CE / CME
Advancing Inflammatory Bowel Disease Management With Precision Medicine and Emerging Data
Physician Assistants/Physician Associates: 0.75 AAPA Category 1 CME credit
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Released: May 08, 2025
Expiration: May 07, 2026

Activity
Inflammatory Bowel Disease Prevalence in the US
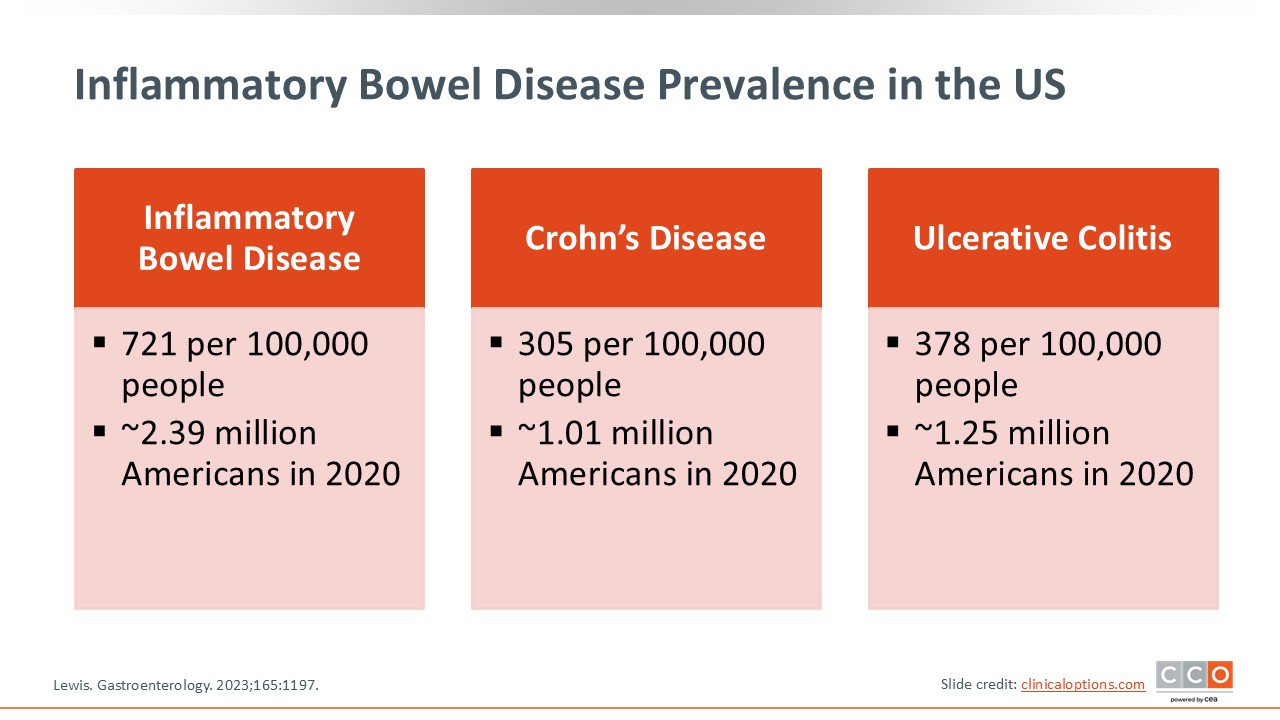
To set the stage, there are more than 2 million people in the United States with IBD. Approximately 1 million have CD or UC, with a slightly higher prevalence seen in UC, so there is a significant number of patients with IBD in the United States. Furthermore, IBD prevalence increases over time because of compounding new diagnoses among those in early adulthood, and then plateauing as people age.1
Inflammatory Bowel Disease Activity in US Patients
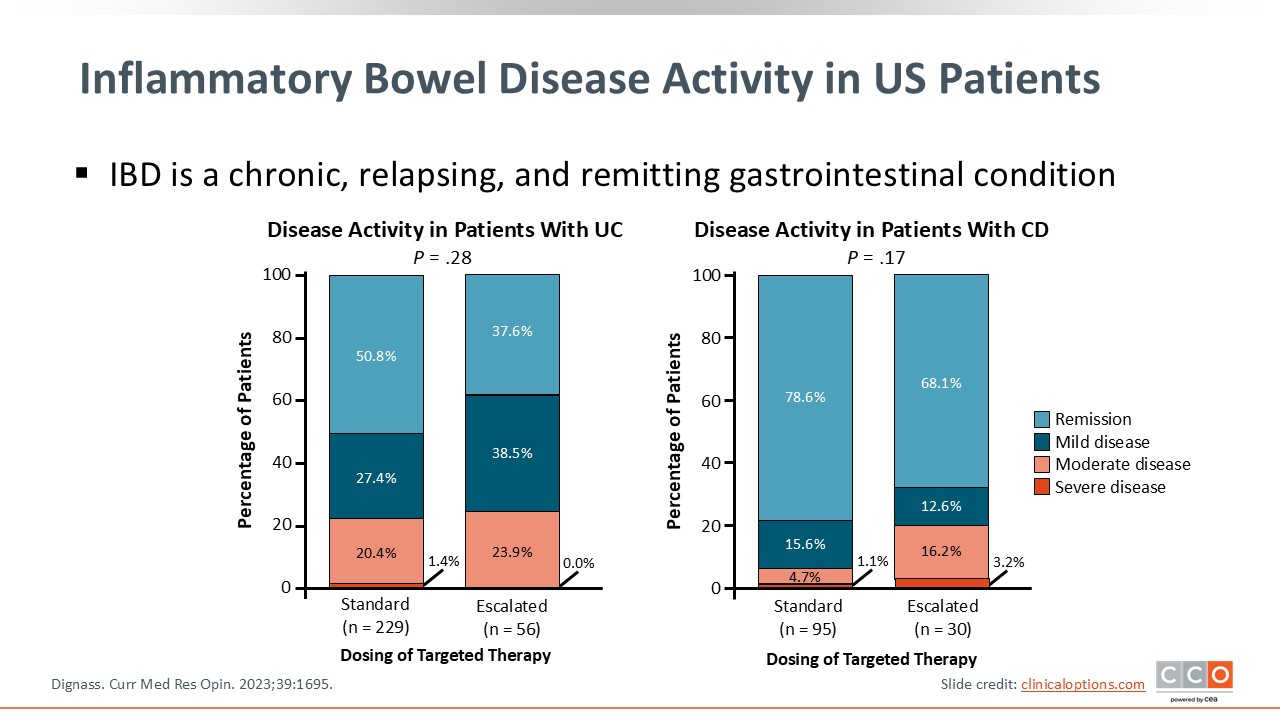
