CE / CME
SAP-port System Building: Empowering Patients With Seizure Action Plans
Nurse Practitioners/Nurses: 1.00 Nursing contact hour, including 1.00 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Pharmacists: 1.00 contact hour (0.1 CEUs)
ABIM MOC: maximum of 1.00 Medical Knowledge MOC point
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Released: January 13, 2026
Expiration: January 12, 2027


Activity
A 19-year-old patient with focal epilepsy has seizure clusters with 2-3 seizures within 24 hours, and the patient typically does not return to baseline immediately between events. The caregiver asks which outpatient rescue options are FDA-Approved.
A 28-year-old woman who was seizure free for 18 months is now pregnant and reports sleep disruption. She asks whether she still needs a seizure action plan (SAP) “since I’ve been doing well.”
You are creating an SAP for a patient with focal impaired awareness seizures who occasionally progresses to bilateral tonic-clonic seizures. The patient’s partner and workplace supervisor may need to use it.
What Is a Seizure Emergency?
Danielle Becker, MD, MS, FAES:
A seizure is considered an emergency when it lasts longer than the patient’s baseline pattern or when multiple seizures occur back to back, and there is no recovery in between them. Breaking it down further, we consider a seizure emergency a cluster of seizures or acute repetitive seizures with 2 or more seizures in 24 hours, with or without returning to baseline between them. We would also consider a prolonged generalized convulsion a seizure emergency.1,2
The question would be: What does “prolonged” mean? Status epilepticus, which is currently defined as a seizure that lasts longer than 5 minutes, is universally considered prolonged.3,4 Beyond that, people have different perspectives on when to trigger the recommendation to take rescue medication.
In my practice, for people who have either focal to bilateral tonic–clonic seizures or primarily generalized seizures with convulsions, I tell them to take rescue medication immediately. As soon as they recognize these seizures, it is an emergency. I consider it an emergency because we know that generalized tonic–clonic seizures, especially if prolonged, are difficult to stop. The longer they go on, the more likely it is that the patient may have neurologic damage, and the longer it will take for the patient to recover. We also consider a seizure an emergency if it causes any type of injury or illness.
Finally, probably the most important aspect when we communicate with our patients is to define the typical seizure characteristics for each patient. Patients should know their baseline seizure patterns and presentations. We then have a discussion to help them to determine what would be different or unusual compared with their typical seizure baseline or pattern. For example, if someone has a focal aware seizure and recovers quickly with no alteration in awareness, we would not necessarily consider that an emergency or recommend the use of a seizure rescue medication. But if the patient never has focal impaired awareness seizures or focal to bilateral tonic-clonic seizures and starts having either of those, then that would be different than baseline and would be considered a seizure emergency and warrant intervention.
To summarize, if the patients’ seizures increase in frequency, intensity, severity, or duration, then that would be considered a deviation from their baseline pattern and a seizure emergency.
Sarah Weatherspoon, MD:
In general, most seizures resolve spontaneously. However, research has shown that seizures lasting longer than 5 minutes are much less likely to resolve spontaneously.1 There are some caveats to this. First, we sometimes do not know when the seizure began. For people who may have subtle seizure activity at the beginning, such as focal seizures with impaired consciousness, we may not know when the true onset was. By the time that person has potentially gone into a convulsive state or a bilateral tonic-clonic state, the seizure may well have been already ongoing for 5 minutes. Second, research has also borne out that the cumulative effect of seizures over time can lead to pathologic neuronal changes, as we see in brain specimens from people who have undergone autopsy.5
Being proactive in stopping seizures, not just on a 5-minute rule of thumb, but treating sooner rather than later, is critical to preventing those pathologic changes, risk of injury, and illness. We must avoid a situation where the medication fails to work because the seizure was going on longer than what was originally realized by the caregiver or the provider.
Seizures can be particularly dangerous. For example, if somebody is swimming at the time of the seizure, there can be a risk of aspiration or drowning. With some more convulsive types of seizures, people may have a dislocated joint, such as a shoulder. In underlying low bone mineral density, like some patients with concomitant cerebral palsy, they are at high risk for fractures. Therefore, minimizing the time spent in seizures is critical to preserving safety regarding overall health. An extreme example would be sudden unexpected death in epilepsy (SUDEP).
This applies no matter the age of the patient because anything above baseline, such as 5 minutes or acute repetitive seizures, can occur in both children and adults. Imaging studies indicate that there may be structural changes to the brain when there are repetitive or prolonged seizures.6 Clinically, we observe that the overall seizure burden may affect neurocognitive function and development, although it is not a one-to-one or a direct causative link that we can track.
Danielle Becker, MD, MS, FAES:
Any generalized convulsion is an emergency and requires immediate intervention because of increased morbidity, mortality, pathologic changes, and impact on cognition over time with more prolonged seizures.
Sarah Weatherspoon, MD:
There are also a few patients with epilepsy who have frequent convulsive seizures despite all the right things being done. These patients have particularly difficult epilepsy to control. They may have generalized convulsive seizures more frequently than we would wish, and we need to think about optimizing the efficacy of the rescue medicine.
Consequences of Seizures
Danielle Becker, MD, MS, FAES:
We know that when we are treating seizures, we are very good at treating the chronicity of a seizure and at using medications long-term to prevent them. We do not always focus on the immediate acute emergency or the consequences of active seizures. My pediatric colleagues do a much better job with this than I do, as an adult epileptologist. It is essential, when treating the whole patient, to educate them and ensure their safety. The consequences of seizures may include injuries and hospitalizations.
While convulsing, people with epilepsy might have a dislocation of their shoulder, and if this recurs, they may need surgery because of chronic injury. With seizures, there is increased morbidity and increased risk of premature death, which in some studies has been related to the ensuing surges of catecholamines that develop during convulsive seizures.7 The seizure burden can weaken the heart over time. Patients who have uncontrolled seizures, specifically convulsions and convulsions during sleep or nocturnally, are at an increased risk of SUDEP. It has been suggested by caregivers of people who have died from SUDEP, that being aware that SUDEP can be a consequence of ongoing uncontrolled seizures, or of nonadherence, can motivate patients and families to stay adherent.
Sarah Weatherspoon, MD:
It may encourage caregivers to consider additional monitoring options to provide layers of protection for their loved ones and for themselves, depending on whether their sleeping situation includes a roommate, a bed partner, or a room partner.
Danielle Becker, MD, MS, FAES:
When medications are not working, it encourages conversation about considering alternative nonpharmacologic options to reduce SUDEP risk, such neuromodulation devices and neurosurgery. As previously mentioned, prolonged seizures can hold an increased risk of morbidity, mortality, long-term cognitive adverse effects, and pathologic changes in the brain.
Seizures also reduce the quality of life of the patients and their caregivers through the constant fear that a seizure could come at any time. This unpredictability creates an emotional burden: always worrying that “the shoe is going to drop,” which often leads to isolation, avoidance, effects on social relationships, employment, or education.
People with epilepsy may be afraid to do activities outside the home. Even going to the ICU or having hospitalizations can affect quality of life, mental health, and the ability to interact with those around them.
Sarah Weatherspoon, MD:
Regarding injuries, these can include head injuries from falls with a seizure, which can further compound neurologic outcomes and neurocognitive function and potentially increase the risk of other seizures.8
Epilepsy Costs and Outcomes
Danielle Becker, MD, MS, FAES:
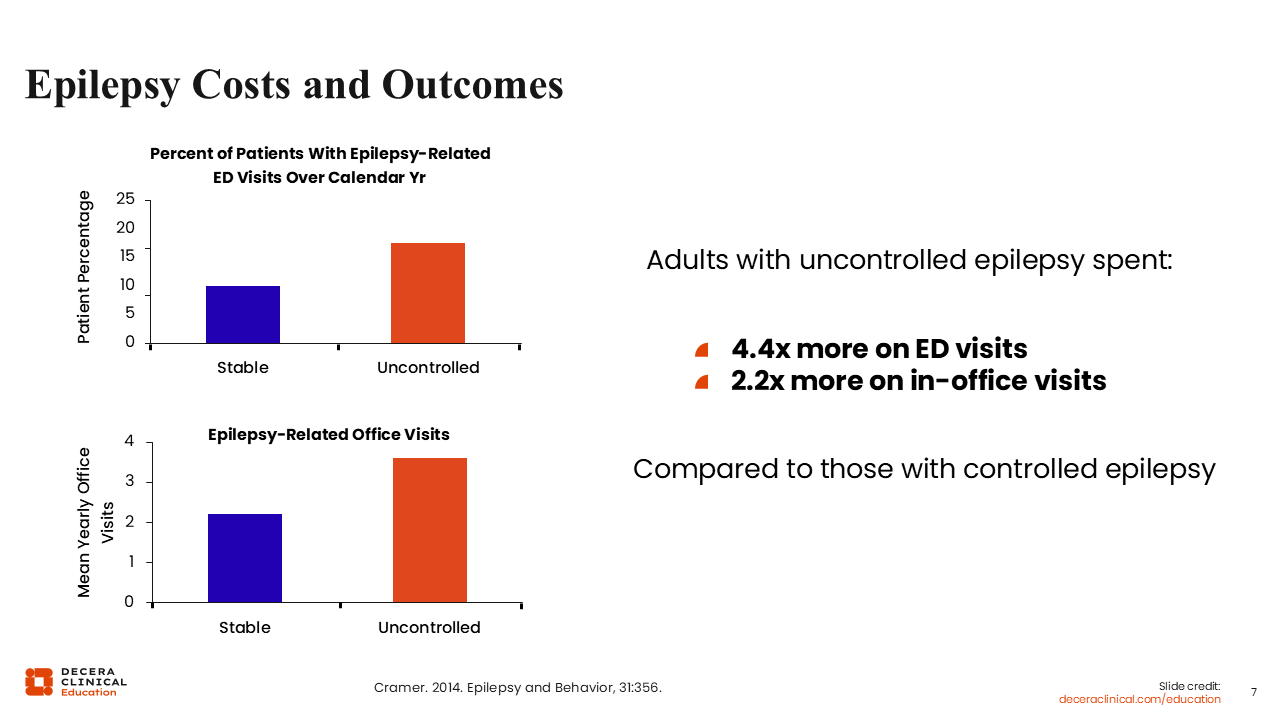
This study by Cramer and colleagues9 highlighted epilepsy costs and outcomes by comparing the percentage of patients with uncontrolled vs well-controlled seizures who had epilepsy-related ED visits during a calendar year as well as epilepsy-related office visits. The study showed that those people with epilepsy who have uncontrolled seizures have 4.4 times more epilepsy-related ED visits and 2.2 times more epilepsy-related office visits compared with those who have controlled epilepsy.
