
CE
SC ICI Delivery Strategies: Supporting Clinical Data for SC Immunotherapies
Pharmacists: 0.50 contact hour (0.05 CEUs)
Released: July 13, 2026
Expiration: January 12, 2027


Activity
Rationale for SC vs IC ICI
Shawna Kraft, PharmD, BCOP:
The available supporting trial data for SC ICI formulations help address the practical question of whether SC administration can deliver advantages such as shorter administration time and reduced treatment burden without compromising the efficacy and safety expected from established IV therapy. This question has now been evaluated across multiple solid tumors through studies examining pharmacokinetics, clinical outcomes, safety, and patient-reported preferences for SC vs IV administration. In this module, we will review these supporting data and consider how they may inform oncology pharmacy practice today.
IMscin001 Part 1: SC Atezolizumab in Patients With Locally Advanced or Metastatic NSCLC
Shawna Kraft, PharmD, BCOP:
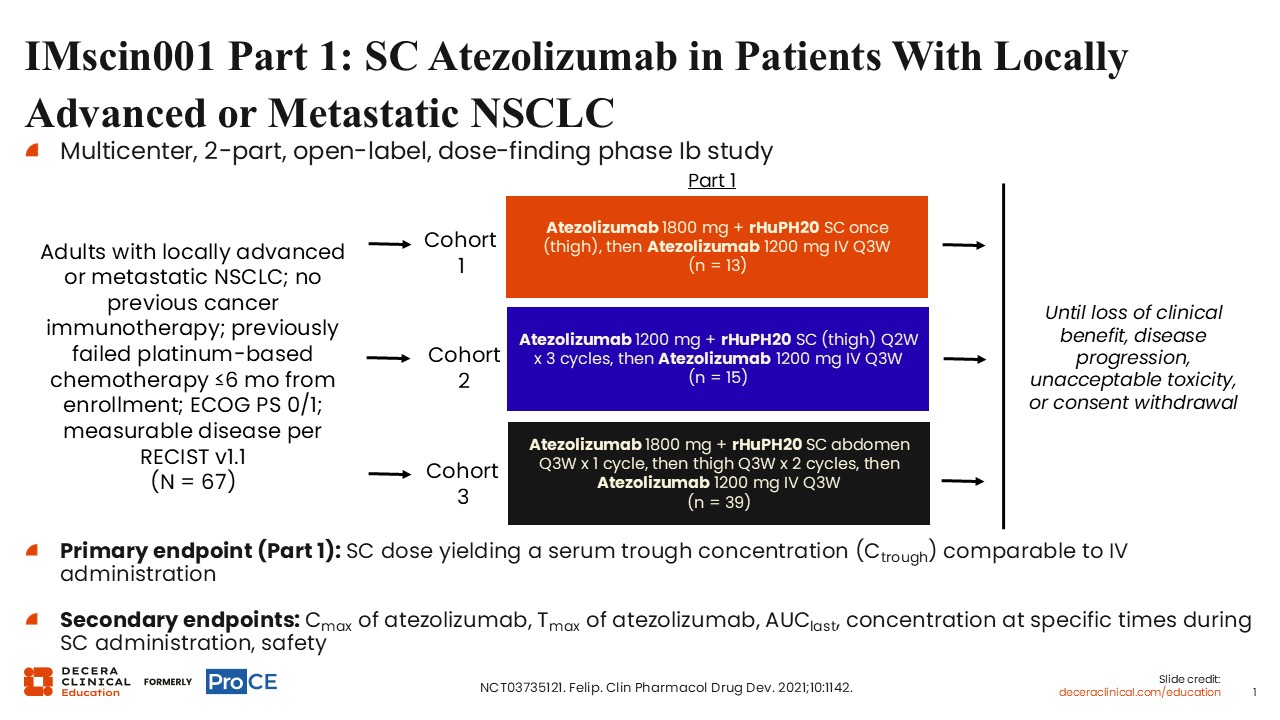
IMscin001 Part 1 was a multicenter, 2-part, open-label, dose-finding phase Ib study in adults with locally advanced or metastatic NSCLC (NCT03735121).1 Eligible patients had not previously received immunotherapy, had previously failed platinum-based chemotherapy within 6 months of enrollment, had Eastern Cooperative Oncology Group (ECOG) performance status (PS) 0/1, and had measurable disease by Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. The Part 1 population included 67 patients.
Cohort 1 received atezolizumab 1800 mg plus rHuPH20 SC once in the thigh, followed by atezolizumab 1200 mg IV every 3 weeks (n = 13). Cohort 2 received atezolizumab 1200 mg plus rHuPH20 SC in the thigh every 2 weeks for 3 cycles, followed by atezolizumab 1200 mg IV every 3 weeks (n = 15). Cohort 3 received atezolizumab 1800 mg plus rHuPH20 SC in the abdomen every 3 weeks for 1 cycle, then in the thigh every 3 weeks for 2 cycles, followed by atezolizumab 1200 mg IV every 3 weeks (n = 39). Treatment continued until loss of clinical benefit, disease progression, unacceptable toxicity, or consent withdrawal.
The primary endpoint for Part 1 was the SC dose yielding a serum trough concentration (Ctrough) comparable to IV administration. Secondary endpoints included atezolizumab Cmax, Tmax, AUClast, concentration at specific times during SC administration, and safety.
IMscin001 Part 1: Atezolizumab Serum Concentration Over Time and SC vs IV Ctrough (Primary Endpoint)
Shawna Kraft, PharmD, BCOP:
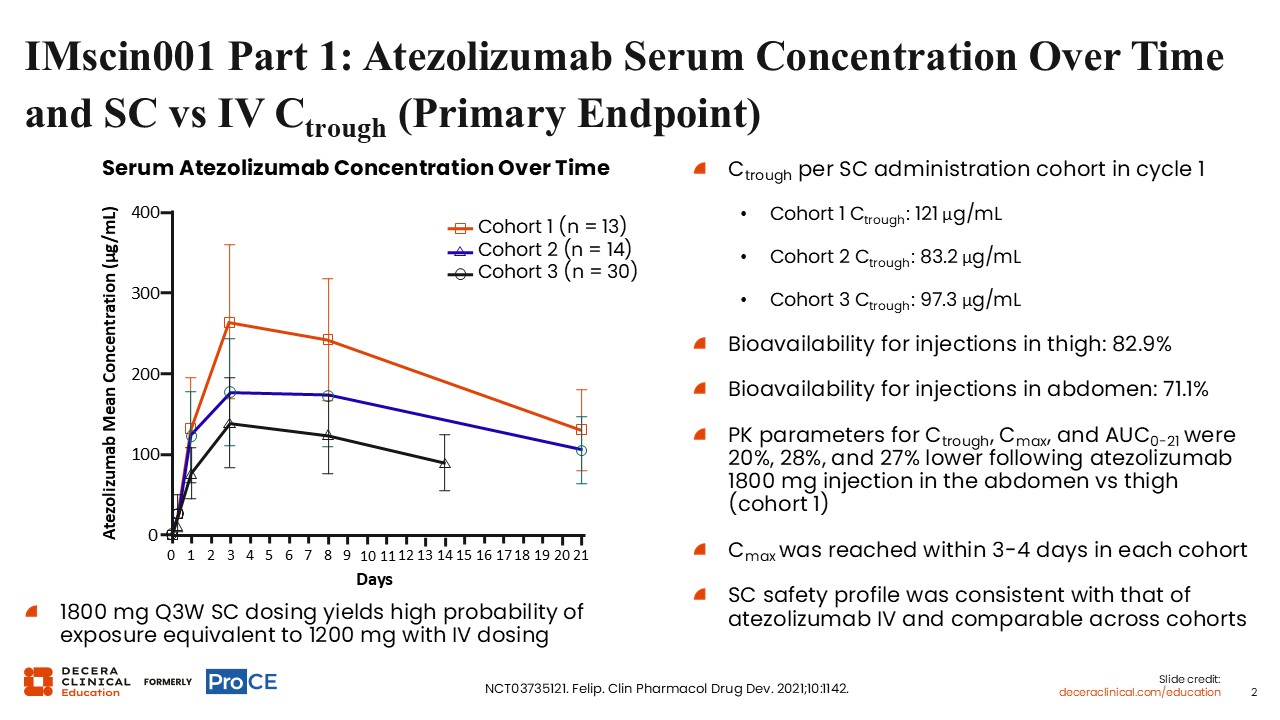
Atezolizumab serum exposure over time was generally comparable between the SC and IV formulations in IMscin001 Part 1. Across the 3 SC administration cohorts, Ctrough values in cycle 1 were in a similar range to those observed with IV atezolizumab, supporting comparable exposure. Bioavailability for thigh injections was 82.9%, and pharmacokinetic parameters for Cmax, Ctrough, AUC0-21d, and AUCinf were broadly consistent with those of atezolizumab IV. Based on these data, SC dosing provided exposure consistent with IV atezolizumab, with a high probability of exposure equivalence to 1200 mg IV every 3 weeks.
