CE / CME
Obesity Management Strategies for Patients With Suboptimal or No Response to Antiobesity Medications
Physician Assistants/Physician Associates: 0.25 AAPA Category 1 CME credit
Nurse Practitioners/Nurses: 0.25 Nursing contact hour
Physicians: maximum of 0.25 AMA PRA Category 1 Credit™
Released: September 30, 2025
Expiration: September 29, 2026

Activity
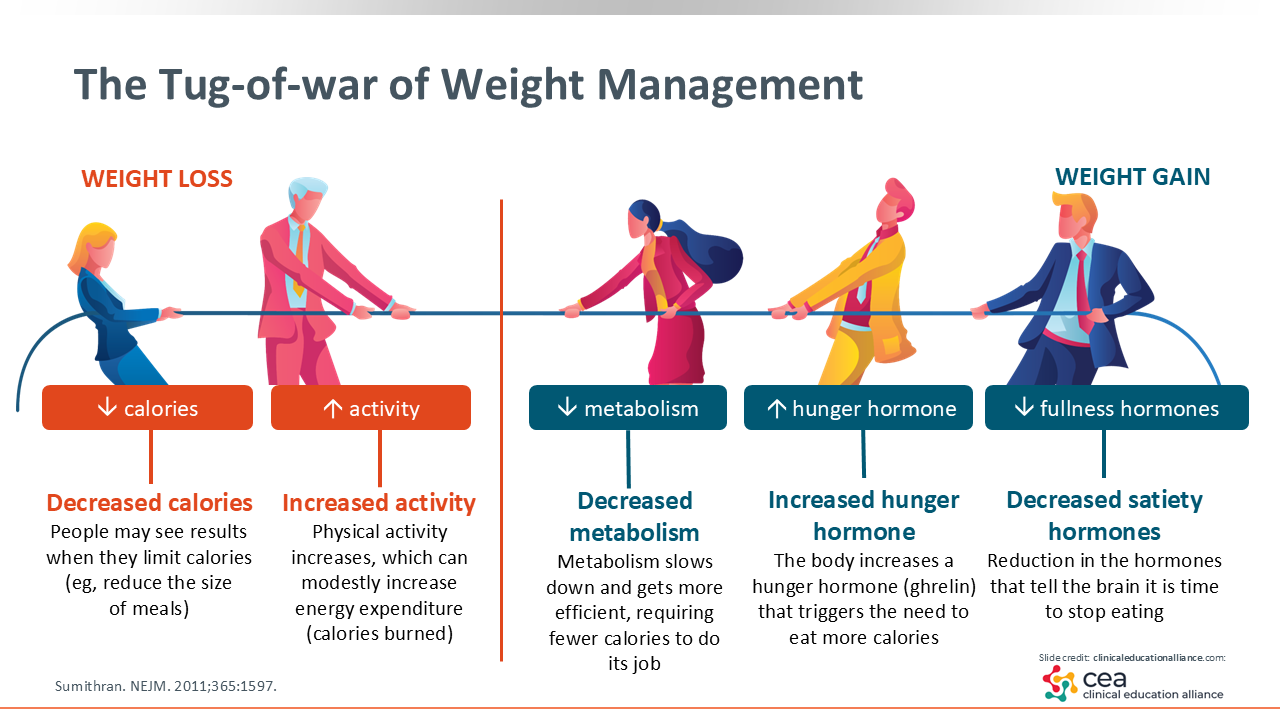
The Tug-of-war of Weight Management
The first thing I must discuss is the tug-of-war that occurs when patients try to lose weight. What I mean by “tug-of-war” is that there are opposing forces going on in the body’s physiology. In trying to lose weight, what patients must do is reduce their food intake and increase their physical activity to create a negative energy balance.
But what many patients do not realize is that this negative energy balance produces several physiologic effects within the body that fights their weight loss attempt. The first thing that happens when one enters that negative energy balance and starts to lose body fat is that a hormone called leptin falls rapidly. What that does is send signals to the brain that the body needs to be eating more and conserving energy. Next the appetite hormones that promote satiety decrease and the hunger hormones that make us want to eat increase. In addition, one’s metabolic rate decreases as their muscles become more efficient. This means that the body’s muscles require fewer calories to do their job. These signals in the body increase food intake, decrease the metabolic rate, and promote muscle efficiency. This intricate system fights the body’s ability to lose weight; that is why it is not easy to lose weight.1
Patients need to know about this tug-of-war because they frequently blame themselves for the inability to successfully lose weight and keep it off. Healthcare professionals (HCPs) should explain this ongoing tug-of-war that goes on when we try to control our weight. The body has an elaborate system to maintain its weight. When we try to thwart that, the body fights back.