Patients Live With the Burden of Not Knowing When Seizure Clusters Will Occur
Danielle Becker, MD, MS, FAES:
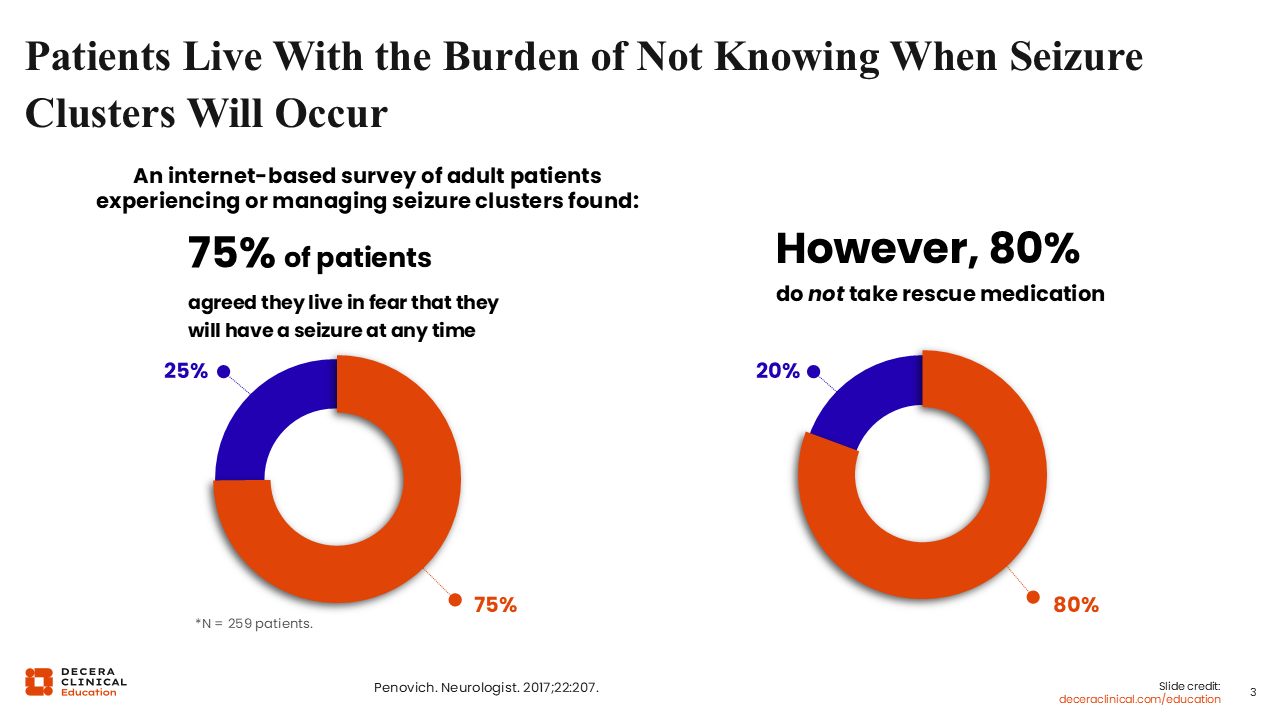
In a study done by Penovich and colleagues,10 an internet-based survey of adult patients experiencing or managing seizure clusters, 75% of patients agreed that they live in fear of having a seizure at any time. As mentioned previously, this goes hand in hand with an increased emotional burden that affects quality of life. However, despite this fear, the survey showed that 80% of patients did not take rescue medication, suggesting a disconnect.
Where does that disconnect happen? Is it happening in communication between HCPs and patients? Is it happening in patient and caregiver education about the impact of seizure rescue medications? Is it because there are misconceptions that rescue medication might cause respiratory depression or make people too tired? Have patients or caregivers been told that patients are going to come out of the seizure regardless of medication in 1-2 minutes, so they can let it take its course, and only if it lasts longer than 5 minutes, do they need to intervene?
With the advent of various rescue medication formulations introduced in 2019 and 2020,4 these conversations have come to the forefront. To change this and ensure patients receive rescue medications, there is greater awareness that education is needed for HCPs, patients, and caregivers.
The statistic that 80% of patients are not taking a rescue medication leads to the question of whether they were not taking it because they did not have it or because they had it but did not know how to use it. As my practice has changed over the years with more acceptable formulations of rescue medications on the market, it is probably a little bit of both.
I did not used to have as many conversations with patients about rescue medication as an option because I also needed more education. Acceptable formulations for patients facilitated more meaningful conversations for me and improved my understanding of the impact of rescue medications on my patients.
Use of Rescue Medication for Seizure Clusters Is Associated With Improved Outcomes and Lower Costs
Danielle Becker, MD, MS, FAES:
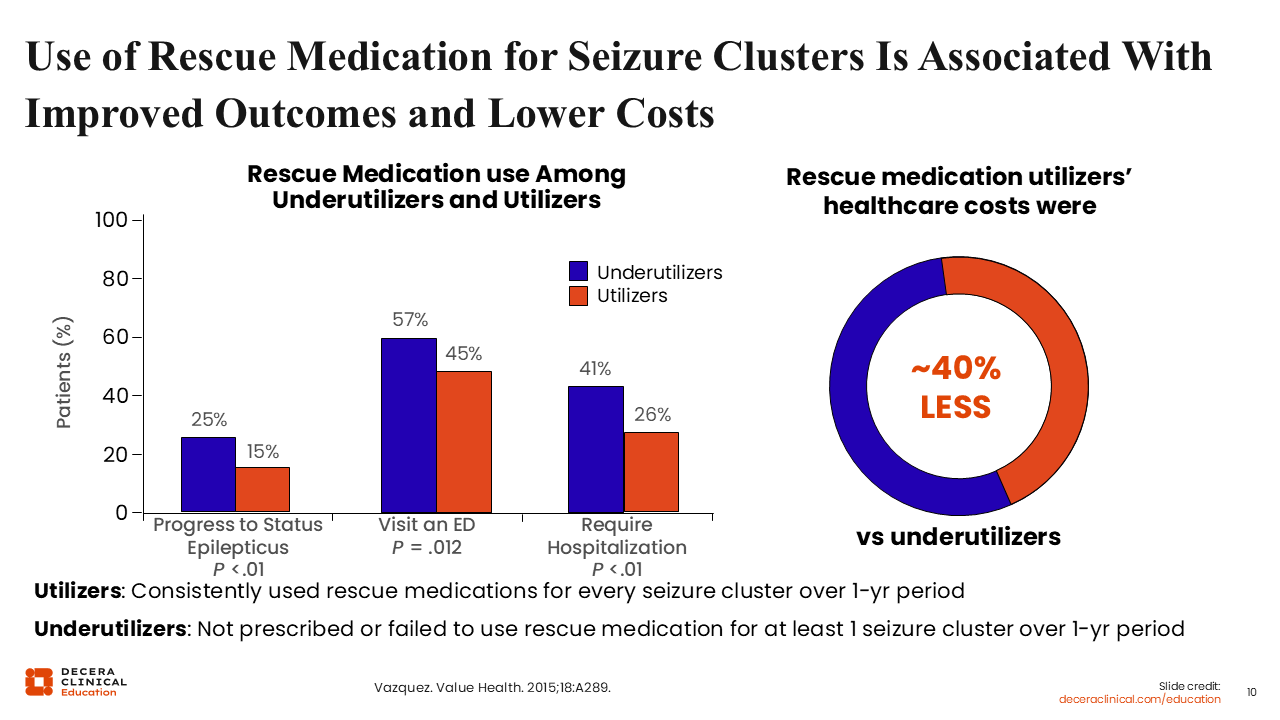
In seizure clusters, the use of rescue medications further supports their association with improved outcomes and lower healthcare related costs. In a study by Vasquez and colleagues11 comparing rescue medications between utilizers (who consistently used rescue medications for every seizure cluster over a year) and underutilizers (who were not prescribed or failed to use rescue medications), underutilizers had a greater percentage of status epilepticus, ED visits, and need for hospitalization. In addition, a 12-month healthcare cost analysis showed that rescue medication users had 40% lower healthcare costs compared with underutilizers.