IMscin001 Part 2: SC vs IV Atezolizumab in Previously Treated LA or Metastatic NSCLC
Shawna Kraft, PharmD, BCOP:
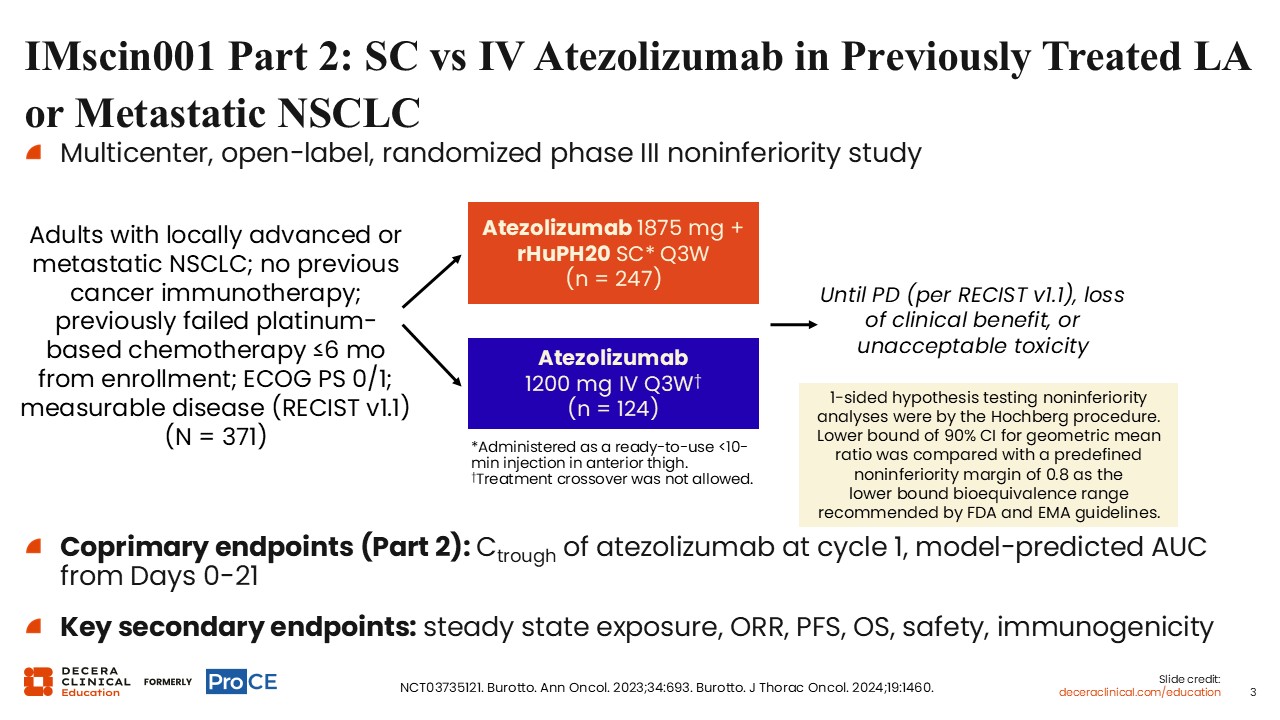
IMscin001 Part 2 was a multicenter, open-label, randomized phase III noninferiority study that compared SC with IV atezolizumab in adults with locally advanced or metastatic NSCLC (NCT03735121).2,3
Eligible patients had measurable disease per RECIST v1.1, ECOG PS 0 or 1, no previous cancer immunotherapy, and prior failure of platinum-based chemotherapy within 6 months before enrollment. Patients were randomized to receive atezolizumab 1875 mg plus rHuPH20 SC every 3 weeks or atezolizumab 1200 mg IV every 3 weeks, with treatment continued until disease progression, loss of clinical benefit, or unacceptable toxicity; crossover was not allowed. The coprimary endpoints for Part 2 were cycle 1 Ctrough and model-predicted AUC0-21, with key secondary endpoints including steady-state exposure, ORR, PFS, OS, safety, and immunogenicity.
IMscin001 Part 2: Cycle 1 Ctrough and AUC on Days 0-21 (Coprimary Endpoints)
Shawna Kraft, PharmD, BCOP:
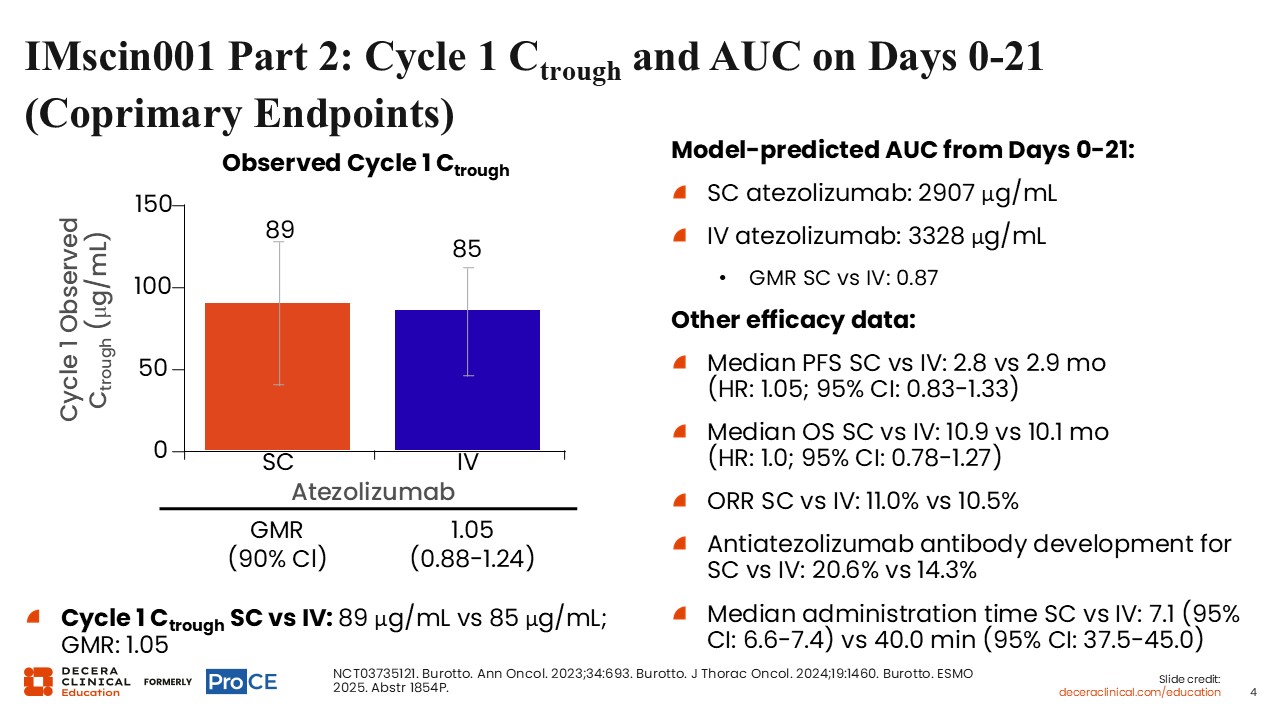
Investigators from the IMscin001 Part 2 study showed that cycle 1 atezolizumab exposure was comparable between the SC and IV formulations, with similar Ctrough and AUC0-21 values across treatment arms. Specifically, geometric mean cycle 1 Ctrough was 207 mcg/mL with SC atezolizumab vs 209 mcg/mL with IV atezolizumab, and model-predicted mean AUC0-21 was 307 vs 328 mcg/day/mL, supporting noninferior pharmacokinetic exposure with the SC formulation.2-4
Efficacy outcomes were also broadly similar for SC vs IV atezolizumab, with median PFS of 2.8 vs 2.9 months (HR: 1.05; 95% CI: 0.83-1.33), median OS of 10.9 vs 10.1 months (HR: 1.0; 95% CI: 0.78-1.27), and ORR of 11.0% vs 10.5%.