IBD is a chronic, relapsing, and remitting gastrointestinal condition. Significant portions of patients, in both CD and UC, have severe disease that is uncontrolled with our current treatment arsenal. The data also show that more patients are achieving remission via a more aggressive treatment strategy. Much of our treatment targets are aligned with aggressive treatment, in particular for patients with severe disease.2
Symptom Impact in IBD as Reported by US Patients
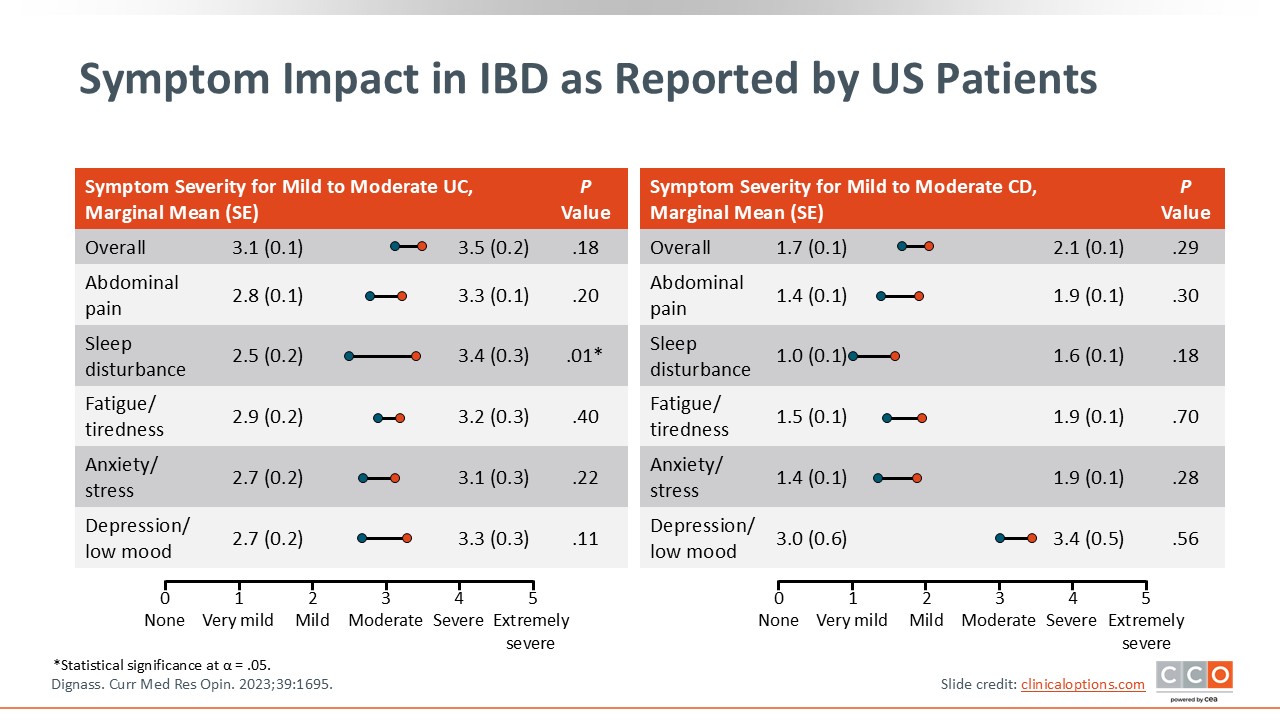
For the patients living with IBD in the United States, their symptom burden is significant. Many report significant moderate to severe abdominal pain, sleep disturbances, fatigue, anxiety, and depression, among other symptoms. This is important because when we evaluate patients with IBD, HCPs should ask about their gastrointestinal symptoms and their systemic symptoms like mental health or extraintestinal manifestations. These are all critical in assessing the symptom burden of IBD on a systemic level.2