Proper Use of Rescue Medication Reduces ED Visits
Danielle Becker, MD, MS, FAES:
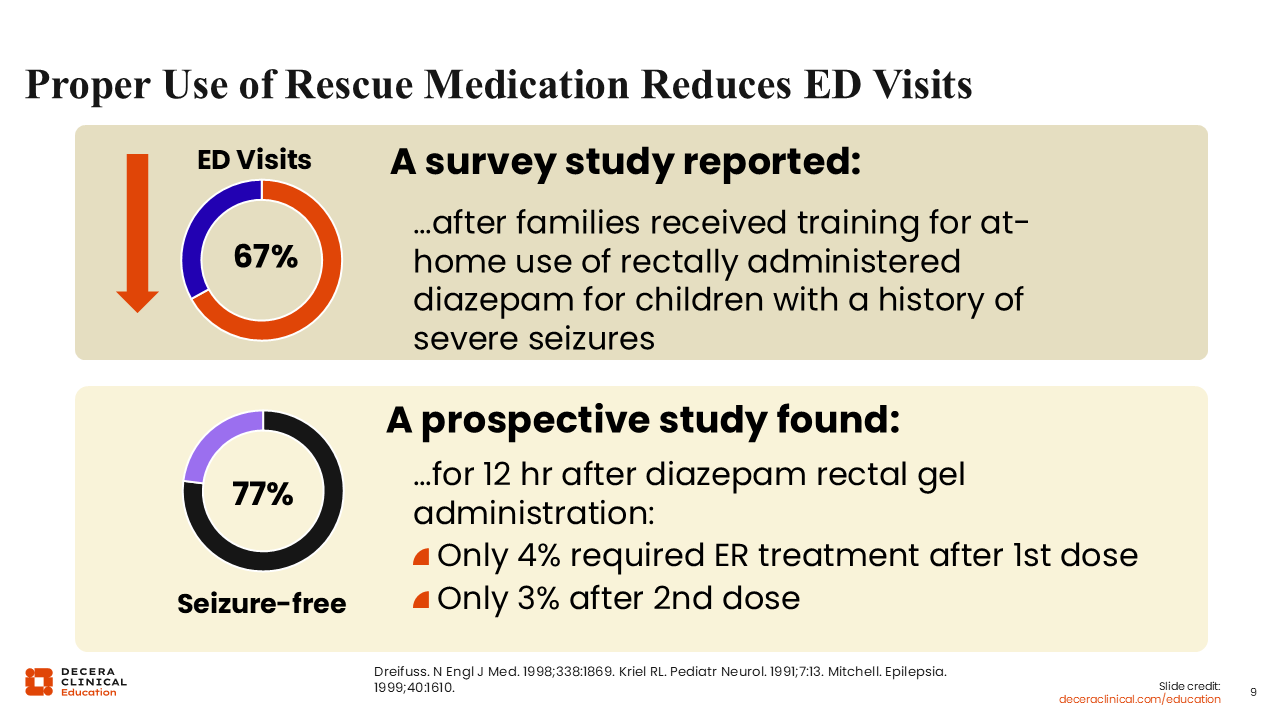
Further supporting that the proper use of rescue medication reduces ED visits, a survey showed that after families received training for at-home use of rectal diazepam for children with a history of severe seizures, their ED visits were reduced by 67%.12
Furthermore, another prospective study found that within 12 hours after rectal diazepam gel was administered, 77% were seizure free, only 4% required ED treatment after the first dose, and only 3% required ED treatment after the second dose.13
Use of Seizure Action Plans and Rescue Medication Are Associated With Reduced Healthcare Utilization
Danielle Becker, MD, MS, FAES:
We know that the use of SAPs and rescue medications are associated with reduced healthcare utilization and that having no rescue medication or having an inappropriately dosed rescue medication is associated with increased ED utilization. A retrospective study of 120 pediatric patients with epilepsy showed that patients who were given either no rescue medication or an inappropriate dose of rescue medication were 11 times more likely to have multiple ED visits and/or unplanned hospitalizations than those given correct dosing.14
Despite Benefits, Seizure Action Plans and Rescue Medications Are Underutilized
Sarah Weatherspoon, MD:
As we mentioned, SAPs and rescue medications appear to be underused, causing EDs to be overused. This puts an additional burden on the overall healthcare system and can lead to further delays in the care of people with epilepsy.
In one survey of more than 500 people with epilepsy and their caregivers about their typical response in the setting of a seizure cluster, up to 80% did not take rescue medication, and 31% of patients and 40% of caregivers ended up relying on the ED for those seizure clusters.10
That same survey also reported that 61% of physicians said that they essentially recommended the ED as the SAP, which again is an avoidable situation. Anything we can do to keep patients safe at home will improve their quality of life. Going to the ED does not necessarily mean that they will get care in a timely fashion, given the overall burden of the healthcare system. It could lead to delayed care and negative outcomes, such as more difficulty terminating that seizure!
What Is a Seizure Action Plan?
Sarah Weatherspoon, MD:
An SAP is a bridge between patients, their fears, their concerns, and their day-to-day experiences of living with epilepsy with a proactive plan. It gives them back a sense of control over their epilepsy and can help them feel empowered, rather than in a state that might otherwise feel helpless.15
In practice, an SAP is a written, tailored guideline for responding to a seizure. One of its key components is identifying the kind of seizure that patients have and what steps need to be taken to help them when they have that seizure.
Some patients may be able to institute it themselves if they retain some awareness during their seizures. For the majority of patients, there is some impairment of consciousness as part of the seizure, which means that an external person (caregiver, teacher, nurse, parent, friend, or spouse) may be the one giving that medication. Because of that, the plan needs to clearly specify the person’s seizure type and include practical steps that caregivers and other responders can follow.
The SAP should summarize several key components of that person’s seizure history. What is their treatment plan? What is their history? What medications are they currently taking? What are some nonmedical interventions available?
This may include how to position that person during the seizure (laying them on their side), reminding people that they do not need to stick anything in that person’s mouth (which could be dangerous in the moment) and options that can sometimes help terminate a seizure in certain patients, for example, a vagal nerve stimulator, where there may be an external magnet that can be swiped to help terminate that seizure quickly. Finally, it should outline the appropriate treatment for these seizure emergencies.
Overall, the SAP facilitates comprehensive communication of care among all members involved in that person’s care, regardless of their healthcare or medical background.
Danielle Becker, MD, MS, FAES:
I appreciate that you used the word “empowerment,” which is what I always use. An SAP gives the patients and the caregiver empowerment against that feeling of helplessness because they cannot control their seizures. They live in a world of unpredictability in which seizures can occur at any time. The SAP gives them something predictable. Although it cannot prevent seizures, it instructs them on what to do if a seizure happens.
Sarah Weatherspoon, MD:
SAPs can also improve quality of life by mitigating the fear of seizures.
Communication With the Patient/Caregiver
Danielle Becker, MD, MS, FAES:
When we talk with people with epilepsy and their caregivers, it is important to formulate strategies for communication and conversations and to promote an understanding that this is a partnership, a journey together, where we will formulate these action plans and put safety mechanisms into place. But you want to make sure that the person with epilepsy understands the conversation and knows when to use the medication, giving them something that is flexible but also individualized.
Sometimes in our community, we are asked by individual patients about the definition of a seizure cluster. Rather than a black-and-white definition that specifies 2 or 3 seizures within 24 hours, we emphasize that it depends on patients’ individual pattern. If their baseline pattern is 2 clusters of myoclonic jerks, and suddenly, they start having 3-4 clusters, that flexibility allows for customizable variations in how we describe seizures based on the patient’s own individual seizure pattern.
Communicating with people with epilepsy and their caregivers to define a baseline and then defining what is abnormal above the baseline enhances both parties’ ability to recognize a seizure cluster or a seizure emergency quickly and, in turn, intervene.
In a study comparing traditional definitions with computerized algorithmic definitions that accounted for baseline seizure frequency and natural variation, traditional definitions were more likely to miss or misidentify seizure clusters.16 This can lead to patients not receiving the treatment they need because plans are overly rigid, inflexible, and not individualized.
Customized definitions allow for a more sensitive and individualized plan to identify seizure clusters and seizure emergencies, facilitate the needed treatment as soon as possible and get the patients back to their usual living as soon as possible.