IMscin002: Patient and HCP Preference for SC vs IV Atezolizumab for the Treatment of NSCLC
Shawna Kraft, PharmD, BCOP:
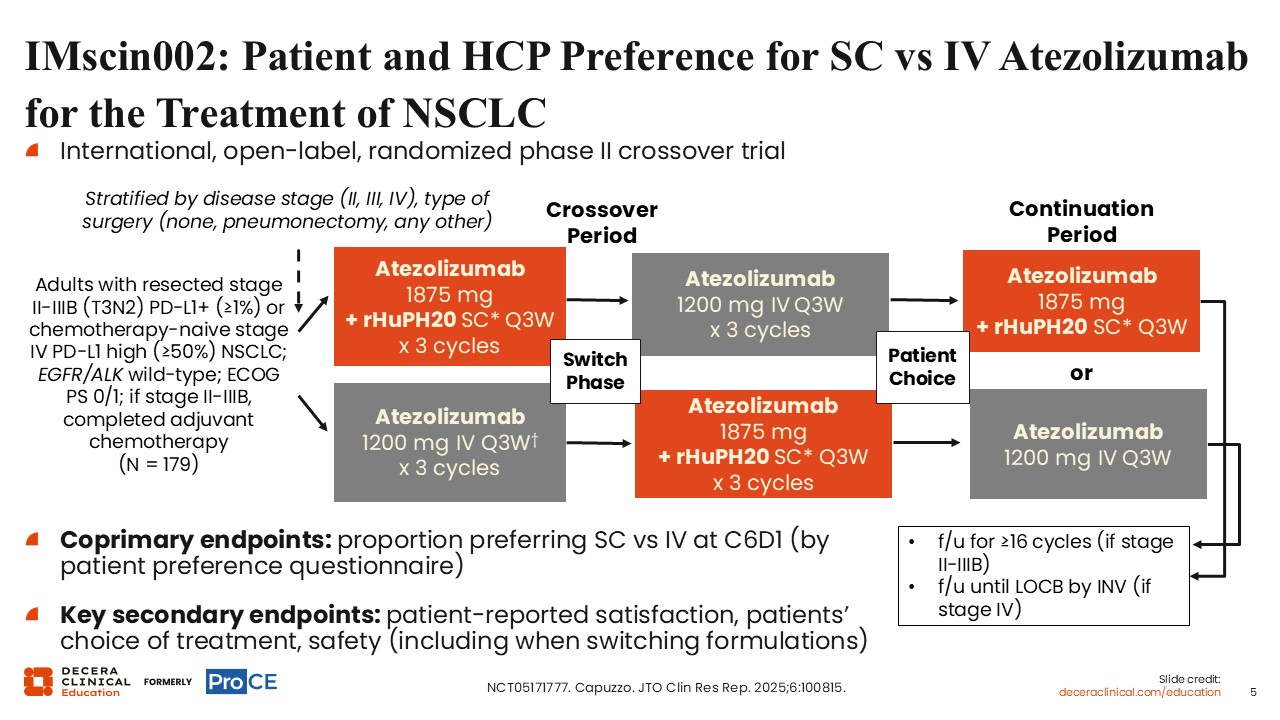
IMscin002 was an international, open-label, randomized phase II crossover trial evaluating patient and healthcare professional preference for SC vs IV atezolizumab in NSCLC (NCT05171777).5 Eligible adult patients had resected stage II-IIIB (T3N2) PD-L1–positive disease with PD-L1 expression of at least 1% or chemotherapy-naive stage IV PD-L1–high disease with PD-L1 expression of at least 50%; EGFR/ALK wild-type status; ECOG PS 0/1; and, for stage II-IIIB disease, completed adjuvant chemotherapy (n = 179).
In the crossover period, patients received either atezolizumab 1875 mg plus rHuPH20 SC every 3 weeks for 3 cycles followed by atezolizumab 1200 mg IV every 3 weeks for 3 cycles, or the reverse sequence. In the continuation period, patients chose atezolizumab 1875 mg plus rHuPH20 SC every 3 weeks or atezolizumab 1200 mg IV every 3 weeks. Patients were stratified by disease stage, surgery type, and related factors shown on the slide. The coprimary endpoint was the proportion of patients preferring SC vs IV administration at cycle 6 Day 1 by patient preference questionnaire. Key secondary endpoints included patient-reported satisfaction, patients’ choice of treatment, and safety, including safety when switching formulations.
IMscin002: Patient Preference for Atezolizumab SC vs IV and Choice of Formulation in the Continuation Period
Shawna Kraft, PharmD, BCOP:
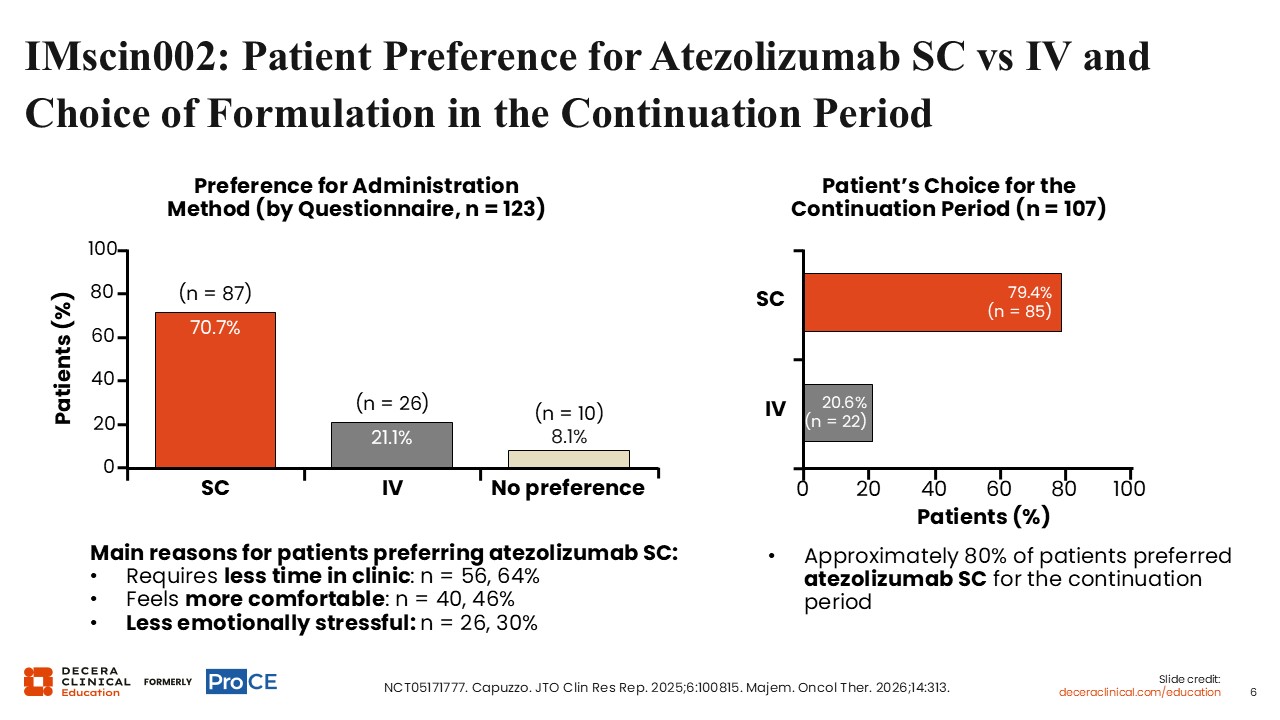
Among 123 patients completing the preference questionnaire, 70.7% preferred SC administration, 21.1% preferred IV administration, and 8.1% had no preference.5,6 The main reasons for preferring atezolizumab SC were less time in clinic (n = 56; 64%), greater comfort (n = 40; 46%), and less emotional stress (n = 26; 30%).
