CE / CME
Management of PBC Pruritus and Fatigue Symptoms
Pharmacists: 0.75 contact hour (0.075 CEUs)
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Released: March 18, 2026
Expiration: March 17, 2027

Activity
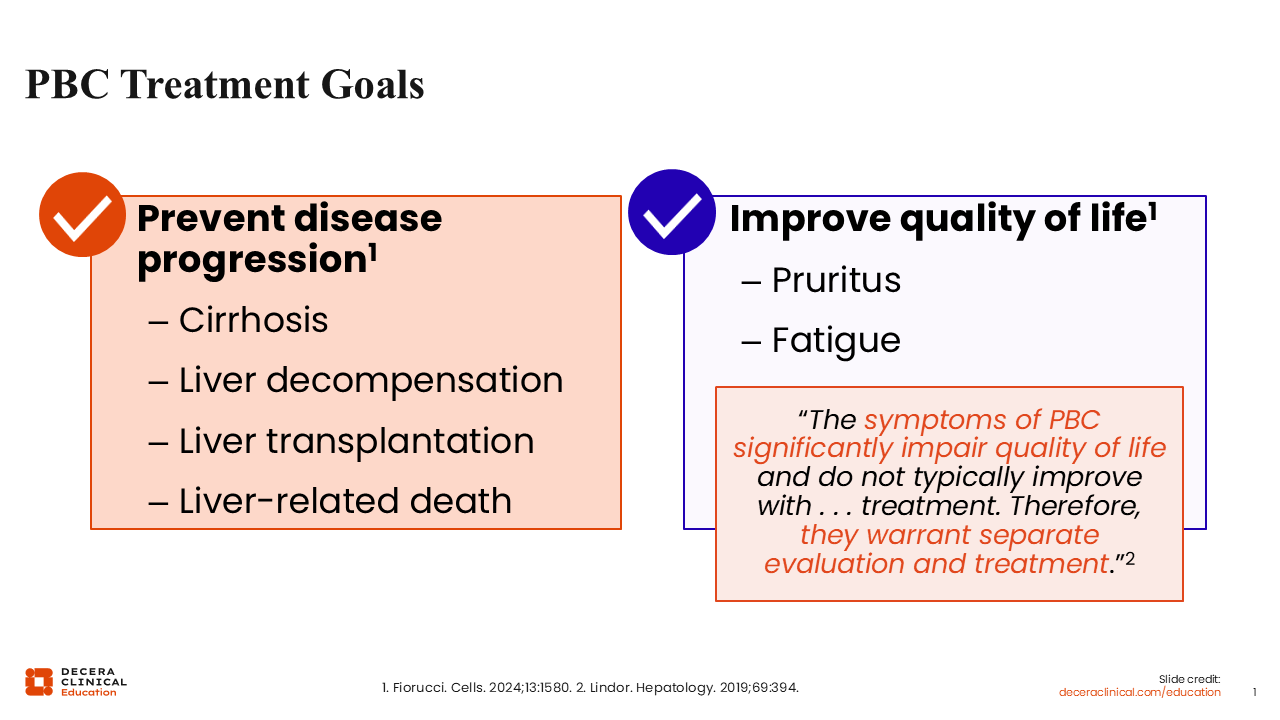
PBC Treatment Goals
Treatment goals in PBC are multifaceted. I think it is important for every HCP caring for patients with PBC to think about things in 2 realms.
The first is preventing disease progression. That includes preventing negative outcomes like cirrhosis, decompensation and liver-related outcomes.1,2
The second is addressing symptom burden, which can significantly affect quality of life and is critically important to evaluate.
Disease progression does not always parallel symptom burden. Thus, it is key to evaluate symptoms, to address them with patients, and to manage them to the best of our ability, independently of disease progression. That includes symptoms of pruritus and fatigue.1,2
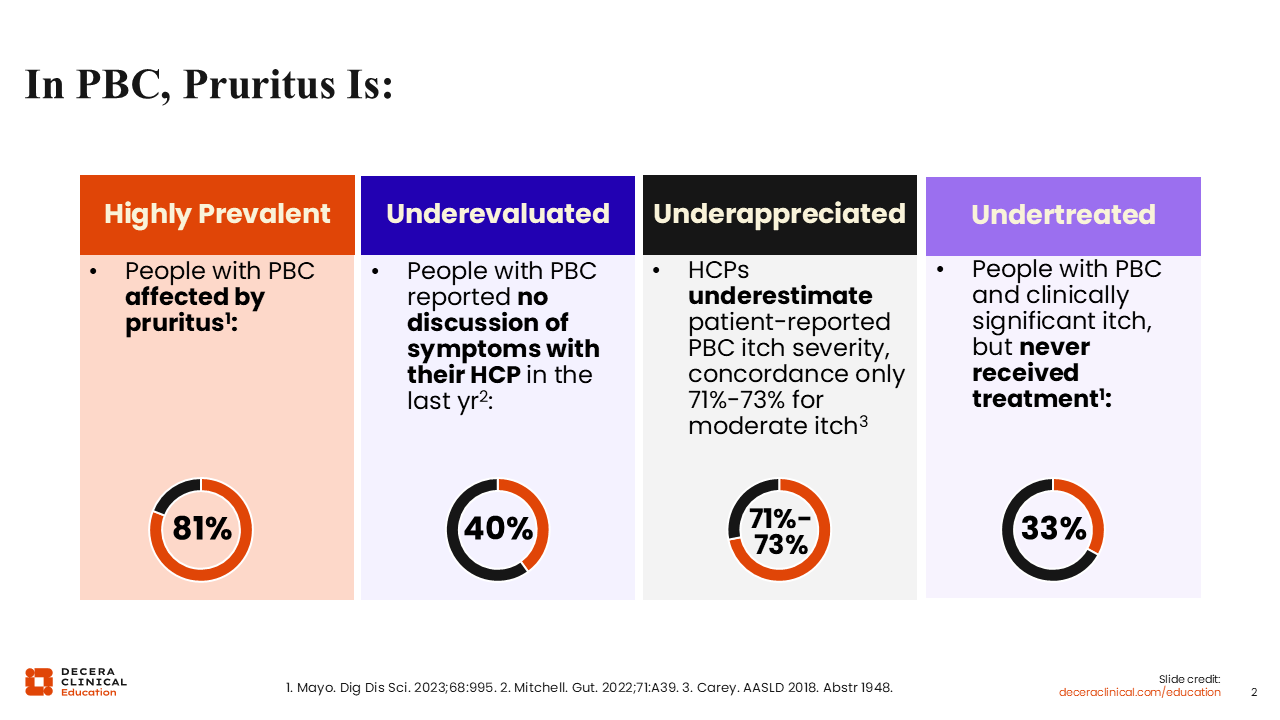
In PBC, Pruritus Is . . .