Planning Gives Empowerment
Danielle Becker, MD, MS, FAES:
When you tell people what to do in an emergency and how to do it, it gives them a sense of empowerment. You want to ensure it is incorporated with an appropriate literacy level, guidance on interpreting visuals, and individualized information, such as seizure type, duration, emergency conditions, and when and when not to administer rescue medication or call 911. This individualization not only helps reduce seizure burden and anxiety but also supports timely care, improving social functioning and reducing hospitalization.
Where Do Seizure Action Plans Fit in?
Sarah Weatherspoon, MD:
Where do SAPs fit into one’s neurology practice?
First, multiple definitions of a seizure cluster make it challenging to standardize when and how to institute an SAP as an HCP.
In addition, the time threshold for status epilepticus has decreased from 30 minutes to 5 minutes in our most current definition. These changes in how we define seizure clusters and status epilepticus support earlier recognition of seizure emergencies and help prompt the use of a rescue medication.
Having an acute SAP in place provides patient-specific guidance.17 Seizure types and seizure frequency can look very different from patient to patient, so the idea of a one-size-fits-all plan is not feasible.18 The goal is to identify and clarify the appropriate course of action when a seizure cluster occurs.
Why It Is Important to Have a Response or Seizure Action Plan
Sarah Weatherspoon, MD:
Patients and families play a central role in seizure management. They are the ones primarily affected on a day-to-day basis by this diagnosis of epilepsy. The success in managing epilepsy depends on being ready to take on whatever may come.
This includes understanding what epilepsy is, what seizure types are, and maintaining seizure control by responding to seizures when they do occur to keep individuals safe. An SAP helps to organize key seizure information and makes it readily accessible, especially when transitioning between clinics, HCPs, school settings, and living situations. It provides patients and caregivers with clear instructions for managing emergencies and can also be adapted to different life contexts, such as transitioning to college.
Danielle Becker, MD, MS, FAES:
Life circumstances can change seizure risk. For example, during pregnancy, a person may be sleep deprived. As the pregnancy progresses, there is an increase in the volume of distribution that can affect antiepileptic drug levels, and their levels can fall. There could be an increased risk for seizures even if we check levels and increase the patient’s medications. Changing the SAP to accommodate this might be needed. The other thing that is important to keep in mind post-delivery is that people with epilepsy during these times may again be sleep deprived, may be stressed, and may be breastfeeding. One must tailor SAPs to the individual situation, modifying them in response to life changes and their individual risk factors. SAPs are not one and done. They are modifiable and need to be revisited at least yearly to make sure that they are accommodating the individual characteristics of each patient and how their seizures may change over their lifetime and more often in cases of rapid change, such as pregnancy and the postpartum period.
Sarah Weatherspoon, MD:
When it comes to weight and age in the pediatric population, that can change quickly too. Ultimately, we may not be able to change a person’s epilepsy diagnosis, but we can reduce fear and support fuller, safer participation in life by putting a plan in place.
Danielle Becker, MD, MS, FAES:
Dosing considerations change with weight, most notably in pediatrics, but also in adults. Some adults may require adjustments to rescue dose after significant weight loss or gain. I have had several patients who were on 20 mg of diazepam nasal spray, and then they lost weight. Now they are on 15 mg.
Beyond having a rescue medication available, people need clear guidance on how and when to intervene during emergencies.
Practical Aspects
Sarah Weatherspoon, MD:
Given the practical aspects of SAPs and rescue medications, the first consideration is where to store them. This will vary by individual and by living situation or family.
At school, for example, the medication may need to be kept in the nurse’s office depending on the school’s requirements, and the SAP is usually provided to the school nurse.
For adults in a workplace, it may look very different and should be discussed with the caregiver or the HCP. Who should have it? Should the person living with epilepsy carry it on themselves? That may be appropriate for somebody who has seizures at the start, with consciousness still intact, where they could potentially self-administer. The SAP should be updated any time somebody’s seizure pattern changes or new seizure types emerge and any time medications are being changed (eg, potentially weaned off).
Who Benefits From a Seizure Action Plan?
Sarah Weatherspoon, MD:
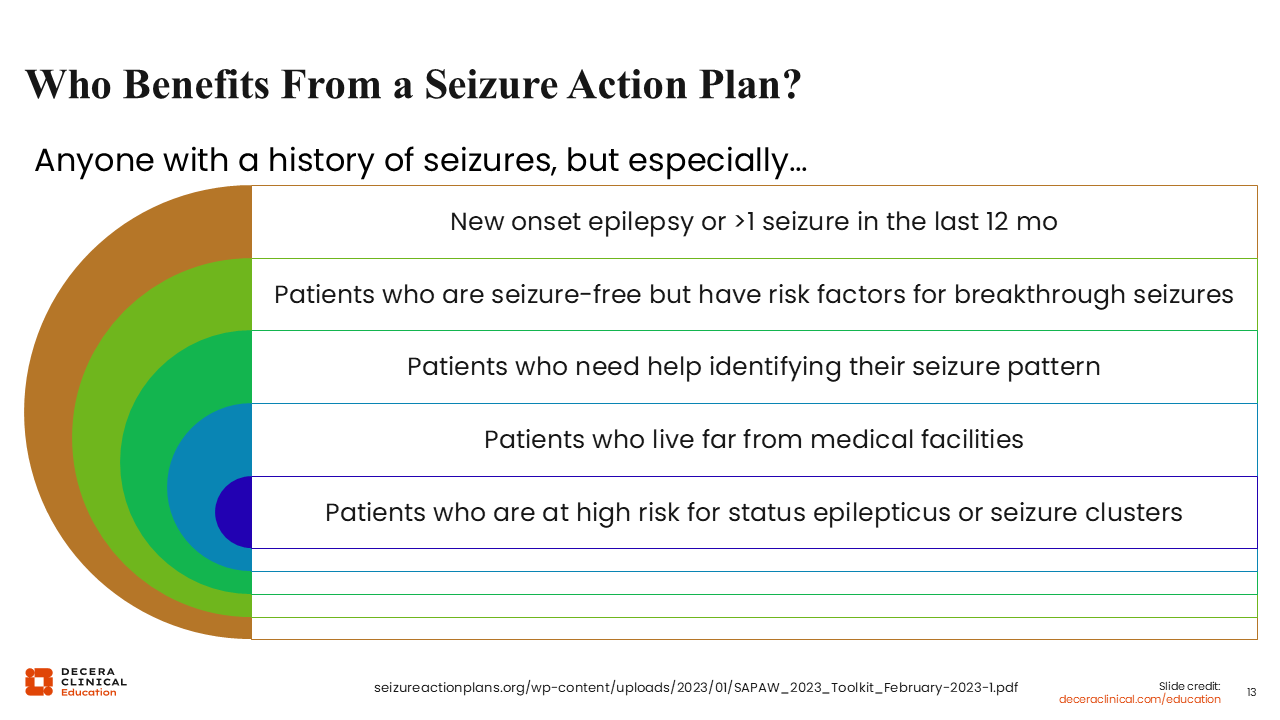
Who benefits from the SAP? Anybody, again, who has a history of seizures, and their caregivers. This can include individuals for whom we have not yet fully defined their baseline seizure frequency or type, simply because there have not been enough data points to really ascertain that.
Even in patients who are seizure free, an SAP may still be warranted. There may be times when there is decreased sleep or a change in routine, like a change in what pharmacy they need to use, or accidentally missed doses. Patients may also need help identifying their seizure pattern and being able to clarify their type of seizure in the SAP. An SAP can also be especially helpful in remote settings, where local emergency care may not be available, or when they need to go to a different facility where their electronic medical records may not be immediately accessible.
People who are at high risk for status epilepticus or seizure clusters, which we sometimes only know retrospectively once it has already occurred, really benefit from SAPs.
Danielle Becker, MD, MS, FAES:
Finally, even people who are seizure free but have risk factors for breakthrough seizures can benefit from SAPs, especially during a major stressor, like the loss of a loved one. It can also help patients identify their seizure triggers, target potential interventions, and have an action plan in place if they cannot always avoid those triggers.
Who Is the IDEAL Candidate for an SAP?
