CME
Foundations of ADC Therapy and the Clinical Rationale for Targeting TROP-2 in TNBC
Physicians: Maximum of 0.25 AMA PRA Category 1 Credit™
Released: July 10, 2026
Expiration: January 09, 2027
Activity
Why the TNBC Paradigm Is Shifting
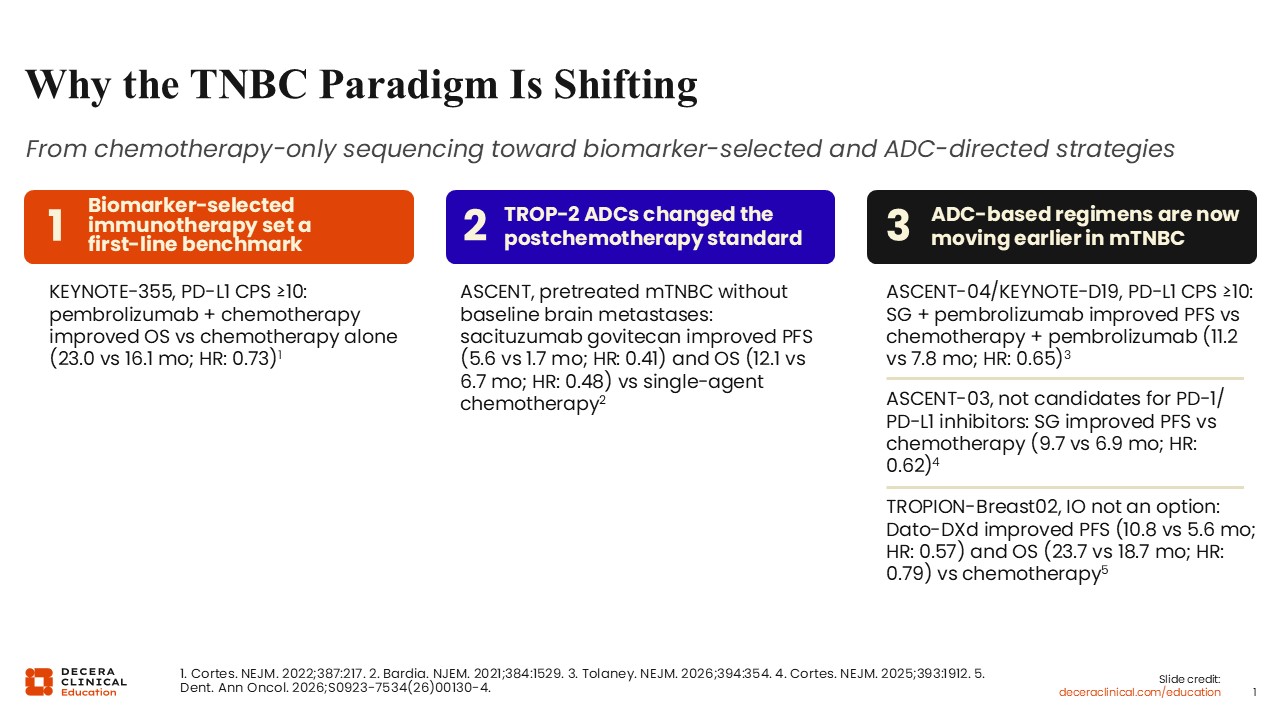
For several decades, chemotherapy has been the mainstay of treatment for metastatic TNBC. This treatment paradigm is now shifting with the integration of biomarker-selected immunotherapy and TROP-2–directed ADCs.
The first inflection point was the integration of immune checkpoint inhibition into TNBC care. In the phase III KEYNOTE-355 trial, adding the PD-1 inhibitor pembrolizumab to chemotherapy improved both progression-free survival (PFS) and overall survival (OS) vs chemotherapy alone in patients with PD-L1–positive (combined positive score [CPS] ≥10) metastatic TNBC (median OS: 23.0 vs 16.1 months; HR: 0.73), establishing a first-line standard of care in a biomarker-selected population.1
The first ADCs approved in metastatic TNBC was sacituzumab govitecan, a TROP-2–directed ADC, for pretreated disease based on the phase III ASCENT trial. In patients without baseline brain metastases, sacituzumab govitecan significantly improved median PFS (5.6 vs 1.7 months; HR: 0.41) and OS (12.1 vs 6.7 months; HR: 0.48) vs single-agent chemotherapy of the physician’s choice.2
More recently, TROP-2–directed ADC–based strategies have moved into the first-line setting, with 3 randomized phase III trials demonstrating improvements vs standard chemotherapy-based regimens. The ASCENT-04/KEYNOTE-D19 trial compared sacituzumab govitecan plus pembrolizumab with the KEYNOTE-355 approach of chemotherapy plus pembrolizumab and showed an improved median PFS with the ADC-containing regimen in PD-L1 CPS ≥10 tumors (11.2 vs 7.8 months; HR: 0.65).3 In patients who are not candidates for PD-1/PD-L1 inhibitors, the ASCENT-03 trial showed that sacituzumab govitecan monotherapy improved median PFS vs single-agent chemotherapy (9.7 vs 6.9 months; HR: 0.62).4 TROPION-Breast02 showed that datopotamab deruxtecan monotherapy improved both median PFS (10.8 vs 5.6 months; HR: 0.57) and OS (23.7 vs 18.7 months; HR: 0.79) vs single-agent chemotherapy.5 On the basis of these data, the FDA approved datopotamab deruxtecan in May 2026 and sacituzumab govitecan in June 2026 for first-line treatment of metastatic TNBC.
What Are Antibody–Drug Conjugates?
