CE / CME
Management of PBC Pruritus and Fatigue Symptoms
Pharmacists: 0.75 contact hour (0.075 CEUs)
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Released: March 18, 2026
Expiration: March 17, 2027

Activity
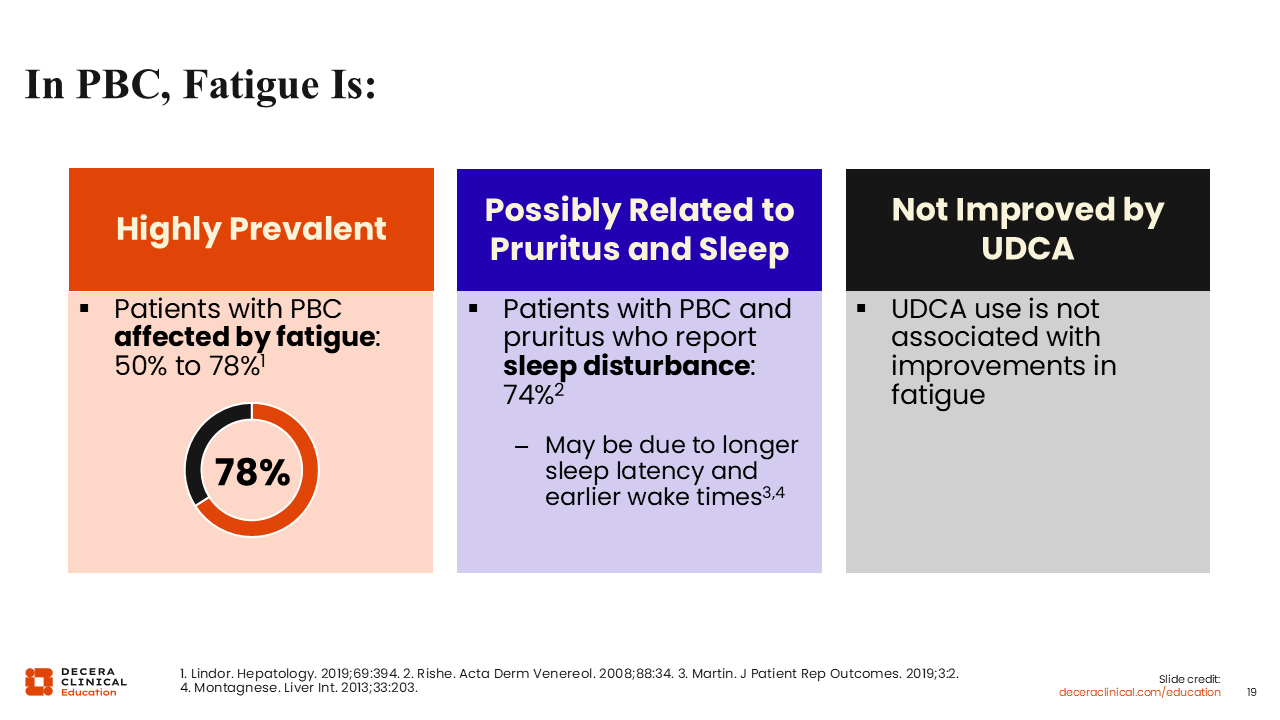
In PBC, Fatigue Is . . .
Fatigue is a real challenge for many patients with chronic disease and PBC in particular. Similar to pruritus, fatigue is highly prevalent among patients with PBC. Approximately 50% to 78% of patients report some degree of fatigue.2
The correlation between symptom burden and fatigue is complex. Some of the fatigue in PBC may be related to burden of pruritus and to pruritus keeping patients up at night. However, fatigue is not solely attributable to pruritus, and sleep disturbance is another important, complex component of PBC symptoms that should also be addressed independently.23-25
Fatigue, like pruritus, is not affected by traditional therapies for PBC, namely, UDCA.
