CE / CME
Mechanism Matters: The Future of Targeted Treatments in Myasthenia Gravis
Nurse Practitioners/Nurses: 0.50 Nursing contact hour, including 0.50 hour of pharmacotherapy credit
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Released: May 26, 2026
Expiration: May 25, 2027

Activity
gMG Treatment Landscape: Where Targeted Agents Fit
Treatment goals in gMG include improving function, reducing exacerbations, minimizing treatment toxicity, and helping patients achieve sustained disease control. Traditional therapies remain foundational and useful, including pyridostigmine, corticosteroids, nonsteroidal immunosuppressants, IVIg, and plasma exchange.1
Targeted therapies add mechanism-specific options to this landscape. C5 and FcRn inhibitors act at different points in antibody-mediated disease and should be selected according to antibody status, disease phenotype, prior treatment response, safety considerations, route and cadence of administration, and patient preference.1-4

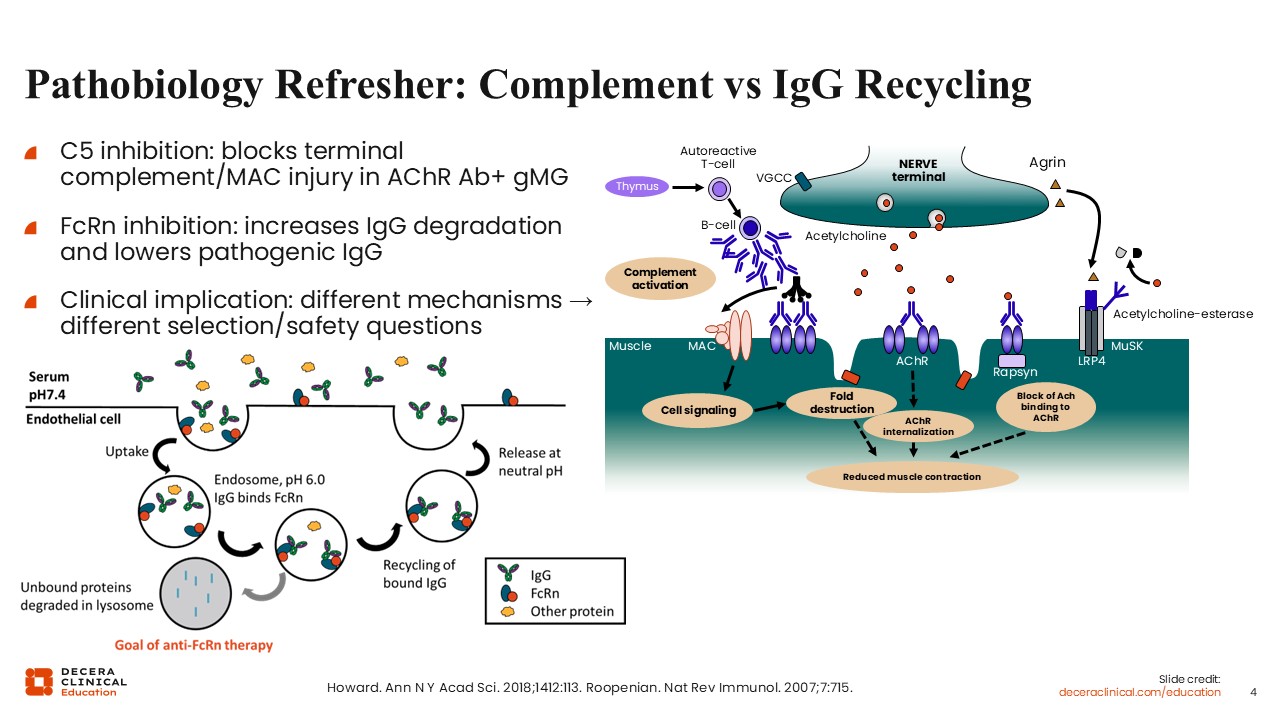
Pathobiology Refresher: Complement vs IgG Recycling
C5 inhibition and FcRn inhibition address different components of gMG pathobiology. In AChR antibody-positive gMG, pathogenic antibodies can activate complement at the neuromuscular junction, leading to membrane attack complex formation, postsynaptic injury, and impaired neuromuscular transmission. C5 inhibitors block terminal complement activation and, therefore, are mechanistically aligned with AChR antibody-positive disease.2,4,11
FcRn inhibitors work by reducing IgG recycling. FcRn normally protects IgG from degradation and returns it to the circulation. Blocking FcRn increases IgG degradation and lowers circulating IgG, including pathogenic autoantibodies. This mechanism differs from direct complement blockade and raises different clinical questions regarding antibody subtype, infection risk, IgG monitoring, and treatment cadence.11-13
This mechanistic distinction now has additional practical implications, as FcRn inhibition is supported by new data in anti-AChR antibody-negative adult gMG populations. Therefore, complement biology should still be presented as most directly aligned with AChR antibody-positive disease, and FcRn biology should be described as broader IgG lowering with agent-specific labeling by antibody subgroup.8,14,15
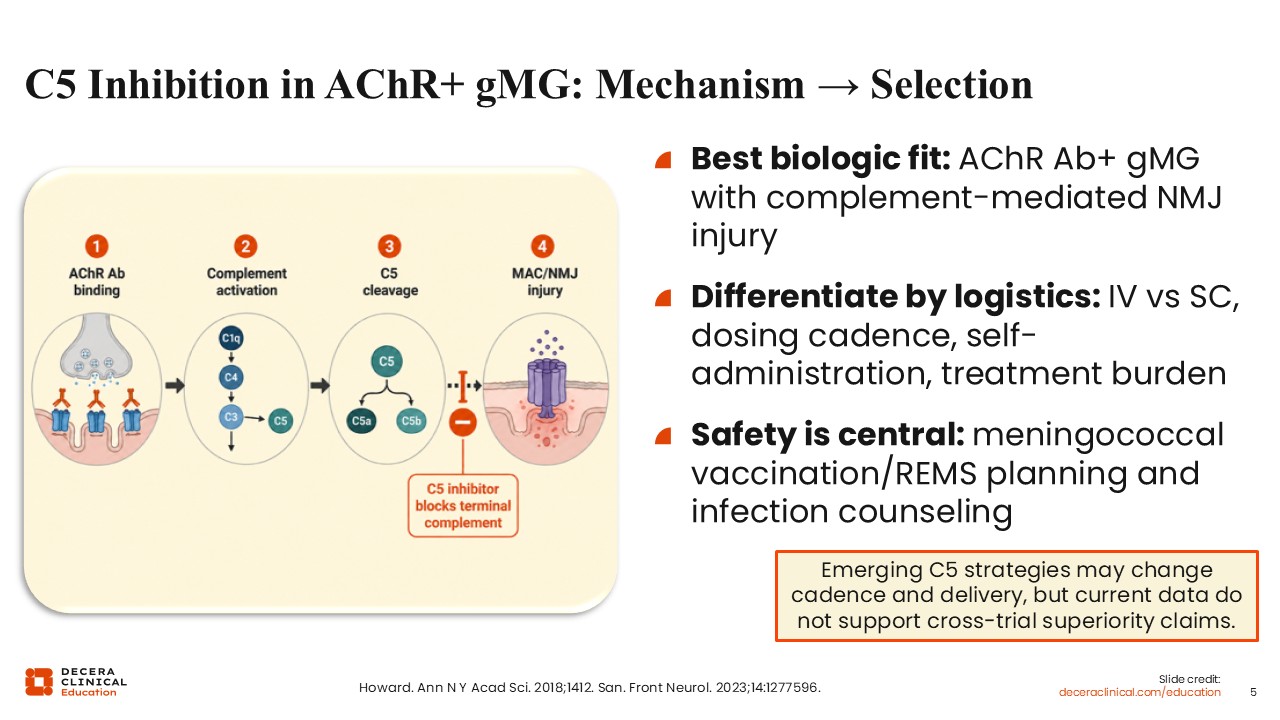
C5 Inhibition in AChR+ gMG: Mechanism to Selection