Pruritus is highly prevalent in PBC. Most patients are affected by pruritus, ranging from mild or moderate symptoms to significantly impactful, severe symptoms.3
Many symptoms of PBC, including pruritus, are underevaluated and underappreciated by HCPs: There is often a dissonance between the significance that HCPs place on symptom burden and the severity of symptoms that patients experience. That is why we must try to be objective about what patients are experiencing to ensure that patients and HCPs are speaking the same language when patients are describing what they are feeling.4,5
Symptoms are undertreated for many reasons, including lack of effective and tolerable treatment options, but also in part because of patient preference. Patients may have concerns about adverse effects or drug–drug interactions and may decline therapy for those reasons despite a significant burden of symptoms.3
Several studies have examined the impact of pruritus on patient quality of life and day-to-day activities. Between 44% to 88% of people surveyed report significant disruptions to 4 key areas: having a social life, doing activities at home and running errands, sleeping, and functioning at work or at school.3
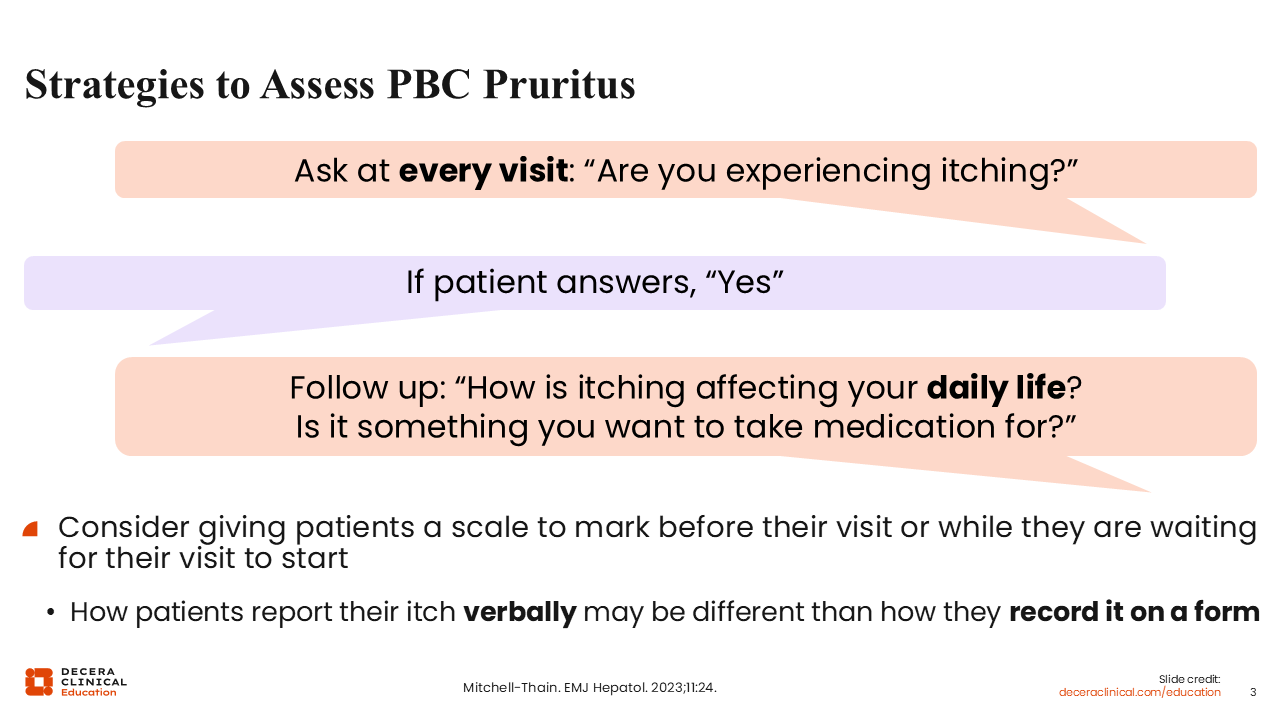
Strategies to Assess PBC Pruritus
It is very easy for us to look at blood tests and determine whether PBC disease is controlled or not controlled, but this does not always parallel the symptom burden patients are experiencing.
Alongside managing disease activity, we must objectively ask about and monitor symptoms, including pruritus. This way, it is possible to assess change in response to therapy and any change or impact on quality of life over time.6
There are straightforward strategies to assess PBC pruritus. As HCPs, although it is important that we ask patients if they are experiencing itch, formal assessment is important since they may report pruritus differently.
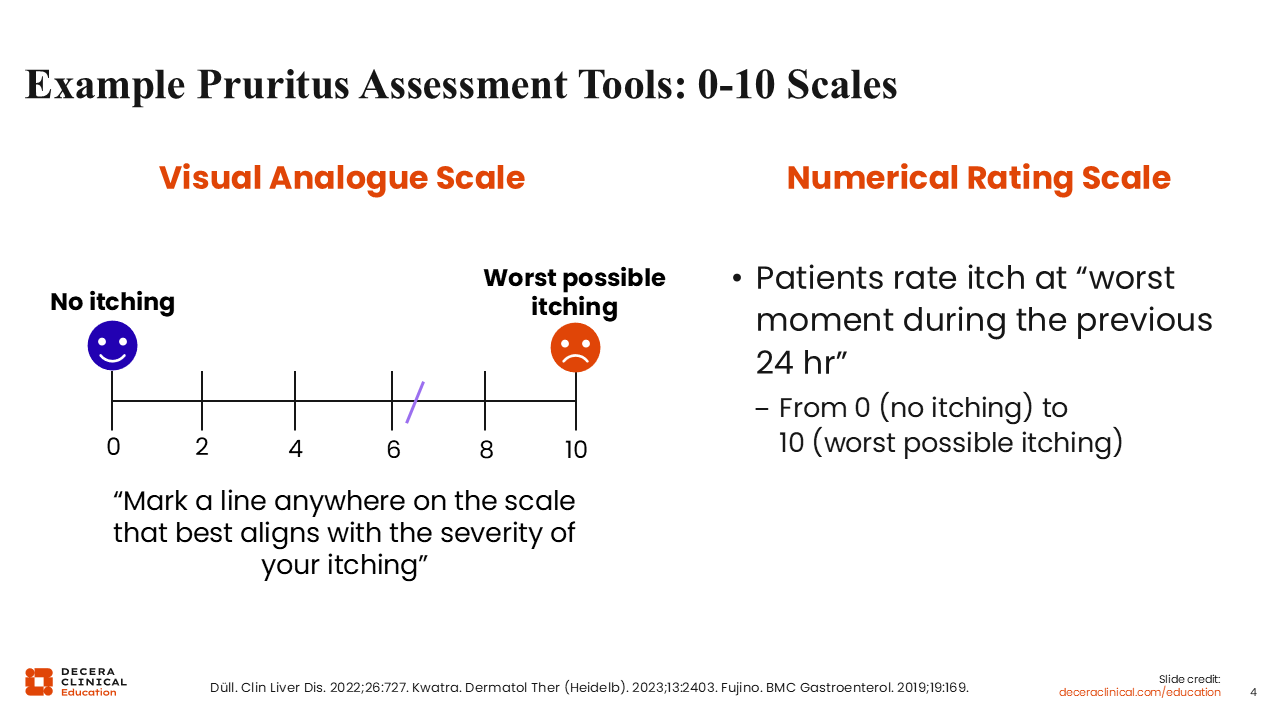
Example Pruritus Assessment Tools: 0-10 Scales
Beyond simply asking about itch, there are several scores used to quantify itch. The key is to use an easy, simple, and reproducible method to monitor and evaluate response at every visit.7-9
When documenting itch, we should be objective and be consistent about monitoring treatment response and symptom burden. You can simply ask “on a scale of 1 to 10, what is the worst itch you have had in the last 24 hours.” This is very quick, objective, and easy for patients to understand.