I think fatigue is underrecognized for how much it contributes to social isolation and how much this can negatively affect quality of life for people with PBC. In my experience, patients with significant symptoms do not socialize. They do not have the energy to do the usual social activities that many of us engage in and often become isolated from friends and family.
Mechanisms of PBC-Associated Fatigue
In all, the key is to recognize that fatigue is complex in PBC. It may correlate with pruritus, but not always. Some patients report no itch but significant fatigue.26,27
The mechanisms of PBC-associated fatigue are complex and seem to involve both inflammation and cholestasis. Chronic inflammation, be it in the liver or anywhere else in the body, is sometimes associated with chronic fatigue in people with PBC. Cholestasis affects PBC symptoms in patients with disease activity, too.26,27
Other factors can affect fatigue as well. Comorbidities, like anemia, vitamin D deficiency, sleep disturbance, depression, and anxiety, affect fatigue.26,27
Evaluating Fatigue in PBC
As with pruritus, evaluating fatigue in patients with PBC consistently and objectively is important. However, it is a little bit more complex because fatigue can be affected by so many different factors. It can be challenging to distinguish PBC-related fatigue from fatigue caused by other conditions. Doing so first requires us to rule out other competing causes.2,28
I also consider conditions that can be affect patients’ sleep, like sleep apnea. Sleep apnea is very common, and I generally ask patients or their partners whether they have a history of snoring or restlessness at night. If so, I generally recommend that they follow up with their primary care HCP to arrange a sleep study.2,28
As noted earlier, pruritus can cause sleep disruption, particularly because these symptoms are often worse at night. Sicca syndrome, or dryness, can also interrupt patients’ sleep and affect day-to-day functioning and energy levels.2,28