C5 inhibition has the most direct biologic fit in AChR antibody-positive gMG, where complement-mediated injury is a central driver of neuromuscular junction damage. By blocking terminal complement activation, C5 inhibitors reduce downstream formation of the membrane attack complex and help protect the postsynaptic membrane.2,11
Clinical selection, however, depends on more than mechanism. Approved and emerging C5 inhibitors differ by regulatory status, including use in childhood, intravenous (IV) vs subcutaneous(SC) administration, frequency of dosing, self-administration potential, vaccination requirements, and treatment burden. Meningococcal risk mitigation remains central to safe use, and emerging C5 strategies should be interpreted within their own trial contexts rather than through unsupported cross-trial ranking.5-7,16-18
Not all complement-directed strategies have translated favorably to the clinic. Recent negative phase II data with vemircopan, an oral factor D inhibitor, help prevent overgeneralization from successful terminal C5 blockade to all complement-pathway strategies. In that AChR antibody-positive gMG trial, vemircopan did not significantly differ from placebo on the primary or secondary efficacy endpoints, and the study was terminated because the prespecified efficacy threshold was not met.16
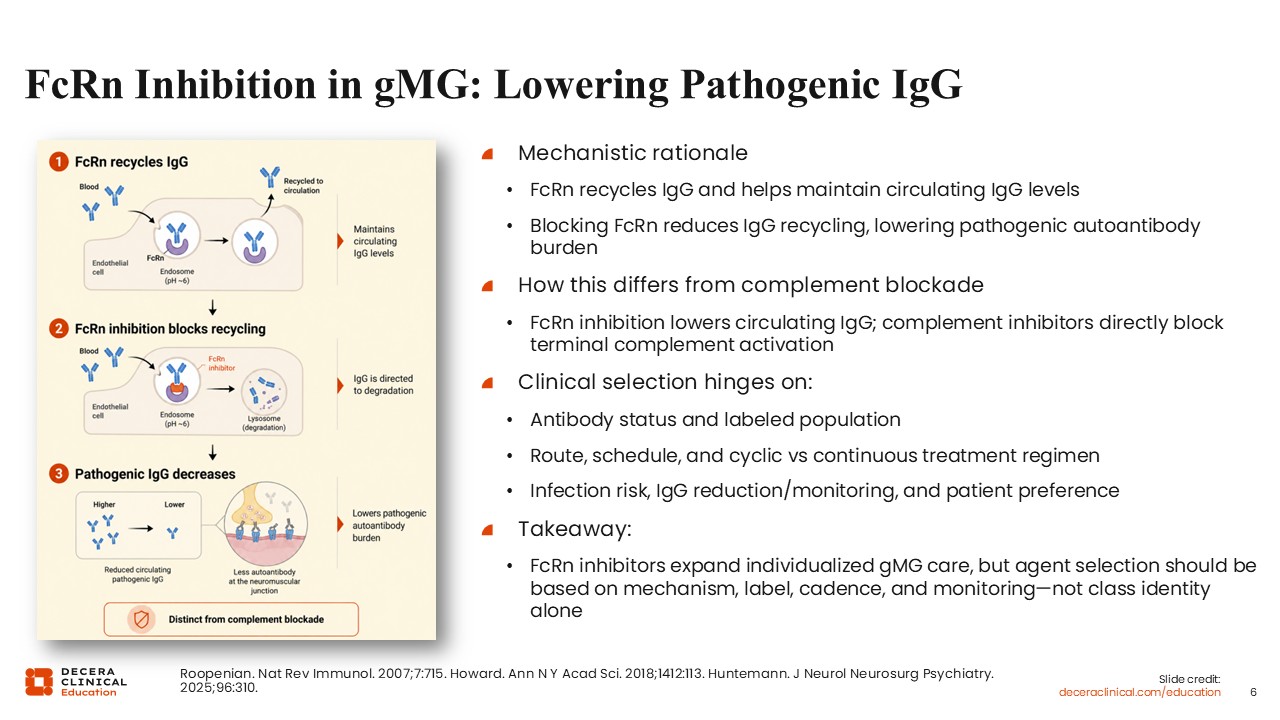
FcRn Inhibition in gMG: Lowering Pathogenic IgG
FcRn inhibition provides a distinct targeted strategy in gMG by lowering circulating IgG, including pathogenic autoantibodies. FcRn normally rescues IgG from lysosomal degradation; inhibition of FcRn accelerates IgG catabolism and reduces autoantibody burden.11,12
This mechanism expands individualized treatment selection beyond complement blockade. FcRn inhibitors differ by labeled antibody population, route of administration, cyclic vs continuous treatment regimens, endpoint timing in pivotal trials, and monitoring considerations. Efgartigimod is now an adult gMG option with evidence in both AChR antibody-positive and AChR antibody-negative populations, including MuSK-positive, LRP4-positive, and triple-seronegative subgroups. Rozanolixizumab is labeled for adult AChR antibody-positive or MuSK antibody-positive gMG, and nipocalimab is labeled for AChR antibody-positive or MuSK antibody-positive gMG in adults and pediatric patients aged 12 years or older. Infection risk, IgG reduction, vaccination planning, and patient preference should be incorporated into therapy selection.8-10,13-15,19-21