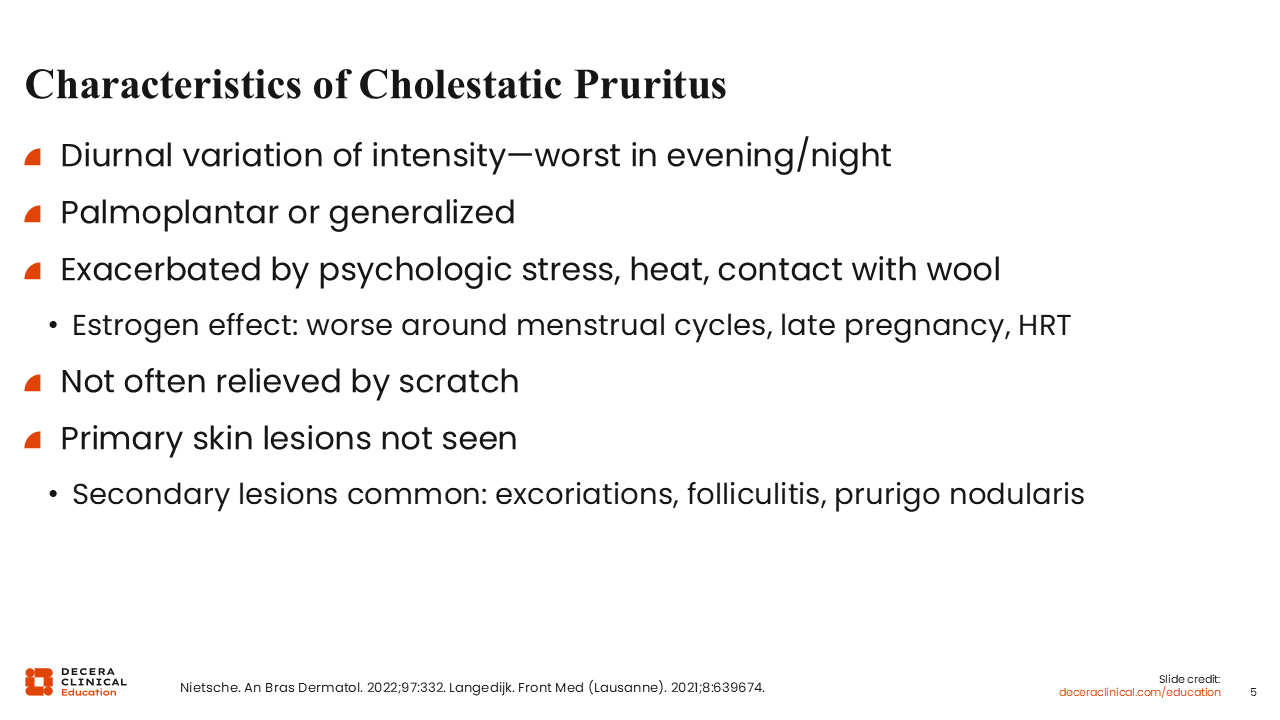
Characteristics of Cholestatic Pruritus
To identify cholestatic pruritus, I first try to rule out other causes of itch, such as a pruritic rash, excoriations, prurigo, folliculitis, allergies, dryness, atopic dermatitis, and eczema. Then, I ask if they have these classic features of cholestatic pruritus: nighttime predominance, localization to the palms and soles, and deep itch not relieved by scratching. I also check for secondary manifestations, like excoriations, which relies on taking a patient history and clinical exam.10,11
Sometimes it can be challenging to determine if pruritus is being caused by PBC or by other factors. If I have patients whose pruritus could be aggravated by factors other than PBC, such as dryness, atopy, or allergies, I think it is reasonable to try managing those issues to see if that resolves the itch.
