CE / CME
Engaging Patients With Obesity in Respectful Conversations About Their Weight and the Latest Advances in Treatment
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: July 10, 2026
Expiration: July 09, 2027

Activity
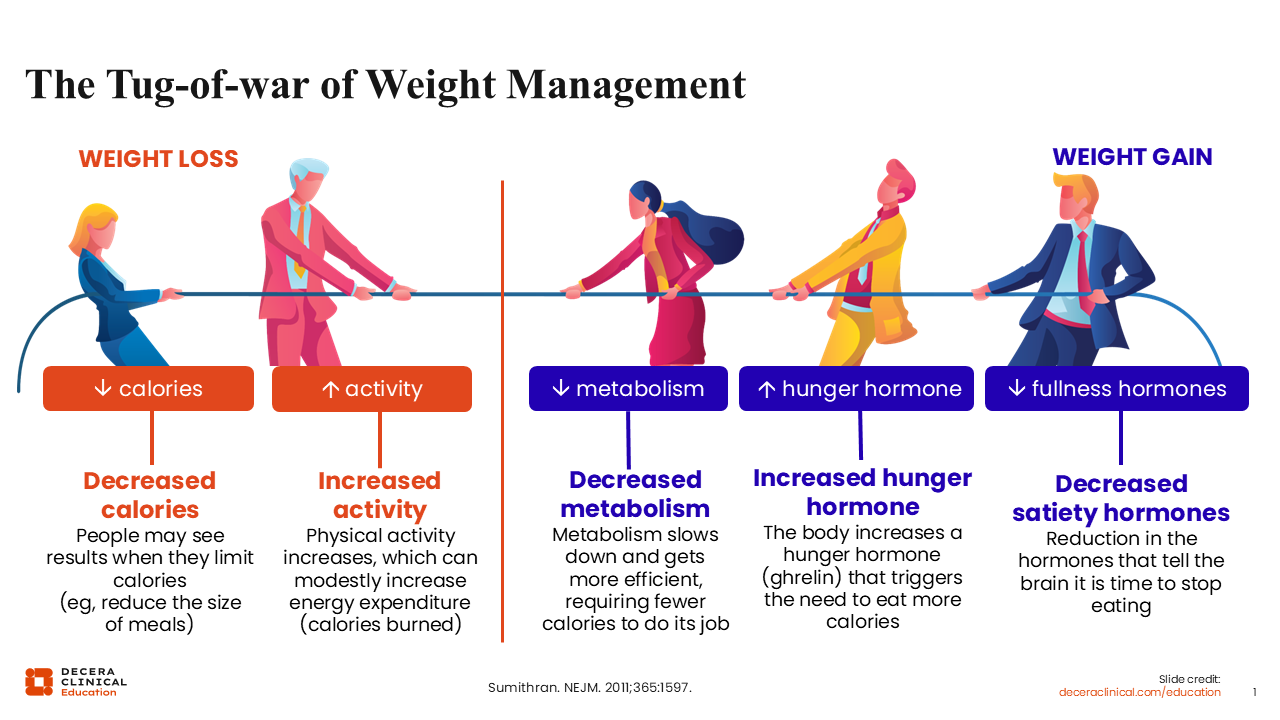
The Tug-of-war of Weight Management
It is important to remember that obesity is a chronic disease state. When patients with obesity try to lose weight, there is a great deal occurring internally within their bodies. To achieve meaningful weight loss, patients often start by reducing their caloric intake and increasing their energy expenditure through physical activity. This is what allows the number on the scale to decrease.
However, the human body is not comfortable with this change. As caloric intake is reduced, the body recognizes this and adapts accordingly. While one’s metabolism becomes more efficient as the body learns to function with fewer calories, the body simultaneously senses this as a potential threat. It responds by increasing levels of ghrelin—the hunger hormone—which triggers an increase in appetite.