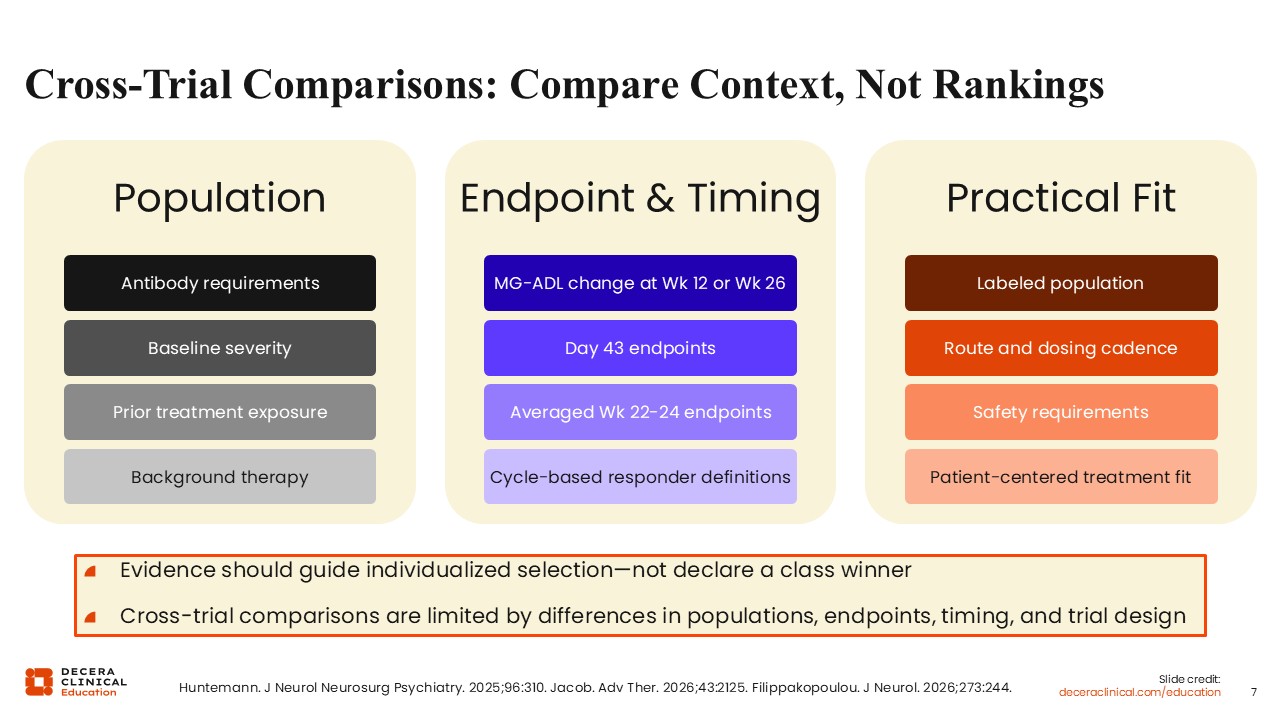
Cross-Trial Comparisons: Compare Context, Not Rankings
Cross-trial comparisons across C5 inhibitors and FcRn inhibitors require caution. Pivotal trials differ in antibody requirements, baseline severity, prior treatment exposure, background therapies, endpoints, and timing of assessment. MG-ADL change at Week 12, Week 24, or Week 26 should not be interpreted as equivalent to Day 43 outcomes, averaged Week 22-24 outcomes, or cycle-based responder endpoints.13,22,23
The more clinically useful approach is to compare trial context rather than declare a class or agent winner. Evidence should be interpreted according to the enrolled population, endpoint definition, timing, route and cadence of therapy, safety requirements, and practical fit for the patient.13,22,23
Such caution is increasingly important because newer datasets use different endpoint structures and timepoints: NIMBLE evaluated cemdisiran-based C5 suppression at Week 24; PREVAIL evaluated gefurulimab at Week 26; ADAPT SERON evaluated efgartigimod in AChR antibody-negative adult gMG; and Vivacity-MG3 evaluated nipocalimab using averaged MG-ADL change across Weeks 22-24. These data are clinically meaningful but should not be converted into cross-trial rank ordering.8,10,15,17,18
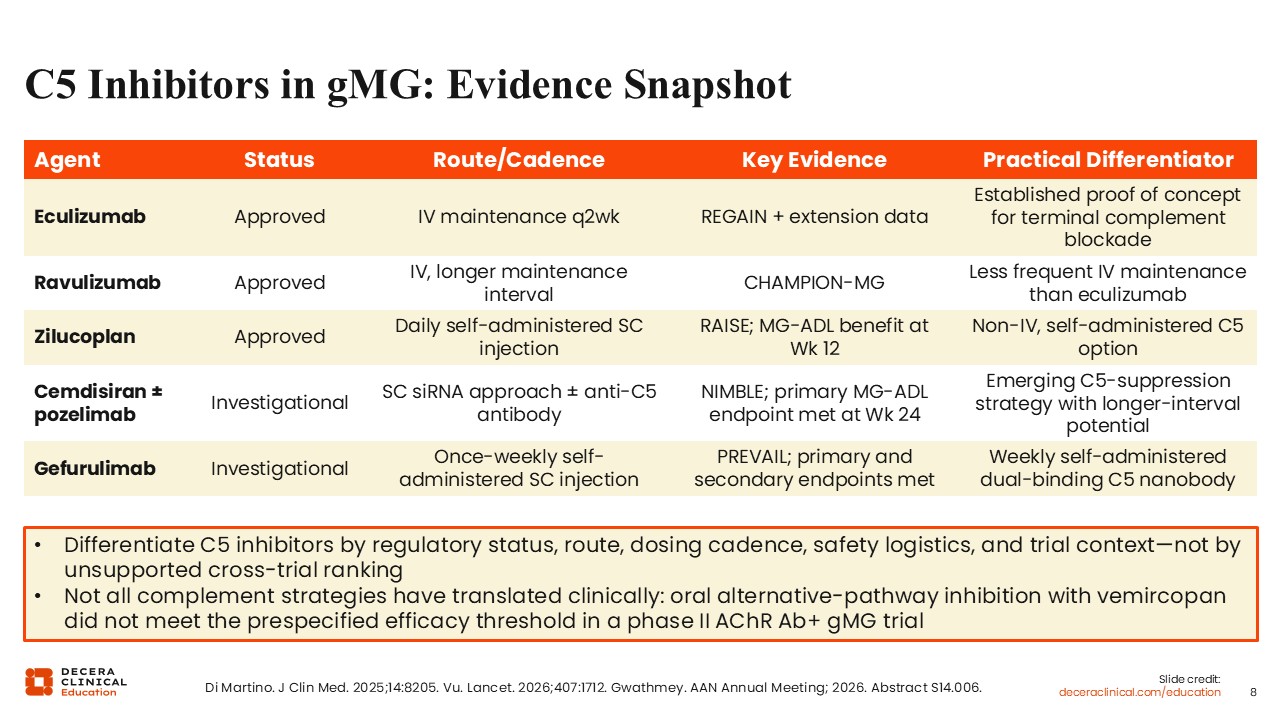
C5 Inhibitors in gMG: Evidence Snapshot
Approved C5 inhibitors have established terminal complement blockade as an important strategy in AChR antibody-positive gMG. Eculizumab provided proof of concept for terminal complement inhibition in the REGAIN trial program. Ravulizumab extended the approach with a longer IV maintenance interval. Zilucoplan introduced a daily self-administered SC C5 inhibitor option with demonstrated MG-ADL benefit at Week 12.5-7,16,24,25
Emerging C5-directed therapies may further change the practical profile of complement inhibition. Cemdisiran, with or without pozelimab, represents an investigational siRNA-based strategy to reduce C5 production. In NIMBLE, cemdisiran dosed subcutaneously every 12 weeks met the Week 24 MG-ADL primary endpoint, with least squares mean change -4.5 vs -2.2 with placebo and a placebo-adjusted difference of -2.3; quantitative myasthenia gravis (QMG) score also improved. Gefurulimab is an investigational dual-binding C5 nanobody designed for once-weekly