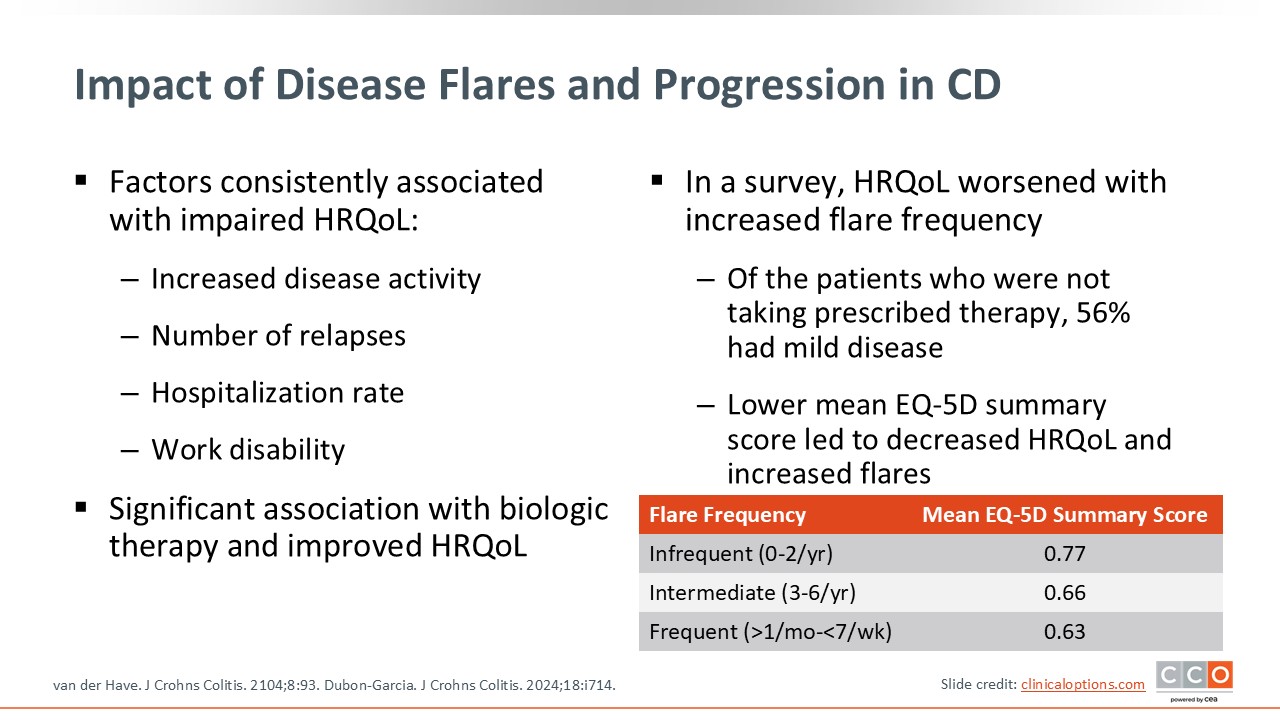
Impact of Disease Flares and Progression in CD
In addition to the symptom burden, disease flares and progression are significant concerns in IBD, particularly in CD, and are associated with impaired quality of life. There is an increased risk for hospitalization, work disability, and missing out on family and personal events. Data demonstrate that quality of life worsens with increased flare frequency. This is important because disease remission, which can wear many hats, includes not only an improvement in disease activity and symptom burden, but also patients’ ability to return to a normal quality of life. Furthermore, there is a significant association with advanced therapy use and improvement in quality of life, so early effective therapy may mitigate patients’ disease flares and progression and directly improve their quality of life.3,4
What Is Treat to Target?