Sarah Weatherspoon, MD:
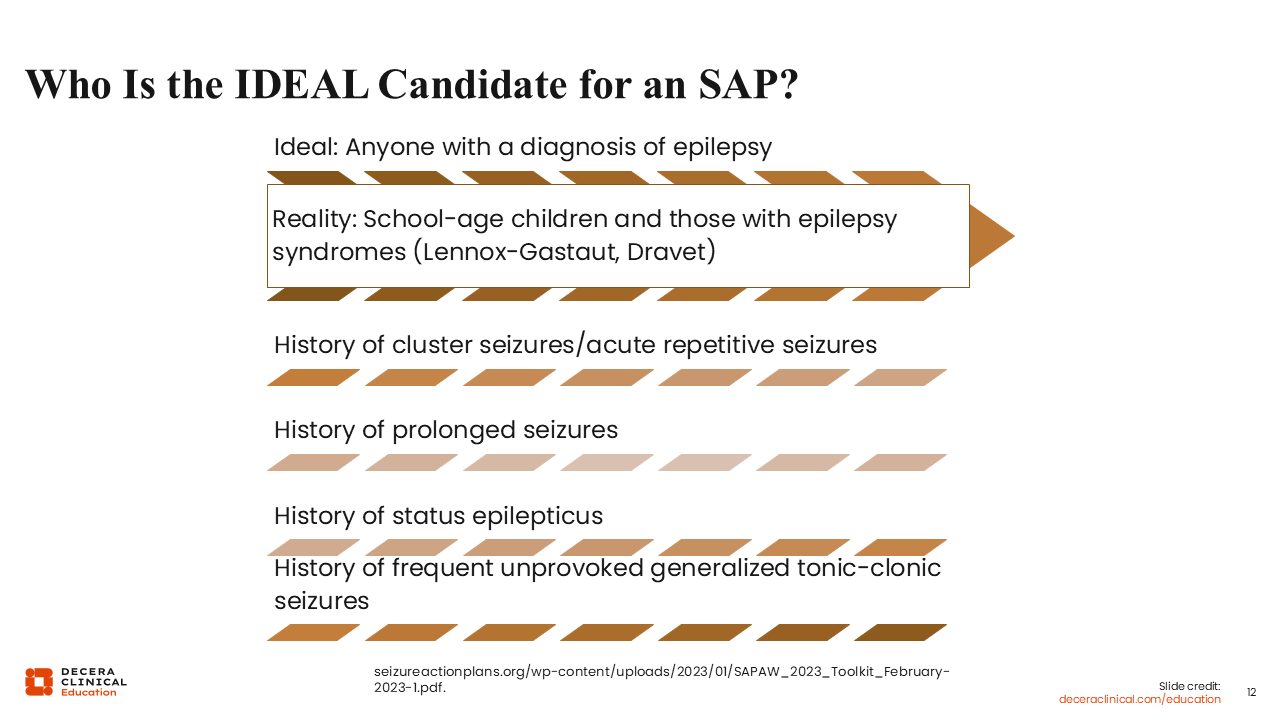
The ideal candidate for an SAP is anyone with epilepsy. In practice, it tends to be mainly school-aged children or people who have particularly intractable epilepsy syndromes like Lennox-Gastaut or Dravet syndromes.19
Certainly, anybody who has a history of cluster seizures or acute repetitive seizures should have an SAP. Anybody with a history of prolonged seizures or status epilepticus absolutely should have one in place. Someone who has frequent, unprovoked generalized tonic-clonic seizures should as well.
Although we can lay out these criteria, the reality is that even in someone who is seizure free, seizures can worsen under certain circumstances, like sleep deprivation, illness, or accidentally missed doses of medication. So even in somebody who has fantastic control, it is still possible to have 2 seizures in 24 hours under enough physiologic stress. Being prepared with an SAP is really critical, therefore, for anybody with a diagnosis of epilepsy.
Who Should Know About the SAP for Children With Epilepsy?
Sarah Weatherspoon, MD:
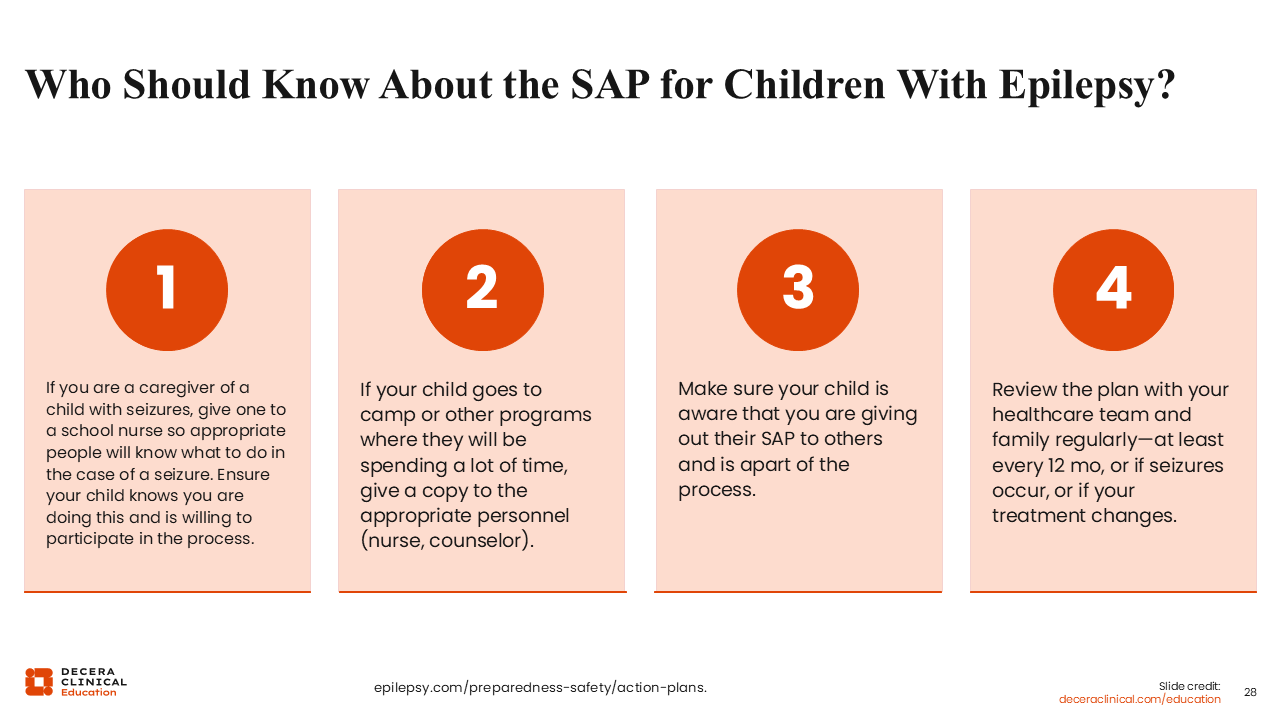
Who should know about the SAP for children with epilepsy? First is the caregivers because these are usually the ones administering rescue medication, especially at home and overnight. Second is the school nurse. Beyond that are other settings where the child spends time, such as after-school programs, summer camp settings, and even situations like a sleepover at a friend’s house. Finally, when developmentally appropriate, the child with epilepsy should also understand the SAP because that autonomy supports independence and helps them participate in their own care over time.
The plan should be reviewed with the healthcare team at least every 12 months and more frequently if seizures occur unexpectedly or treatment changes.
What Should a Seizure Action Plan Look Like?
Danielle Becker, MD, MS, FAES:
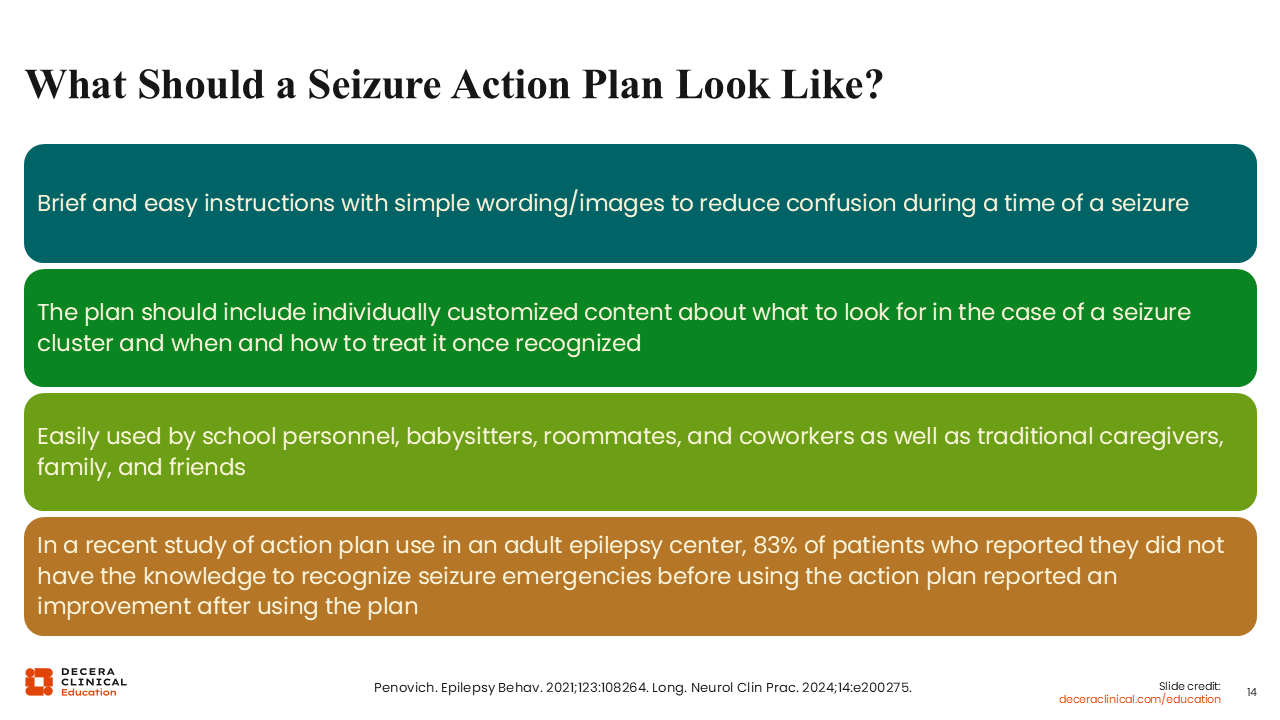
What should an SAP look like? First, it should be brief, concise, and easy to follow. Ideally, it would include simple wording and pictures because we are trying to reduce confusion during a time of stress. The plan should include individualized content on what would be recognized as a seizure emergency or a seizure cluster for that patient, and what to do when such events occur.17 Once it is recognized, it should be easy for school personnel, babysitters, roommates, coworkers, caregivers, family, and friends to use.