It is normally straightforward to rule out atopic dermatitis, as it is usually visible on exam. However, consulting with a dermatologist is always appropriate.10,11
Allergies also cause itch. Patients often have seasonal allergies that they associate with rhinorrhea or coryza, which can be relieved using antihistamines. Although antihistamines will not relieve cholestatic itch, trying an antihistamine could help rule out allergic itch.10,11
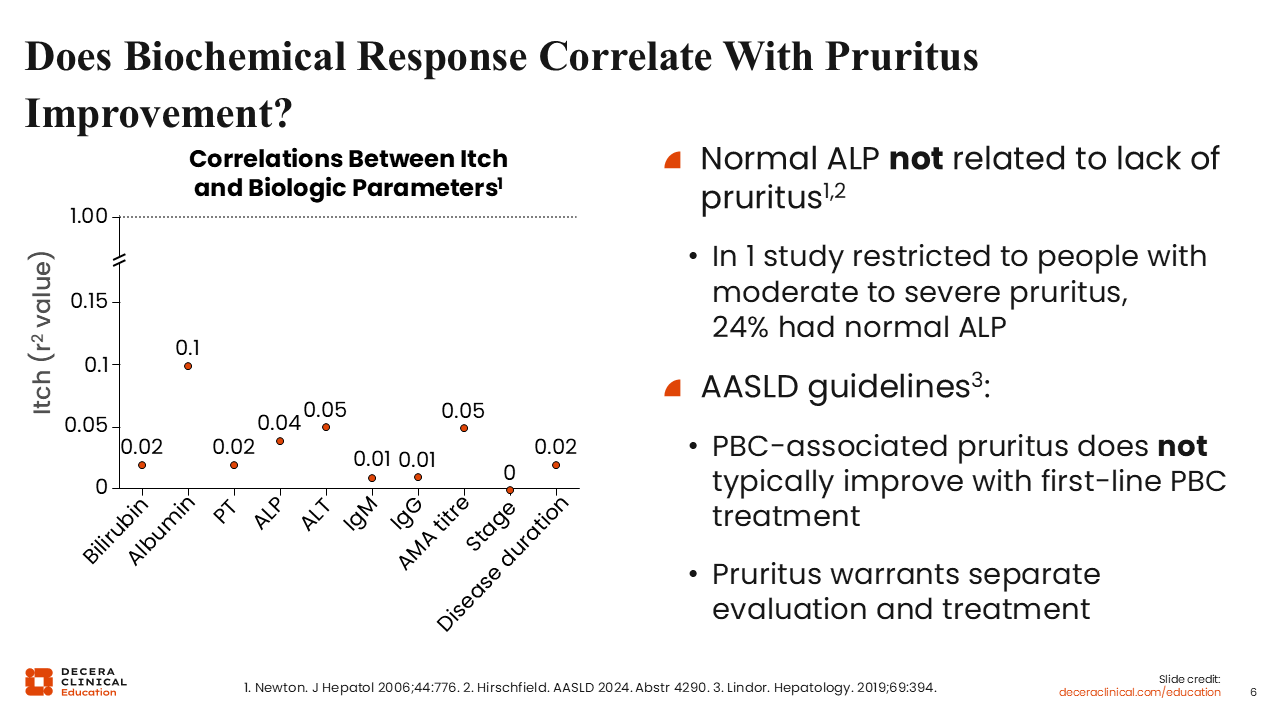
Does Biochemical Response Correlate With Pruritus Improvement?
As I said earlier, biochemical response is not the same thing as symptom management, and disease severity does not correlate with symptoms.12,13
Although we treat PBC with therapies aiming to improve blood test results and to improve disease outcomes, there are people who have normal blood tests and still have significant symptom burden. Not evaluating and treating their symptoms does not do them justice.12,13
This slide shows the correlation between pruritus and disease activity as measured by blood tests, such as bilirubin, albumin, ALP. You can see that pruritus does not correlate with disease activity and that the correlation between itch and biological parameters is actually quite low.12,13
Furthermore, treatment for disease is not the same as treatment for pruritus. First-line treatment of PBC with UDCA only improves the biochemical parameters of PBC disease, but it typically does not improve symptoms such as pruritus.2
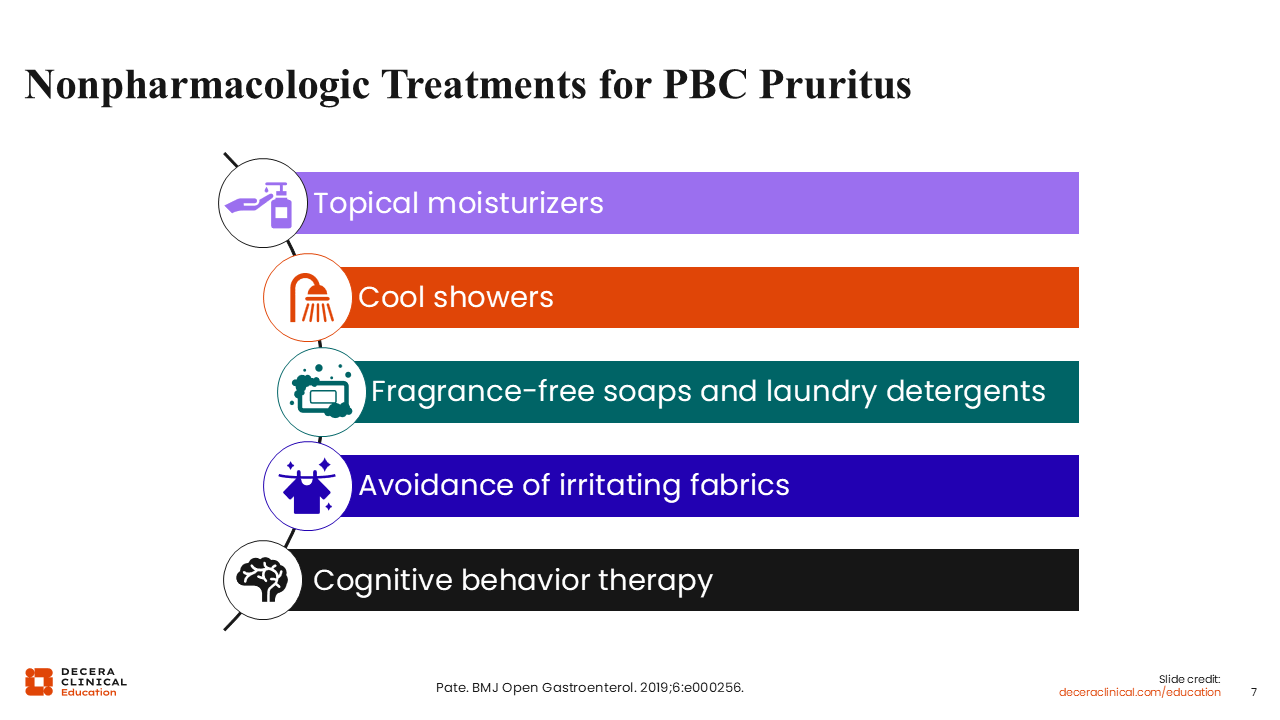
Nonpharmacologic Treatments for PBC Pruritus
Whenever I treat a person, I find it important to think about both nonpharmacologic and pharmacologic options because I find that people generally do not like taking more medicines. If pruritus can be managed with effective, nonpharmacologic treatment, I find that my patients appreciate that option.
Using topical moisturizers and avoiding dryness that can aggravate pruritus can be very helpful. I advise patients to take cool showers, as heat tends to aggravate cholestatic pruritus. Avoiding potential irritants, like scented detergents and rough fabrics such as wools, can also be helpful.14
Cognitive behavioral therapy may also be useful for improving symptoms, particularly when there is a cycle of symptoms interrupting sleep, mood, and day-to-day function. That cycle can affect many aspects of daily life, so using cognitive behavior therapy to break that cycle can be effective for some patients.14
Ultimately, I believe it is best to manage pruritus holistically, understanding that chronic disease is a burden on patients’ cognitive wellness and using a multifactorial approach to treatment. Different things will work for different patients.
Historic Management of Cholestatic Pruritus
Historically, disease control has been managed in parallel to symptoms.2 There was a historic therapeutic ladder for management of cholestatic pruritus that started bile acid resins like cholestyramine.2,15 Then the next step was antibiotics, including rifampin, then other off-label options like sertraline, naltrexone, and gabapentin.