For the continuation period, approximately 80% of patients chose atezolizumab SC. In the patient choice analysis shown (n = 107), 79.4% (n = 85) chose SC administration and 20.6% (n = 22) chose IV administration.
IMscin002: Final IMscin001 Part 2 and IMscin002 Analyses
Shawna Kraft, PharmD, BCOP:
Final IMscin001 Part 2 and IMscin002 analyses continued to support broadly similar efficacy, safety, and immunogenicity for atezolizumab SC and IV. In IMscin001 Part 2, at the final data cutoff of November 22, 2024, median OS was 10.9 months with atezolizumab SC vs 10.1 months with atezolizumab IV (HR: 1.00; 95% CI: 0.78-1.27). In IMscin002, at the final data cutoff of October 25, 2024, ongoing clinical benefit after cycle 16 was observed in 44.7% of patients, no new or unexpected safety signals were identified, and treatment-emergent antidrug antibody rates were similar with SC and IV atezolizumab.
CheckMate 67T: SC Nivolumab (+ Hyaluronidase) vs IV Nivolumab in Advanced/Metastatic ccRCC
Shawna Kraft, PharmD, BCOP:
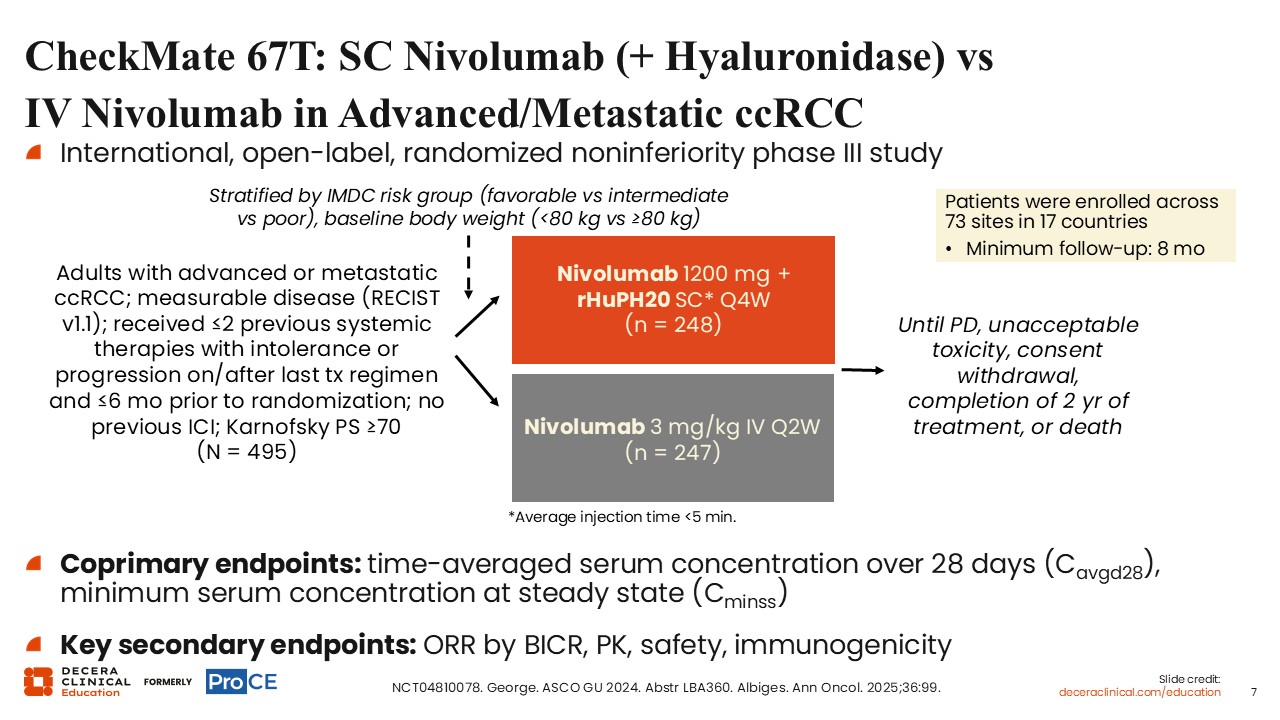
CheckMate 67T was an international, open-label, randomized noninferiority phase III study that compared SC and IV nivolumab in adults with advanced or metastatic clear cell renal cell carcinoma (NCT04810078).7,8 Eligible patients had measurable disease per RECIST v1.1, Karnofsky PS of at least 70, no previous ICI exposure, and up to 2 previous systemic therapies with intolerance or progression on or after the last regimen within 6 months before randomization. Patients were stratified by International Metastatic RCC Database Consortium risk group and baseline body weight and randomized across 73 sites in 17 countries to receive nivolumab 1200 mg plus rHuPH20 SC every 4 weeks or nivolumab 3 mg/kg IV every 2 weeks. Treatment continued until disease progression, unacceptable toxicity, consent withdrawal, completion of 2 years of treatment, or death. The coprimary endpoints were time-averaged serum concentration over 28 days in cycle 1 (Cavgd28) and minimum serum concentration at steady state. Key secondary endpoints included ORR by blinded independent central review (BICR), pharmacokinetic, safety, and immunogenicity.
CheckMate 67T: PK Noninferiority
Shawna Kraft, PharmD, BCOP:
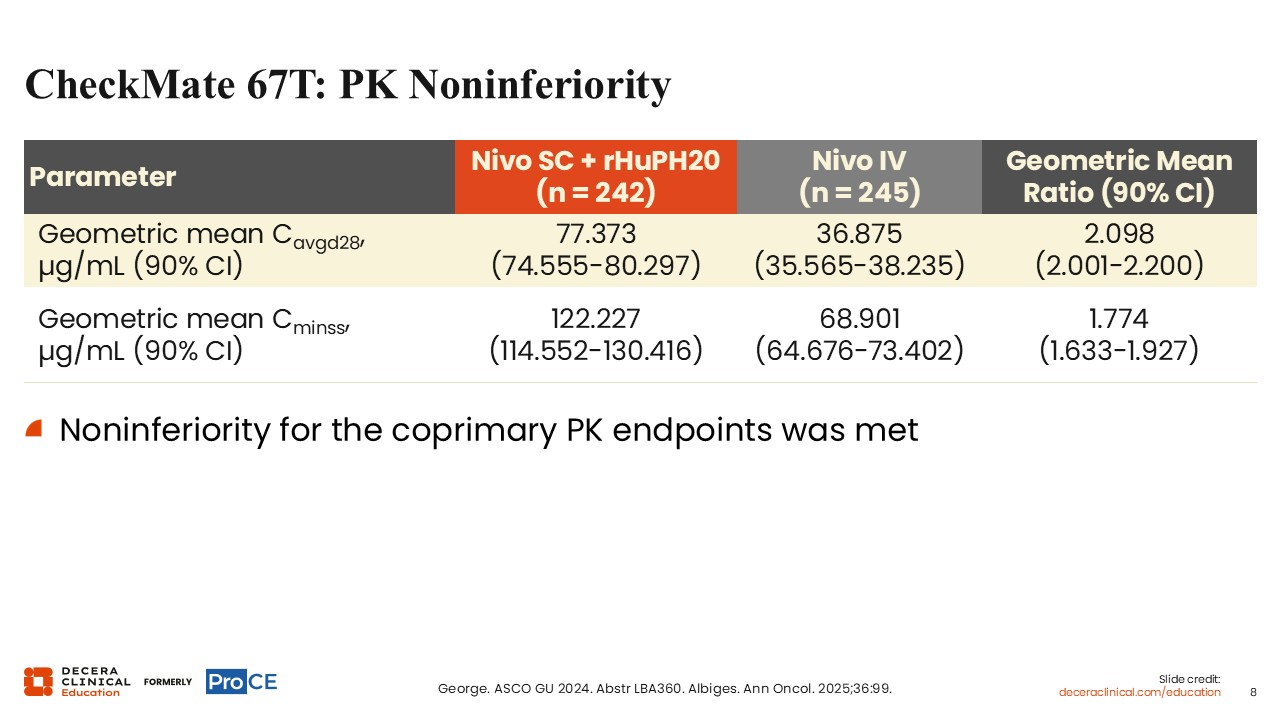
CheckMate 67T met noninferiority for both coprimary pharmacokinetic endpoints. Geometric mean Cavgd28 was 77.373 mcg/mL with SC nivolumab plus rHuPH20 vs 36.875 mcg/mL with IV nivolumab, with a geometric mean ratio of 2.098 (90% CI: 2.001-2.200). Geometric mean Cminss was 122.227 vs 68.901 mcg/mL, respectively, with a geometric mean ratio of 1.774 (90% CI: 1.633-1.927). Overall, these data supported noninferior pharmacokinetic exposure with the SC formulation.