In a recent study of SAPs used in an adult epilepsy center, 83% of people with epilepsy who initially reported not recognizing seizure emergencies before using the action plan reported improvement after a detailed discussion, being given an action plan, and using it.20
What to Convey in an SAP
Danielle Becker, MD, MS, FAES:
Going a little bit more into actual tangible examples of an SAP, you want to convey that a seizure is a medical emergency and that it is important to have a treatment plan, so you know what to do in that circumstance and, of most importance, to stay calm. Making sure that all people with epilepsy have an individualized emergency plan with them helps to ensure that the needed intervention is given to stop the emergency as soon as possible.
Rescue Medications Should be Part of Every SAP
Sarah Weatherspoon, MD:
There are multiple SAP templates available through various nonprofit organizations, and these resources can be very helpful in creating a clear, standardized plan. Rescue medications should be part of every SAP, so that when a seizure emergency occurs, families and caregivers are not trying to make decisions in the moment without guidance.
The Current State of the Conversation
Sarah Weatherspoon, MD:
Regarding SAPs, the current state is that they are typically required only in schools and group homes. Many states may have seizure safety legislation in place that requires, for example, nurses to be available to give seizure emergency medications when needed.
Children attending school outside the home will almost always have an SAP, whether they are in a private or public setting. However, only 20% of patients use rescue medication, as we saw in the data presented earlier.10
It becomes a problem when patients are in a situation where an SAP is not required or when they are transitioning from the structured situation of going to school every day and being a minor into adulthood, where they may no longer be attending school and instead are attending a workplace.
In these situations where we do not have an SAP in place, patients and caregivers can find themselves relying more heavily on emergency services. This can lead to delays in care and more negative outcomes. For instance, it may take time for emergency medical services to arrive at a person’s home, depending on whether the person lives in an urban or rural setting and on the demands placed on emergency medical services, which can further delay administration of seizure emergency medicine. This increases the likelihood that seizures will last longer than 5 minutes, which, as noted earlier, are less likely to resolve spontaneously.
In addition, prior to 2019 and 2020, the only FDA-approved rescue medication was rectal diazepam, which was not always socially amenable to many of our patients and caregivers or feasible to give.4 For instance, if a person with epilepsy is of a body size where their caregiver is unable to position them properly to give something rectally, then it becomes physically difficult, if not impossible, to administer an emergency medication, even if it is available.
Another component with rectal diazepam is variable absorption. Just because a certain dose, 10 mg for example, was prescribed and administered does not mean that 10 mg was absorbed. Without the same predictability in absorption, efficacy with the rectal formulation can be diminished.
There can also be mixed messaging when there is not a documented SAP about how and when to take a rescue medication. We know that during verbal conversation in the clinic, not all the information exchanged is always absorbed. In the midst of discussions about daily seizure medications, SUDEP, seizure safety, and quality of life, that piece about when to give the medication may not be fully registered. So having something documented to look back at is very useful for people with epilepsy and their caregivers. It reminds them when to give seizure rescue medication and supports appropriate use.
Danielle Becker, MD, MS, FAES:
When benzodiazepines that are not approved by the FDA for a rescue situation are used,21 the message can be confusing. In the SAP, we advise caregivers not to place anything in the mouth of a person having a seizure. With these medications, we tell them to slip something in the side of their cheek or under their tongue. That can be conflicting to the point that in an emergency, a caregiver may not know what to do.
Another potentially unclear aspect is when patients with epilepsy have multiple prescribed benzodiazepines and have a seizure. They and their caregiver may not know which one to use. Messages may not be as clear, quick, or easy to follow in an emergency as they should.
Finally, and this is not always addressed during office visits, it is important to begin engaging trainees and advanced practice providers in educational settings to ensure this is covered during initial office visits.
Practice Gaps?
Danielle Becker, MD, MS, FAES:
Examining practice gaps, we see deficiencies in discussing SAPs and the use of seizure rescue medications. For example, how are adult vs pediatric patients with epilepsy managed acutely for their seizures? There are various approaches that may be better suited to different age groups and different populations with different demands.
For children, especially those in schools and summer camps, SAPs are required. They are also often required in group home settings. But it is also important to have SAPs within a work environment, especially to determine if rescue medication needs to be given or if 911 needs to be called. This is especially helpful for individuals who may not see seizures often or know what to do.
We know that a lack of knowledge about when or how to develop and implement an SAP and the use of seizure medications exists. Regarding practice gaps and education gaps, it is on the HCP side, but also on those with epilepsy. It falls on HCPs to support this education and ensure that people with epilepsy understand the importance of an SAP, a rescue medication, and what it can mean for their lives and quality of life.
We also know that there are differences in training programs for managing seizure emergencies. In some programs, residents do not necessarily receive education on SAPs and rescue medications; these should be included in every neurology program nationwide.
Sometimes, there are differences in practice between general neurologists and epilepsy centers, but the bottom line is that we want to increase education for all HCPs who see people with epilepsy, promoting awareness of seizure clusters, seizure emergencies, and appropriate management for patients in these circumstances.
Sarah Weatherspoon, MD:
In some cases, seizure emergency medication may also be provided by a primary care physician, like a pediatrician, or by an ED physician. Therefore, promoting information about the danger of prolonged seizures and cluster seizures to all HCPs is critical.
Who Is the Ideal Candidate for Rescue Medication?
Danielle Becker, MD, MS, FAES:
We discussed who the ideal candidate is for an SAP, and that goes hand in hand with who is the ideal candidate for a rescue medication: anyone who has a history of seizure clusters, acute repetitive seizures, prolonged seizures, seizures different than their baseline pattern, or status epilepticus, especially convulsive status epilepticus. But what about those patients who are seizure free for over a year, but live in fear of when that next seizure could start at any time?
SAPs go hand in hand with the seizure rescue medications because in the action plan, you are telling them what to do in this emergency, that is, using an intervention like a seizure rescue medication to try to stop the seizure as soon as possible, preventing prolonged seizure,22 status epilepticus, accumulated cognitive/structural changes over time and, in turn, improving overall quality of life.
Sarah Weatherspoon, MD:
Always keep in mind that seizure patterns can change over time, and we see this particularly in our pediatric population. Seizures that were previously well controlled may become uncontrolled, for example, as patients move through puberty.
We see this in some adult patients as well, where their seizure type may change over time, especially if they have multifocal epilepsy, like in the setting of tuberous sclerosis complex, or an epilepsy syndrome like Lennox-Gastaut syndrome. We know seizure patterns and types can change over time, shifting from more atonic seizures early in life to more convulsive seizures in adulthood. The SAP has to be ready to accommodate the unexpected changes that can occur with epilepsy, and we need to anticipate them.
Danielle Becker, MD, MS, FAES:
This is another place to stress again that SAPs are not one and done. They need to be revisited and modified as seizure and epilepsy characteristics change and as patients age and/or life factors change.
Thought question: When is the ideal time to use a rescue medication?
Sarah Weatherspoon, MD:
Even though status epilepticus may have a definition of a seizure lasting 5 minutes or longer, that does not mean that is when the rescue medication should be given. These are 2 different questions, although they are clearly linked.23 Some people may say immediately after a seizure starts. Some people may provide a time-based definition, such as after 2 minutes, 3-5 minutes, or 5 minutes, and there is considerable variability in how HCPs may counsel their patients.