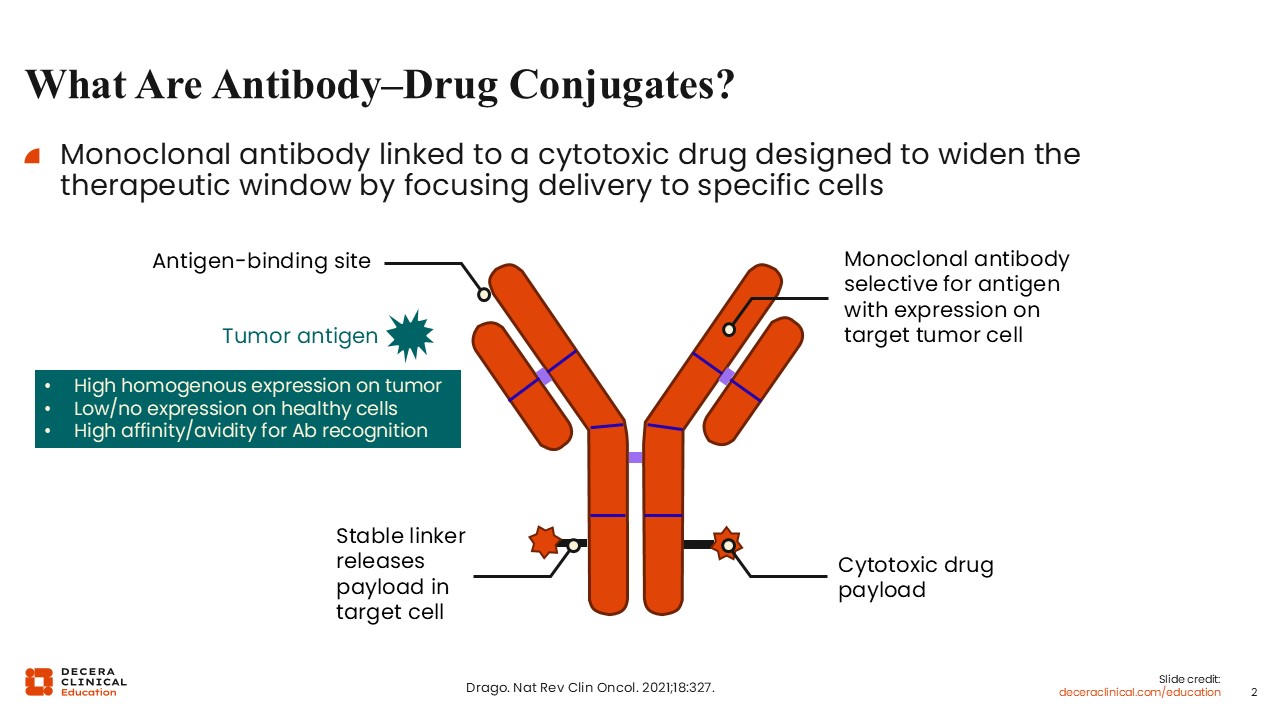
ADCs are monoclonal antibodies linked to a cytotoxic chemotherapy payload, designed to widen the therapeutic window by focusing the delivery of the chemotherapy to specific cells.
There are 3 key components to an ADC. One is the monoclonal antibody that binds to a specific target expressed, for example, on the surface of tumor cells. A second is the highly potent cytotoxic chemotherapy known as the payload that is carried by the antibody. The third component is the linker that attaches the chemotherapy to the monoclonal antibody. The linker is generally stable in plasma, with most of the payload being released upon internalization of the ADCs within the target cell.6
TROP-2
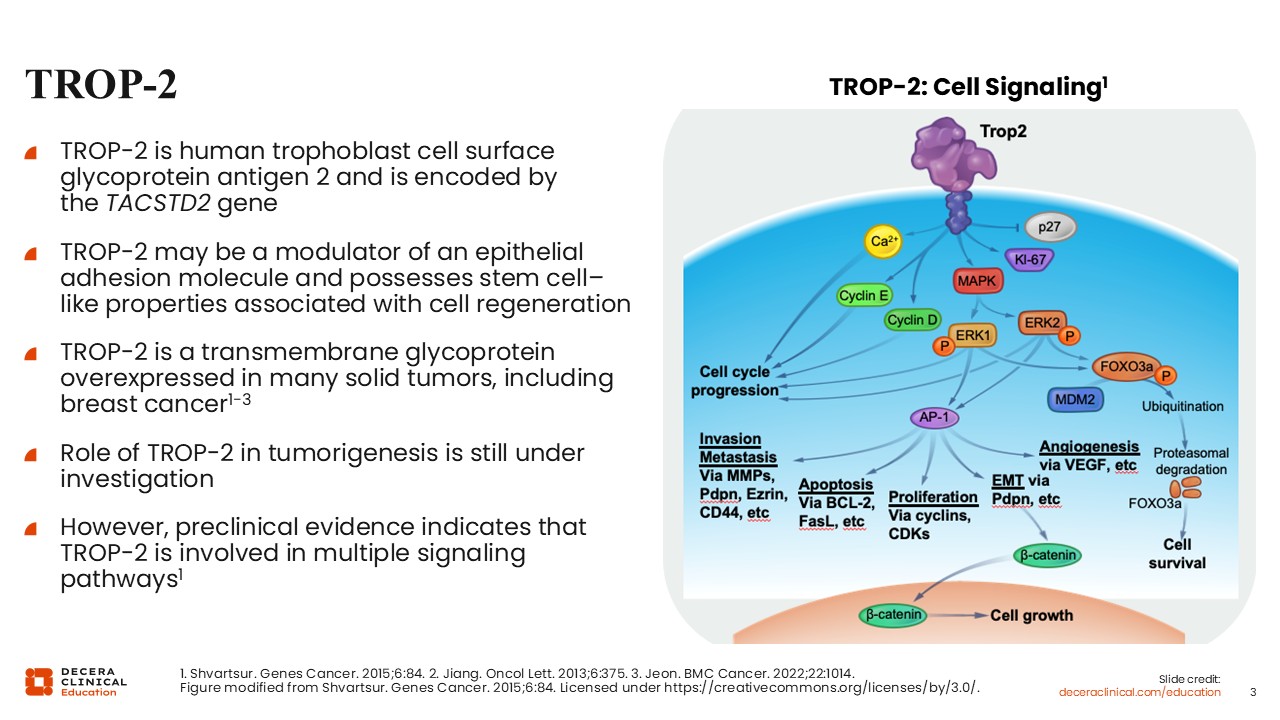
TROP-2 is a transmembrane glycoprotein that is overexpressed in many solid tumors, including breast cancer. The role of TROP-2 in tumorigenesis remains under investigation, but it may be a modulator of an epithelial adhesion molecule and possesses stem cell–like properties associated with cell regeneration. Preclinical evidence indicates that TROP-2 participates in multiple signaling pathways linked to cell proliferation, cell invasion, epithelial-mesenchymal transition, and metastatic behavior.7,8