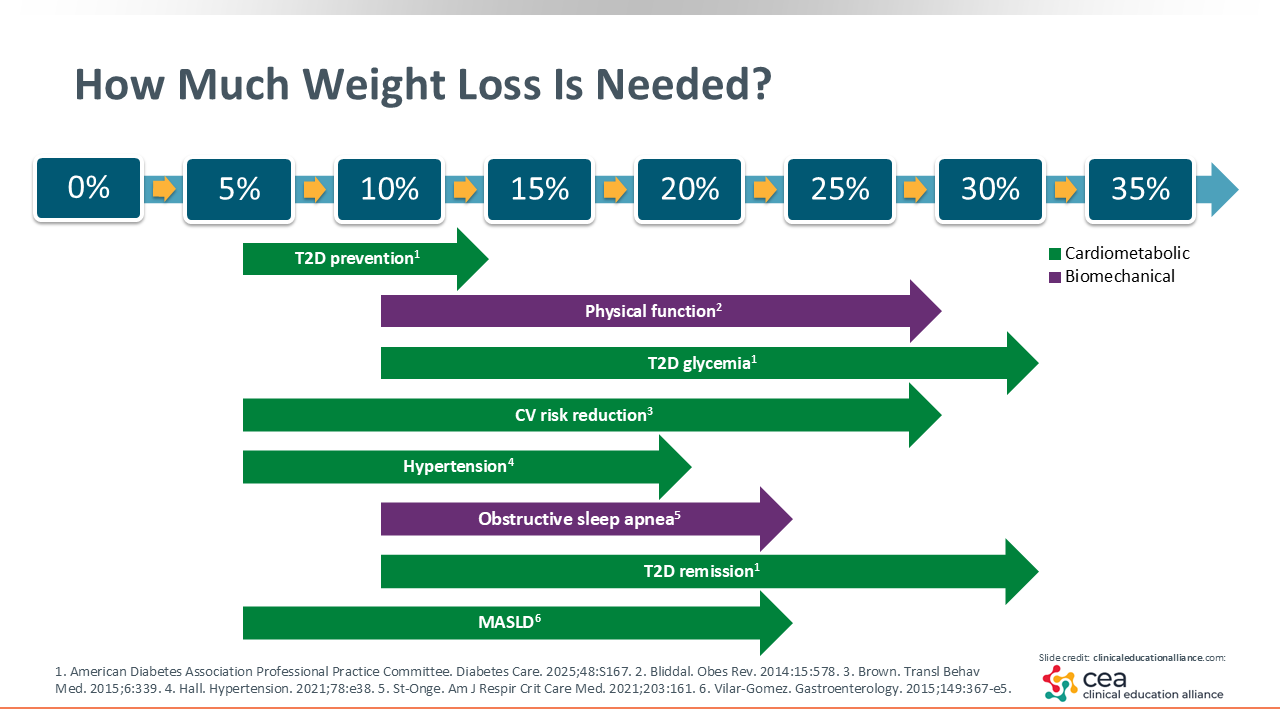
How Much Weight Loss Is Needed?
The good news is that patients do not need to achieve a so-called “normal” body weight or healthy body weight to receive health improvements with weight loss. Modest weight loss (3% to 5%) improves glycemia and triglyceride levels, although patients should aim for 5% to 10% weight loss to see improvements in their metabolic risk factors. Of note, approximately 7% of weight loss is all that is needed to prevent diabetes in those with prediabetes. Furthermore, patients can see great improvements in their blood pressure, cardiovascular risk factors, and/or histologic features of metabolic dysfunction–associated steatotic liver disease at that 5% to 10% weight loss range.2-4
But it is important to recognize that, yes, a little bit of weight loss is good; 5% to 10% total weight loss can produce some improvements and reduce many risk factors, but more weight loss is better. HCPs usually aim for 10% to 15% total weight loss in patients if we are trying to get their diabetes back into a normal glycemia or prediabetes state.
