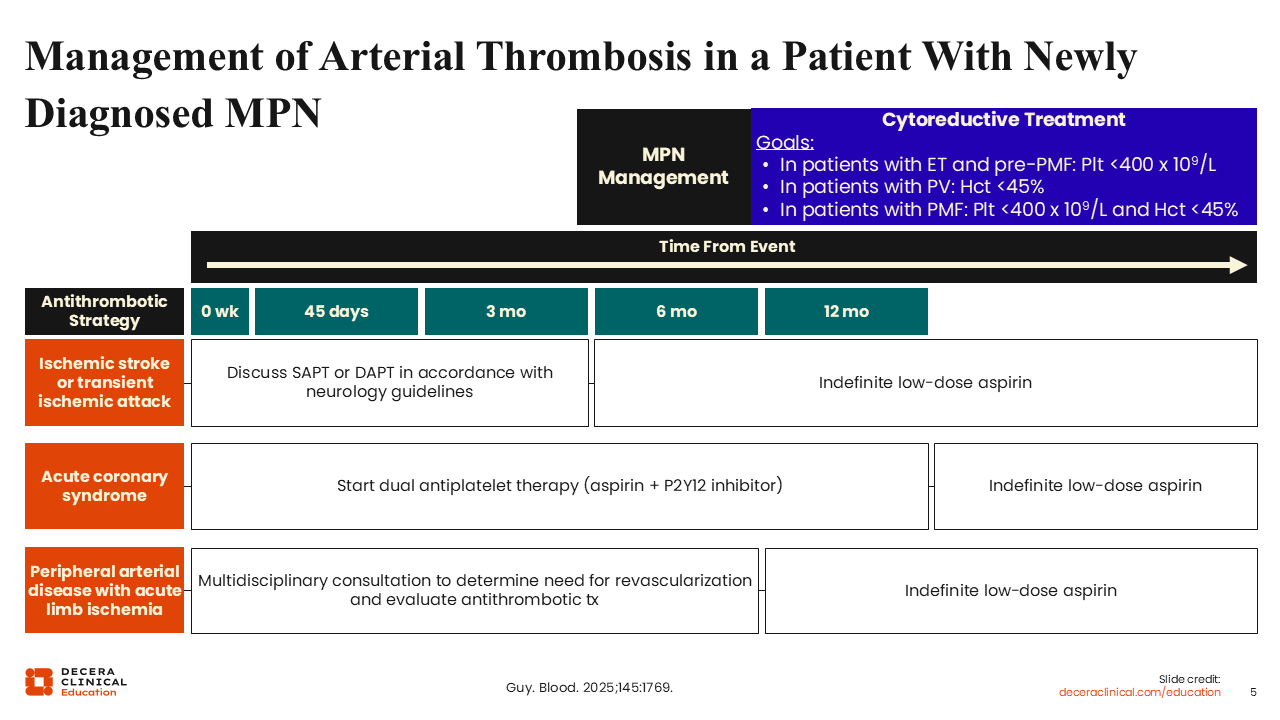
Management of Arterial Thrombosis in a Patient With Newly Diagnosed MPN
If there were a thrombotic event, how should healthcare professionals (HCPs) manage these episodes? First, I will review the management of arterial thrombotic events in a patient with newly diagnosed MPN. This patient presented with an arterial thrombotic event and was diagnosed with MPN shortly thereafter.1 Such a patient would be considered high risk for additional thrombotic events. I would initiate cytoreductive therapy with the goal of reducing and maintaining blood counts.
In PV, the focus is on a hematocrit <45%. In ET, the goal is a platelet count <400 x 109/L. HCPs are increasingly recognizing the role of increased white blood cell count and higher chances of thrombotic events, so another goal is a white blood cell count less than 11 to 12 x 109/L.8
Anticoagulant management depends on the kind of arterial thrombotic event (ie, ischemic stroke or transient ischemic attack). These events are serious, and neurology consults should be done to discuss single vs dual antiplatelet therapy for the first few months, followed by indefinite low-dose aspirin therapy. For acute coronary syndrome, consultation with cardiology is critical. Dual antiplatelet therapy may be needed for up to 1 year, followed by indefinite low-dose aspirin.