What I think is fundamentally important to understand is that those drugs are all historic. Many, aside from cholestyramine, are used off-label for cholestatic pruritus. They each have challenges related to tolerability, drug interactions, and efficacy.2,15
These agents continue to have a place in PBC pruritus management, and it is also important to understand the benefits and risks of each of them.
Pros and Cons of Historic Pruritus Therapies
First, bile acid resins, like cholestyramine, are helpful, although they are difficult to tolerate in terms of gastrointestinal adverse effects. They may also have some interactions with other drugs, including UDCA, necessitating precise timing intervals between doses.2,15
Rifampin is a good drug for the management of cholestatic pruritus, especially refractory itch, but it is associated with a significant risk of hepatotoxicity and can be associated with hemolytic anemias so regular blood tests are needed.2,15
Itch in patients with PBC is partly neurally mediated. This means that drugs affecting central itch and pain pathways have been associated with improvement in pruritus. That includes naltrexone, sertraline, and even gabapentin. Nonetheless, these drugs also present challenges in terms of tolerability. For example, even at a low dose, naltrexone can result in aggravation of pain. Sertraline is also difficult to use for patients who are receiving other selective serotonin reuptake inhibitors for mood disorders. HCPs must consider the context of the patient’s other comorbidities and medications to choose the right therapy.2,15
If other pharmaceutic options are ineffective, salvage options are used in extreme cases. These include the molecular absorbance recirculating system that uses albumin-enriched dialysate to remove albumin-bound toxins. Plasmapheresis can be used in severe cases. UVB light can be used as well, in collaboration with dermatologists. Liver transplantation may also be considered for people with very severe and refractory pruritus.2,15,16
Aside from these historical therapies, the landscape of management of cholestatic pruritus is changing. Peroxisome proliferator–activated receptor (PPAR) agonists have emerged on the market, and the ileal bile acid transporter (IBAT) inhibitor linerixibat received FDA approval for cholestatic pruritus in adults with PBC in March 2026.2,15,40
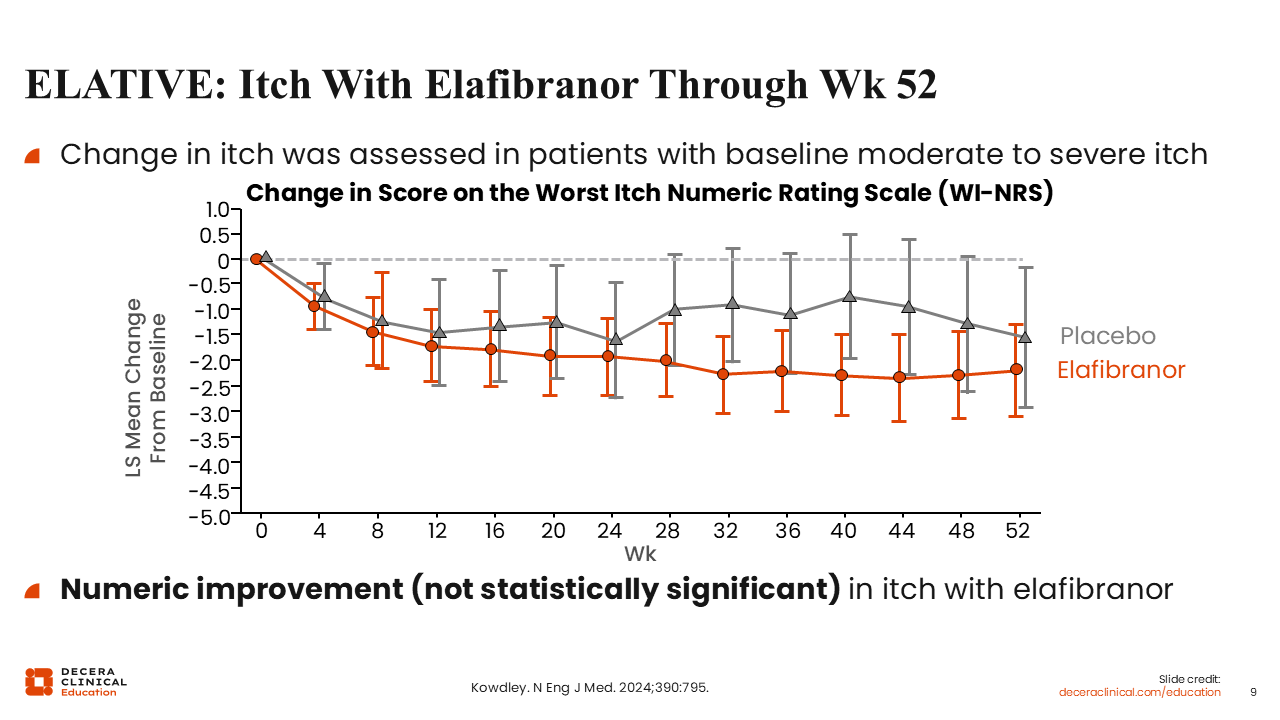
ELATIVE: Itch With Elafibranor Through Week 52
The novel PPAR agonists elafibranor and seladelpar are approved for second-line treatment of PBC disease based on their evidence in improving disease control. And even though they are not approved for symptom management, they both have some evidence for improvement in pruritus.
This graph shows the change in pruritus after treatment with elafibranor in people with PBC, one of the key secondary endpoints of ELATIVE.