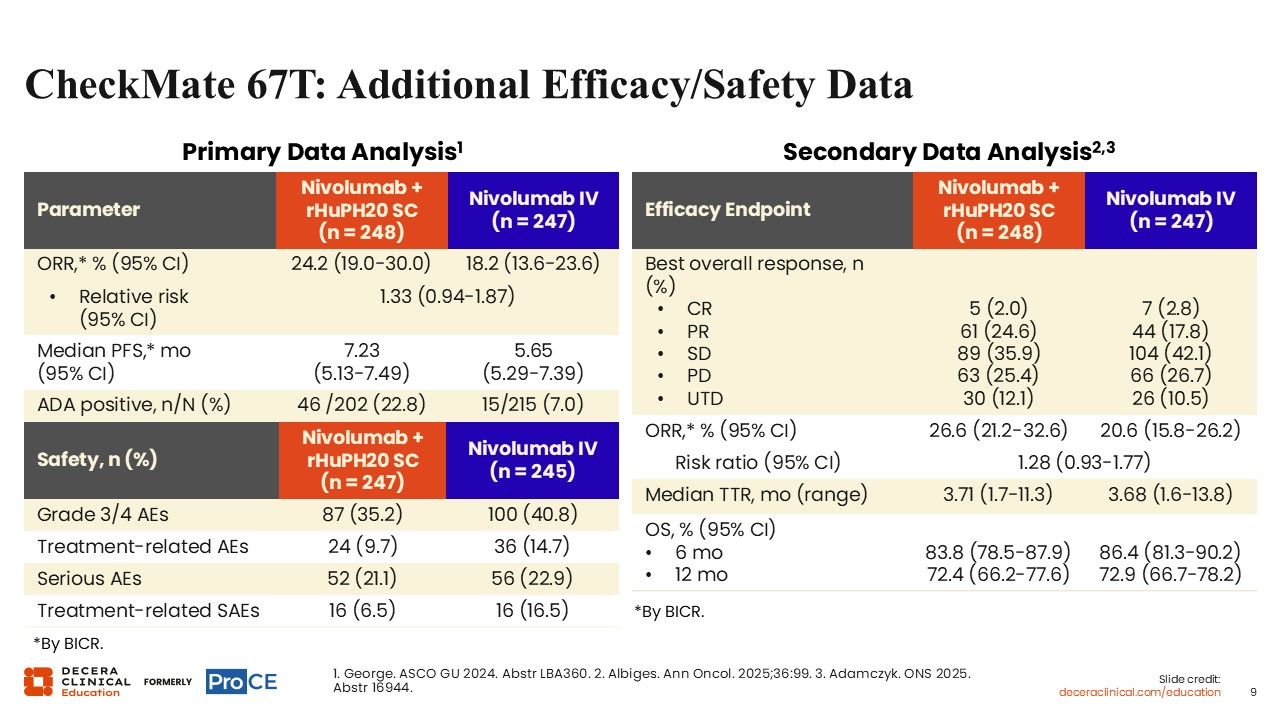
CheckMate 67T: Additional Efficacy/Safety Data
Shawna Kraft, PharmD, BCOP:
In CheckMate 67T, efficacy and safety outcomes were broadly comparable between the SC and IV nivolumab arms.7-9 In the primary data analysis, ORR by BICR was 24.2% vs 18.2% (relative risk: 1.33; 95% CI: 0.94-1.87), and median PFS was 7.23 vs 5.65 months (95% CI: 5.13-7.49 vs 5.29-7.39) for SC vs IV nivolumab, respectively. In the secondary data analysis, ORR was 26.6% vs 20.6%, median time to response was 3.71 vs 3.68 months, and OS rates at 6 months were 83.8% vs 86.4% and at 12 months were 72.4% vs 72.9%, respectively. Safety was also generally comparable, with grade 3/4 adverse events (AEs) reported in 35.2% vs 40.8%, treatment-related AEs in 9.7% vs 14.7%, and serious AEs in 21.1% vs 22.9%.
CheckMate 8KX: PROs With SC Nivolumab in Solid Tumors
Shawna Kraft, PharmD, BCOP:
CheckMate 8KX included an 8-item patient experience and preference questionnaire administered after treatment on Day 1 of cycles 1 and 2 in Parts A and B and on Day 1 of cycle 1 in Parts C and D. Most patients reported high satisfaction with SC nivolumab, preferred SC over IV administration, and reported limited pain associated with SC administration.
Most patients also reported that SC injection times were either shorter than expected or acceptable. Across the study, nivolumab SC was generally administered manually by syringe, with median injection times of 5 minutes or less. The exceptions were Part B Group 2 and Part B Group 4, in which nivolumab SC was administered by syringe pump and the median injection time was 30 minutes in each group.
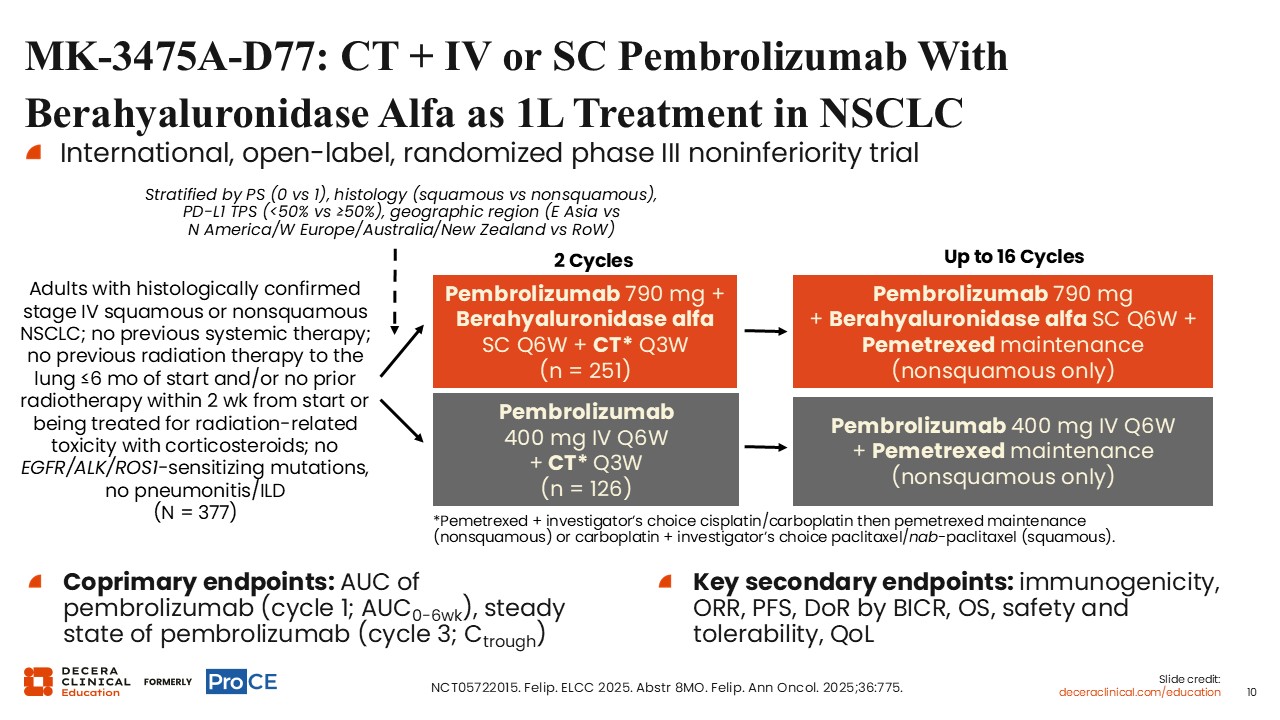
MK-3475A-D77: CT + IV or SC Pembrolizumab With Berahyaluronidase Alfa as 1L Treatment in NSCLC
Shawna Kraft, PharmD, BCOP:
MK-3475A-D77 was an international, open-label, randomized phase III noninferiority trial that compared SC pembrolizumab plus berahyaluronidase alfa with IV pembrolizumab, each given with chemotherapy, as first-line treatment for advanced NSCLC.10 Eligible patients were adults with histologically confirmed stage IV squamous or nonsquamous NSCLC; no previous systemic therapy; no sensitizing EGFR, ALK, or ROS1 alterations; and no pneumonitis or interstitial lung disease. Patients were randomized to receive pembrolizumab 790 mg plus berahyaluronidase alfa SC every 6 weeks or pembrolizumab 400 mg IV every 6 weeks, each with chemotherapy every 3 weeks for 2 cycles, followed by continued pembrolizumab for up to 16 cycles with pemetrexed maintenance in patients with nonsquamous disease. The coprimary endpoints were pembrolizumab AUC in cycle 1 and steady-state pembrolizumab Ctrough in cycle 3, with key secondary endpoints including immunogenicity, ORR, PFS, duration of response (DoR) by BICR, OS, safety and tolerability, and quality of life.