On the other hand, for peripheral arterial disease, especially with acute limb ischemia, vascular specialist colleagues should be consulted. In these patients, revascularization attempts in conjunction with interventional radiology can be considered. After the initial event, low-dose aspirin, unless there is an absolute contraindication, would be recommended indefinitely.
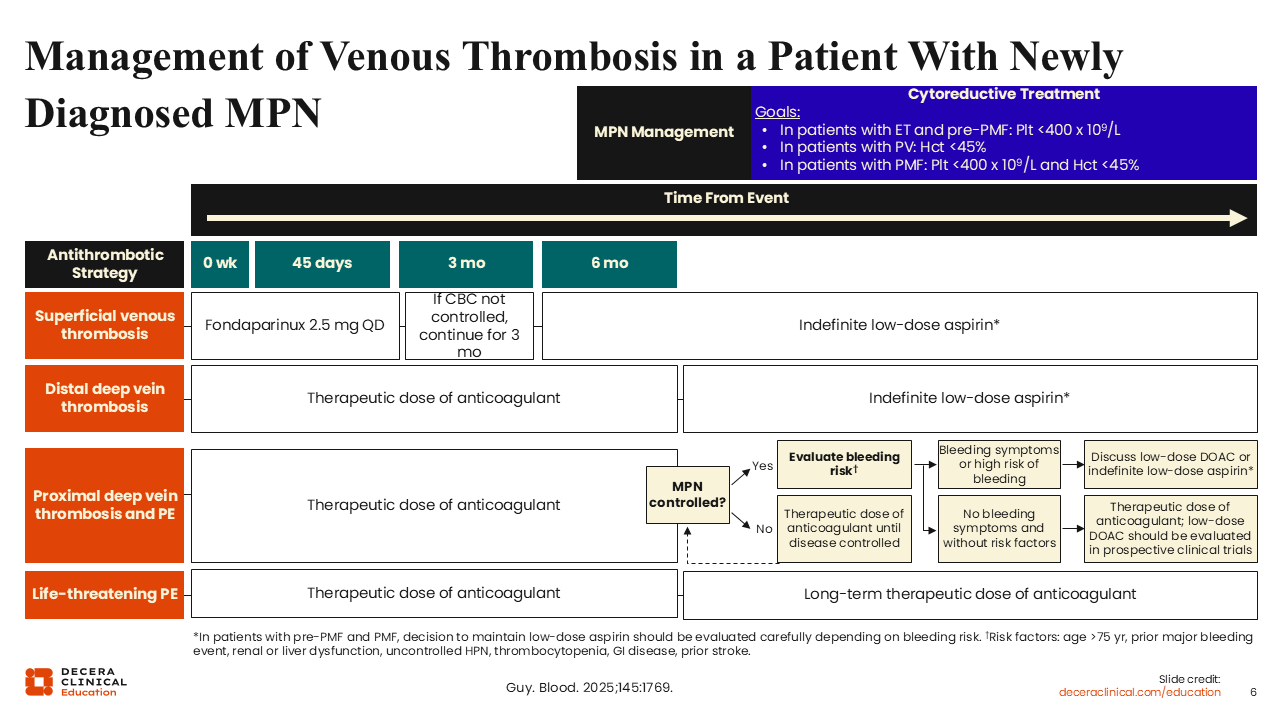
Management of Venous Thrombosis in a Patient With Newly Diagnosed MPN
Venous thrombotic events are more common after diagnosis, as previously noted. If a patient presents with a venous thrombotic event in the newly diagnosed MPN setting, much like with arterial thrombosis, cytoreductive therapy should be initiated.1 This patient would be considered high risk for future thrombotic events, and the hematologic parameter goals are the same.
For superficial venous thrombotic events, low-dose fondaparinux (2.5 mg/day) could be considered for a few months, followed by indefinite low-dose aspirin.
In the event of DVT, HCPs should distinguish between proximal and distal DVT because distal DVT is at a lower likelihood for progressing to PE, whereas proximal DVT is at a much higher risk. For distal DVT, management involves a therapeutic dose of anticoagulant for between 3 and 6 months, followed by indefinite low-dose aspirin.