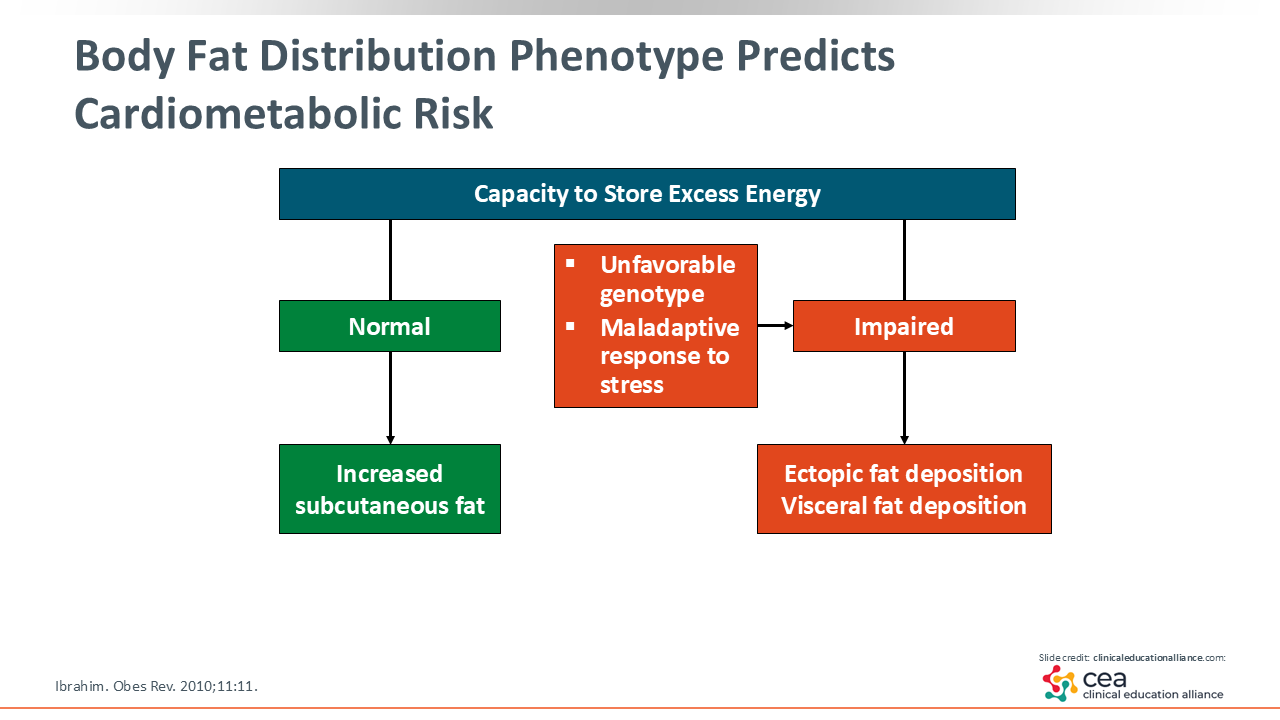
Body Fat Distribution Phenotype Predicts Cardiometabolic Risk
Obesity drives all these complications through 2 mechanisms. The first is cardiometabolic through its effect on blood pressure, lipid levels, inflammation, and dysglycemia. The other is biomechanical and considers the burden of excess body fat, which contributes to issues like gastroesophageal reflux disease, increased intra-abdominal pressure from too much fat in the abdomen, obstructive sleep apnea, and increased fat around the neck.5 Patients must achieve more weight loss (at least 10%) to improve those biomechanical risk factors. If we can get patients’ BMI down to approximately 27 kg/m2, we should see increased improvement in the biomechanical comorbidities of obesity.
Why do we even need body fat? It is important to our overall health. We need a certain amount of body fat because it has a cushioning effect. It also helps store energy for emergencies, such as when you are sick and cannot eat or are in an environment where food is scarce. The body needs extra calories stored for those instances.6 In addition, women need about 22% body fat to maintain their fertility.7 Therefore, we must recognize that body fat is not the enemy. Enough healthy body fat is a good thing.
It is when we go overboard and start exceeding our capacity to store energy in normal ways that leads to health risks and obesity. Furthermore, subcutaneous fat stores in the hips and thighs are great places to do that in women, which is fine. That does not hurt them. But what happens when we exceed our capacity to store fat subcutaneously? We start storing it within the abdomen (so-called visceral fat) and ectopically in certain organs like the heart, pancreas, liver, kidneys. This is incredibly bad for our health.8 Some patients also have an unfavorable genotype where they cannot store subcutaneous fat well naturally. A good example of this are our Asian populations. These folks are considered to have obesity once their BMI exceeds 23 kg/m2 for South Asian adults and 27 kg/m2 for Chinese people compared with a BMI of ≥30 kg/m2 for White populations.9
HCPs should use waist circumference to detect excess body fat. It more accurately measures the amount of visceral fat deposition in a person vs BMI and is a good surrogate to detect those who have body fat stored in places it does not belong.