What is treat to target? When HCPs evaluate patients and think about starting an advanced therapy, how do they monitor response? That is the foundation of treat to target—a medical management strategy that focuses on achieving defined goals and mucosal healing via deep remission. With this approach, HCPs assess patients for improvement in symptom burden and biomarker normalization, as well as endoscopic, histologic, and radiographic endpoints to determine if there is mucosal healing. They continually assess patients for these short-term and long-term targets, making treatment adjustments along the way until patients achieve all targets. No longer do we simply start patients on therapy and check back with them years later. Instead, HCPs now should follow up with patients in the short and long term.5,6
Why Is Treat to Target Important in IBD?
Treat to target is associated with a reduction in long-term disease complications and progression. It also improves quality of life and decreases surgery and hospitalization rates. Compared with conventional therapy, treat to target is further associated with improved remission rates. Because symptom burden and objective inflammatory outcomes are integrated into treat to target, this approach to care aligns much more closely with patients’ preferences and outcomes.5,6
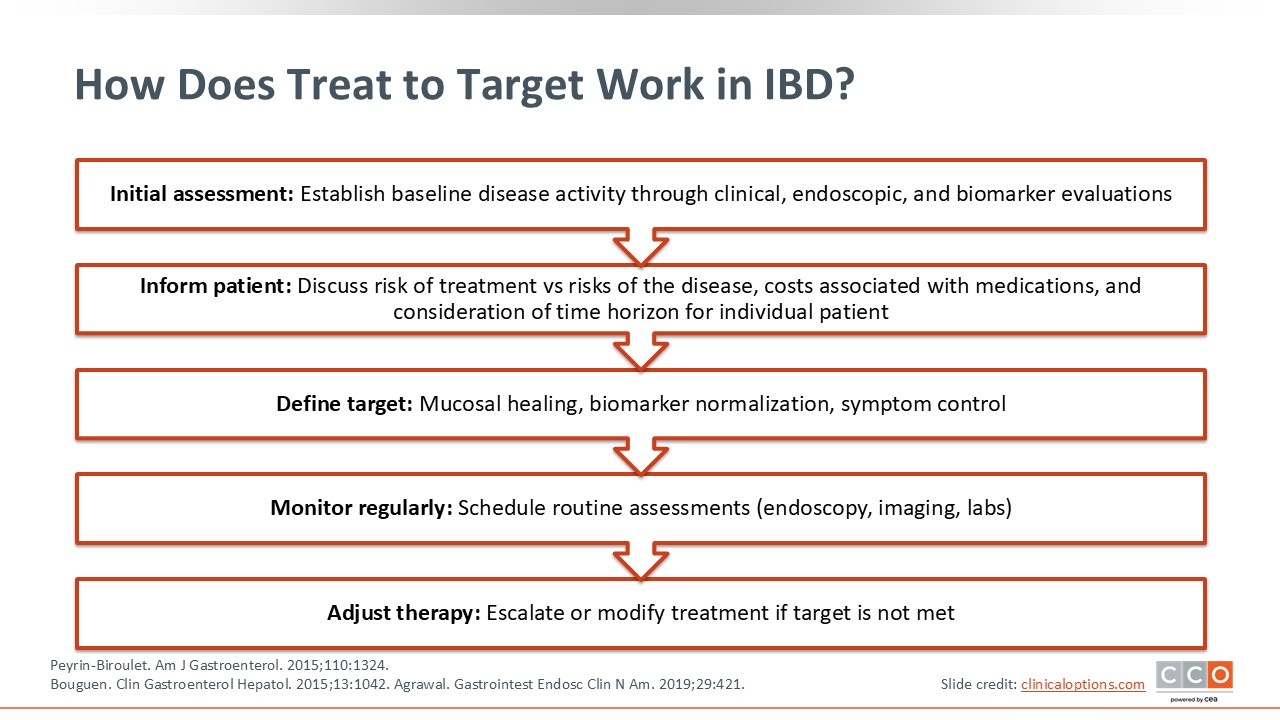
How Does Treat to Target Work in IBD?