In the event of proximal DVT and PE, management depends on severity. Whether the MPN was controlled at the time of the event plays a major role. For life-threatening PE, a long-term therapeutic dose (ie, indefinite) of anticoagulant is recommended. Generally speaking, the use of aspirin and a low-dose direct oral anticoagulant together is not recommended. However, this combination is not well studied, so the decision to maintain low-dose aspirin should be evaluated based on bleeding risk.
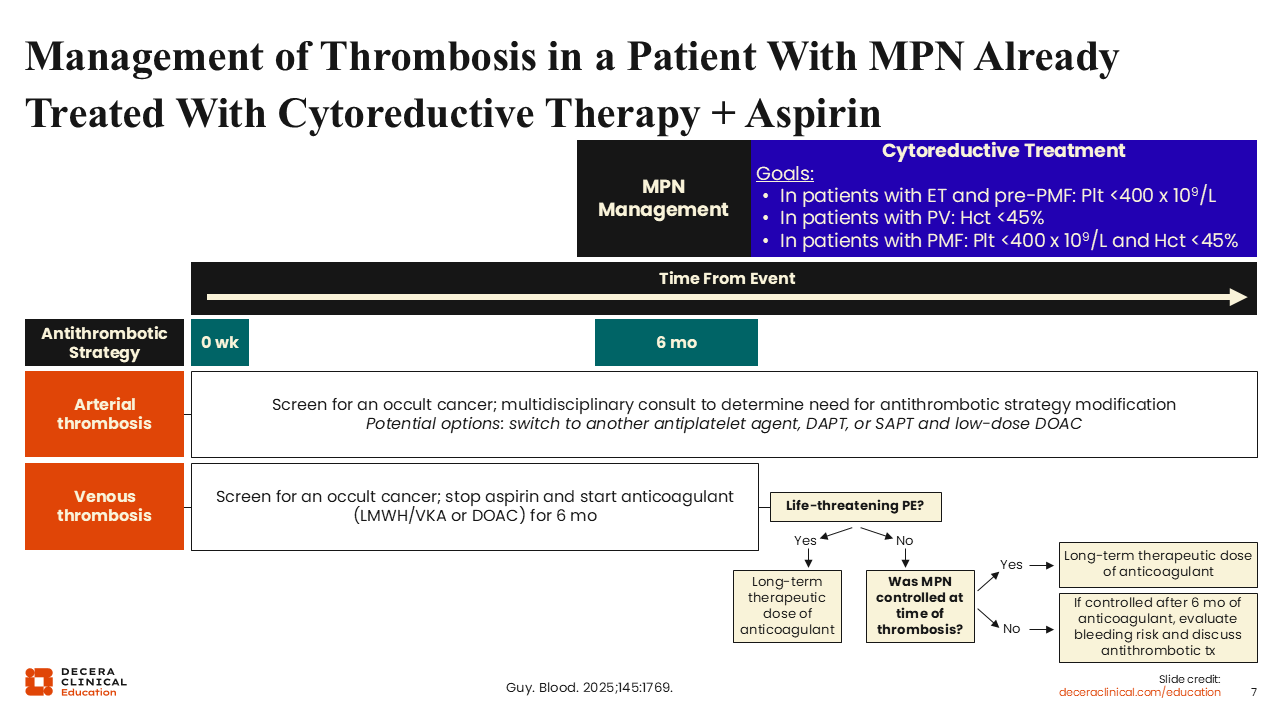
Management of Thrombosis in a Patient With MPN Already Treated With Cytoreductive Therapy Plus Aspirin
What about the management of thrombosis in a patient who had a thrombotic event while receiving cytoreductive therapy and aspirin? First, assess adherence to cytoreductive therapy and whether ideal goals were achieved while receiving cytoreductive therapy.1 Second, examine whether additional factors may have contributed to the thrombotic event. Such factors include occult cancer and/or other notable reversible risk factors that may have played a role, for example, a recent surgery or long-distance travel without good ambulation.
In the event of an arterial thrombotic event, a switch to a different antiplatelet agent could be considered. For a venous thrombotic event, one could consider stopping aspirin and treating the venous thrombotic event with an anticoagulant for a few months. Management beyond that depends on whether the thrombotic event was life-threatening and/or how well the MPN was controlled at the time of the event.