Ultimately, I think being systematic about ruling out and addressing other causes of fatigue is an important first step before attributing fatigue to PBC.
Characterizing Fatigue in PBC
As alluded to earlier, characterizing fatigue in PBC is more clinically challenging than pruritus because patients describe it more vaguely.
In my experience, that can range from “I'm tired; I can't do my day-to-day activities” to “My battery is just depleted. I cannot get through the full day, whether I nap or not. By midday, I have nothing left.” I find that once I rule out the other treatable causes of fatigue, that type of description persists.
It is also critical to understand the impact that fatigue has on individual patients. Are they able to socialize, work, and do their routine day-to-day activities? Characterizing how fatigue affects each individual and monitoring that over time is crucial for managing this symptom.2,28
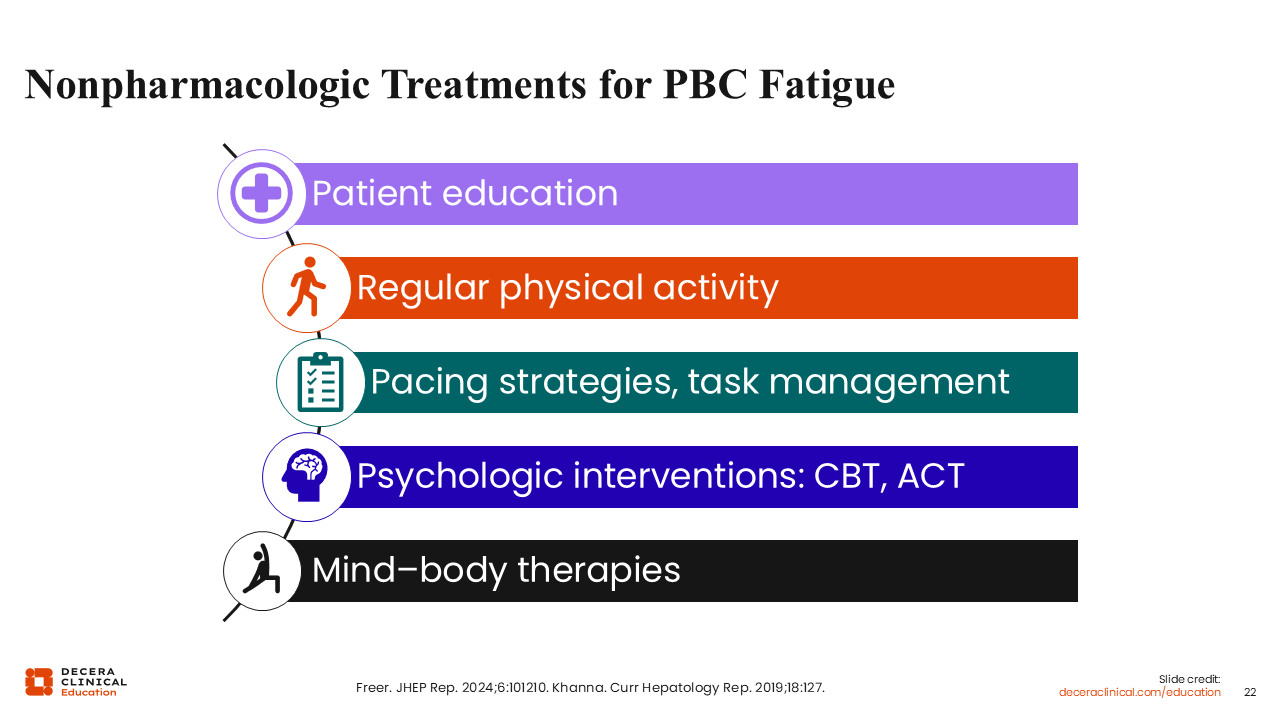
Nonpharmacologic Treatments for PBC Fatigue
As with pruritus, for treatment of fatigue in PBC, I begin with nonpharmacologic options.
The first step is patient education. I think validating patients’ fatigue symptoms, teaching them that this is part of their disease, and acknowledging that it is impactful are paramount. That validation of impact by their HCP can help build trust and make patients feel less isolated.29
Although perhaps counterintuitive, regular physical activity is important. If patients do not have energy, they are less likely to engage in physical activity, which can be associated with further reductions in energy. It is a cycle: The less you do, the less you want to do. Conversely, regular exercise can help build strength and stamina.30
Pacing strategies and task management can help patients learn to manage their symptoms. Every patient is different, and I tell them they know their body best. They need to understand what they are able to do and structure their days such that they are able to get tasks done. This means prioritizing and pacing oneself, making sure to have good sleep hygiene, and trying to get the best sleep possible.29