Now unfortunately, some people are genetically predisposed to this and certain medications also can cause weight gain. The protease inhibitors used to treat HIV infection impair patients’ ability to store subcutaneous fat correctly; these agents cause ectopic fat deposition. Patients also can experience weight gain and fat redistribution when receiving glucocorticoids for inflammation. Furthermore, some patients may have visceral fat accumulation because of a maladaptive response to stress. Therefore, it is important to recognize that where the body fat is distributed determines the obesity phenotype, which can help us identify patients at high risk for cardiometabolic disease.10-13
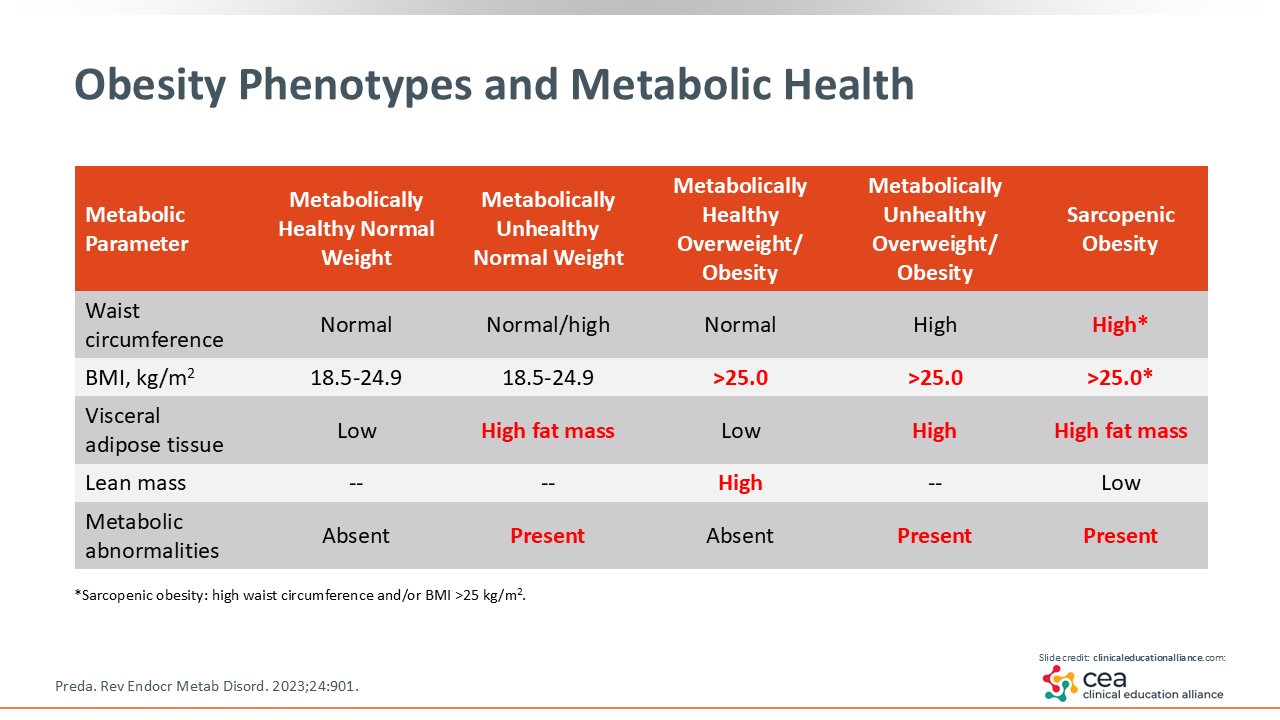
Obesity Phenotypes and Metabolic Health
Now I want to discuss the phenotypes that can influence cardiometabolic risk. One is the metabolically unhealthy normal weight phenotype comprising people with a normal weight and BMI of 18.5-24.9 kg/m2, but they are storing too much fat viscerally. They can have a high waist circumference and do have a high fat mass in the visceral adipose tissue. That drives cardiometabolic abnormalities, even though their body weight or BMI might be “normal.”
Similarly, there are some people with overweight or obesity (BMI >25 kg/m2) who are metabolically healthy. The reason for this is that these patients have high lean muscle mass. These are bodybuilders and/or young individuals. The way we identify these folks is their having a normal waist circumference. In addition, they have no metabolic abnormalities because of their body size, which is what BMI is measuring. And their body fat distribution is normal. This describes the metabolically healthy overweight/obesity phenotype.
Another phenotype is metabolically unhealthy overweight/obesity. That is the phenotype that is generally referred to when discussing obesity. These people have a high BMI, high waist circumference, and metabolic abnormalities because of visceral and ectopic adiposity.