Unfortunately, the hormones that promote fullness and satiety, like leptin, also decrease when the body recognizes and adapts to caloric restriction. As a result, we are often fighting against our own physiology in this ongoing tug-of-war of weight management.1
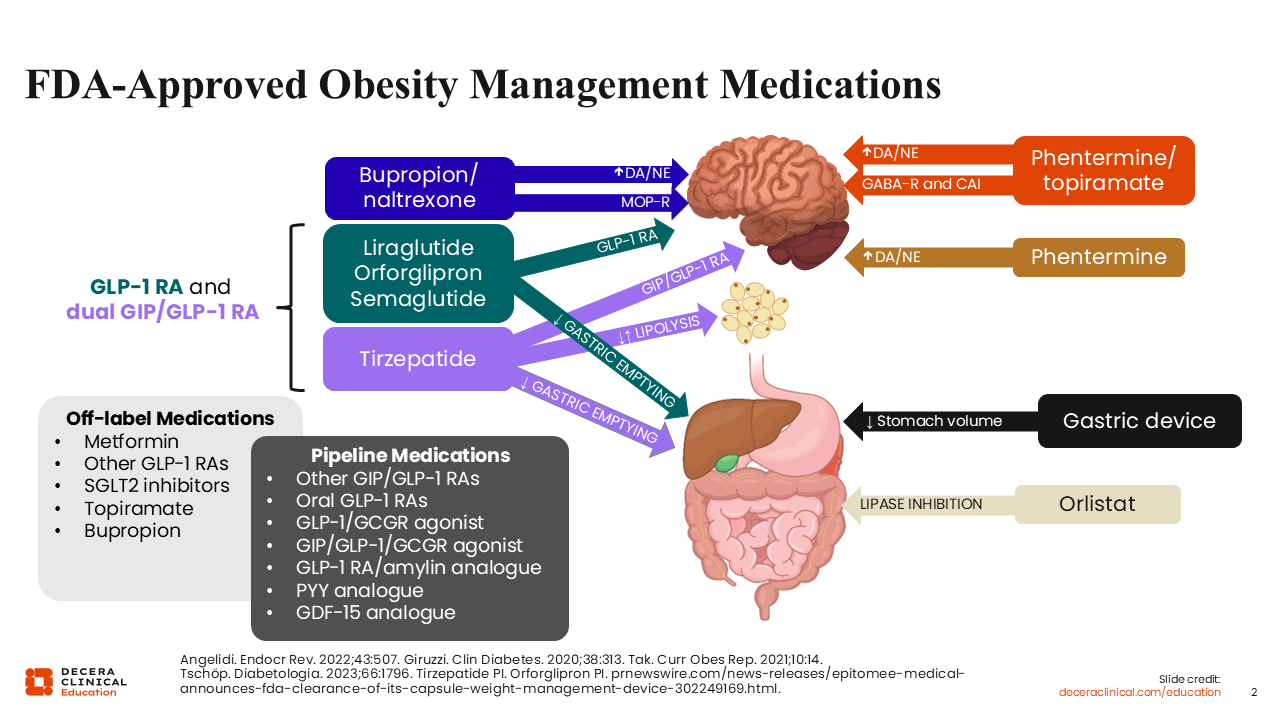
FDA-Approved Obesity Management Medications
The figure on this slide highlights the currently approved obesity management medications (OMMs), demonstrating how far we have come in obesity medicine.
From the late 1990s to 2011, we had limited treatment options available to offer our patients with overweight or obesity. Phentermine was once a primary OMM. It works by targeting dopamine and norepinephrine pathways within the hypothalamus, but it is only approved for short-term use in the United States. We also had orlistat, a lipase inhibitor. Unfortunately, it only provides relatively modest weight loss and often is associated with gastrointestinal adverse events (AEs). Then, between 2012 and 2014, combination OMMs became available, including phentermine plus topiramate at lower individual doses as well as naltrexone plus bupropion. These OMMs in particular represented an important advancement in obesity medicine because they provided meaningful weight loss and could be used long-term.2,3
Today, further advances in medicine have expanded the OMM landscape. Several incretin-based OMMs are now available, including GLP-1 receptor agonists and dual GIP/GLP-1 receptor agonists. Looking at GLP-1 receptor agonists specifically, the first was liraglutide. It is a once-daily injectable approved to reduce excess body weight and maintain long-term weight loss in patients 12 years of age or older with obesity who weigh more than 60 kg or adults with overweight and at least 1 weight-related comorbidity.4 Semaglutide subsequently became available as a once-weekly injectable approved for the same indication as liraglutide but without the weight limitation for pediatric patients. More recently, the FDA approved the oral formulation of semaglutide, which can only be used in adults.5 Orforglipron is the latest oral GLP-1 receptor agonist to be approved to reduce excess body weight and maintain long-term weight loss in adults.6
The only dual GIP/GLP-1 receptor agonist that is FDA approved is tirzepatide. It is similarly indicated to reduce excess body weight and maintain long-term weight loss in adults with obesity or overweight and at least 1 weight-related comorbidity.7
These incretin-based therapies work by slowing gastric emptying and signaling the brain to promote satiety and fullness. Although the percentage of total weight loss varies across clinical trials, these therapies consistently demonstrate clinically meaningful reductions in total body weight. Furthermore, through additional studies and indications, they have also been shown to improve several weight-related comorbidities and quality of life.8,9
For too many years, healthcare professionals (HCPs) had to rely on various off-label therapies that generally produced modest weight loss. Today, it is especially exciting to see the robust OMM pipeline as it expands with the many therapies that are currently under investigation.