TROP-2 Expression in Metastatic Breast Cancer
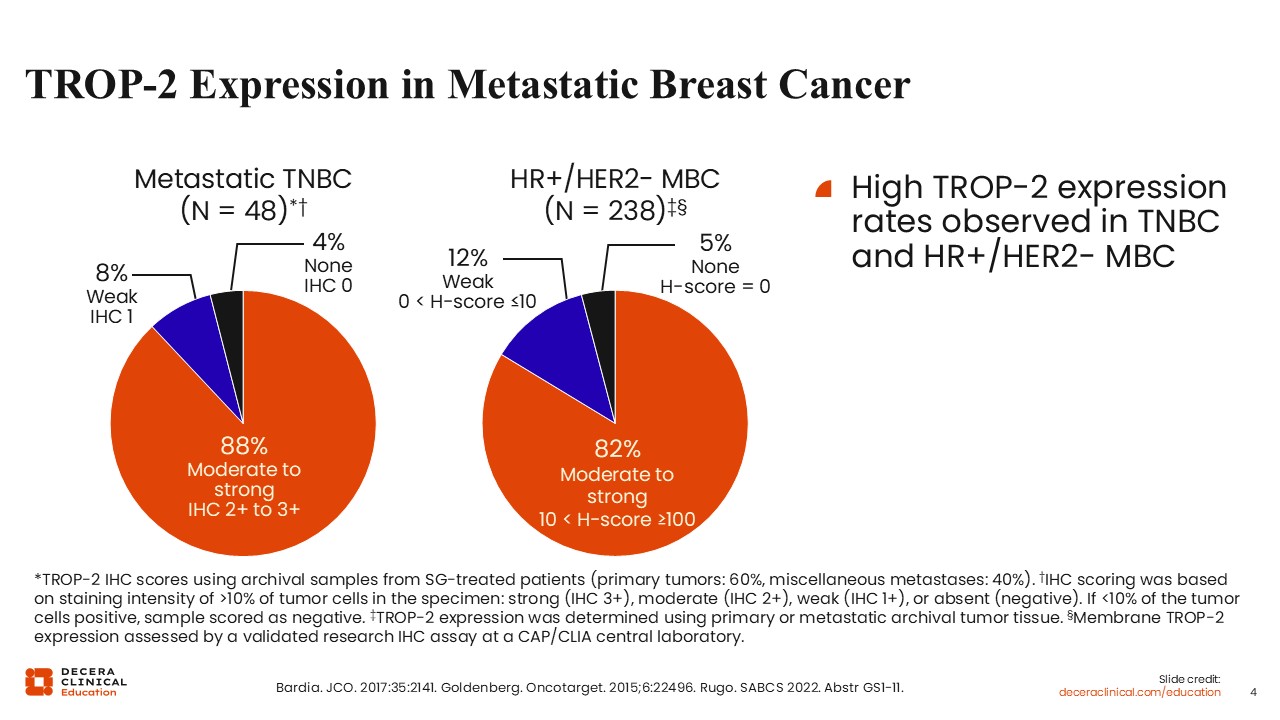
TROP-2 is highly expressed across breast cancer subtypes. In an analysis of metastatic TNBC using archival tumor samples, 88% exhibited moderate to strong TROP-2 expression by IHC.9 For context, in hormone receptor–positive/HER2-negative metastatic breast cancer, approximately 82% of tumors show moderate to strong TROP-2 expression.10 Expression can vary by assay, sample type, and scoring method, so these figures should be interpreted as supporting target prevalence rather than as a treatment threshold.
Why TROP-2 Matters Clinically in TNBC
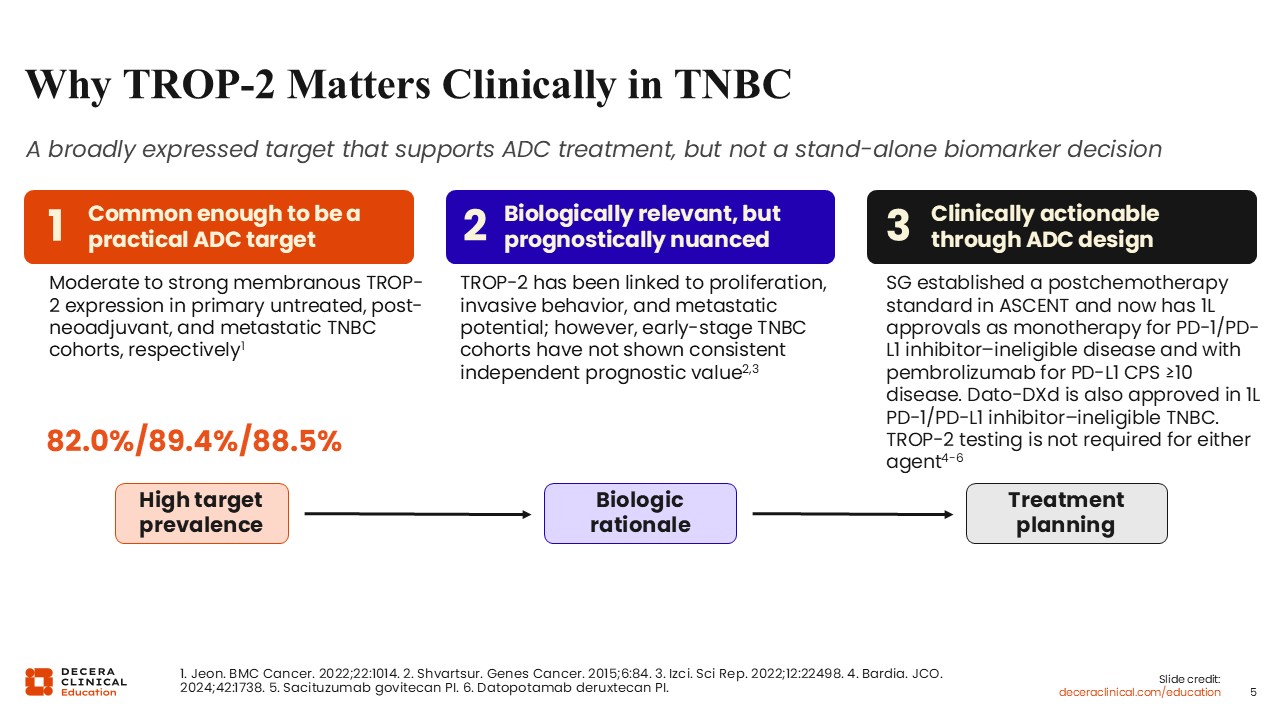
TROP-2 matters clinically in TNBC for several reasons. First, it is common enough to be a practical ADC target. Most TNBCs have moderate to strong membranous TROP-2 expression across disease stages: primary untreated TNBC, tumor samples postneoadjuvant therapy if there is residual disease, and at the time of recurrence in metastatic TNBC. TROP-2 expression tends to be relatively constant over time at these different disease stages (82.0%, 89.4%, and 88.5%, respectively).8