Finally, there is one special phenotype called “sarcopenic obesity.” This includes people with overweight or obesity, a high BMI and/or waist circumference, high fat mass, and low lean mass. This group is often made up of older adults, and large proportions of them are women because they do not have high muscle mass to begin with. I worry about excessive weight loss in this population because they do not have high muscle mass to start with. Therefore, HCPs must be careful about weight loss with this specific population.14
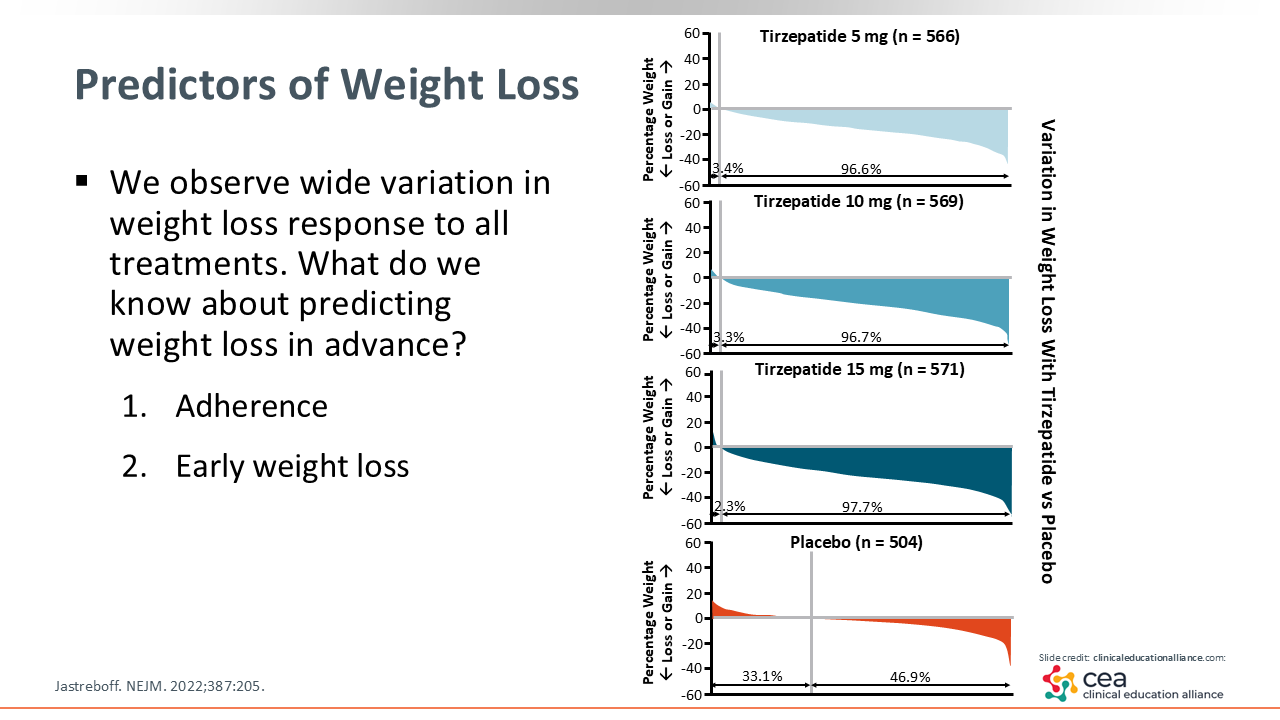
Those are the obesity phenotypes that can occur per fat distribution. But there are additional phenotypes that consider the pathophysiology of overweight and obesity. Furthermore, some patients have different responses to treatment. With every one of our weight loss treatments, there is a wide variation in response, and the reason for this is not fully understood yet.
Predictors of Weight Loss
One of the best predictors of response is adherence to the treatment regimen—whether that includes diet, physical activity, and/or an AOM. Treatment adherence is a big factor that drives response.15
Another way to identify those who are going to struggle with weight loss is to watch for the amount of weight loss that occurs early on (eg, within 4-8 weeks). Early weight loss is a good predictor of ultimate weight loss.16
Assessing Suboptimal Responders: Lifestyle and Behavioral Factors
To help those who are having a suboptimal response to treatment, HCPs must understand what exactly is going on with patients. Many drivers of this issue are biologic in nature. But it is important to confirm patients are following their prescribed diet. If they are not, what are the problems with that diet and any physical activity recommendations that they are following alongside their AOM? We need to ensure patients get adequate sleep because sleep hygiene is important. One cannot lose weight if they do not have good sleep hygiene.
In addition, we need to understand what is going on with patients' motivation and readiness to change. Are there barriers that are making it difficult for them to adhere to their treatment plan?
Next addressing any psychologic contributors is critical. Depression and anxiety can thwart weight loss attempts. A lack of social support and stigma can drive this, too. It is not unusual for friends and family to sabotage some patients’ weight loss attempts. They often do this because they feel threatened by the person who is losing weight. So it is important that patients have a good social support network around them when they are on their weight loss journey.
It also is vital for HCPs to understand that those who must do the treatment or change their behavior to lose weight are our patients, not us. That is why we always use shared decision-making when determining treatment plans. It must be endorsed and followed by patients.