self-administered SC dosing; PREVAIL reported a Week 26 MG-ADL treatment difference of -1.6 vs placebo. These approaches differ by mechanism, cadence, and delivery, but available data do not support head-to-head efficacy ranking across agents. By contrast, vemircopan, an oral factor D inhibitor, did not meet the prespecified efficacy threshold in a phase II AChR antibody-positive gMG trial, underscoring that complement-directed strategies are not interchangeable. The phase III NIMBLE trial results were published in The Lancet and presented in an oral plenary session at American Academy of Neurology 2026; cemdisiran monotherapy has also been submitted for US regulatory review.16-18,26
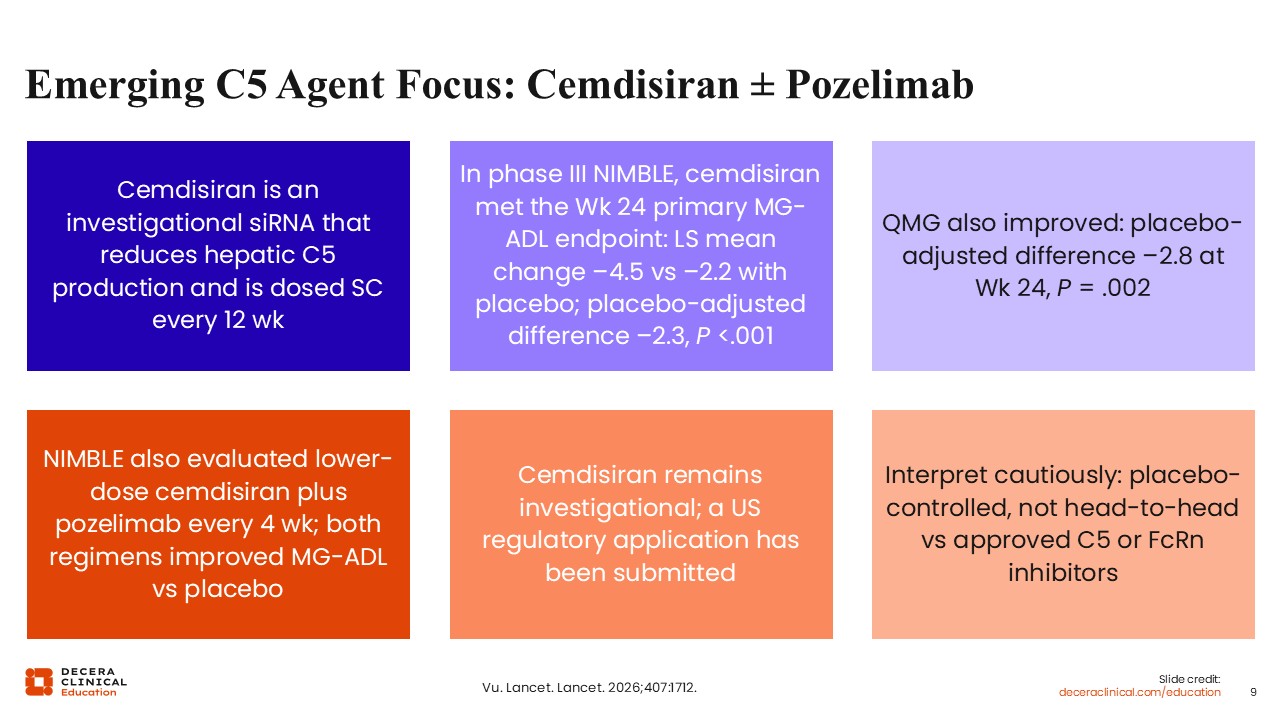
Emerging C5 Agent Focus: Cemdisiran with or without Pozelimab
Cemdisiran is an investigational siRNA that reduces hepatic C5 production and is administered subcutaneously every 12 weeks. In the phase III NIMBLE trial in adults with AChR antibody-positive and/or LRP4 antibody-positive gMG, cemdisiran met the Week 24 primary MG-ADL endpoint vs placebo, with least squares mean MG-ADL change -4.5 vs -2.2 with placebo and placebo-adjusted difference -2.3. QMG also improved, with placebo-adjusted difference -2.8 at Week 24. The study also evaluated lower-dose cemdisiran plus pozelimab every 4 weeks, and both regimens improved MG-ADL vs placebo.17
In addition to meeting the Week 24 primary and key secondary endpoints, cemdisiran demonstrated clinically meaningful MG-ADL improvement within 2 weeks, with benefits deepening over time and sustained through Week 24. NIMBLE also provides an important mechanistic insight: Cemdisiran monotherapy achieved robust clinical benefit without complete terminal complement blockade, whereas cemdisiran plus pozelimab achieved near-complete complement inhibition but did not numerically outperform cemdisiran monotherapy across gMG-specific outcomes.17
The trial also included a pozelimab monotherapy arm. Pozelimab monotherapy did not show significant benefit vs placebo, as expected, supporting cemdisiran monotherapy as the regimen submitted for regulatory review while preserving the scientific relevance of cemdisiran plus pozelimab for understanding C5 suppression and complement biology.17