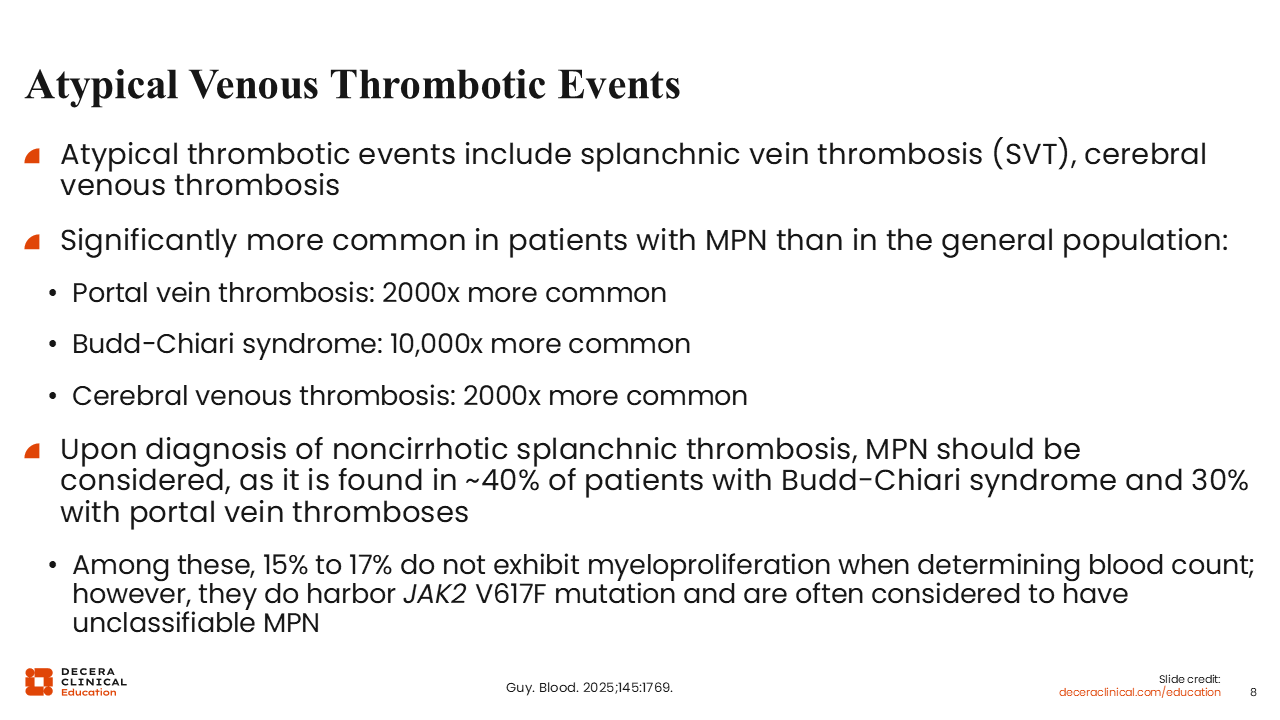
Atypical Venous Thrombotic Events
An important point here concerns atypical or unusual venous thrombotic events.1 HCPs are taught to recognize and pay close attention to these. In the event of MPNs, 2 in particular should be recognized: splanchnic vein thrombosis or mesenteric vein thrombosis and cerebral vein thrombosis. These are not just any venous thrombotic events; these are potentially life-threatening. They are found more commonly in patients with MPNs than in the general population. If a patient is diagnosed with noncirrhotic splanchnic vein thrombosis, MPN should be strongly considered because it is found in nearly 40% of patients with Budd-Chiari syndrome and in 30% of those with portal venous thrombosis.
Note that some patients who experience thrombotic events may harbor a JAK2 mutation, but if a bone marrow biopsy or blood counts do not indicate definitive MPN, these patients are often diagnosed with MPN-unclassifiable. Again, the important point is that when a patient presents with an atypical or unusual thrombotic event, HCPs should screen for MPNs.