Now research shows that patients with obesity and type 2 diabetes lose less weight with AOMs vs those with obesity and no type 2 diabetes.17 This is why HCPs should always check patients’ prescription list because some medications will fight weight loss. If we can get patients off those medications and on a different one, we can address some low-hanging fruit to make weight loss a little easier.
Finally, HCPs should consider all these lifestyle and behavioral factors and tailor treatment plans to the individual patient. This is where phenotyping can help—figure out what exactly is going on with the patient and develop a treatment plan that matches their needs.
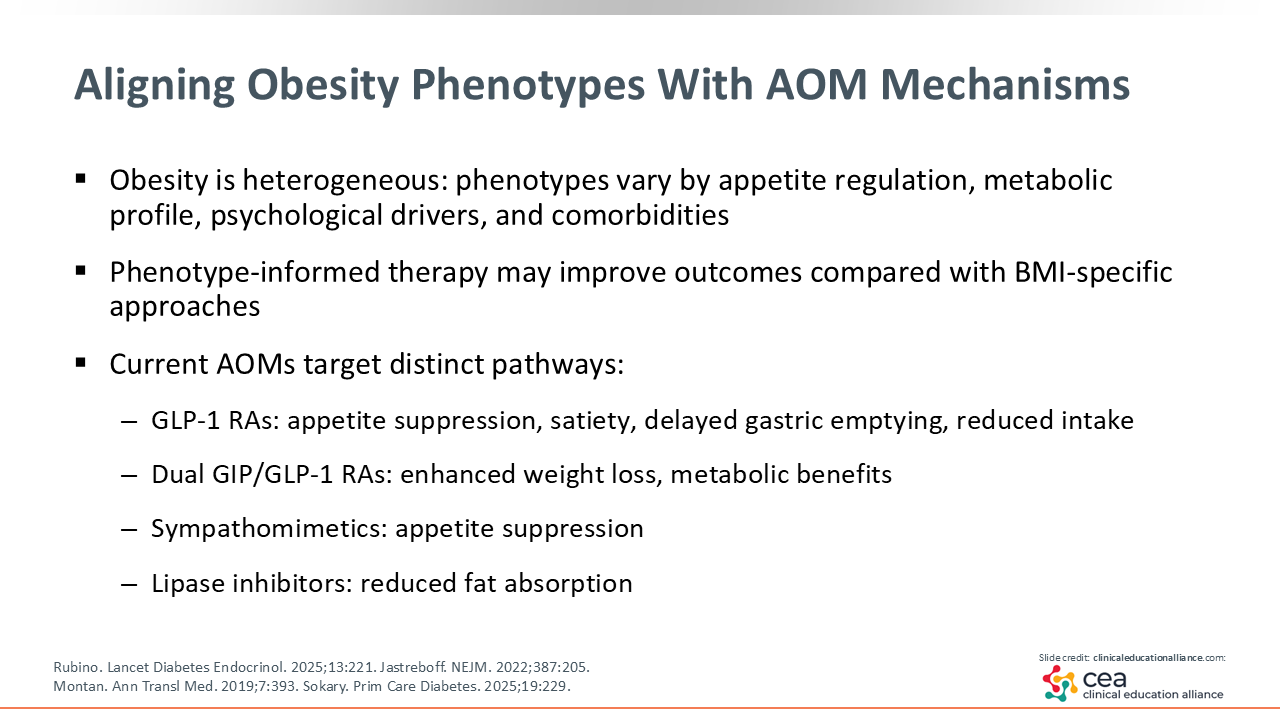
Aligning Obesity Phenotypes With AOM Mechanisms
The available AOMs all have different mechanisms of action. And obesity phenotypes can vary by patients’ appetite regulation, metabolic profile, psychologic drivers, and comorbidities. Therefore, HCPs should understand the problems that patients are having with their weight loss efforts and choose the right AOM that will work for them.