Fatigue and difficulty being able to perform day-to-day functions can affect mood and cause frustration, thereby impacting family and work life. This can further exacerbate depression and anxiety. Thinking outside the box and using cognitive behavioral strategies may be helpful here for patients’ mental health.29
There are also programs for mind–body wellness that engage elements of cognitive behavioral therapy in addition to physical activity and peer support to help patients with chronic disease manage some of the associated symptoms. Trials investigating such interventions have reported some benefits, and I am hopeful that they will continue to show benefit moving forward.31,32
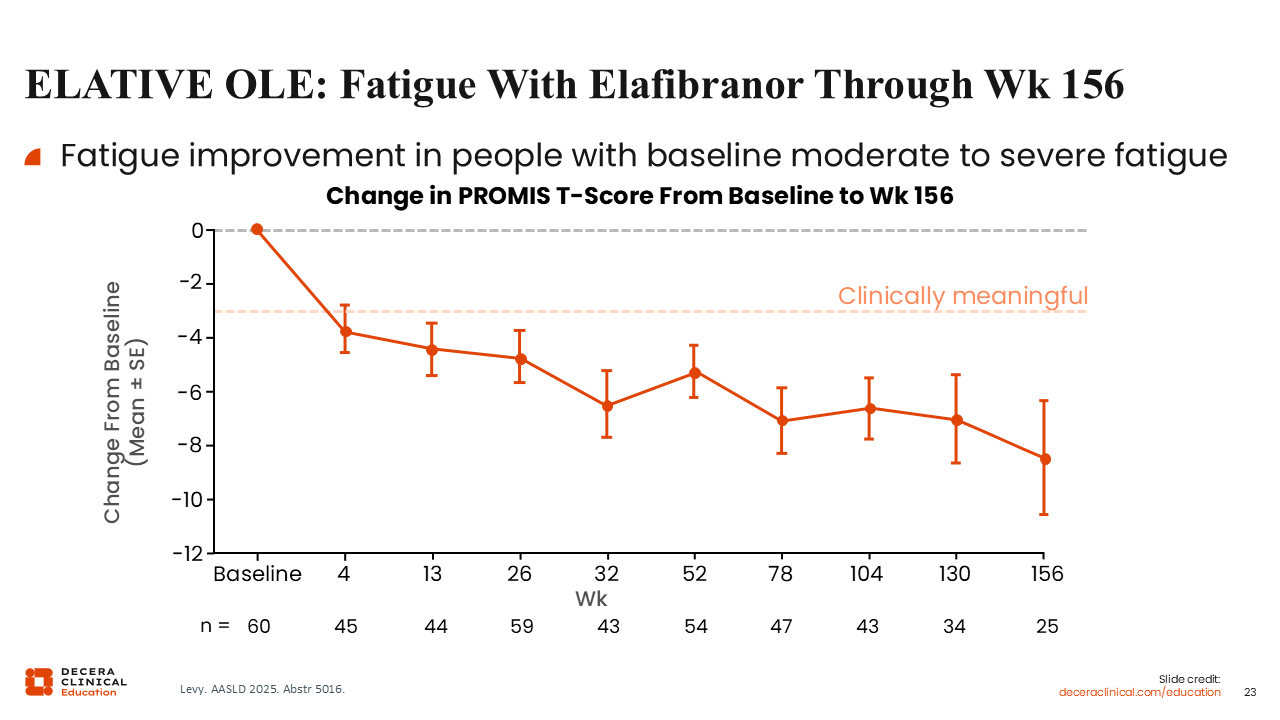
ELATIVE OLE: Fatigue with Elafibranor Through Week 156
We already briefly looked at the data on how novel PPAR agonists affect PBC pruritus; let’s now consider how they affect fatigue.
Data from the ELATIVE open-label extension show fatigue improvement in patients with moderate to severe fatigue at baseline through 156 weeks of treatment with elafibranor.18
This improvement in fatigue parallels the improvement in pruritus, although I think how much these trends are correlated still needs to be teased out. Another caveat to these data is that there is no placebo in the open-label extension to document if fatigue changes over time in patients without treatment.18
In all, I believe these data show a potential improvement in fatigue with elafibranor, but I find these data a little bit less robust than for pruritus. However, there are not many effective options for treatment of fatigue in PBC, so if there is potential for improvement in symptoms with elafibranor, I would still offer it to patients despite the lack of robust evidence.