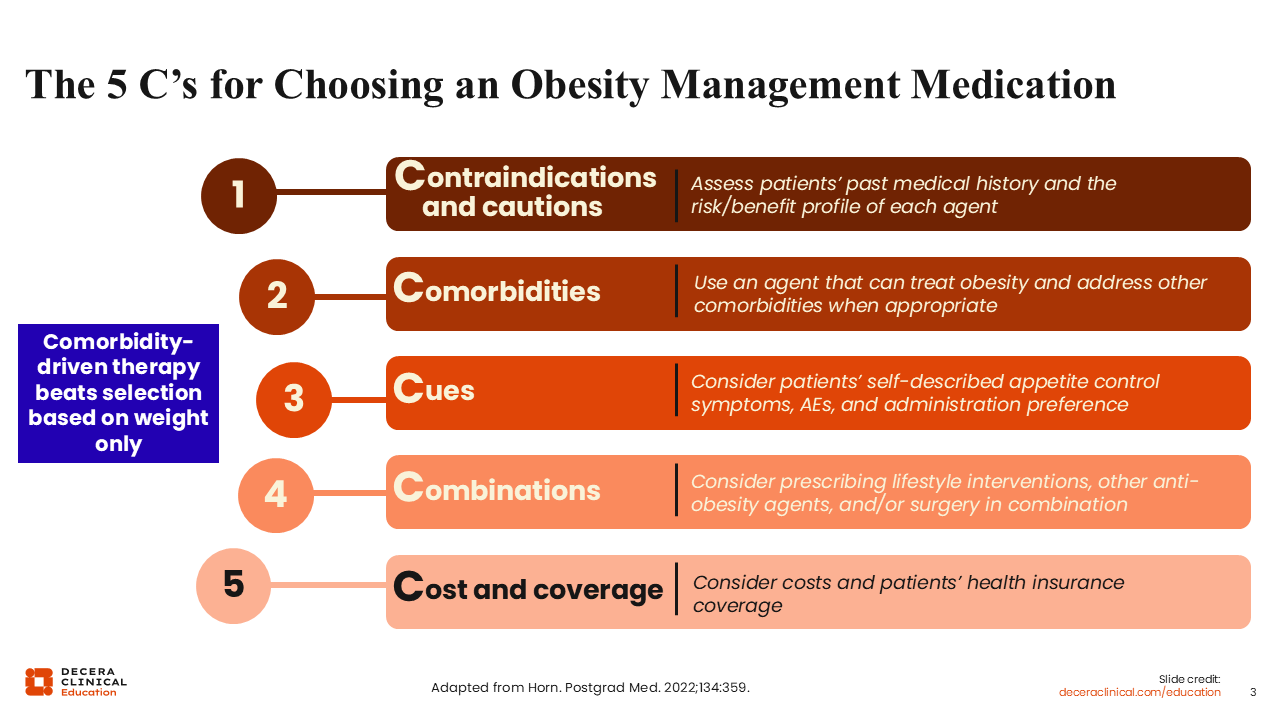
The 5 C's for Choosing an Obesity Management Medication
As with other chronic diseases, the goal of care is to provide individualized treatment based on patients' needs, preferences, and comorbidities. This is where the 5 C's for choosing an OMM come into play. In obesity medicine, HCPs and patients need to move beyond focusing on the number on the scale. Instead, OMM selection should be driven by patients’ comorbidities and weight management goals.