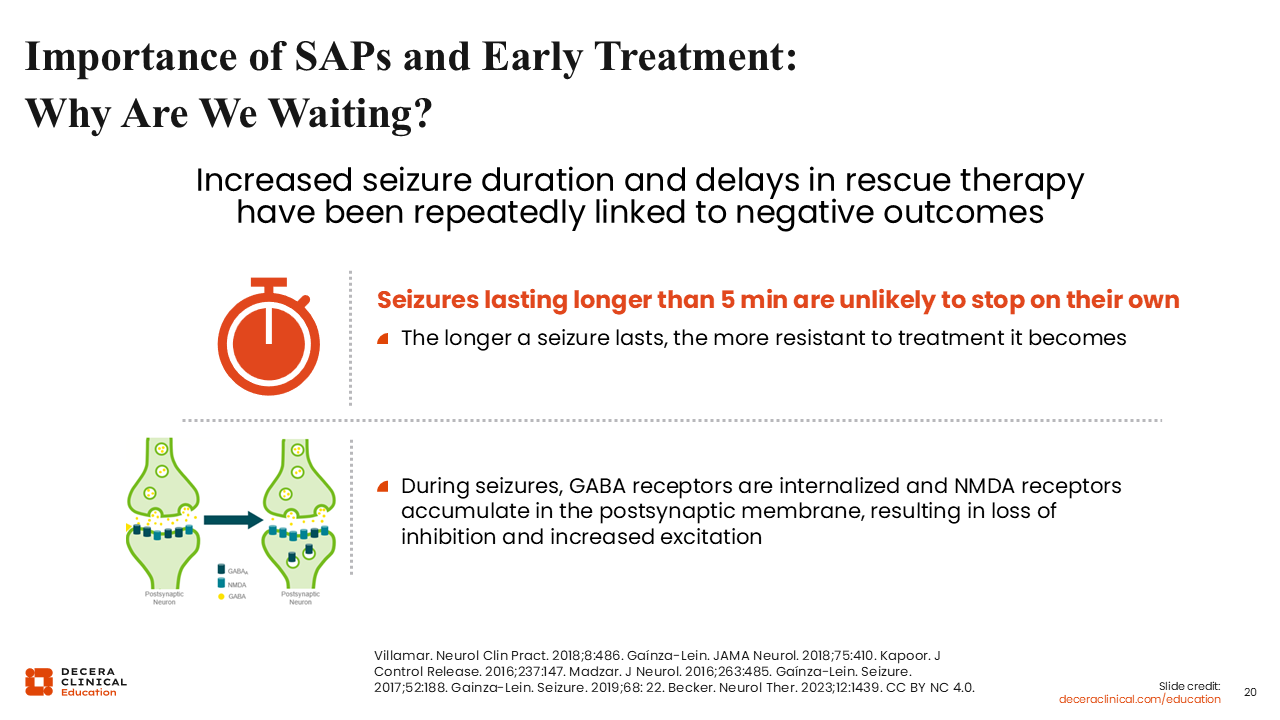
Importance of SAPs and Early Treatment: Why Are We Waiting?
Sarah Weatherspoon, MD:
Early treatment is important for preserving brain function. Seizures lasting longer than 5 minutes are unlikely to stop spontaneously and become increasingly resistant to treatment.24 At a physiological level during seizures, GABA receptors, which are part of our primary inhibitory neurotransmitter system, become internalized within the synapse of the neuron. The receptors are unavailable at the terminal to bind GABA once it is present, attempting to stop or inhibit the seizure. Instead, NMDA receptors, which are responsive to glutamate, part of our primary excitatory neurotransmitter system, accumulate in the postsynaptic membrane. The balance between inhibition and excitation becomes markedly skewed toward excitation during prolonged seizures.25
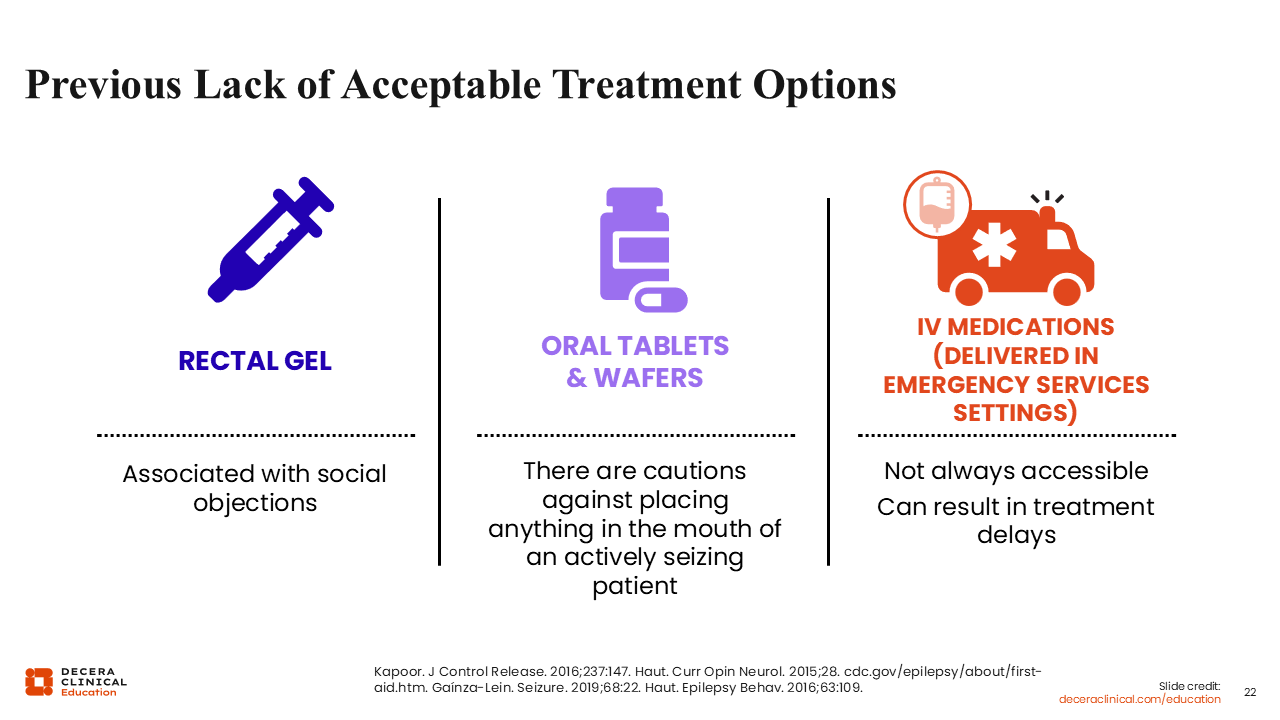
Previous Lack of Acceptable Treatment Options
Danielle Becker, MD, MS, FAES:
It is important to note that up until 2019, the only FDA-approved rescue medication was rectal diazepam. However, rectal gel can have social objections, particularly among children, adolescents, and adults in a work setting.
What did we do as HCPs before 2019? From an adult epileptologist’s perspective, I was often prescribing medications that were not approved by the FDA to treat seizure clusters or seizure emergencies, like clonazepam or lorazepam.26,27 I was also sending mixed messages because I would tell them to put their loved ones on their side, put something soft under their head, and not to put anything in their mouth. But, when I reviewed the SAP, I would recommend to slide the clonazepam tablet in the side of their cheek. That sends a confusing message.
Finally, intravenous medications that are tried and true and shown to stop seizure emergencies were not always available, especially in the home setting, and that could result in treatment delays and negative outcomes.24
Sarah Weatherspoon, MD:
In addition, with off-label medications, the administered dose does not necessarily equal the absorbed dose. Some of the medication may be aspirated or not fully enter the mouth if it comes out with saliva. Also, not all of them cross the blood-brain barrier well.
Where Are We Now?
Sarah Weatherspoon, MD:
There are now 3 FDA-approved medications for seizure rescue.
The first, which we have already mentioned, is rectal diazepam, which was approved by the FDA on July 29, 1997, as a rescue therapy for acute repetitive seizures. This approval allowed, for the first time, at-home administration of diazepam to control severe epileptic seizures by nonmedical caregivers, potentially avoiding ED visits in people 2 years of age or older.
Second, we have nasal diazepam, the same molecule administered via a nasal device and absorbed through the nasal mucosa; it is also approved for people aged 2 years or older.
The third is nasal midazolam, a different molecule, also given nasally through a device and absorbed through the nasal mucosa, and approved for people 12 years of age or older.
Currently under investigation, there is inhaled alprazolam, which is a different benzodiazepine, given via yet another novel route.
When we are considering which one to prescribe to the person with epilepsy we see in clinic, we need to consider several aspects. One is patients’ preference: nasal or rectal administration. What is right for them? What is the easiest to use? This may come down to their living and social situation. What is their body habitus? What is actually feasible for a caregiver to give? Then, finally, what are the pharmacokinetics of these molecules? They are all benzodiazepines, so they are all GABA receptor agonists, activating the inhibitory neurotransmitter system, but there are variations in absorption and half-life to take into consideration.