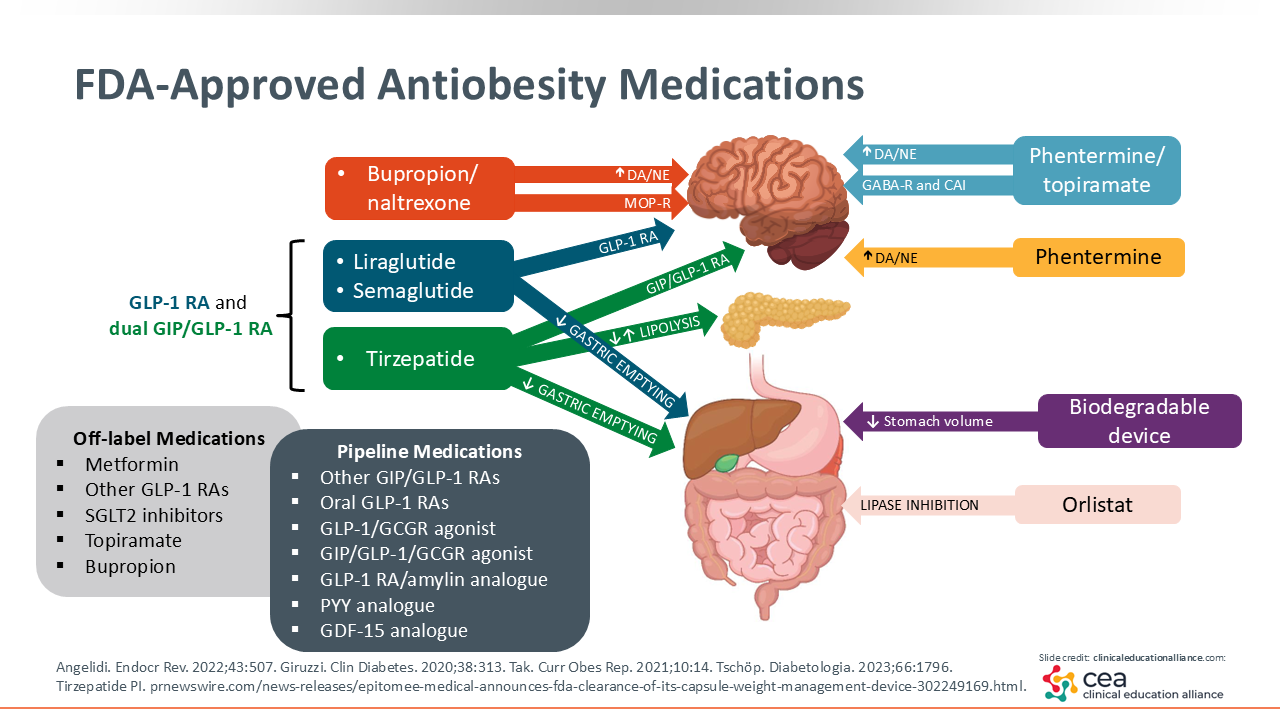
The way GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists work is by promoting satiety and delaying gastric emptying, so patients feel fuller for longer. The ultimate result of this is reduced food intake and weight loss. In addition, there are anecdotal reports that these agents affect what is called “food noise” or intrusive thoughts about food. Some patients report that suddenly they are no longer tormented by these intrusive and continuous thoughts of food.18,19 So that is another way that GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists work.
Orlistat is a lipase inhibitor that reinforces the desire to be on a low-fat diet. If patients eat fat while receiving orlistat, they will have a bad outcome. It teaches patients that they do not want to have a high-fat diet while receiving lipase inhibitors like orlistat.
The sympathomimetics like phentermine operate by suppressing one’s appetite. They are anorexic agents.
One agent, bupropion naltrexone, has some evidence showing its impact on reducing cravings.20 The typical patient with cravings will report that after dinner, when they are not hungry, they have thoughts about the ice cream in the freezer calling to them. It is this craving for either sweets or salty snacks that patients can associate with a high hedonic reward, and so they may benefit with this specific treatment option.
Most AOMs—liraglutide, semaglutide, tirzepatide, phentermine-topiramate, phentermine alone, and naltrexone-bupropion—all work in the brain to help reduce food intake. But it is the GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists that also reduce gastric emptying. Then orlistat is the other AOM that works by preventing the absorption of fat, reinforcing the need for low-fat diets.21
FDA-Approved Antiobesity Medications
As shown on the slide here, recognizing how each AOM works and why a patient is struggling with weight loss are important. In these cases, HCPs should use this information to help direct therapy to the right obesity phenotype.
Although recent improvements in obesity management have revolutionized the field, we still do not have much information on which AOM to match with which patients. There is a lot of research on this that is emerging, and this is something we absolutely need to solve.
Future Directions With Novel AOMs
Now there are newer therapies that are being developed based on the early successes seen with GLP-1 agonism and dual GIP/GLP-1 agonism. We are seeing greater amounts of weight loss and fewer people are failing to achieve clinically significant weight loss when receiving these AOMs. That is something to be optimistic about. And this is reinforcing the idea that if we can provide AOMs that hit multiple areas that regulate appetite, more patients can achieve greater and sustained weight loss.
There is new interest in glucagon (GCG) receptor agonism, which affects energy expenditure. This is a very good thing because there are some patients with low metabolic rates who need that stimulation. Right now, we are not certain that GCG will pan out there, but I am watching this space. GCG agonism is being investigated to potentially promote energy expenditure and fat oxidation.