I will not discuss disease control here, but the data show that compared with placebo, people with moderate to severe itch treated with elafibranor experienced a numerical (but not statistically significant) improvement in itch.17
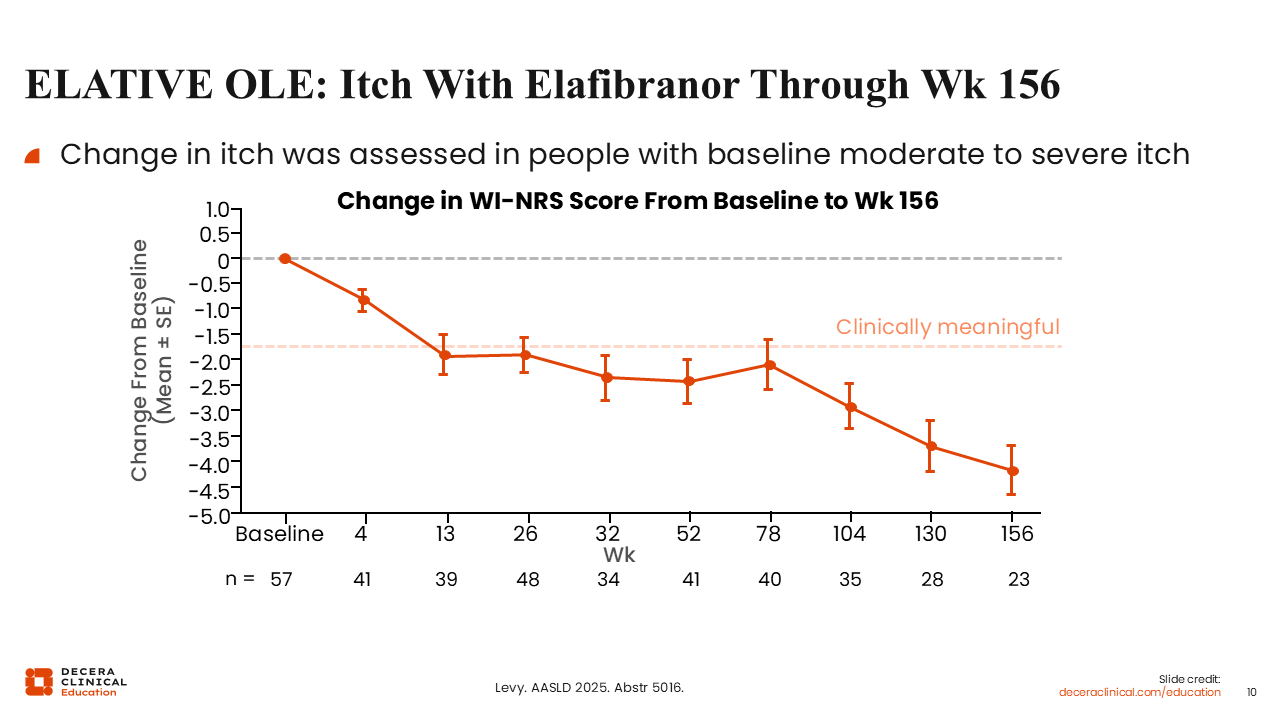
ELATIVE OLE: Itch With Elafibranor Through Week 156
In the open-label extension, comprising patients treated with elafibranor long term, participants demonstrated a clinically meaningful improvement in itch over time, as measured by the Worst Itch-numerical rating scale (NRS).
However, there is no placebo control here. So we do not know how the curves in the placebo arm would look or how itch might have changed over time in the absence of any pharmacologic intervention.18
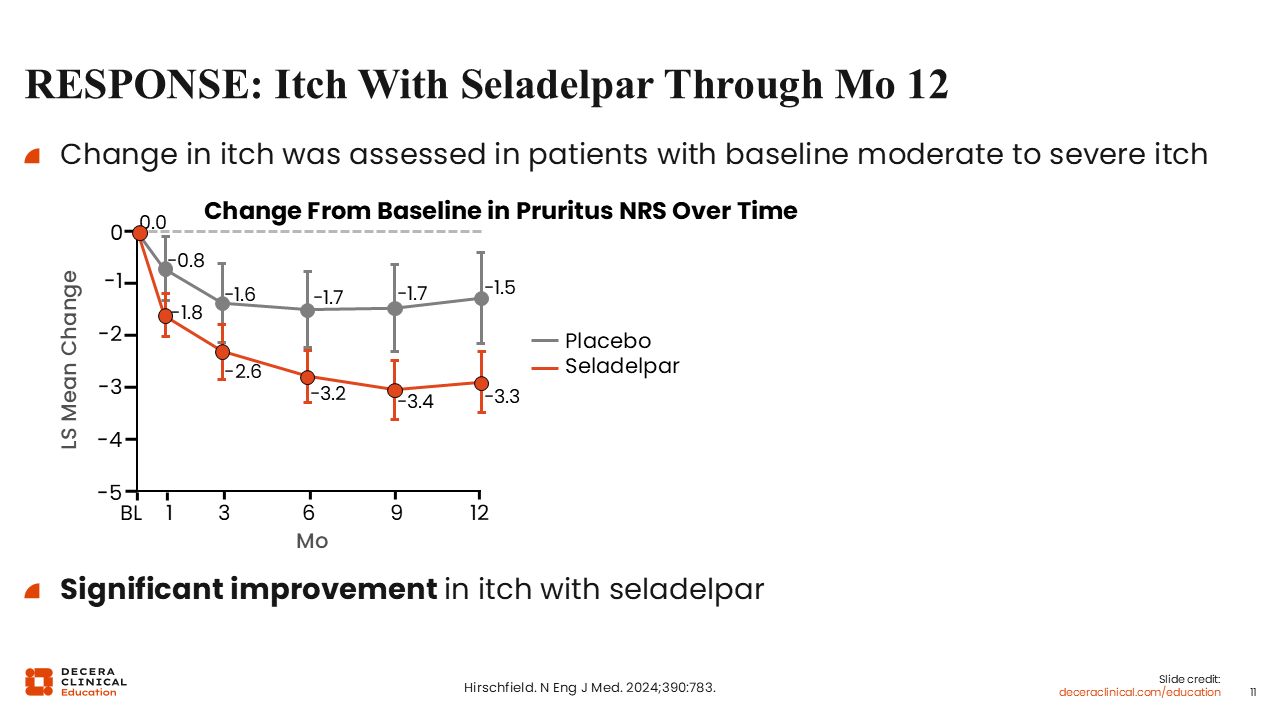
RESPONSE: Itch With Seladelpar Through Month 12
As in the ELATIVE trial of elafibranor, the RESPONSE trial of seladelpar also included a key secondary endpoint of change in itch over time.19
These data showed that, compared with placebo, people with moderate to severe itch experienced a statistically significant improvement in itch, with a mean reduction of approximately 3 points on the NRS.19
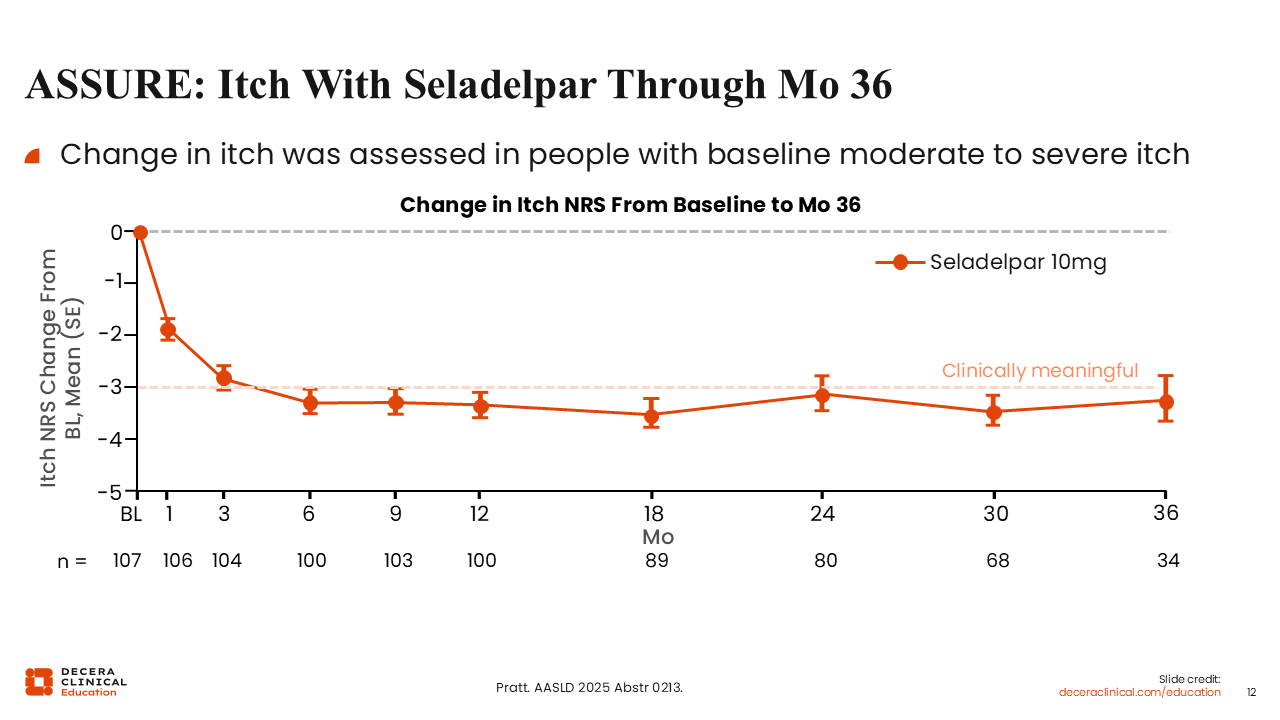
ASSURE: Itch With Seladelpar Through Month 36
ASSURE was the long-term extension of RESPONSE for people with high-risk PBC treated with seladelpar.20
Similar to the ELATIVE OLE, there is no placebo control here. However, these data show that the initial reduction in itch achieved during the RESPONSE study was maintained over time, at a clinically meaningful threshold of more than 3 points lower than baseline.20
Managing Pruritus in Patients With Biochemical Response
There are patients with PBC who are symptomatic despite normal liver tests. In these cases, although they do not need additional therapies to treat disease activity, they still require symptoms to be managed in parallel. To date, there is insufficient data to support the use of PPARs in patients with PBC with normal liver tests. Although these data may evolve over time, we are not quite there as yet. Currently, in these patients with PBC with pruritus despite normal liver tests on therapy, I use the traditional pruritus ladder with agents including cholestyramine, rifampin, sertraline, naltrexone, gabapentin, and so on. In the future, IBAT agents could be a good option for management of pruritus.
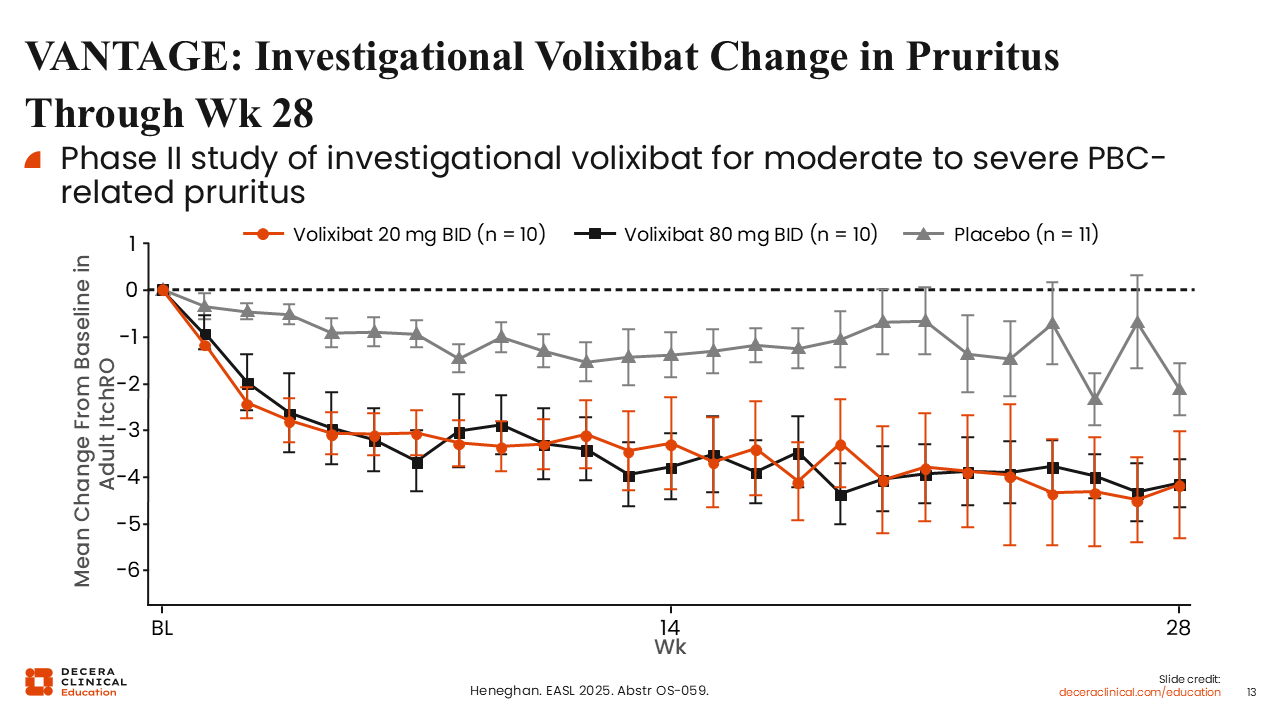
VANTAGE: Investigational Volixibat Change in Pruritus Through Week 28