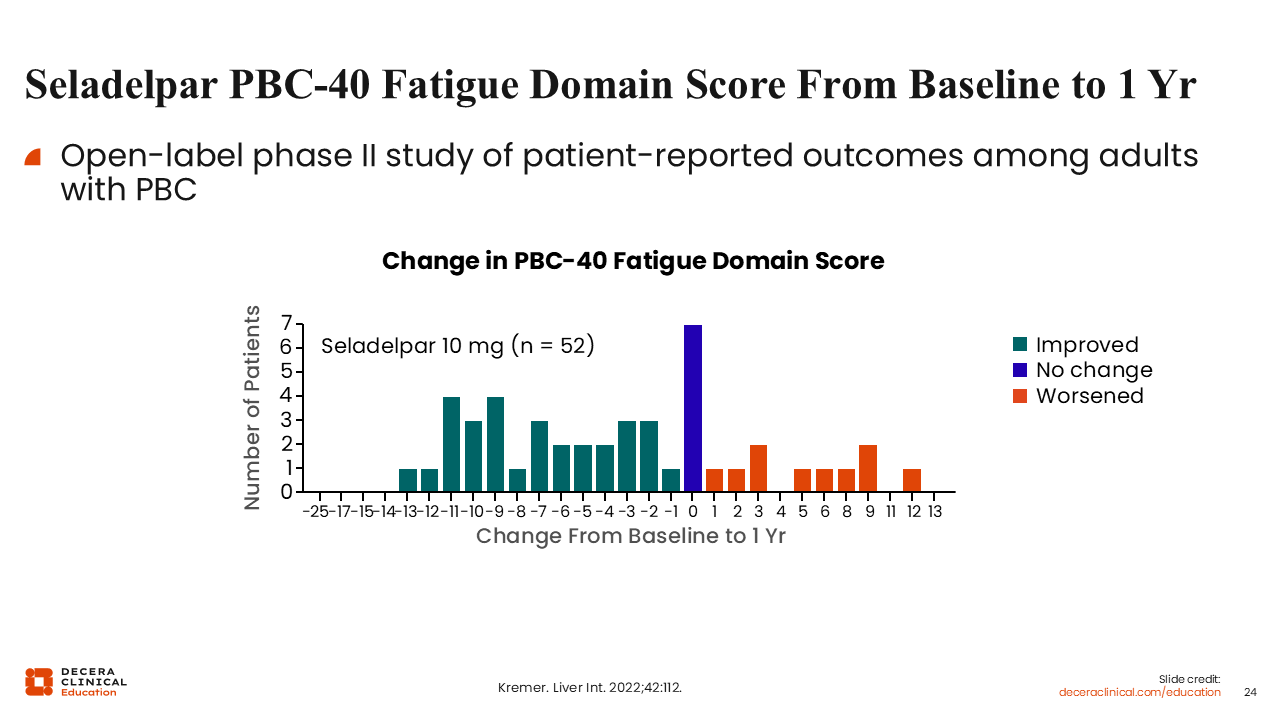
Seladelpar PBC-40 Fatigue Domain Score From Baseline to 1 Year
There are also data on fatigue effects with seladelpar. This open-label phase II study evaluated the change in PBC-40 fatigue domain score in people with PBC from baseline to after 1 year of treatment with seladelpar.33
Some patients’ symptoms of fatigue improved, some did not change, and some worsened. To me, it is difficult to parse out if these changes were a result of the natural history of their disease because of the lack of placebo. So, I think how this correlates with improvements in practice remains to be seen.33
Overall, there may be improvement in fatigue with the novel PPAR agonists, but the mechanism behind that benefit and the robustness of that benefit over time remain to be seen.