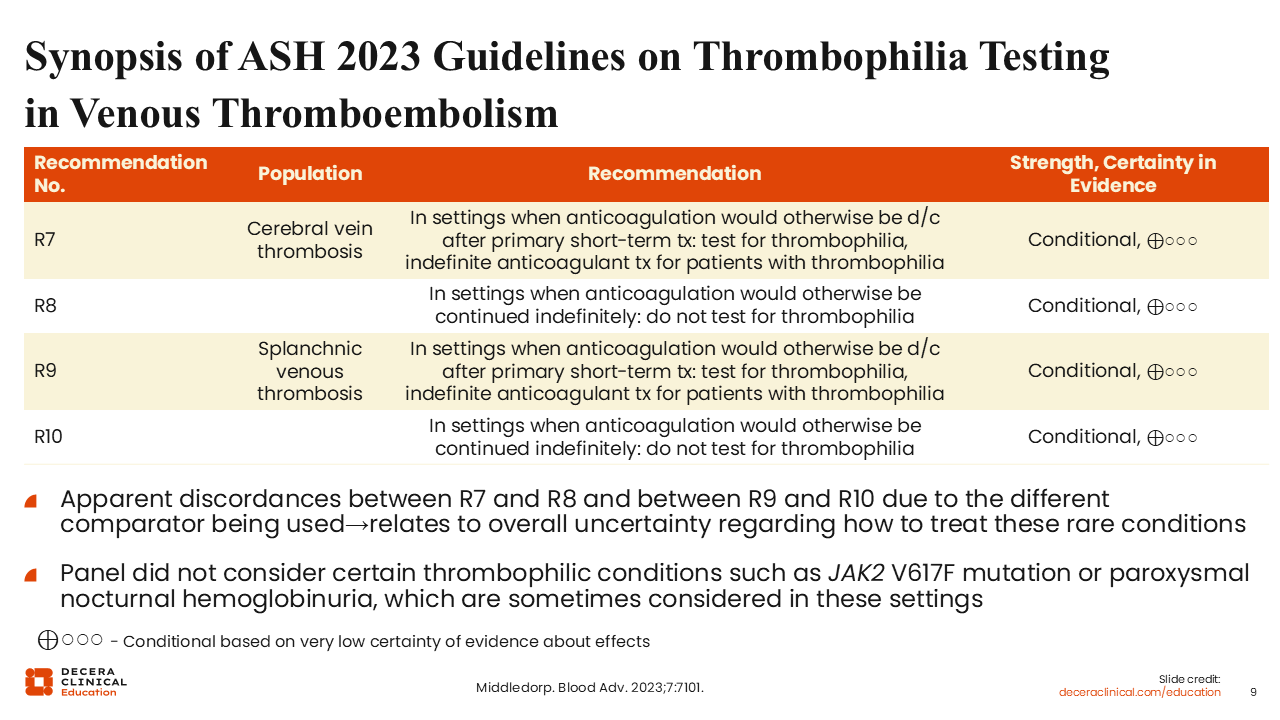
Synopsis of ASH 2023 Guidelines on Thrombophilia Testing in Venous Thromboembolism
In 2023, the American Society of Hematology (ASH) published guidelines on thrombophilia testing in venous thromboembolic events.9 There are 4 recommendations concerning testing and treatment for cerebral vein thrombosis and splanchnic vein thrombosis.
Of importance, the ASH 2023 guidelines did not consider some causes of thrombotic events like thrombophilic conditions such as a JAK2 V617F mutation or paroxysmal nocturnal hemoglobinuria. These recommendations are more relevant to common familial or hereditary thrombophilic events. Therefore, although guidelines are available, the presence of cerebral vein thrombosis and splanchnic vein thrombosis events should be considered significant and worthy of indefinite anticoagulation.
Conclusions
In summary, the goal of day-to-day management of MPNs is designed to reduce the risk of thrombosis, particularly in PV and ET, where thrombotic events occur at a higher rate than in the general population. Nearly 1 in 5 patients newly diagnosed with MPN have already experienced a thrombotic event at or prior to their diagnosis. Rare thromboses, such as splanchnic vein thrombosis and cerebral vein thrombosis, should trigger a high level of suspicion of an MPN as the root cause. Cytoreductive therapy is the key to risk management in MPNs, along with aspirin or anticoagulants, as indicated in patients who experience thrombotic events.