In applying treat to target, HCPs should complete a baseline assessment of patients’ endoscopic, biochemical, and symptom activity before initiating advanced therapy. HCPs then should review with patients how they will monitor response over time and at what intervals. For example, we want to see symptom control in the short term, biomarker normalization in the medium term, and mucosal healing in the long term. Furthermore, HCPs should discuss the specific assessments (eg, blood stool or endoscopy) that will applied and how therapy may be adjusted to achieve those goals.7-9
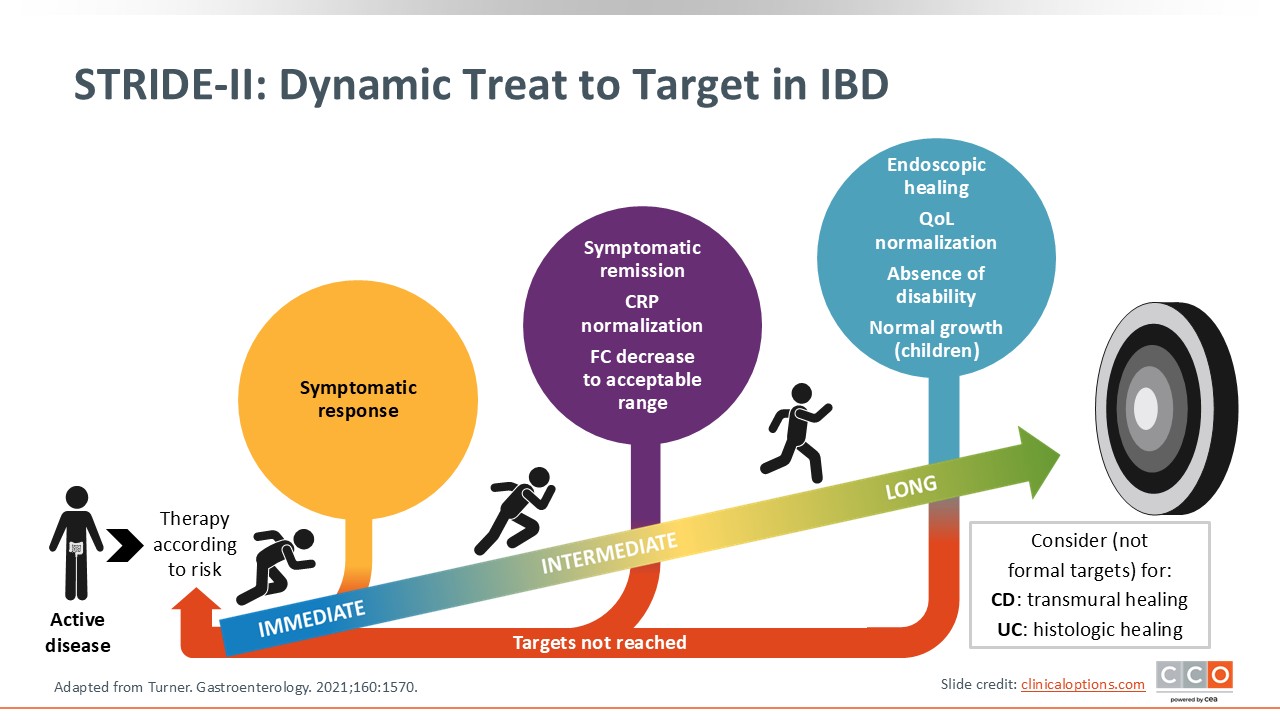
STRIDE-II: Dynamic Treat to Target in IBD
This slide illustrates another way of looking at treat to target, showing how this is a dynamic approach to care. We are setting goals, discussing with patients how we plan on achieving those goals, and adjusting their therapy if a target is not reached. As shown in the figure, the main goal is mucosal healing, with transmural, histologic, and radiographic healing still being explored.10
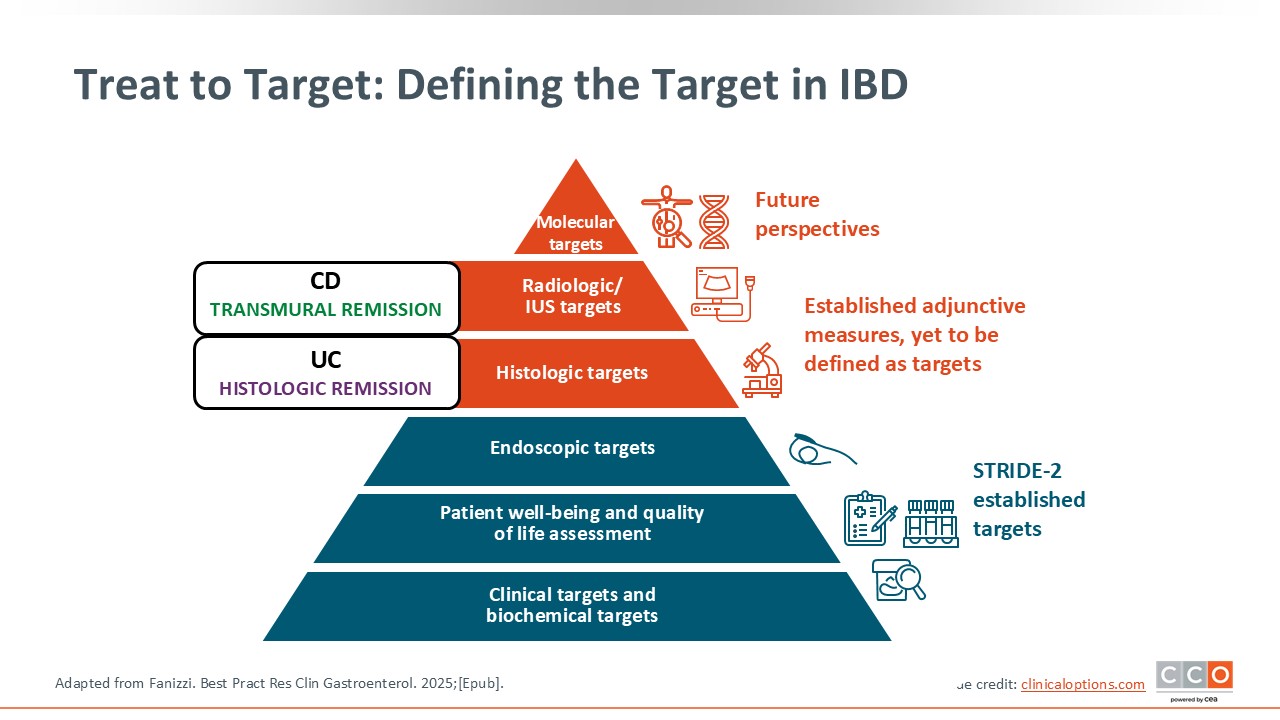
Treat to Target: Defining the Target in IBD