Second, TROP-2 is biologically relevant but prognostically nuanced. It has been linked to cell proliferation, invasive behavior, and metastatic potential, although the precise prognostic value of TROP-2 expression remains unclear.8,11
Third, TROP-2 is clinically actionable through ADCs design. Two TROP-2–directed ADCs are now approved by the FDA in TNBC, and additional approvals or expanded indications may follow.
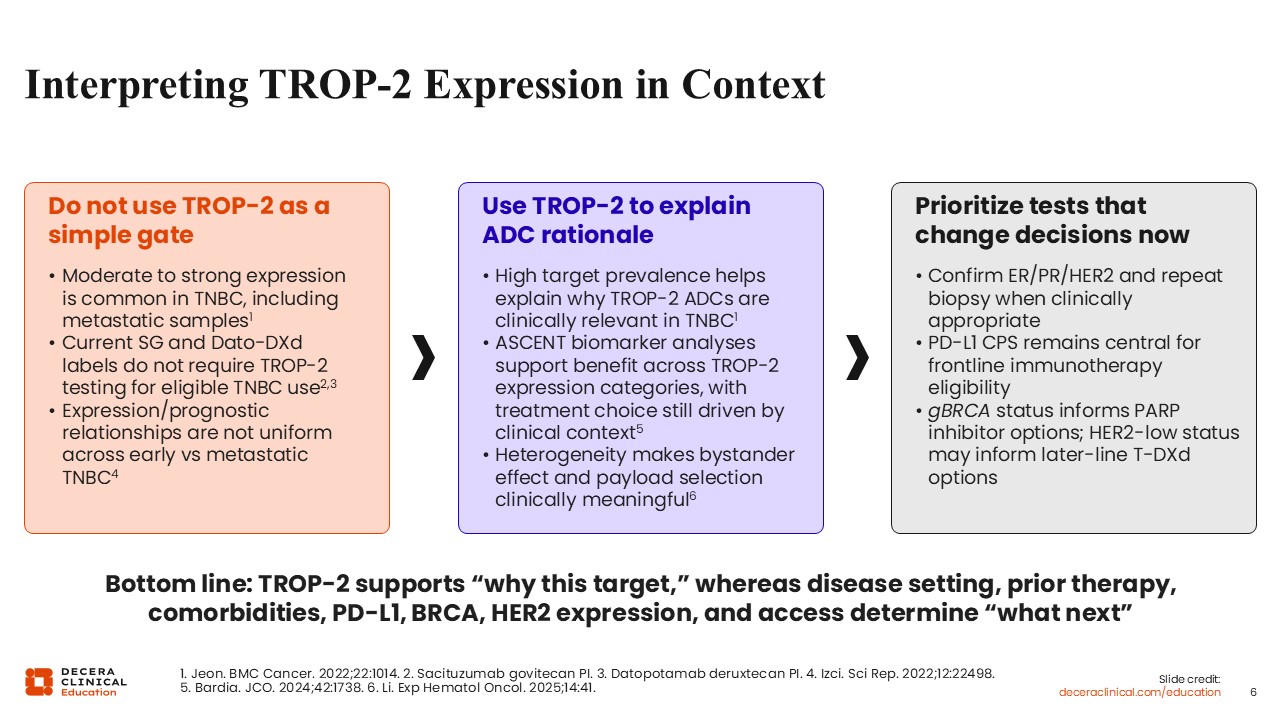
Interpreting TROP-2 Expression in Context
Although moderate to strong expression is common, the current prescribing information for sacituzumab govitecan and datopotamab deruxtecan does not require TROP-2 testing to identify candidates for these therapies. This is because randomized trials of TROP-2–directed ADCs have shown clinical benefit across a range of TROP-2 expression levels; patients with higher expression may derive a greater magnitude of benefit, but even those with lower expression appear to benefit more from the ADC than from standard chemotherapy.12
Therefore, when a patient is first diagnosed with recurrent or metastatic TNBC, testing should prioritize results that change management now: confirmation of estrogen receptor, progesterone receptor, and HER2 status; PD-L1 CPS to inform first-line immunotherapy-based approaches; and