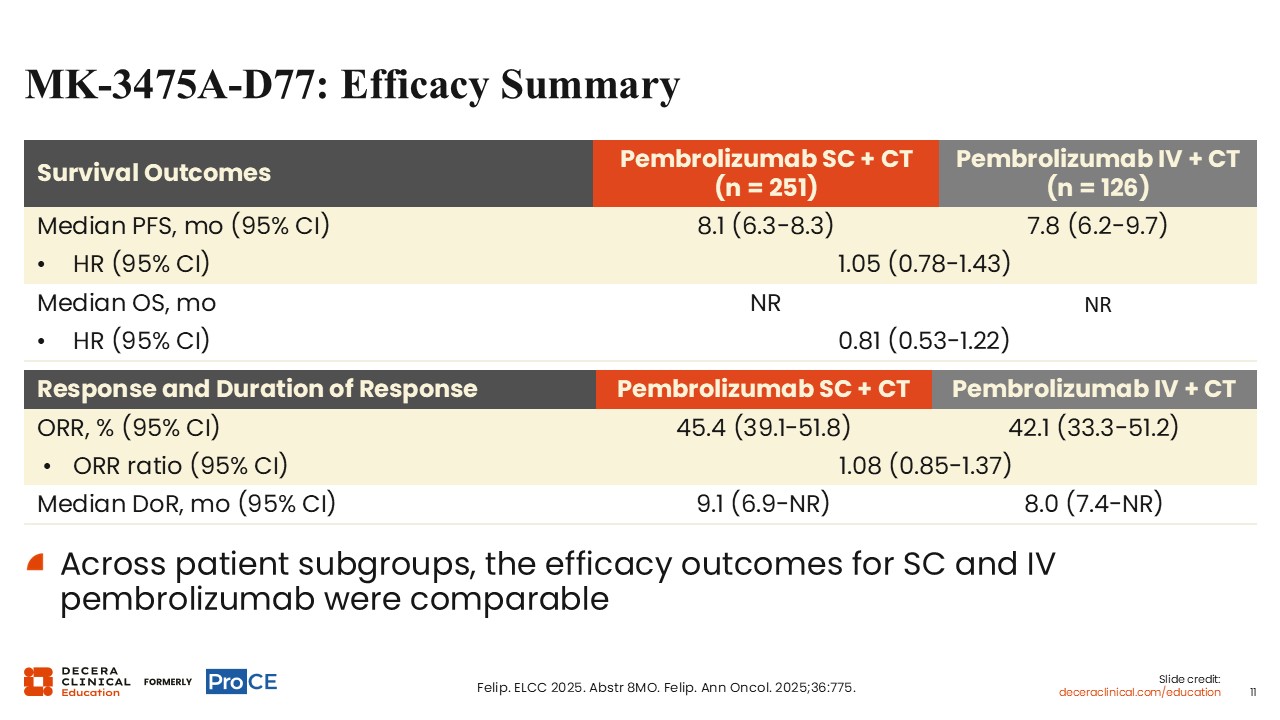
MK-3475A-D77: Efficacy Summary
Shawna Kraft, PharmD, BCOP:
Survival outcomes were similar between pembrolizumab SC plus chemotherapy (n = 251) and pembrolizumab IV plus chemotherapy (n = 126). Median PFS was 8.1 months (95% CI: 6.3-8.3) with SC pembrolizumab plus chemotherapy vs 7.8 months (95% CI: 6.2-9.7) with IV pembrolizumab plus chemotherapy, with an HR of 1.05 (95% CI: 0.78-1.43). Median OS was not reached in either arm, with an OS HR of 0.81 (95% CI: 0.53-1.22).
Response and DoR outcomes were also comparable. ORR was 45.4% (95% CI: 39.1-51.8) with SC pembrolizumab plus chemotherapy vs 42.1% (95% CI: 33.3-51.2) with IV pembrolizumab plus chemotherapy, with an ORR ratio of 1.08 (95% CI: 0.85-1.37). Median DoR was 9.1 months (95% CI: 6.9-NR) vs 8.0 months (95% CI: 7.4-NR), respectively. Across patient subgroups, the slide states that efficacy outcomes for SC and IV pembrolizumab were comparable.
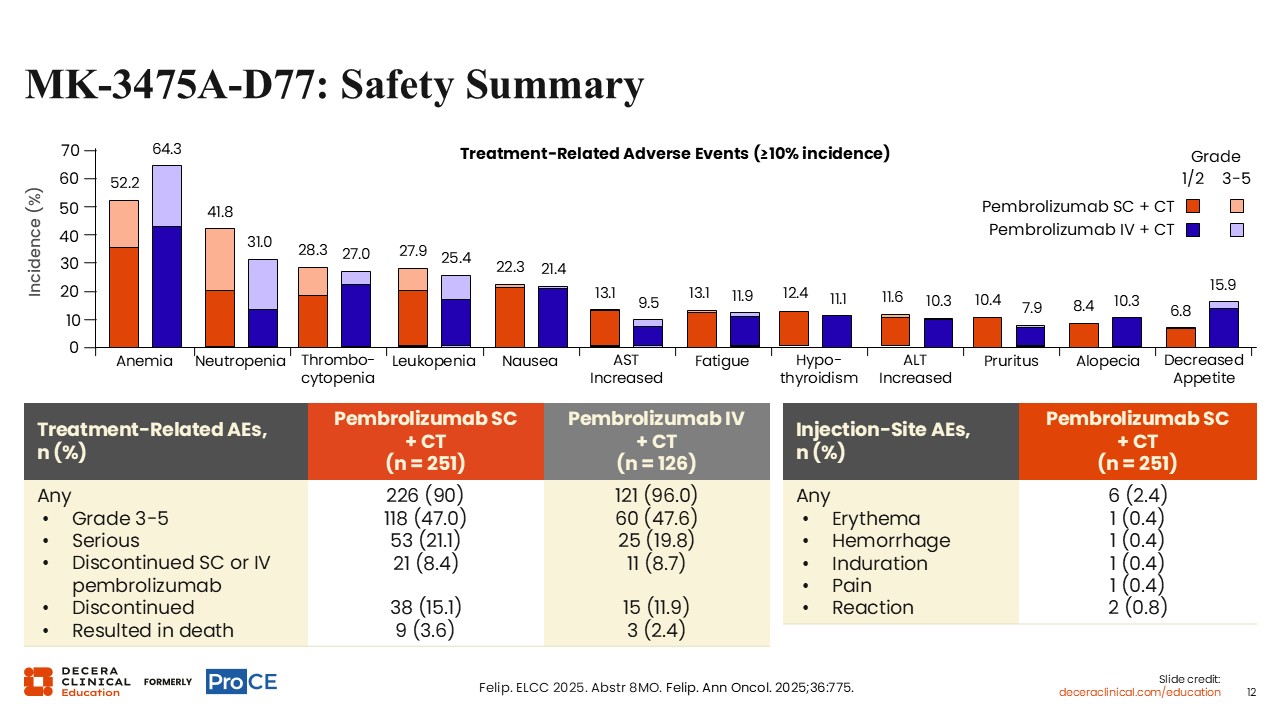
MK-3475A-D77: Safety Summary
Shawna Kraft, PharmD, BCOP:
Safety was generally comparable between the SC and IV pembrolizumab arms, with treatment-related AEs reported in 90.0% vs 96.0% of patients, grade 3-5 treatment-related AEs in 47.0% vs 47.6%, and serious treatment-related AEs in 21.1% vs 19.8%, respectively. Discontinuation of SC or IV pembrolizumab because of treatment-related AEs occurred in 8.4% and 8.7% of patients, whereas discontinuation of any treatment occurred in 15.1% and 11.9%, and treatment-related AEs resulting in death were reported in 3.6% and 2.4%, respectively.