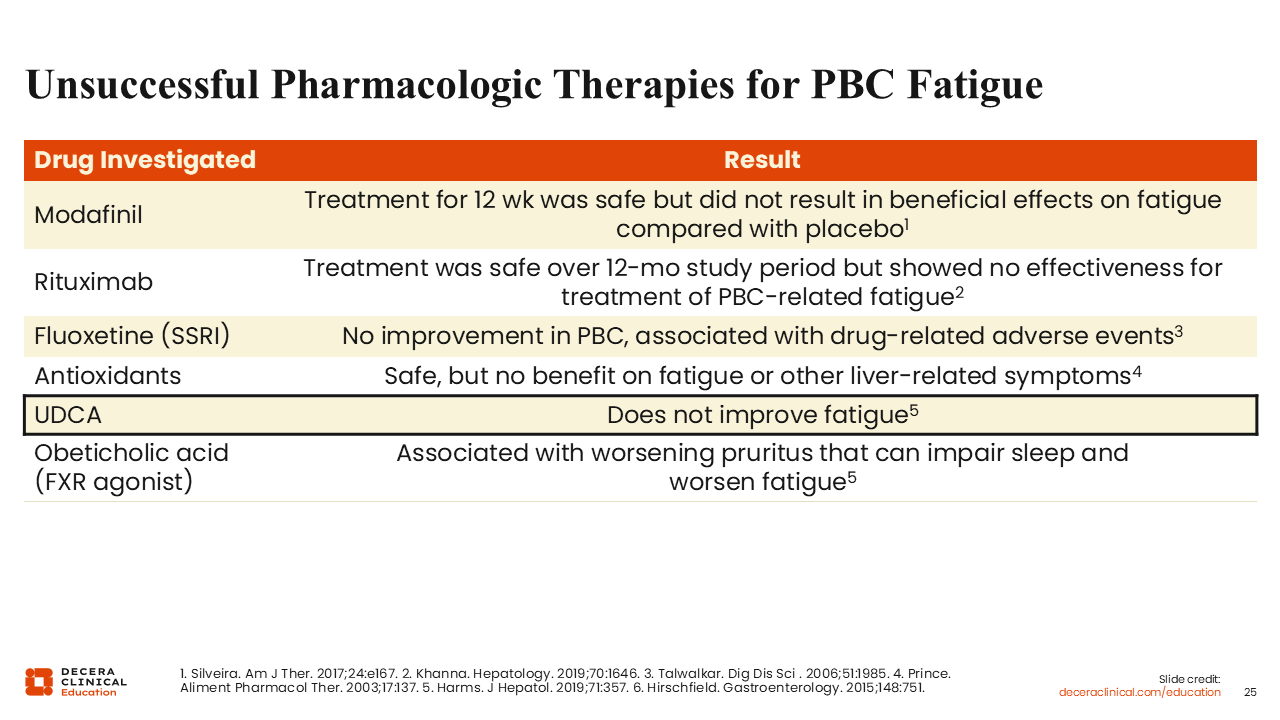
Unsuccessful Pharmacologic Therapies for PBC Fatigue
Beyond the novel PPARs we just discussed, most drugs that have been studied for fatigue in patients with PBC were ineffective. That includes drugs like modafinil, rituximab, selective serotonin reuptake inhibitors, and antioxidants. As mentioned, drugs that treat disease do not necessarily improve symptoms, and UDCA and farnesoid X receptor agonists should not be expected to improve fatigue in patients with PBC.34-39
It is unfortunate, but we do not have any reliably beneficial options right now for treatment of fatigue in patients with PBC. However, there is a lot of clinical interest in improving symptoms of fatigue, and I think that the treatment landscape will change in the coming years.
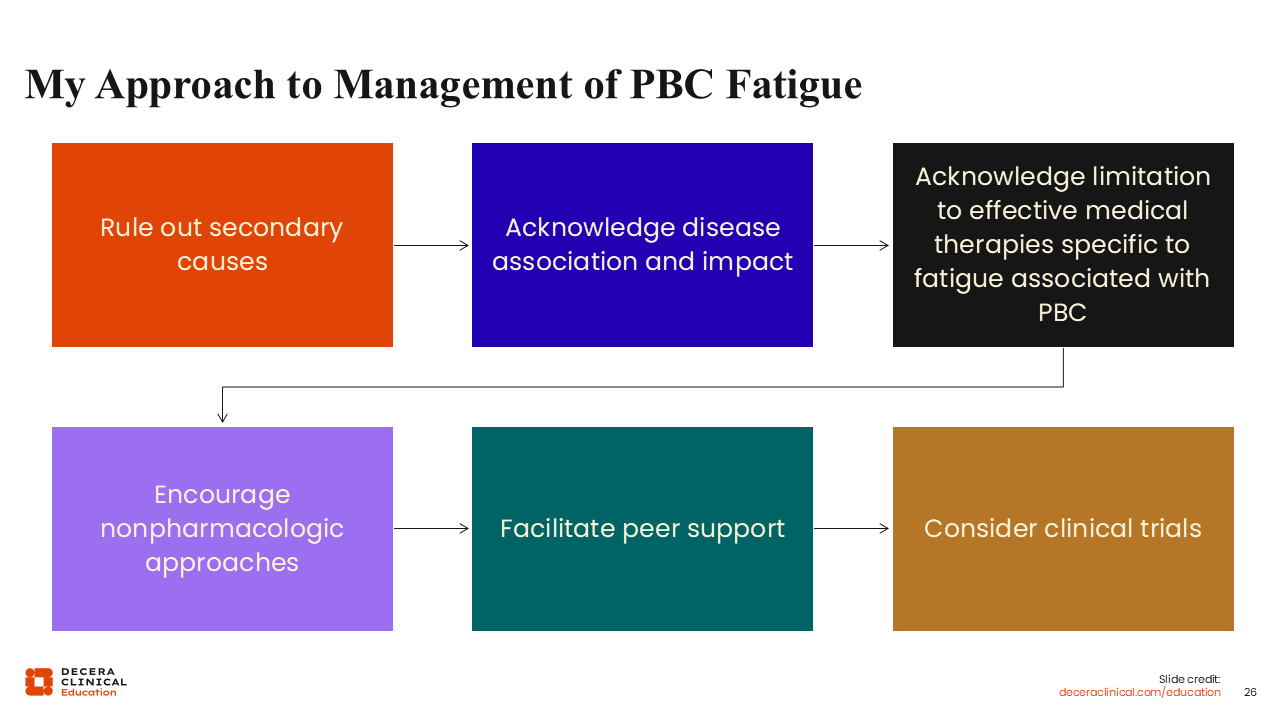
My Approach to Management of PBC Fatigue
My approach to fatigue follows the same basic principles as my approach to managing pruritus. The key is asking patients about their symptoms and objectively evaluating symptoms on a consistent basis. Before treating PBC fatigue, it is important to rule out secondary causes because fatigue is so prevalent and the differential diagnosis for fatigue is so complex.
Next, acknowledging the disease association and the impact on patients is validating and is an important part of disease management. It is okay to acknowledge the lack of reliable pharmacologic interventions specific for fatigue. I tell patients that perhaps novel PPAR agonists may affect fatigue in some way, be it related to pruritus or not, but that more studies must be done to be sure. Recognizing the symptom impact and lack of reliable treatment is helpful for building patient–HCP trust. I let my patients know that, as a community, we are working on understanding fatigue better in PBC.
I also encourage nonpharmacologic options like physical activity, practicing good sleep hygiene, prioritizing tasks, and understanding one’s own limitations. Cognitive behavioral therapies and mind–body wellness approaches can be very helpful for patients.
I also actively facilitate peer support, as having a rare disease can be extremely isolating. Chronic disease and chronic symptoms can make it difficult to function and socialize or even to want to socialize. Connecting with other people who have that same experience, whether that be through patient support programs or online programs, is very valuable. I find that peer support can be very impactful for patients.
Finally, I advise HCPs to consider clinical trials for patients experiencing PBC fatigue. In addition to pharmacologic clinical trials, there are trials evaluating wellness through exercise, peer support, and cognitive behavioral therapies that are enrolling patients with PBC to examine the benefit of mind–body wellness in improving symptoms. One example is the eMPower study evaluating mind–body wellness with strategies of exercise, peer support, cognitive behavioral interventions, and wellness on impact on fatigue, stress, and overall mental well-being (NCT06861465).