These data are clinically relevant because they suggest that C5 suppression may be achievable through a mechanism distinct from direct monoclonal antibody blockade of circulating C5. Cemdisiran results should be interpreted as placebo-controlled trial data rather than evidence of superiority over approved C5 inhibitors or FcRn inhibitors. A US regulatory application has been submitted for cemdisiran monotherapy, but cemdisiran remains investigational at this point.17
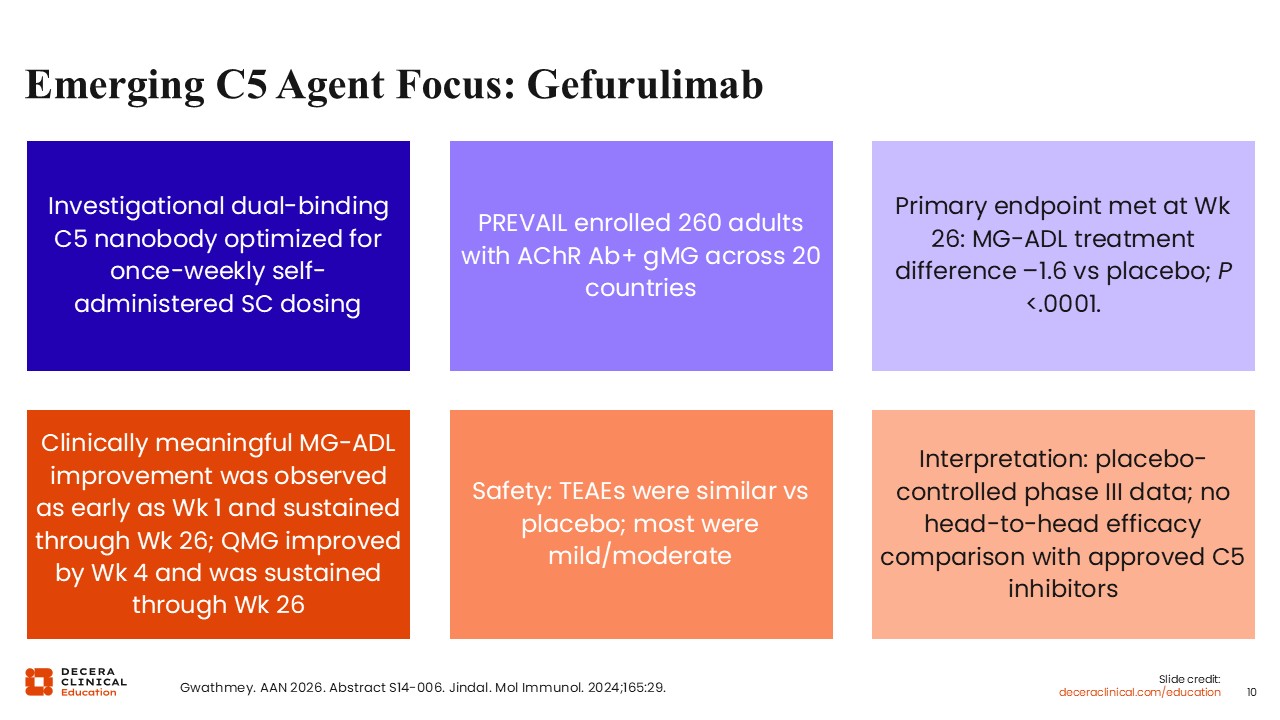
Emerging C5 Agent Focus: Gefurulimab
Gefurulimab is an investigational dual-binding C5 nanobody optimized for once-weekly self-administered SC dosing. In the phase III PREVAIL study, which enrolled adults with AChR antibody-positive gMG, gefurulimab met the primary endpoint at Week 26, with an MG-ADL treatment difference of -1.6 vs placebo. Improvement was observed early and sustained through Week 26, with QMG improvement also reported.18,26
The potential clinical relevance of gefurulimab lies not only in efficacy but also in its route and administration model. A once-weekly self-administered complement inhibitor could reduce clinic-based treatment burden for selected patients. Until full peer-reviewed publication is available, interpretation should remain tied to the placebo-controlled phase III context and should not imply comparative superiority vs approved C5 inhibitors.18
Evidence Snapshot: FcRn Inhibitors in gMG
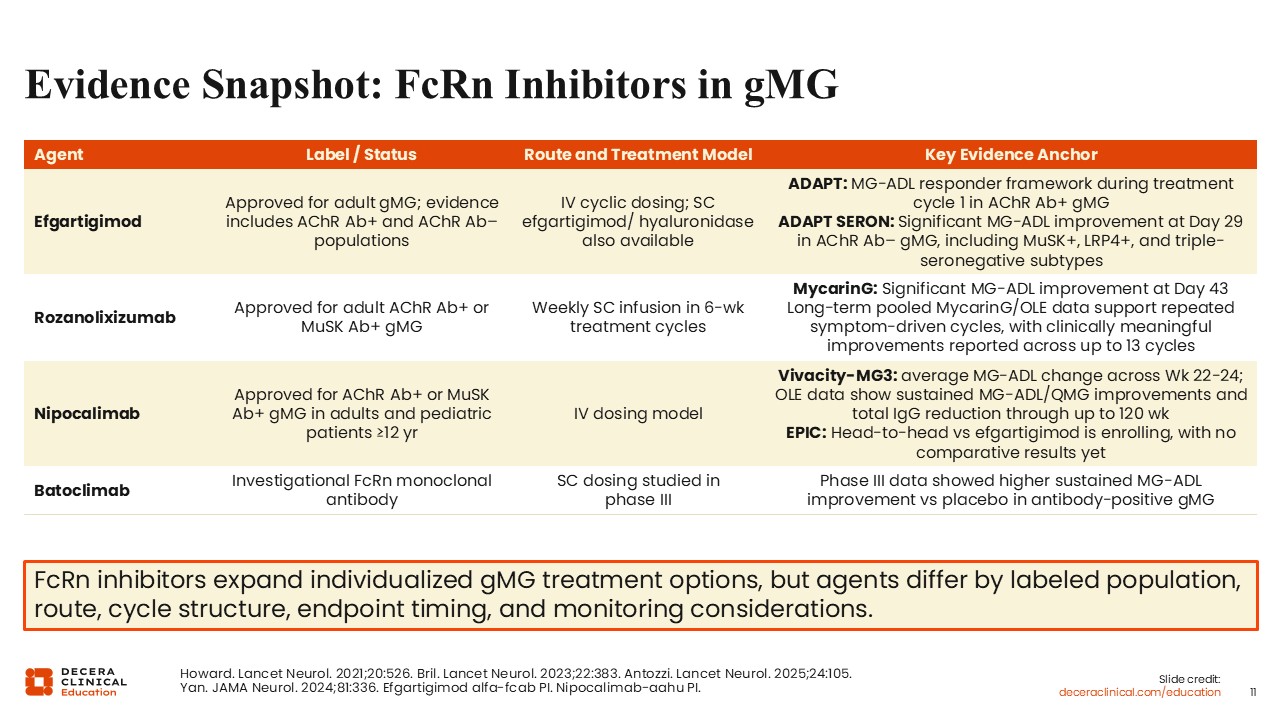
FcRn inhibitors have become an important targeted treatment class in gMG by reducing pathogenic IgG. Efgartigimod established the FcRn approach through the ADAPT trial in AChR antibody-positive gMG and is available in IV and SC formulations. A key update is that efgartigimod now has adult gMG labeling supported by evidence in both AChR antibody-positive and AChR antibody-negative populations; ADAPT SERON included MuSK antibody-positive, LRP4 antibody-positive, and triple-seronegative subgroups.8,14,21
Rozanolixizumab demonstrated significant MG-ADL improvement in MycarinG and is administered as weekly SC infusions in treatment cycles. It is labeled for adult AChR antibody-positive or MuSK antibody-positive gMG. Nipocalimab demonstrated benefit in Vivacity-MG3 using an IV dosing model, with longer-term data supporting sustained MG-ADL and QMG improvement with IgG reduction. It is labeled for AChR antibody-positive or MuSK antibody-positive gMG in adults and pediatric patients aged 12 years or older.9,10,15,19