germline BRCA1/2 testing to identify candidates for approved PARP inhibitor therapy. HER2-low status may inform later-line HER2-directed ADC options. Germline PALB2 status may inform hereditary risk assessment, clinical trial eligibility, or individualized treatment discussions, but it is not an FDA-labeled criterion for PARP inhibitor selection in breast cancer.13,14
TROP-2‒Directed ADCs: Sacituzumab Govitecan and Datopotamab Deruxtecan
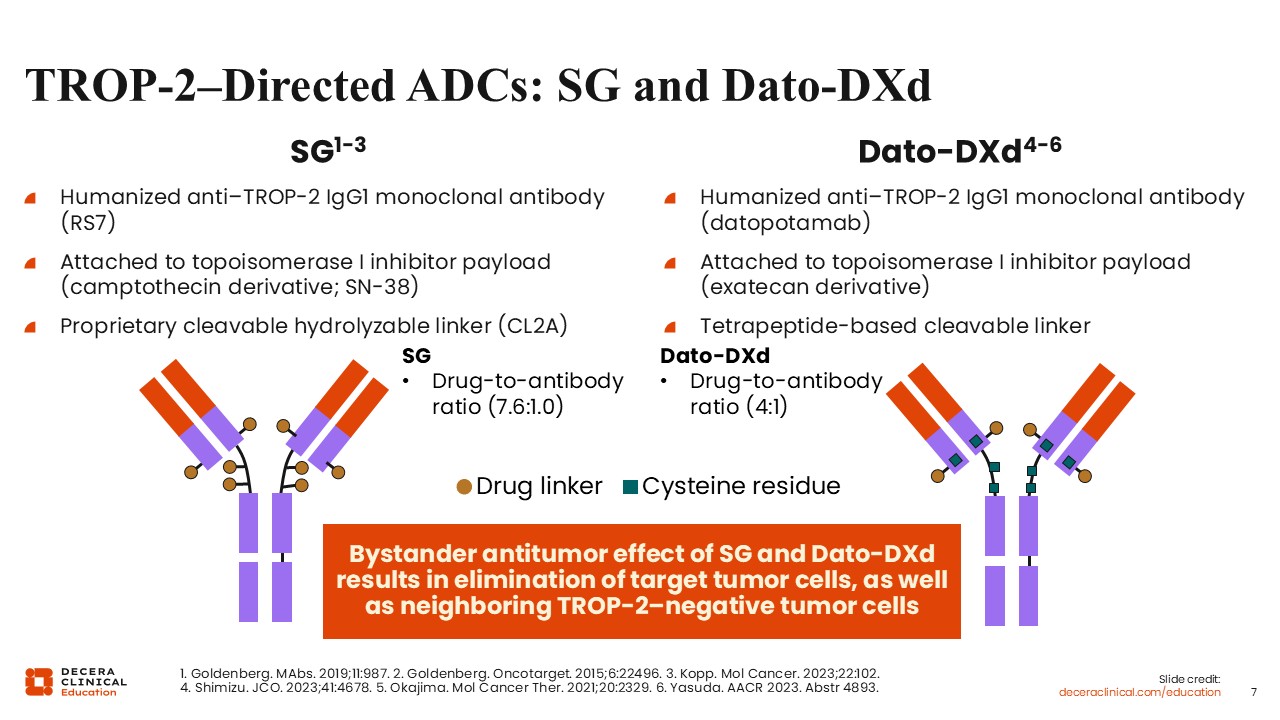
As of the end of June 2026, there are 2 FDA-approved TROP-2–directed ADCs for the treatment of patients with locally advanced unresectable and metastatic TNBC: sacituzumab govitecan and datopotamab deruxtecan. Both are monoclonal antibodies that bind to TROP-2 and both carry a topoisomerase I inhibitor payload, but there are differences in their ADC constructs.
The payloads differ. Sacituzumab govitecan carries SN-38, a camptothecin derivative, whereas datopotamab deruxtecan carries DXd, an exatecan derivative. The linkers differ as well. Sacituzumab govitecan uses a hydrolyzable linker that can be cleaved in the extracellular compartment and metabolized by lysosomal enzymes within the cell, whereas datopotamab deruxtecan uses a more plasma-stable, tetrapeptide-based