The first C requires HCPs to consider relevant contraindications and cautions. That means assessing patients' past medical history and the risk–benefit profile of each therapy to determine the most appropriate option.
Next, HCPs should evaluate any present comorbidities. Do patients have established cardiovascular disease, metabolic dysfunction–associated steatohepatitis, or obstructive sleep apnea? Understanding their past medical history and current comorbidities allows HCPs to determine the optimal OMM for patients that not only supports weight loss but also has additional benefits to their overall health.
The third C is to consider cues, such as patients' self-described appetite control symptoms, prior AEs, and preferences regarding administration. Some patients may prefer daily oral therapy, whereas others might be more comfortable with weekly injectables. Reviewing the benefits, risks, and potential AEs of each OMM can help guide shared decision-making.
After this, HCPs should consider combination therapy. This is critical because many patients with obesity have struggled with achieving and maintaining meaningful weight loss throughout their lives, and they may need a combination of approaches. That could include lifestyle interventions, OMMs, and, in some cases, metabolic or bariatric surgery. When used appropriately, combination therapy can help patients achieve their individualized health goals.
Finally, HCPs must consider cost and coverage. Health insurance coverage varies considerably across commercial plans, Medicare, and Medicaid. Although progress continues to be made, affordability and access remain important barriers to address. HCPs must understand both the patient's health insurance coverage and their ability to afford treatment over time. This is particularly relevant because obesity is a chronic disease, requiring patients to adhere to long-term therapy.10
Roadmap for Patient-Centered Conversations in Obesity Care
Now I will discuss the roadmap for patient-centered conversations in obesity care. The goal during these conversations is to base discussions on the current evidence, just as one would do when determining a treatment plan. It is important that HCPs use respectful, patient-centered language when discussing the latest advances in obesity care and align treatment recommendations with patients’ health goals, preferences, and long-term follow-up needs.
Every patient's journey is different, and HCPs must be mindful and respectful of this reality. Furthermore, many patients with obesity have experienced stigma and shame over the years. This is why it is essential to approach patients respectfully by asking permission. Once permission is given, the discussion can then begin about their weight and framing obesity as a chronic disease.
HCPs should also reframe outcomes beyond weight loss alone by focusing on overall health gains. For example, even a 5% to 10% reduction in total body weight can provide meaningful benefits beyond appearance or the number on the scale. Such health gains include reductions in cardiometabolic risk, improvements in joint health, and enhanced overall well-being.
As previously mentioned, it is also important to respectfully address patients' concerns about cost, safety, stigma, and treatment duration. There is a lot of information available on OMMs, some accurate and some inaccurate. As HCPs, it is our responsibility to provide patients with factual, evidence-based information so patients can make informed decisions about their care.11,12