Batoclimab remains investigational and has shown higher sustained MG-ADL improvement vs placebo in phase III data, but the manufacturer has stated that it does not currently intend to seek regulatory approval for batoclimab in MG and is focusing instead on IMVT-1402. FcRn inhibitors should be differentiated by labeled population, route, treatment-cycle structure, endpoint timing, infection risk, IgG-lowering profile, and monitoring requirements.13,20,27
Emerging FcRn Agent Focus: Batoclimab
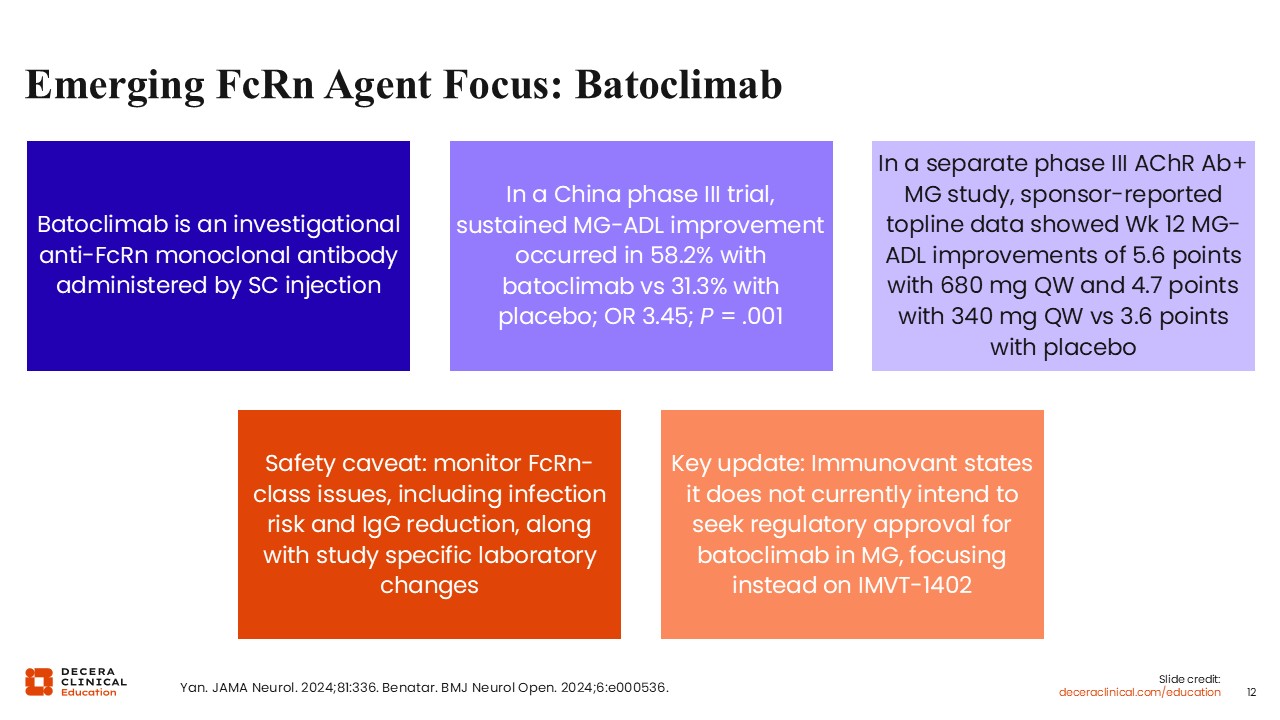
Batoclimab is an investigational anti-FcRn monoclonal antibody administered by SC injection. In a phase III trial in adults with gMG, sustained MG-ADL improvement occurred more frequently with batoclimab than placebo. Additional manufacturer-reported phase III data in AChR antibody-positive MG showed greater Week 12 MG-ADL improvement with batoclimab than placebo.20,27
Safety considerations are central to interpretation. As an FcRn inhibitor, batoclimab lowers IgG, requiring attention to infection risk and immunoglobulin monitoring, as with other FcRn-blocking agents. Current development strategy should be considered when discussing clinical relevance because the manufacturer has stated that it does not currently intend to seek regulatory approval for batoclimab in MG and is focusing instead on IMVT-1402.20,27
Comparing Safety: Infection, IgG Reduction, Vaccination, Monitoring
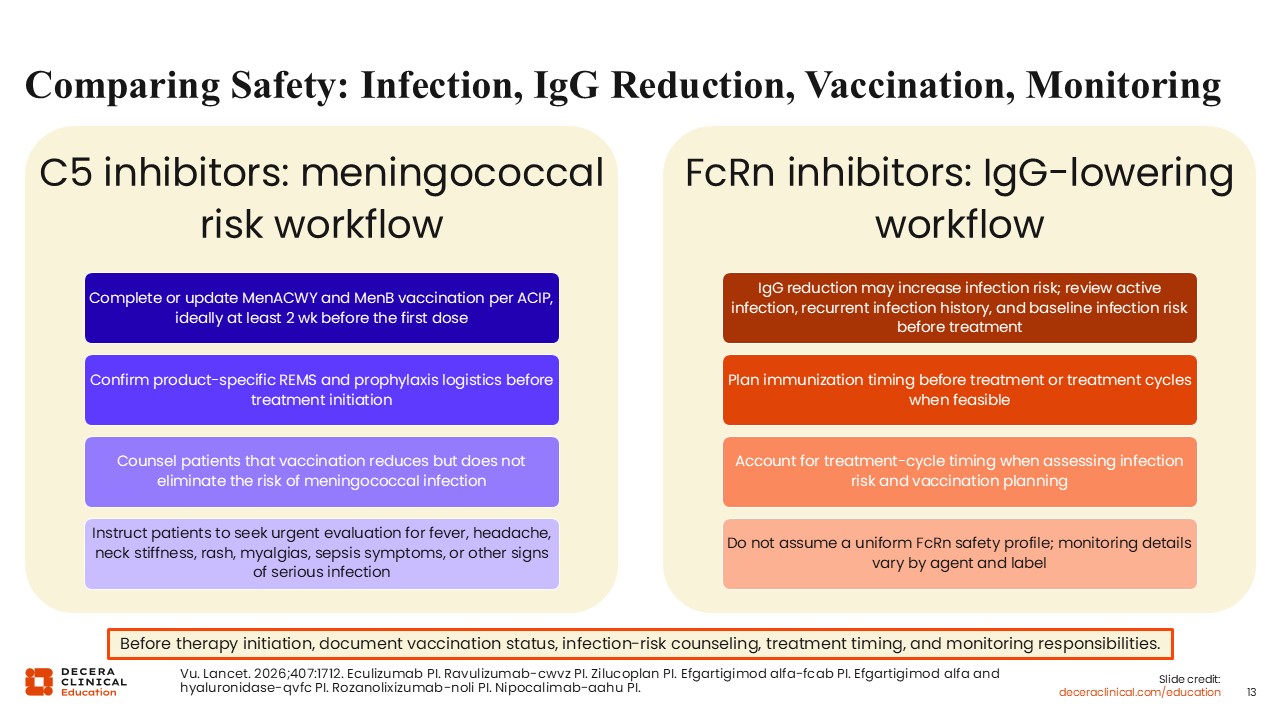
Safety planning should begin before targeted therapy is initiated. For C5 inhibitors, meningococcal risk mitigation is essential. MenACWY and MenB vaccination should be completed or updated according to Advisory Committee on Immunization Practices guidance, ideally at least 2 weeks before the first dose when feasible. Product-specific REMS requirements, prophylaxis logistics, and patient education should be addressed before treatment begins. Longer-term safety follow-up should continue to be interpreted as data mature. Patients should be counseled that vaccination reduces but does not eliminate risk of meningococcal infection.5-7,17
For FcRn inhibitors, the major safety consideration is IgG reduction and related infection risk. Active infection, recurrent infection history, baseline infection risk, and immunization timing should be reviewed before treatment or treatment cycles. Monitoring requirements vary by agent and label, so class-level assumptions are insufficient. Patients should receive clear instructions about symptoms that require urgent evaluation. FcRn safety planning should be agent specific because dosing model, IgG trajectory, vaccination timing, and monitoring expectations differ among efgartigimod, rozanolixizumab, nipocalimab, and investigational batoclimab.8-10,20,21