Defining the target in IBD is critical. Right now, we mostly use clinical, biomarker, and endoscopic targets. But there are emerging data demonstrating that biopsy, histologic targets in UC, and transmural targets in CD are likely associated with better reductions in future complications, quality of life, flares, and adverse complications of active disease. Current research has started to look at integrating some of these deeper levels of remission and how these can be achieved or measured. These are not formal guideline recommendations, but there are emerging targets that are associated with further clinical benefit if they are achieved.11
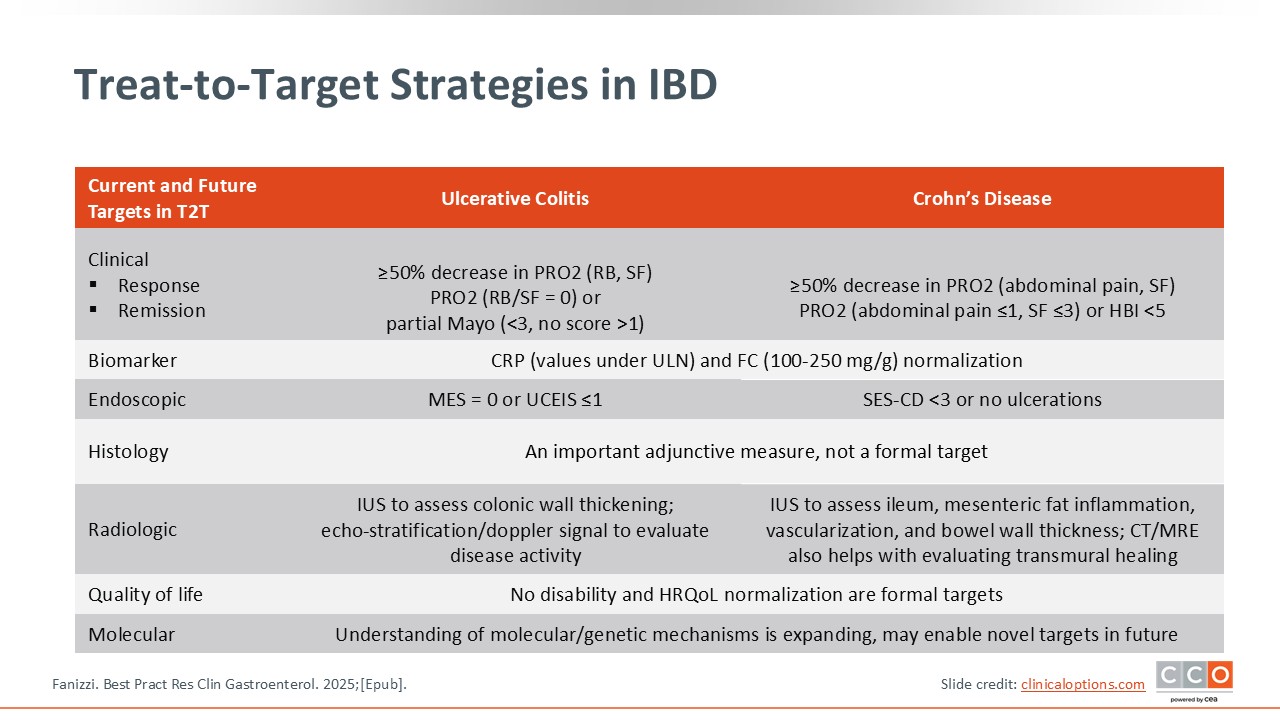
Treat-to-Target Strategies in IBD
In UC, improvement in clinical symptoms is measured via the Mayo score. Of course, response can be assessed via biomarkers like CRP and FCP. Endoscopy would include the Mayo endoscopic subscore, whereas histologic findings are more so aspirational by assessing either clearance of active histology or at least inactivity. Ultrasound is used less frequently in UC, but it is a useful surrogate for evaluating bowel wall activity. For quality of life, HCPs should make sure that patients are getting back to school or work and feeling better generally. Then there are molecular targets that are being explored as a potential surrogate for advanced healing techniques.