There also are agents that are targeting whole new areas. One of which includes amylin analogs, as these agents have potent satiety signals and show potential synergy with incretin-based therapies. Furthermore, researchers are looking to better understand and develop agents that are going to address the sarcopenic obesity phenotype.22,23
Combining AOMs with treatment that promotes muscle preservation and may improve muscle function are additional areas of active research.24
We have the opportunity to shift the paradigm. Instead of simply picking an AOM that we think might have the greatest odds for weight loss, we can better align the mechanism of action of the AOM to what exactly is going on with patients. Meaning, we have the potential to transform care from just looking at BMI to knowing more about obesity phenotypes and using phenotype-directed AOM selection.10
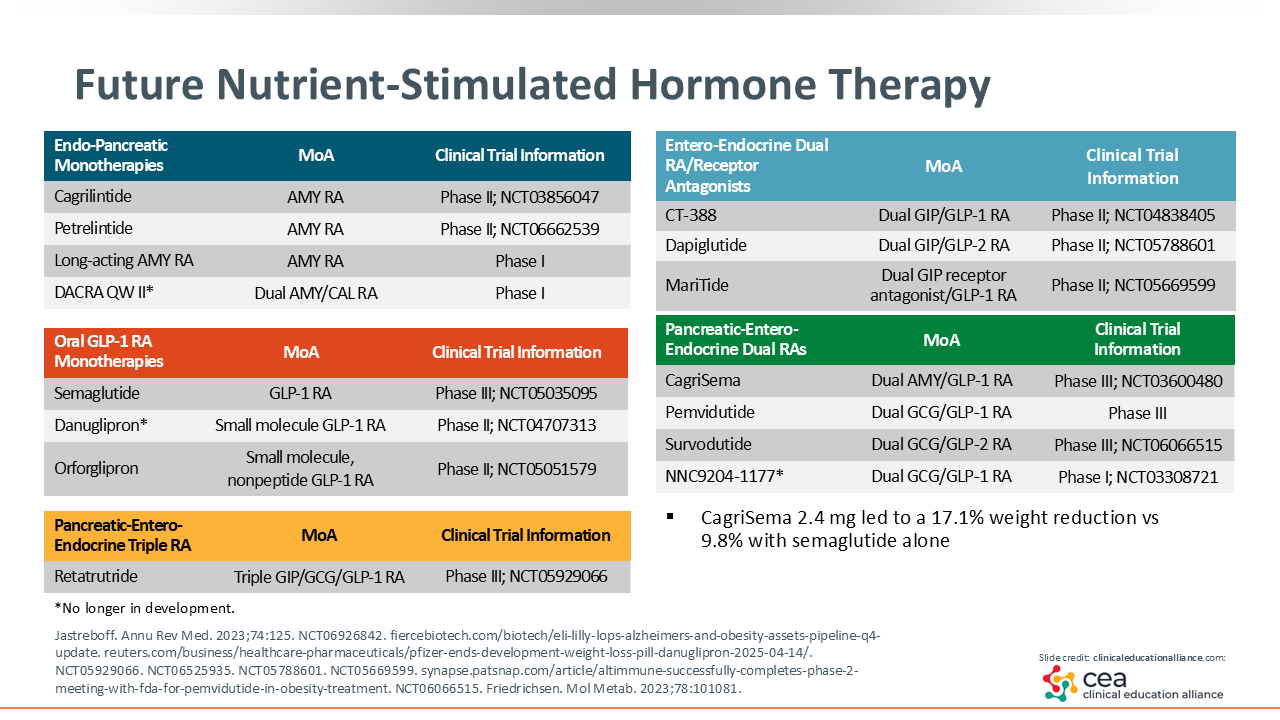
Further Nutrient-Stimulated Hormone Therapy
This slide highlights the many AOMs currently in development and/or being studied in clinical trials. Of note, the asterisk symbol identifies the agents that are no longer in development. As mentioned previously, one can see that there are several dual-targeted agents and 1 triple-targeted agent being studied in phase II or III clinical trials.25
Risks of Excessive or Rapid Weight Loss
Last, I discuss the risks associated with excessive or rapid weight loss. This is often defined as more than 1.5-2.0 kg per week of weight loss beyond the initial water weight phase.
Clinical risks include loss of lean mass, which is why HCPs should prioritize lean mass preservations in patients’ treatment plans by recommending resistance exercise and ensuring patients are getting enough protein. Other risks include nutritional deficiencies (eg, iron, vitamin B12, and vitamin D), gallstone formation, and an increased risk of sarcopenia in older adults. These risks should be addressed in any patients who are losing too much weight or weight too quickly.
The current recommendation is to lose 0.5-1.0 kg per week for safety and sustainability. HCPs should reassess treatment plans if weight loss is excessive or unintentional.26-28