cleavable linker metabolized by lysosomal enzymes within the cell. The drug-to-antibody ratios also differ: approximately 7.6:1.0 for sacituzumab govitecan and 4:1 for datopotamab deruxtecan. Of importance, both ADCs exert a bystander antitumor effect, meaning they can also eliminate neighboring tumor cells that may not express TROP-2.6,13,14
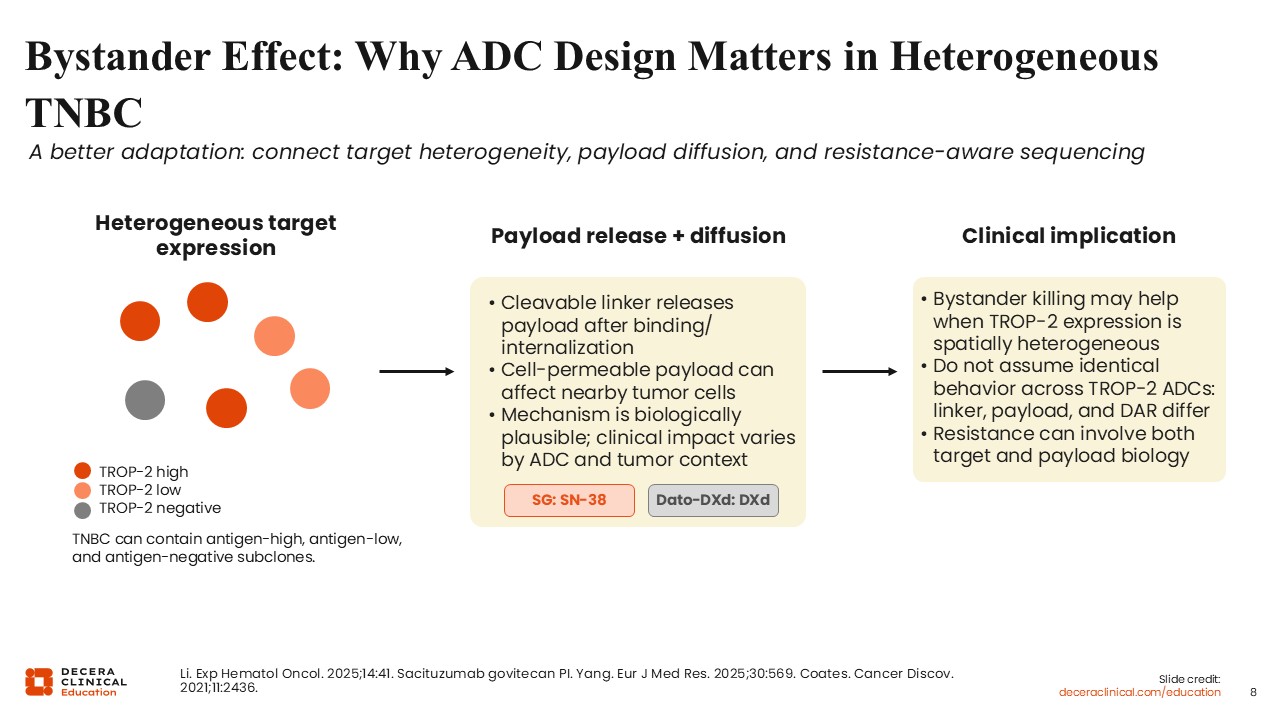
Bystander Effect: Why ADC Design Matters in Heterogeneous TNBC
This bystander effect is particularly relevant for tumors with heterogeneity of TROP-2 expression. After an ADC binds TROP-2 on the tumor cell surface and is internalized, lysosomal enzymes release the payload to exert its antitumor effect. Many newer-generation ADCs contain membrane-permeable payloads that can diffuse out of the primary cancer cell and enter adjacent cancer cells, including those with low or absent TROP-2 expression. This bystander killing effect may help overcome heterogeneous TROP-2 expression.6,15
ADC Design Features Help Anticipate Toxicity
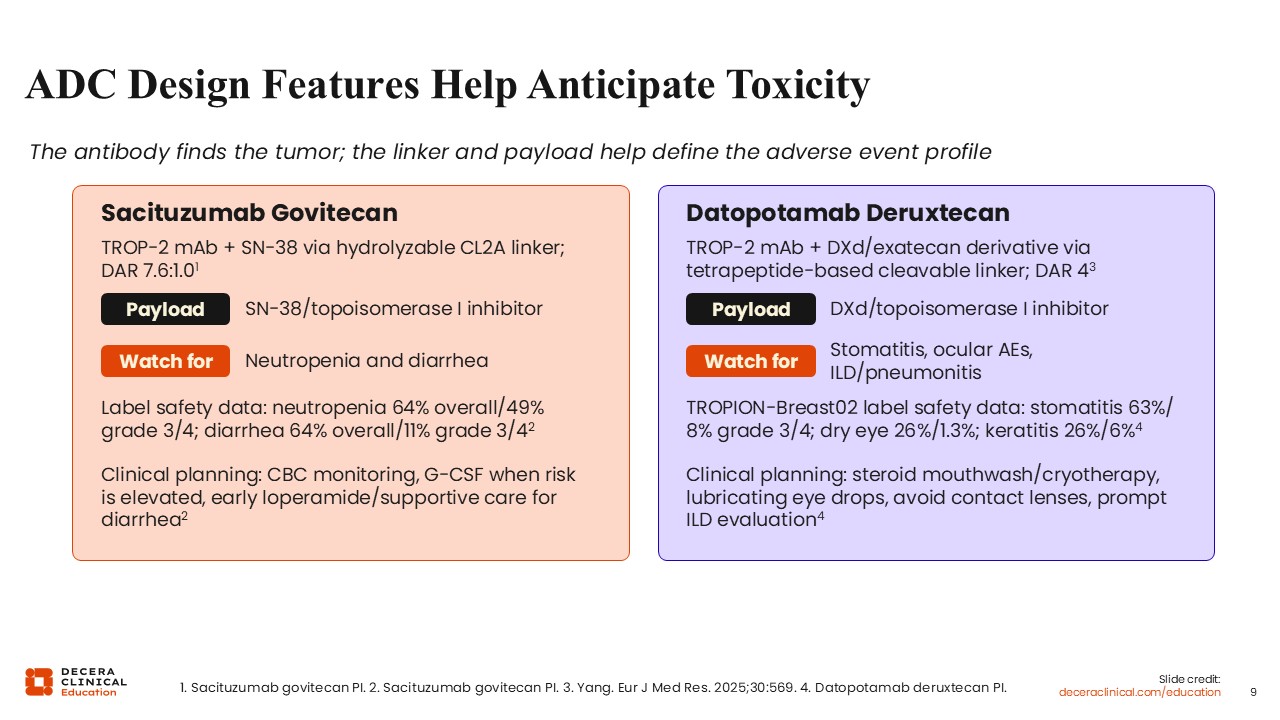
ADC design can also help anticipate the toxicity profile, and there are clear differences in the adverse event profiles of sacituzumab govitecan and datopotamab deruxtecan.