In CD, we use patient-reported outcomes (ie, Harvey-Bradshaw Index) to measure improvement as well as biomarkers like CRP and FCP. Endoscopy comprises the simple endoscopic score for CD, whereas histologic findings assess for clearance of inflammatory burden and lack of complications (eg, stricture). Radiographic outcomes in CD are important, and transmural healing remains an aspirational target. Ultrasound, CT, or MRE is helpful in assessing disease activity, as radiographic normalization can be considered a treatment target for select patients.11
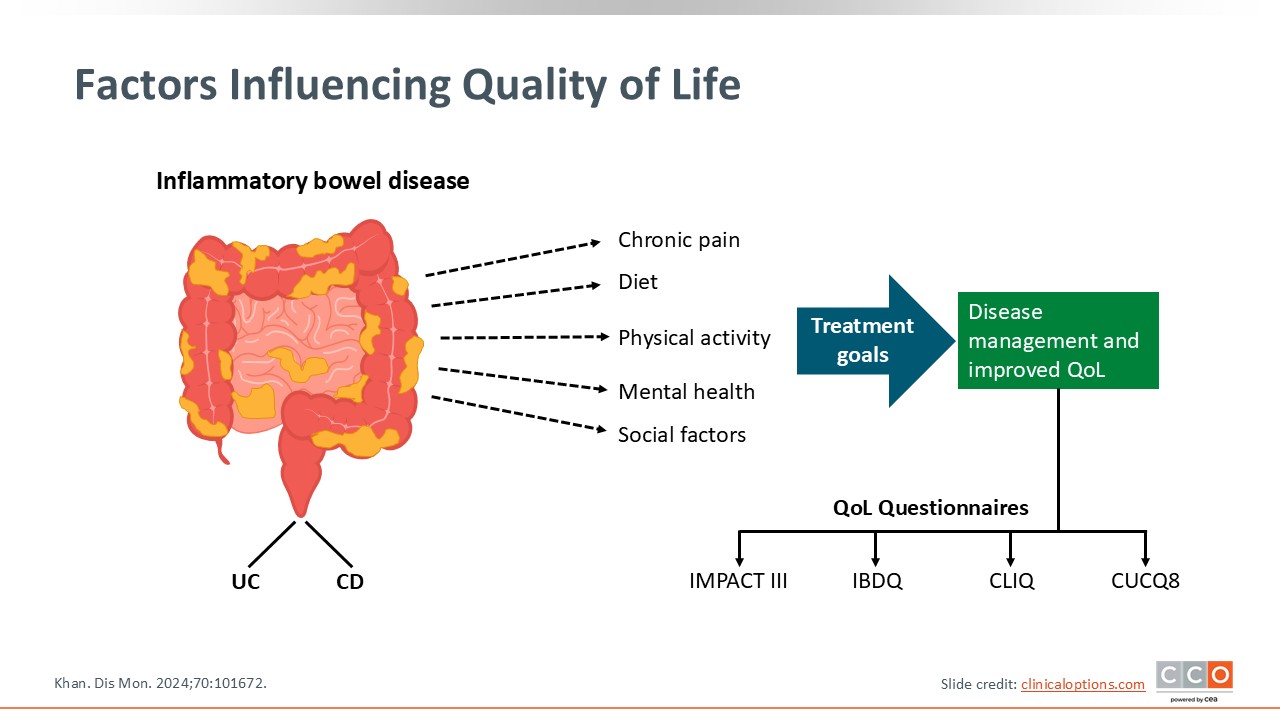
Factors Influencing Quality of Life
There are many factors of IBD that influence quality of life. Of course, disease activity is the primary driver of symptoms, which is associated with chronic pain; reduced physical activity, quality of life, and mental health; and various social factors. Of importance is that advanced treatment to achieve targets, mucosal healing in particular, is directly associated with improvements in