VANTAGE was a phase II study that assessed volixibat for treatment of moderate to severe pruritus in patients with PBC. Of importance, the studies that evaluated IBATs—VANTAGE and GLISTEN—did not require patients to have elevated ALP. This means that these studies could enroll patients who had normal liver tests or mildly elevated ALP levels but significant symptoms and again emphasizes the discordance between disease activity and symptom burden.21
These results show that patients treated with either 20 mg or 80 mg of volixibat had a significant improvement in itch compared with placebo, as measured by the adult ItchRO score.21
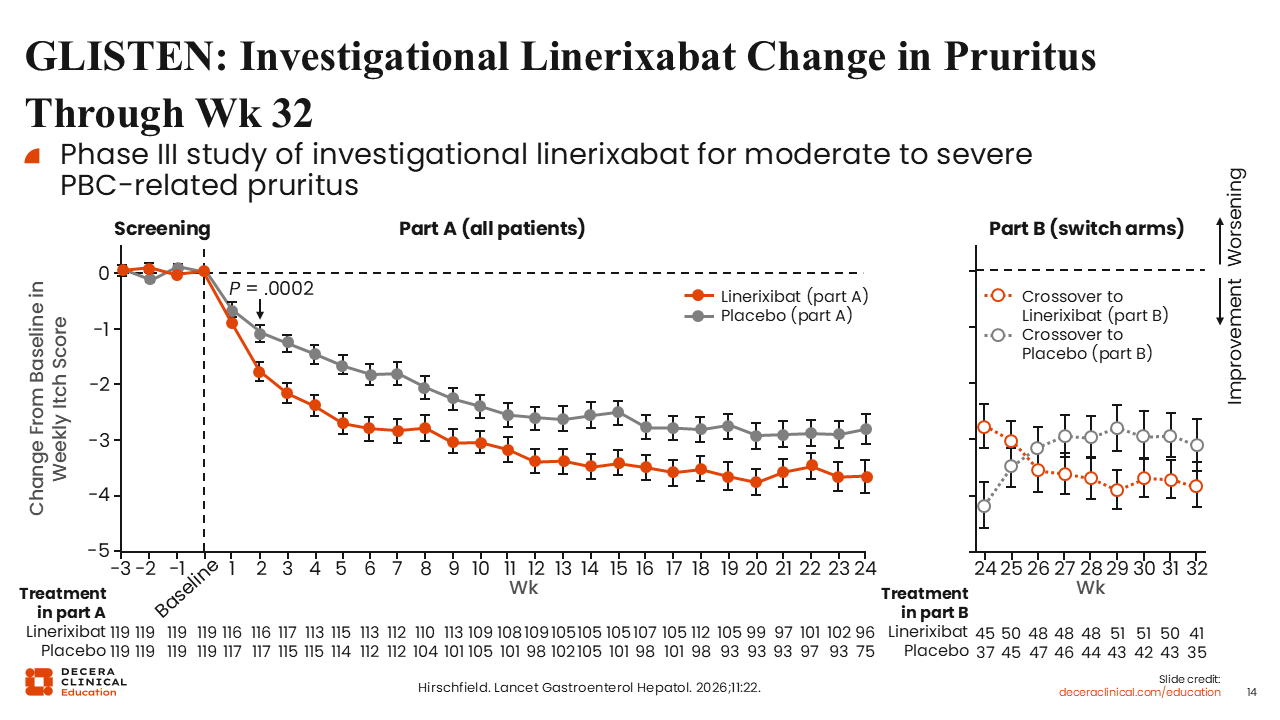
GLISTEN: Linerixibat Change in Pruritus Through Week 32
The GLISTEN study examined linerixibat in patients with PBC. Again, this study only required participants to have diagnosed PBC and moderate to severe pruritus.22
This study showed a statistically significant improvement in pruritus from baseline as measured by the Worst Itch-NRS by 2 weeks after treatment initiation. This is very early in treatment, and remained significant at Week 24.22
The figure on the right side of the slide shows how pruritus changed after patients who were initially receiving placebo crossed over to linerixibat and vice versa. Following the treatment crossover, the symptom burden trend lines crossed. This essentially shows the drug’s effect.22
Linerixibat is Now FDA Approved for Cholestatic Pruritus In PBC
Based on the results of the phase III GLISTEN trial, the FDA approved linerixibat for the treatment of cholestatic pruritus associated with PBC in adults. Its use should be avoided in patients with decompensated cirrhosis or those with prior or active hepatic decompensation events.40
It is dosed at 40 mg and taken twice a day, at least 30 minutes before eating or drinking (other than water). If used in conjunction with bile acid binding resins, those should be administer at least 4 hours before or 4 hours after linerixibat.40
Liver test elevations, diarrhea, fat-soluble vitamin deficiency, bleeding, and fractures should be monitored for and addressed as described in the prescribing information. In clinical trials, the most common adverse reactions were abdominal pain, increased liver enzymes, diarrhea, headache, gastroesophageal reflux disease, dizziness, dyspepsia, abdominal distension, and arthralgia.40
My Approach: Addressing PBC Pruritus
When it comes to pruritus, my approach is to ask all patients about their symptoms and to have a systematic approach that starts with objectively documenting how patients experience itch.
I use the Worst Itch-NRS. I ask patients about their pruritus every time they come to the clinic, which can be every 3 months, every 6 months, or every year, depending on their scheduled visits.