Stepwise Approach to Building Trust in Obesity Care
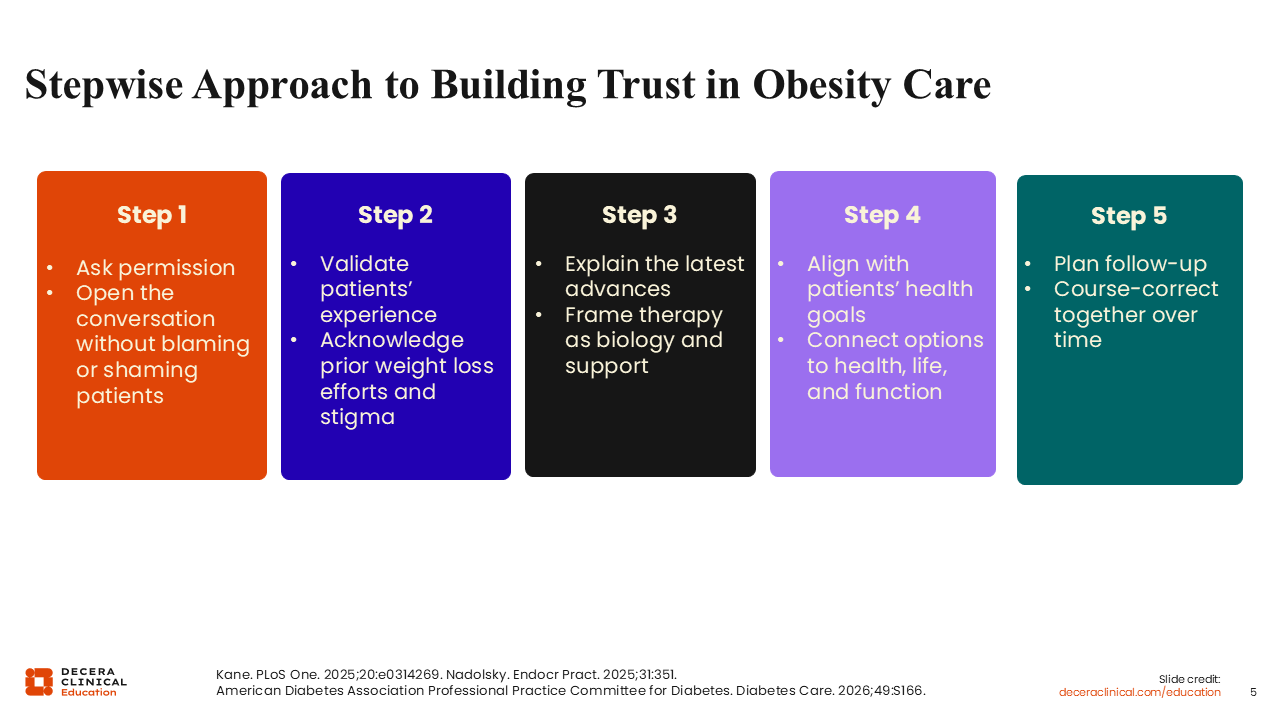
With all this in mind, HCPs can take a stepwise approach to building trust with patients in obesity care. The first step is to ask patients’ permission before initiating discussions about their weight. Doing so opens the conversation without placing blame or shame.
After receiving their permission, HCPs should validate patients’ experiences by acknowledging their prior weight loss efforts and experiences with stigma. They can then explain the latest advances in obesity care, while framing treatment as support for the underlying biology of this chronic disease.
The fourth step is to align treatment with patients’ health goals by connecting available therapies and strategies to their preferred health outcomes, daily function, and quality of life. Finally, HCPs must establish a follow-up plan. This step requires being prepared to adjust treatment plans over time. If a particular strategy is not working, HCPs should reassess the situation and consider alternative approaches.11-13
Patient Case: Obesity Care After a Dismissive Experience
Our patient case is a 46-year-old man with obesity (BMI: 33 kg/m²). He also has hypertension, poor sleep, and a family history of diabetes. He expresses frustration with being told to simply eat less and move more because he has already attempted these approaches. He says, “I keep hearing there are weight loss pills now. I do not want injections, but I also do not want to be blamed if another treatment does not work.” Finally, this patient is seeking a respectful partnership with his doctor.
Take a moment to think about this individual and his experience. Do you see patients like this frequently in your practice? It is clear that this patient has a history of negative encounters and stigma related to obesity care, and I am certain many HCPs encounter patients with similar experiences in their practice. I have also found that those who have struggled with obesity throughout their lives often express similar concerns repeatedly in the clinical setting.
The question then becomes how we should open the conversation on weight in an empathetic manner that rebuilds trust and invites partnership with the patient.

Patient Case: Obesity Care After a Dismissive Experience
The clinical task here is not to simply discuss the new OMMs that are available. Rather, it is to build a partnership with the patient. HCPs must build trust and understanding with the patient by listening carefully to what he has experienced and the challenges he has faced.
In general, it is critical to reassure patients, support them, and guide them through the process. Obesity management is not a short-term fix, but a long-term journey that includes lifestyle modifications and ongoing support. Encouraging patients to focus on achievable short-term goals can help build momentum toward long-term success.

Course Correction: Poll 3
Remember, it is always important to ask patients for their permission before discussing their weight. Opening the conversation in this manner invites patients to engage when they feel ready and comfortable.