With the SN-38 payload of sacituzumab govitecan, adverse events such as neutropenia or diarrhea should be closely monitored. Approximately 50% of patients treated with sacituzumab govitecan experience grade ≥3 neutropenia, so it is very important to consider primary prophylactic use of growth factor support in patients who are at high risk for febrile neutropenia.13
By contrast, the tetrapeptide-based cleavable linker of datopotamab deruxtecan can lead to adverse effects such as stomatitis or oral mucositis and ocular surface toxicities such as keratitis. In addition, because of the deruxtecan-based ADC structure, there should be close monitoring for interstitial lung disease or pneumonitis.14
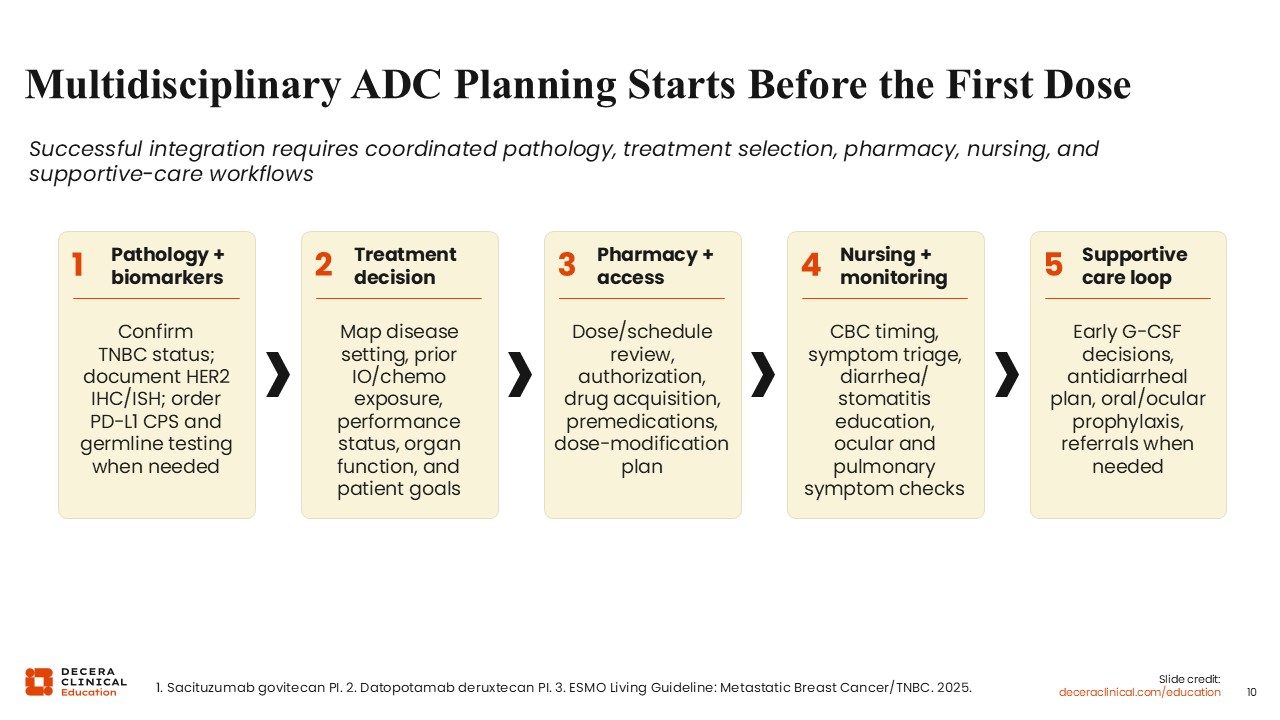
Multidisciplinary ADC Planning Starts Before the First Dose
Multidisciplinary ADC planning starts before the first dose and requires coordinated efforts across pathology, treatment selection, pharmacy, nursing, and supportive care. From the time of initial diagnosis of metastatic or recurrent TNBC, it is important to confirm estrogen receptor, progesterone receptor, and HER2 status and PD-L1 CPS for patients who may be candidates for first-line immune checkpoint inhibition and to review germline BRCA1/2 status and prior chemotherapy, immunotherapy, and ADC exposure.
Treatment selection should also account for disease setting, performance status, organ function, comorbidities, prior toxicities, and patient goals, and the team should review dosing, scheduling, premedications, and dose modifications upfront. Close collaboration with nursing and advanced practice providers supports patient education and proactive toxicity management, and supportive care should be planned in advance, including early growth factor support decisions, an antidiarrheal plan, and oral or ocular prophylaxis. For example, patients receiving datopotamab deruxtecan may be advised to use a steroid-containing mouthwash (and to consider cryotherapy during infusion) to reduce stomatitis and to avoid wearing contact lenses and use preservative-free lubricating eye drops at least 4 times daily, along with recommended eye examinations at initiation of therapy, while receiving treatment, and at the end of treatment.13,14
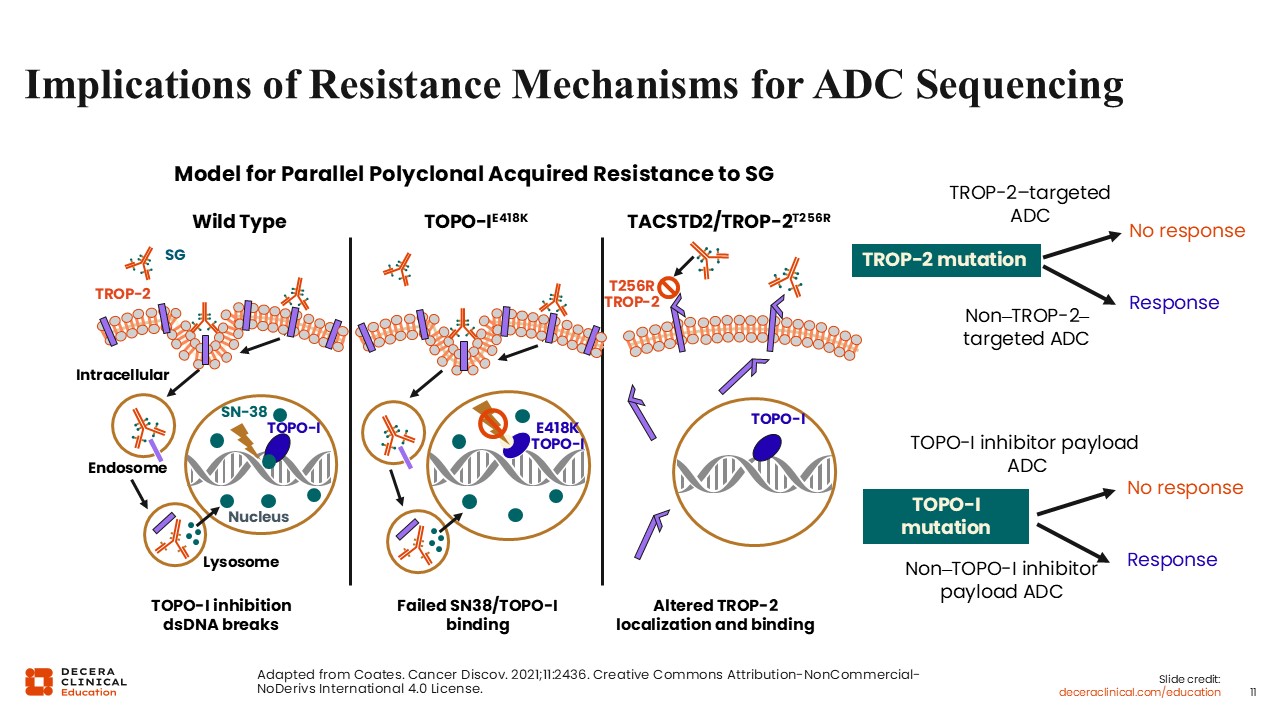
Implications of Resistance Mechanisms for
ADC Sequencing
Several mechanisms of resistance to ADCs have been proposed. Among the best characterized are resistance to the cytotoxic payload and resistance related to the target antigen itself. For example, resistance to topoisomerase I inhibitor–based ADCs may arise through alterations in the payload target. Mutations in the TOP1 gene can reduce the binding of payloads such as SN-38 to topoisomerase I, thereby decreasing their cytotoxic activity and contributing to treatment resistance. One potential strategy to overcome this mechanism of resistance is to use a different cytotoxic payload.