Every time a patient comes to my clinic, I document an NRS as the first step to evaluate the severity of their symptoms. Next, I ask them about the impact of their symptoms on their quality of life and on their day-to-day function.
Then I ask them whether they want therapy. Some do not want additional therapy, whereas some are affected more severely and are open to the option of therapeutic intervention.
For those wanting therapeutic intervention, I first talk about nonpharmacologic approaches, such as using moisturizers, cool baths, and other nonmedicinal options that may help improve itch. I also evaluate for primary causes of pruritus, like allergies, or primary dermatologic conditions.
If nonpharmacologic approaches do not provide relief and I have established that they have significant cholestatic itch that cannot be improved by treating primary causes of pruritus, then I begin to think about what drug to use, independently of what treatment they are receiving for disease control.
Options here include the IBAT inhibitor linerixibat, which I think about particularly for those who have normal liver tests and do not need escalation of therapy for disease; bile acid resins, such as cholestyramine; rifampin; and itch or pain pathway modulators such as sertraline or gabapentin.
I may also think about PPARsS, for those who need escalation of therapy for disease.
Ultimately, it is about individualizing options based on the patient. HCPs must consider each patient’s unique circumstances, comorbidities, medications, and potential interactions to pick the right option for that individual patient.
Pruritus Monitoring and Follow-up
In terms of monitoring and follow-up, objective reassessment over time must be incorporated into routine practice for patients with PBC. The key is being consistent and using a scale that can easily demonstrate trends, such as the NRS.
Personalized therapies rely on patient context to guide selection of medication. If a person’s other medical needs change, then their pruritus treatment can change too, and consistent follow-up can help with staying up to date with a patient’s medical history.
Finally, consistent monitoring will help to optimize the agents of choice. I recommend starting slowly, up titrating as tolerated. I see regularly reevaluating your patients as an important component of their care.
PBC Pruritus Take-home Points
Fortunately, the therapeutic landscape for management of pruritus is evolving, including drugs like PPAR agonists and IBAT inhibitors that may provide clinically and statistically significant benefits. Hopefully, these will soon be used more in patients with PBC to improve symptoms, but older, historic options are still available as well.