Patient-Centered Language Reduces Stigma, Invites Partnership
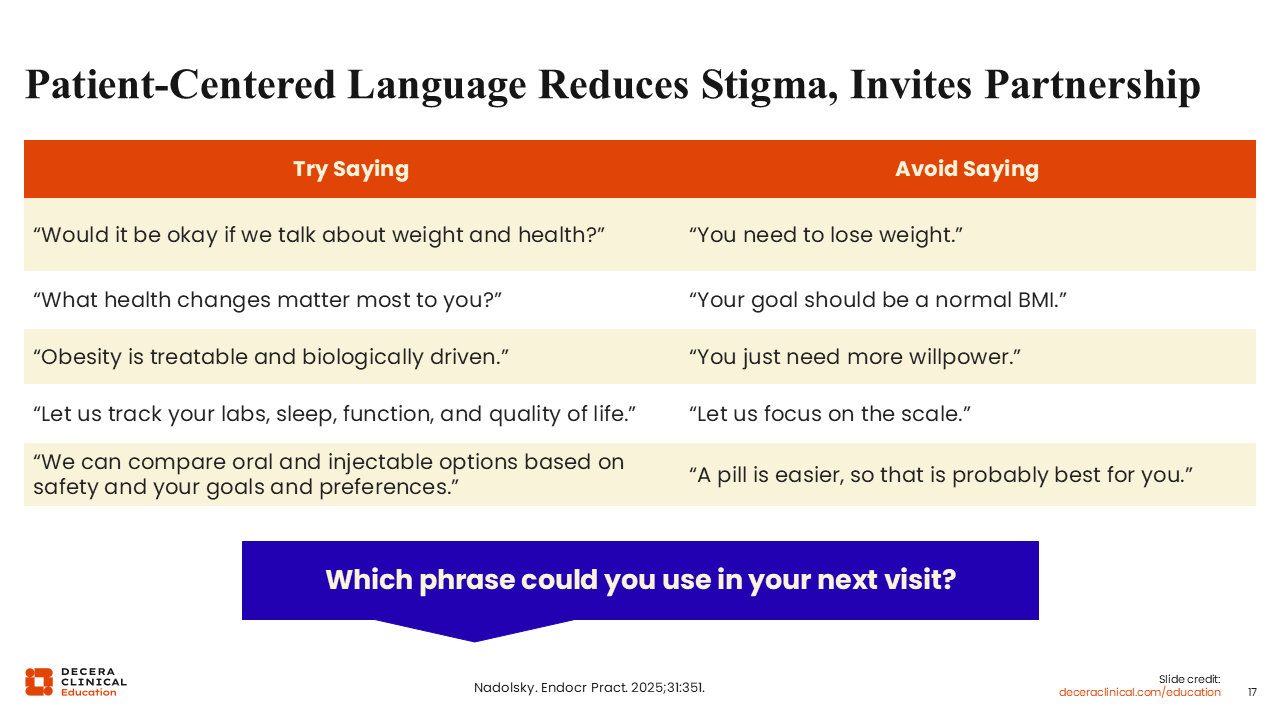
Remember, your language and word choice are powerful. HCPs must use patient-centered language in obesity care to reduce stigma and foster a collaborative partnership with patients. Looking at the table on this slide, you can consider which of these approaches you might use during your next visit.
For example, you might say, “Would it be okay if we talk about weight and health?” instead of telling patients that they simply need to lose weight. Similarly, you might ask patients, “What health changes matter most to you?” instead of telling them that their goal should be a normal BMI.
Another approach is to explain to patients that obesity is a treatable, biologically driven disease rather than suggesting they simply need more willpower to lose weight. In addition, you can help patients focus on tracking their laboratory values, sleep quality, functionality, and quality of life as markers of health gains rather than exclusively the number on the scale.
Finally, HCPs can compare oral vs injectable OMMs based on relevant safety considerations as well as patients’ goals and preferences rather than making assumptions about which option may be best for them.
These examples highlight a key point: our role as HCPs is to advocate for patients by providing education and evidence-based information, so they can make informed decisions about their care.
Course Correction: Poll 4
It is crucial that patients understand the mechanisms of the newer OMMs, whether they are administered orally or via injection. Patients should understand that incretin-based therapies can help manage their appetite, satiety, and the metabolic drivers of obesity. When discussing these therapies with patients, HCPs also should connect the treatment plan to patients' individual health goals and long-term objectives.