various aspects of patients’ quality of life. Currently, many IBD clinical trials integrate objective measures of quality of life that can tell us about improvements in some of these areas, which is separate from objective disease measures that also are important to assess. This slide underscores that quality of life has many factors in IBD, and HCPs should assess for this, too.12
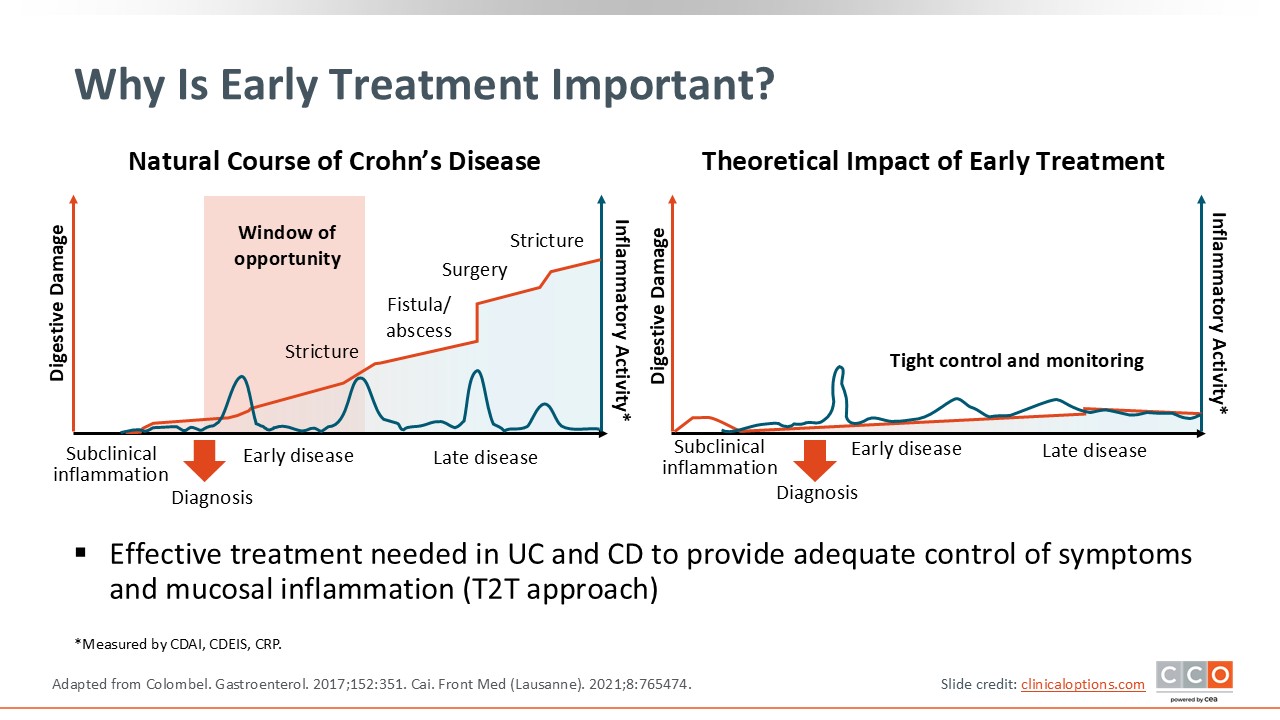
Why Is Early Treatment Important?
Early treatment is vital because before patients develop complications, particularly ones like stricture and fistula that may require surgical intervention, there is a window of opportunity where we can reduce that complication rate and prevent the future development of these adverse sequela of disease. In that window of opportunity, data suggest that the more aggressive treatment is in getting patients in mucosal healing, the more it dramatically reduces the risk of future complications, surgery, and more.5,13 The way we can achieve this is through treat to target. After an early diagnosis, HCPs should start aggressive, advanced therapies to reduce the risk of fistula, abscess, stricture, and surgical requirements.