Administration Burden Is a Treatment-Selection Variable
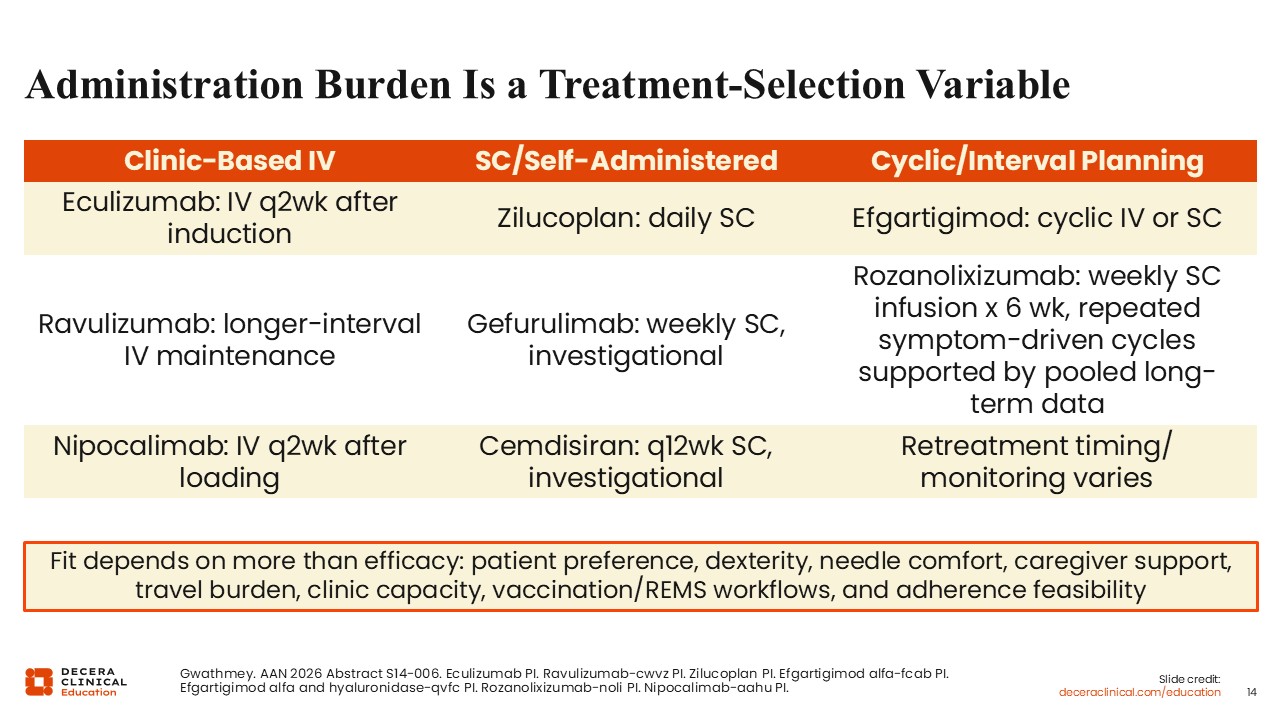
Administration burden is a clinically meaningful treatment-selection variable. Some targeted therapies require clinic-based IV administration, including eculizumab, ravulizumab, and nipocalimab. Other agents are SC or self-administered, including zilucoplan and efgartigimod/hyaluronidase SC, as well as investigational agents such as gefurulimab and cemdisiran. Rozanolixizumab is administered as weekly SC infusions in treatment cycles and should be distinguished from simple self-injection. FcRn inhibitors may also involve cyclic or interval-based treatment models, which affect retreatment planning and follow-up.5-10,17,18,21
Practical fit depends on patient preference, dexterity, needle comfort, caregiver support, travel burden, clinic capacity, payer access, adherence feasibility, and safety workflow requirements. A therapy that is biologically appropriate may still be poorly matched if the administration model or monitoring expectations are unrealistic for the patient.1,13
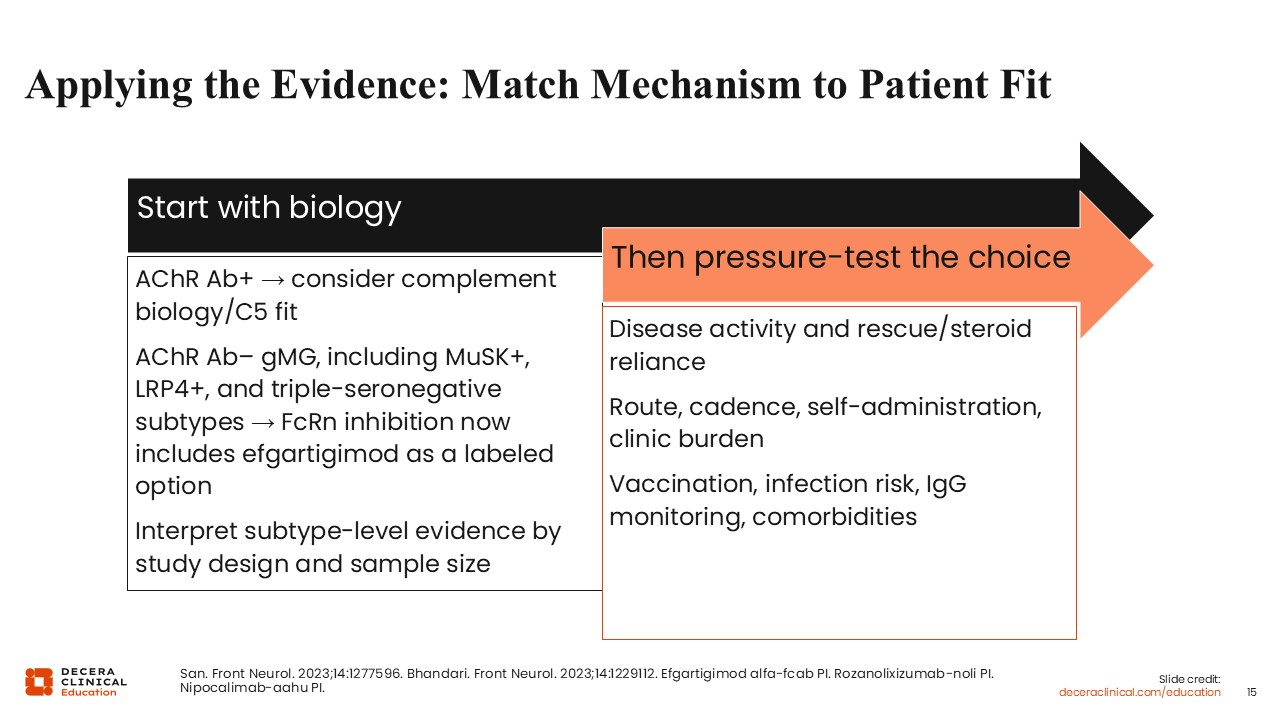
Applying the Evidence: Match Mechanism to Patient Fit
Treatment selection should begin with disease biology and labeled evidence. In AChR antibody-positive gMG, complement-mediated postsynaptic injury at the neuromuscular junction may make C5 inhibition an especially relevant strategy. In patients for whom broader IgG lowering is appropriate, FcRn inhibition may be the better mechanistic fit. Current FcRn labeling now includes efgartigimod as an adult gMG option with evidence in AChR antibody-positive and AChR antibody-negative populations, including MuSK antibody-positive, LRP4 antibody-positive, and triple-seronegative subgroups, as well as rozanolixizumab and nipocalimab for AChR antibody-positive or MuSK antibody-positive gMG.2,4,8-10
The choice then should be tested against clinical reality. Disease activity, exacerbation history, corticosteroid or rescue therapy reliance, comorbidities, infection risk, vaccination status, IgG-monitoring considerations, route and cadence of administration, and patient preference all influence treatment selection. Mechanism provides the framework; patient context determines the fit.1,13