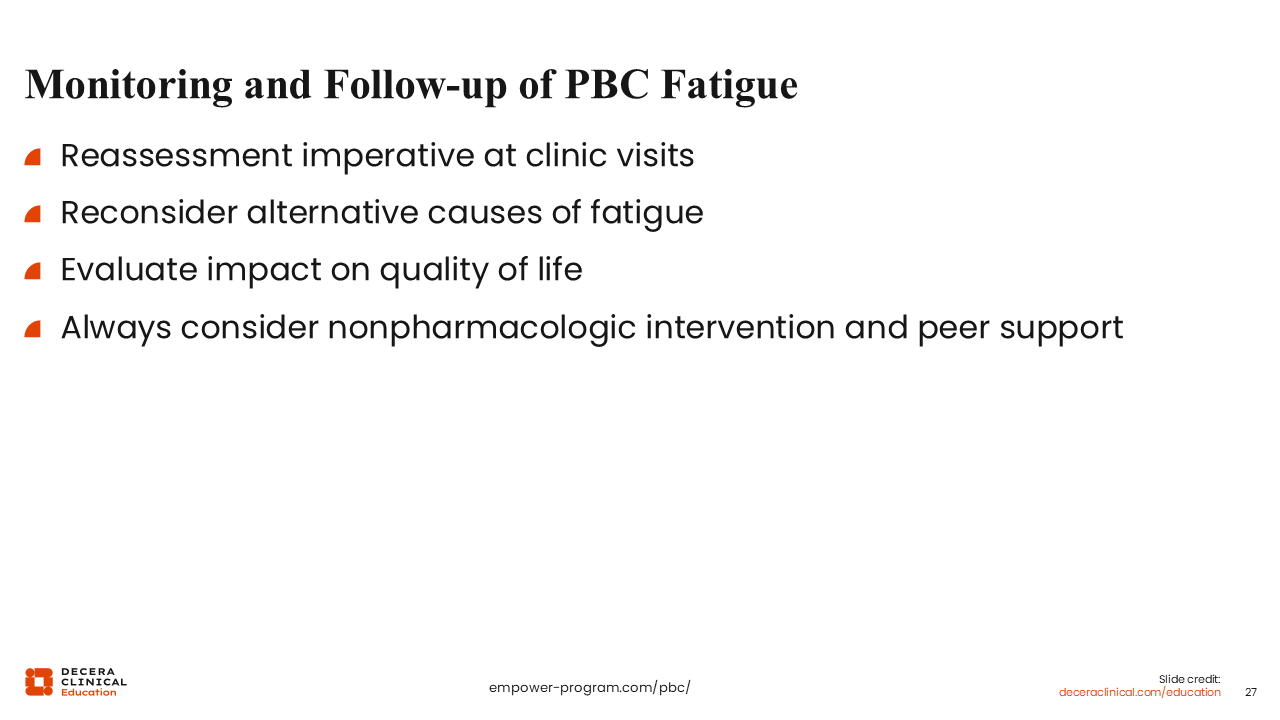
Monitoring and Follow-up of PBC Fatigue
Also similar to the management of PBC pruritus, being consistent and objective about monitoring and follow-up of PBC fatigue is important. Revisit the topic on a routine basis at each clinic visit.
If patients’ symptoms change, go back to the beginning. See whether anything changed in their medical history. Assess their thyroid function and determine if they need titration of medication. The question to ask whether something affected the trajectory of their symptoms, and can you modify treatment to improve their quality of life?
I also recommend reconsidering alternative causes of fatigue when symptoms change and evaluating if the impact on quality of life and patients’ day-to-day function has changed. Disruption of daily activities can start the cycle of impact on social isolation and mood, which becomes difficult to break out of if these changes are not addressed as they come up.
Finally, I think we should always consider nonpharmacologic treatment options and peer support. There is nothing to lose, and everything to gain if one of these interventions havs a positive impact on quality of life.
PBC Fatigue Take-home Points
Fatigue is a common and often highly burdensome symptom in PBC that can significantly impair daily functioning, work, social engagement, and quality of life, and it should be assessed routinely even when biochemical disease control appears adequate.
Because fatigue in PBC is multifactorial, we should systematically evaluate for contributing factors before attributing symptoms solely to PBC. Management should be individualized and begin with validation of the patient’s experience.