Another target-related mechanism of resistance involves genetic alterations that lead to reduced expression or structural changes in the target antigen. One potential strategy to overcome this mechanism of resistance is to use an ADC directed against an alternative target that is still expressed by the tumor.16
Key Takeaways: Foundations of ADC Therapy and TROP-2 in TNBC
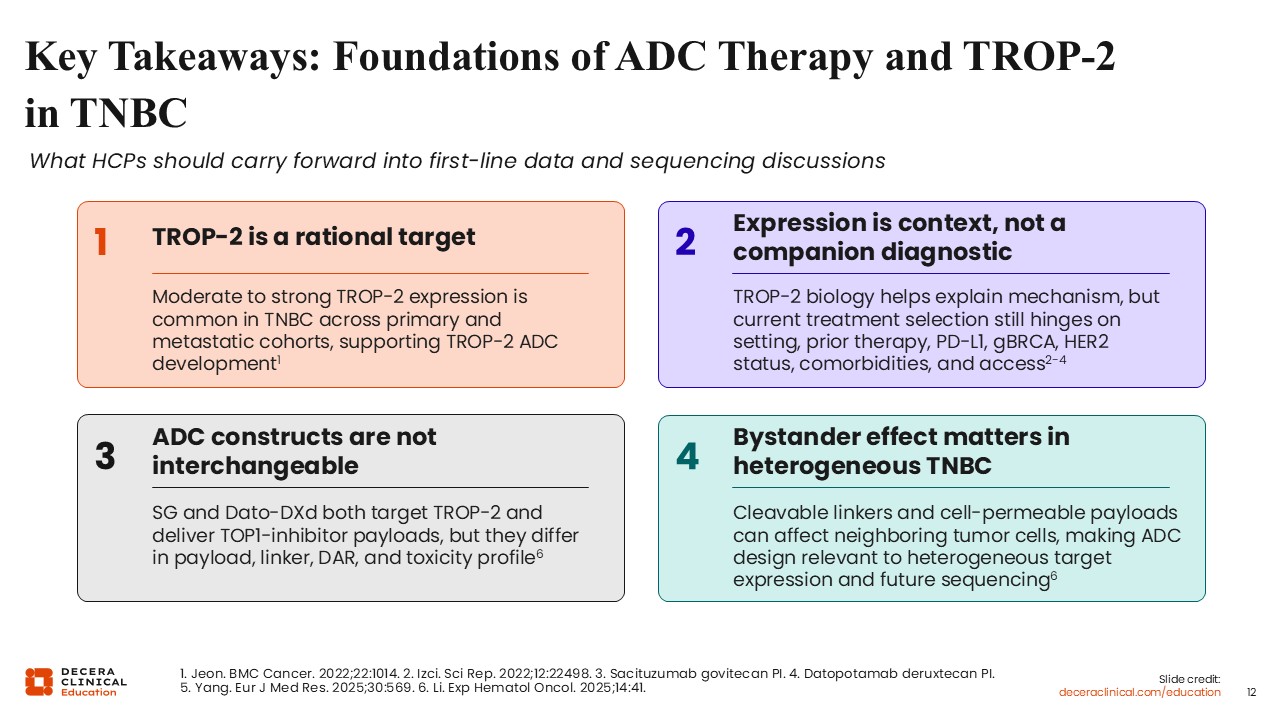
Four key takeaways summarize the foundations of ADC therapy and TROP-2 in TNBC.
First, TROP-2 is a well-established therapeutic target in metastatic TNBC, as it is frequently expressed at moderate to high levels across primary and metastatic tumors. This has supported the development and clinical evaluation of TROP-2–directed ADCs for patients with metastatic TNBC.
Second, although TROP-2 expression provides biological rationale for the use of targeted ADCs, it is not currently used as a companion diagnostic or to guide treatment selection. TROP-2–directed ADCs do not require TROP-2 testing prior to treatment. Instead, treatment selection is driven by clinical factors, including disease setting, prior therapies, and comorbidities, and biomarkers such as PD-L1 status, HER2 expression, and germline BRCA1/2.
Third, ADC constructs are not interchangeable. Although both sacituzumab govitecan and datopotamab deruxtecan target TROP-2 and deliver topoisomerase I inhibitor payloads, they differ in several key structural and pharmacologic characteristics, including the specific payload, linker design, drug-to-antibody ratio, dosing schedule, and toxicity profile.
Fourth, the bystander effect is an important feature of many ADCs, particularly in tumors with heterogeneous target expression. Cleavable linkers and membrane-permeable payloads enable the release of cytotoxic agents that can affect neighboring tumor cells, including those with lower target expression. These design features may help overcome intratumoral heterogeneity and could influence the clinical activity of ADCs across different treatment settings.