Injection-site AEs with SC pembrolizumab were uncommon overall, occurring in 2.4% of patients, with individual events such as erythema, hemorrhage, induration, and pain each reported in 0.4% and injection-site reaction in 0.8%. Overall, these findings supported a broadly similar safety profile for the SC and IV pembrolizumab formulations.
MK-3475A-F11: Preference for IV or SC Pembrolizumab With Berahyaluronidase Alfa for the Treatment of Solid Tumors
Shawna Kraft, PharmD, BCOP:
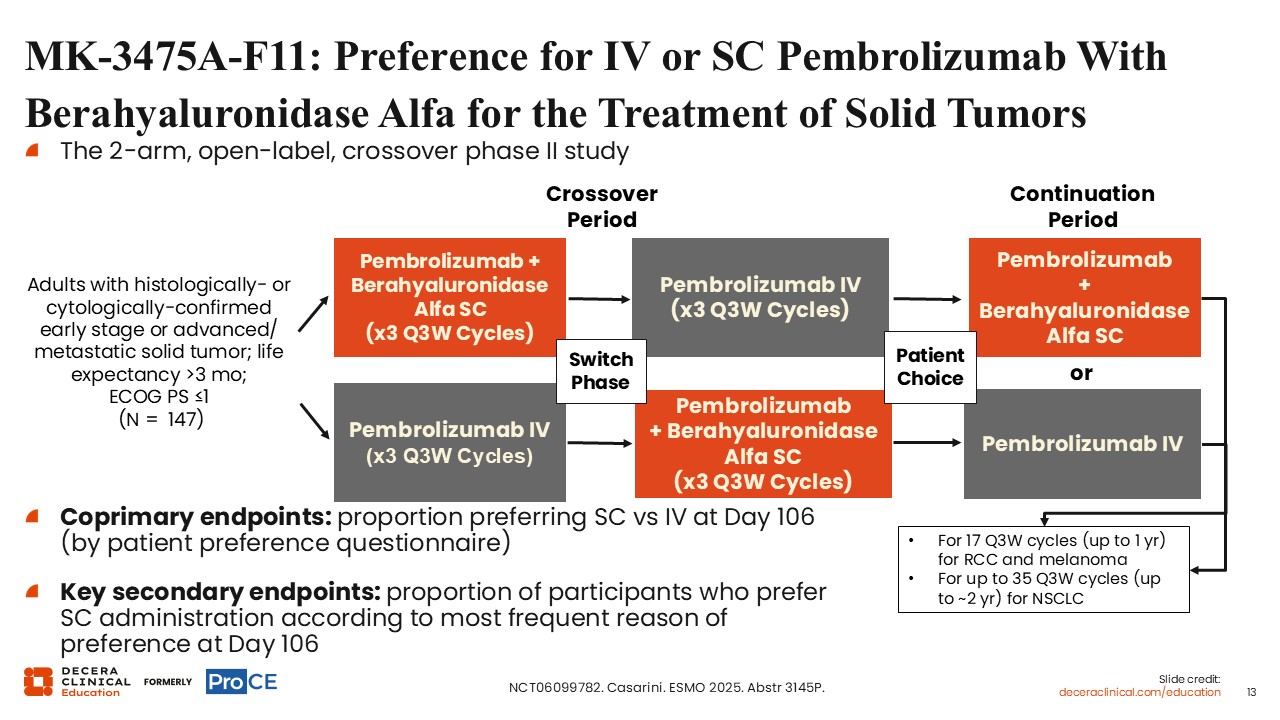
MK-3475A-F11 was a 2-arm, open-label, crossover phase II study evaluating preference for IV or SC pembrolizumab with berahyaluronidase alfa in patients with solid tumors (n = 147).11 Eligible adult patients had histologically or cytologically confirmed early-stage or advanced/metastatic solid tumor, life expectancy longer than 3 months, and ECOG PS ≤1.
Patients crossed over between pembrolizumab plus berahyaluronidase alfa SC for 3 every-3-week cycles and pembrolizumab IV for 3 every-3-week cycles. The continuation period allowed patient choice of pembrolizumab plus berahyaluronidase alfa SC or pembrolizumab IV for 17 every-3-week cycles for renal cell carcinoma and melanoma or up to 35 every-3-week cycles for NSCLC.
The coprimary endpoint was the proportion of patients preferring SC vs IV administration at Day 106, as assessed using a patient preference questionnaire. A key secondary endpoint was the proportion of participants who preferred SC administration at Day 106, categorized by the most frequently reported reason for that preference.
MK-3475A-F11: Patient Preference Results
Shawna Kraft, PharmD, BCOP:
Among 118 evaluable patients, the preference rate for SC pembrolizumab with berahyaluronidase vs IV pembrolizumab was 65% (95% CI: 56%-74%). Patients’ reasons for preferring SC pembrolizumab with berahyaluronidase vs IV pembrolizumab included less clinic time (64%), improved comfort during administration (62%), less injection-site pain (38%), and less emotional distress (21%).
Satisfaction results favored the SC formulation numerically. Approximately 64% and 25% of patients were very satisfied and satisfied, respectively, with the SC formulation, compared with approximately 54% and 31% who were very satisfied and satisfied with the IV formulation. More patients chose to continue SC pembrolizumab than IV pembrolizumab (68% vs 32%). Investigators suggested that together, results from the MK-3475A-D77 and MK-3475A-F11 studies support SC pembrolizumab as an alternative administration route with potential to improve patient satisfaction and convenience without compromising efficacy or safety compared with IV pembrolizumab.