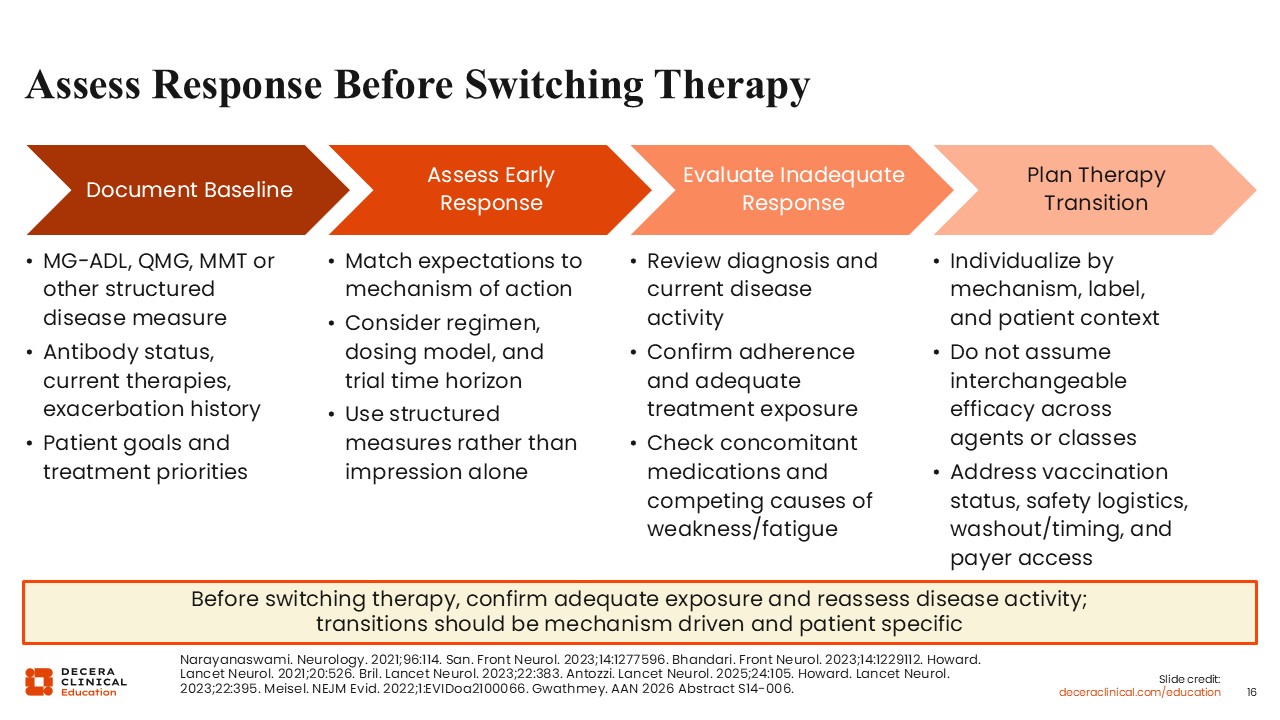
Assess Response Before Switching Therapy
Before switching therapy, healthcare professionals should confirm adequate treatment exposure and reassess disease activity using structured measures whenever possible. Baseline MG-ADL, Manual Muscle Testing, or QMG, antibody status, current therapies, exacerbation history, and patient treatment goals should be documented to support objective response assessment.1
If response is inadequate, diagnosis, adherence, dosing, concomitant medications, and competing causes of weakness or fatigue should be reviewed. Therapy transitions should be mechanism driven and individualized rather than based on assumptions of interchangeability. Vaccination status, infection risk, IgG monitoring, washout or timing considerations, payer access, and treatment logistics should be addressed before switching.1,2,4,13
Response expectations should be matched to each therapy’s mechanism and trial design. For example, efgartigimod outcomes are often interpreted in treatment cycles, rozanolixizumab pivotal data are anchored at approximately Day 43, nipocalimab uses averaged MG-ADL change across Weeks 22-24, zilucoplan is anchored at Week 12, and ravulizumab and gefurulimab are anchored at Week 26. These differences matter before declaring inadequate response or switching mechanisms.14,15,18,19,24,25
Clinical Bottom Line: Match Mechanism to Patient Context
C5 inhibition and FcRn blockade target different points in antibody-mediated gMG. C5 inhibitors directly interrupt terminal complement activation, with the clearest biologic and labeled fit in AChR antibody-positive disease. FcRn inhibitors lower circulating IgG, including pathogenic autoantibodies, and now include an adult seronegative gMG option following the efgartigimod label expansion and ADAPT SERON trial evidence.2,4,8,11,12
The practical goal is not to choose a winning class, but to match mechanism to patient context. Antibody status, safety requirements, route and dosing cadence, treatment burden, monitoring needs, pediatric vs adult labeling, and patient preference should guide selection. Newer evidence, including NIMBLE for cemdisiran, PREVAIL for gefurulimab, ADAPT SERON for efgartigimod, and the negative vemircopan phase II trial, should sharpen the mechanism-based framework without encouraging unsupported cross-trial rankings.8,13,16-18