Differential Characteristics of Pharmacologic Options
Sarah Weatherspoon, MD:
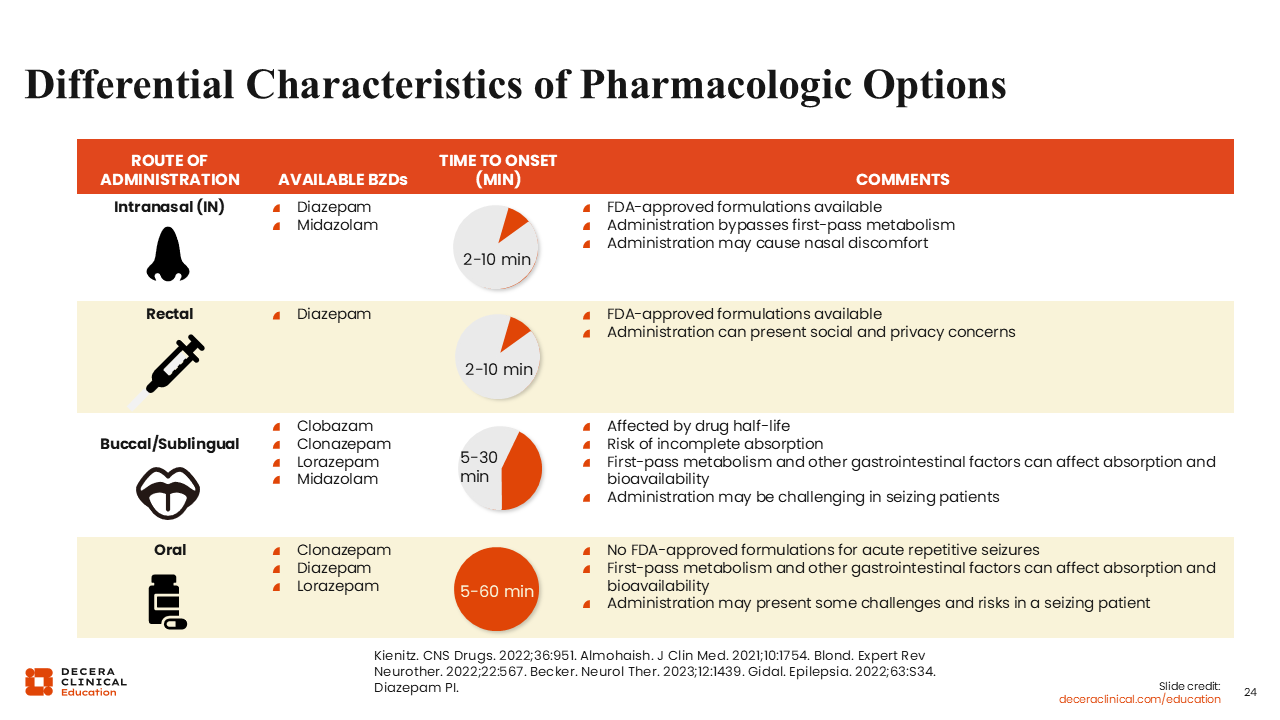
Variability in the molecule and route of administration leads to differences in time to onset and other nuances across the available options.28
Intranasal is the newest route of administration for which we have diazepam and midazolam, both approved by the FDA. The time to onset, which approximately corresponds to seizure termination, is 2-10 minutes.
They both have the benefit of bypassing first-pass metabolism, meaning that they are not absorbed through the gastrointestinal tract and therefore do not undergo any metabolism from the gastrointestinal tract or pass through the liver before getting to the site of action. They may cause nasal discomfort.
The second route is rectal, with the only currently approved molecule being rectal diazepam, and its onset is 2-10 minutes. In addition, in this case, there is variability in absorption, and there are social and privacy concerns about that route of administration.
A third route of administration is buccal and sublingual, which applies to several molecules. For instance, clobazam is available as a dissolvable oral film. However, this is a medication with a long half-life and often is not ideal for when you are dealing with an emergency. We have clonazepam dissolvable tablets that, like conventional tablets, carry the risk of incomplete absorption and a slightly longer half-life. As third-choice and fourth-choice buccal/sublingual options, lorazepam and midazolam tend to have shorter onset times but may not be completely absorbed from their available formulations and may undergo first-pass metabolism, ultimately leading to delayed onset of action. This administration may be particularly difficult to achieve in seizing patients when attempting to place a liquid or tablet into their mouth; the jaw may be clenched, and there may be excessive salivation. It should be kept in mind that none of these is approved by the FDA as acute seizure treatment, but rather as long-term treatment of seizures.
Finally, we have oral administration, again not approved for by the FDA acute repetitive seizures, which is also subject to first-pass metabolism, and presents the challenge of placing it in the oral cavity during a seizure. In addition, this route of administration leads to a much longer time to onset of up to an hour.
Benefits of Nasal Over Rectal Administration?
Sarah Weatherspoon, MD:
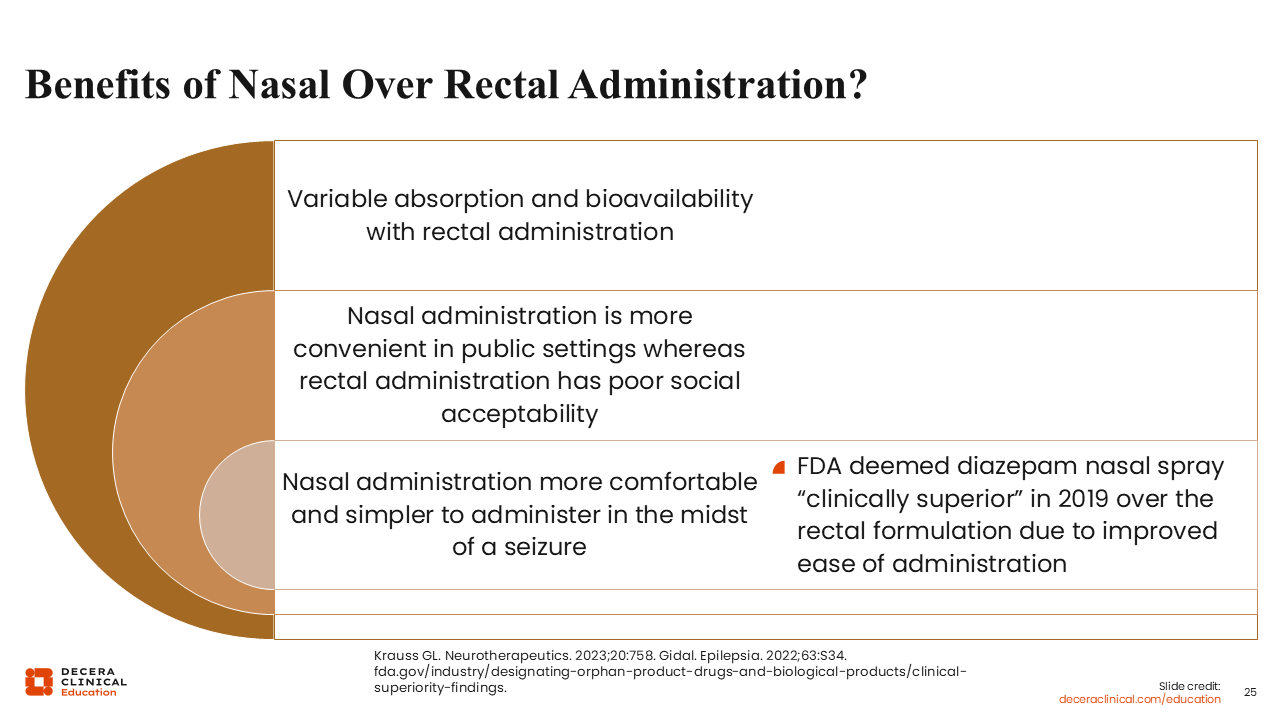
What are the benefits of nasal administration over rectal administration?
With rectal administration, absorption and bioavailability differ. For example, the intranasal formulation of diazepam is nearly equivalent to that of its intravenous counterpart, and the same is not necessarily true for the rectal formulation.
Nasal administration is also more convenient, particularly in public settings where rectal administration may have poor social acceptability, and it is more comfortable and simpler to administer during a seizure. This can be especially important for patients who may have a larger body habitus, may have physical limitations like cerebral palsy or contractures, or may also be predominantly using a wheelchair for mobility where it becomes more difficult for a caregiver to put them in a proper position on their side on a flat surface to administer a rectal medication. All these factors led the FDA to deem intranasal diazepam clinically superior to the rectal formulation when it was approved in 2019.
Take-home Message
Sarah Weatherspoon, MD:
An SAP is essentially a personalized, written “what to do” guide for seizures. It should describe what the person’s seizures typically look like and provide clear, practical steps that others can follow. Since many seizures affect awareness, it is often a caregiver or someone nearby (a parent, spouse, teacher, school nurse, friend, or coworker) who gives the rescue medication. The goal is that if a seizure happens, the SAP is easy to find and easy to use, even for people who do not manage seizures frequently.
A key takeaway is to think ahead about where the SAP and rescue medication will be stored. That decision depends on the person and their routine. For some people, especially those who can still respond at the very beginning of a seizure, it may make sense to keep the SAP and medication with them so they can self-administer when appropriate. For others, it is more important that the plan be placed where others can access it quickly.
Make sure the people most likely to help are included. Caregivers are usually first, since they are often the ones administering rescue medication, particularly at home and overnight. Keeping patients safe at home can make a big difference in quality of life. For children, the school nurse is a crucial point of contact, and depending on school policies, medication may need to be stored in the nurse’s office. Beyond school, it is worth considering any setting where the child regularly spends time (after-school programs, camps, and even sleepovers) and sharing the SAP with the supervising adults if the family feels comfortable doing so.