MK-3475A-F84: IV or SC Pembrolizumab With Berahyaluronidase Alfa as 1L Tx for Metastatic NSCLC and High PD-L1 (TPS ≥50%)
Shawna Kraft, PharmD, BCOP:
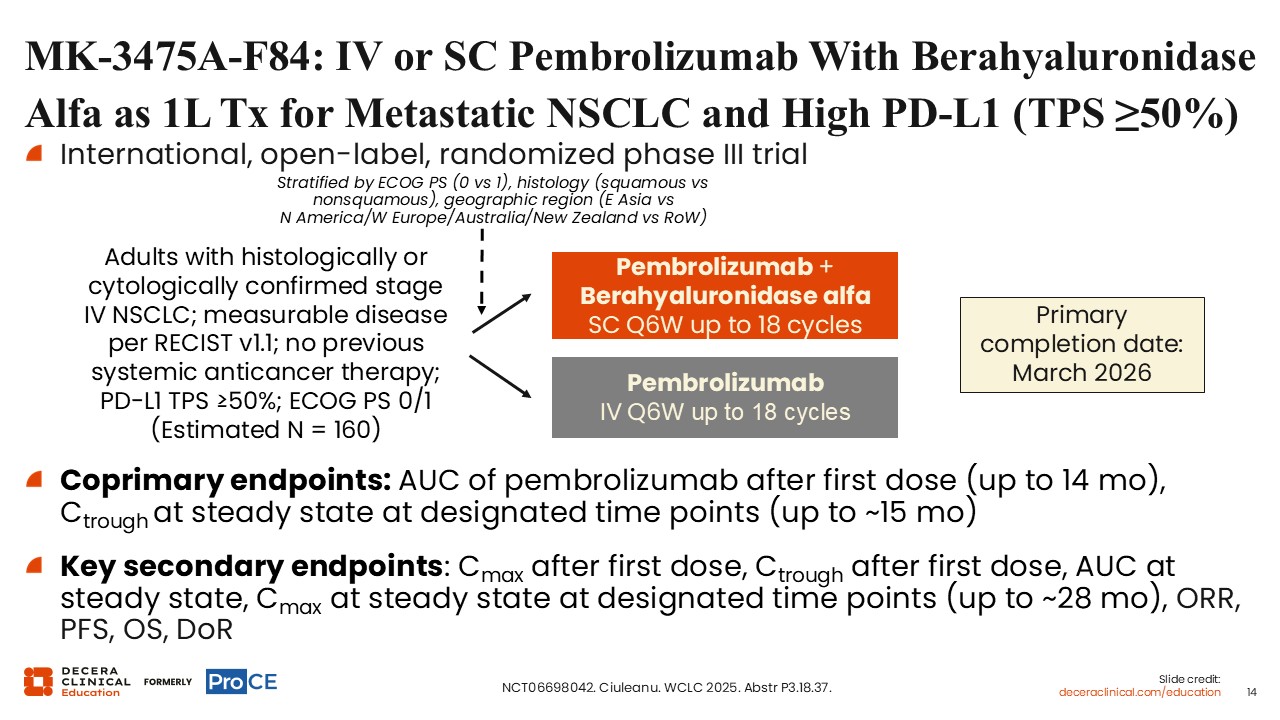
MK-3475A-F84 is an international, open-label, randomized phase III trial evaluating IV or SC pembrolizumab with berahyaluronidase alfa as first-line treatment for metastatic NSCLC with high PD-L1 expression, defined as tumor proportion score (TPS) of at least 50%. Eligible adults have histologically or cytologically confirmed stage IV NSCLC, measurable disease by RECIST v1.1, no previous systemic anticancer therapy, PD-L1 TPS at least 50%, and ECOG PS ≤1 were enrolled (n = 160). Patients receive pembrolizumab plus berahyaluronidase alfa SC every 6 weeks for up to 18 cycles or IV pembrolizumab every 6 weeks for up to 18 cycles. Stratification factors include ECOG PS, histology, and geographic region. Coprimary endpoints are pembrolizumab AUC after the first dose up to 14 months and Ctrough at steady state at designated time points up to approximately 15 months. Key secondary endpoints include Cmax after first dose, Ctrough after first dose, AUC at steady state, Cmax at steady state at designated time points up to approximately 28 months, ORR, PFS, OS, and DoR.
Other Clinical Trials of SC vs IV Immunotherapies
Shawna Kraft, PharmD, BCOP:
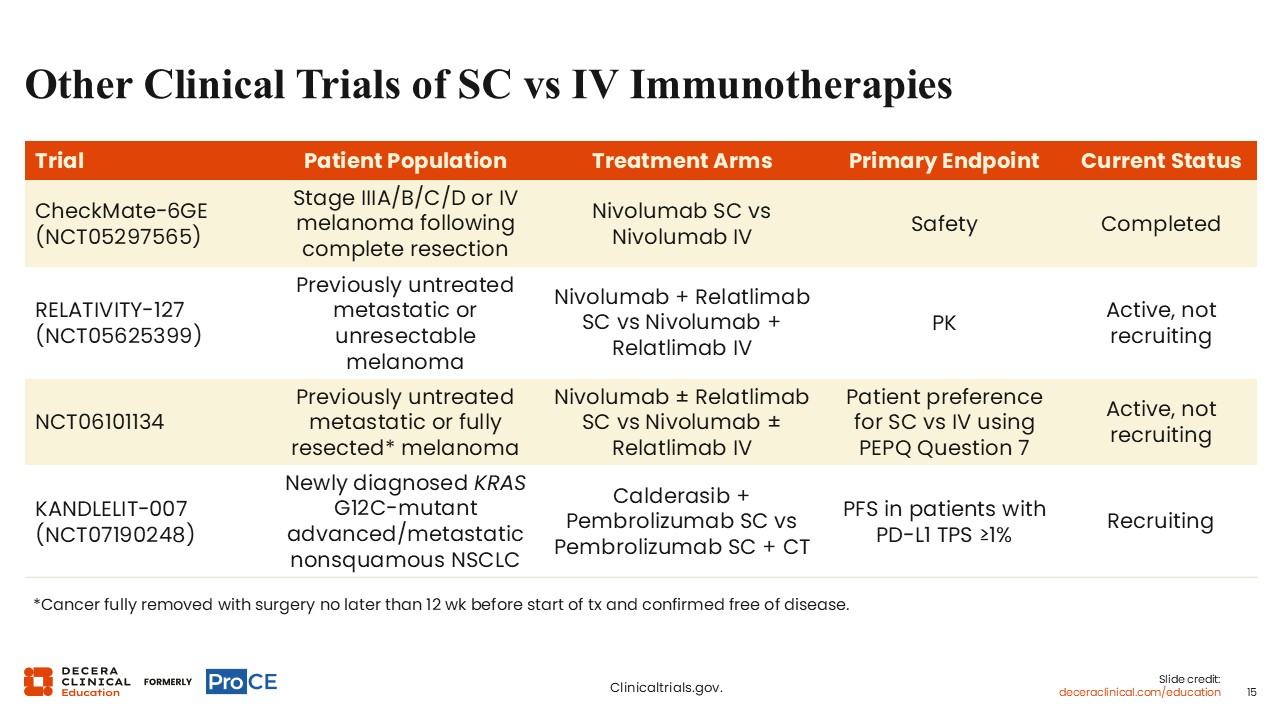
Additional clinical trials continue to evaluate outcomes including safety, pharmacokinetics, patient preference, and efficacy in various solid tumors.12
The phase III CheckMate-6GE (NCT05297565) evaluated nivolumab SC vs nivolumab IV in stage IIIA/B/C/D or IV melanoma after complete resection, with safety as the primary endpoint; the study is listed as completed.
The phase III RELATIVITY-127 (NCT05625399) is listed as active, not recruiting, in previously untreated metastatic or unresectable melanoma, evaluating nivolumab plus relatlimab SC vs nivolumab plus relatlimab IV with pharmacokinetics as the primary endpoint.
The phase II trial evaluating nivolumab with or without relatlimab SC vs nivolumab with or without relatlimab IV (NCT06101134) in previously untreated metastatic or fully resected melanoma, with patient preference for SC vs IV by PEPQ Question 7 as the primary endpoint, is currently active and not recruiting.
The phase III KANDLELIT-007 comparing calderasib plus pembrolizumab SC vs pembrolizumab SC plus chemotherapy in newly diagnosed KRAS G12C–mutant advanced or metastatic nonsquamous NSCLC (NCT07190248) is recruiting. The primary endpoint of the study is PFS in patients with PD-L1 TPS of at least 1%.
Takeaways
Shawna Kraft, PharmD, BCOP:
Taken together, the available data support SC ICI formulations as an emerging option that may reduce administration time and treatment burden while maintaining pharmacokinetic exposure, efficacy, and safety generally comparable to IV therapy in studied settings. For oncology pharmacists, the practical takeaway is to interpret these data by agent, regimen, and patient population, while incorporating patient preferences, safety monitoring, and site-of-care logistics into shared treatment planning.