Moving the Conversation From Scale Only to Whole Health Goals
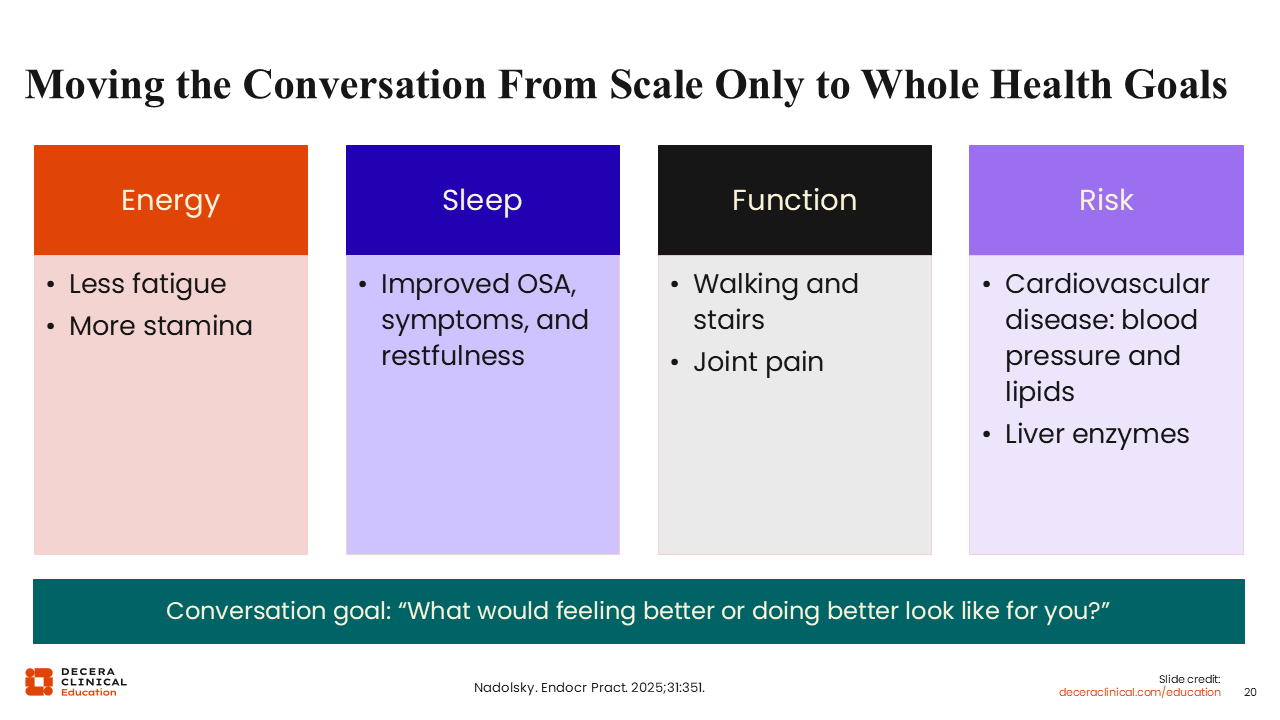
Moving the conversation beyond the scale to whole health goals is vital. This means reminding patients that success is not measured by their weight loss alone. Improvements in energy and stamina, as well as reductions in fatigue, are meaningful outcomes that can positively affect their daily life.
Sleep may also improve, particularly for those with obstructive sleep apnea, which results in better restfulness and overall well-being. Then there are improvements in physical function, such as walking, climbing stairs, and joint pain, that can significantly enhance patients’ quality of life.
Finally, HCPs can discuss reductions in cardiovascular risk as an added benefit. This includes improvements in blood pressure, lipid levels, and liver enzymes for those with metabolic dysfunction–associated steatotic liver disease or metabolic dysfunction–associated steatohepatitis.12
A useful question to ask patients is, “What would feeling better or doing better look like for you?” In my practice, I do more than review the number on the scale at each visit. I also discuss patients’ percentage of total body weight loss and changes in their BMI, A1C, lipids, and other metabolic measures. Evaluating these factors allows us to assess how treatment is improving their overall health, not simply their body weight.
Handling Concerns: Follow Curiosity Before Correction
When addressing patients’ concerns, it is important to lead with curiosity before correction. For example, when discussing treatment costs, one approach is to check patients’ health insurance coverage before settling on a plan. Understanding affordability and access is an important part of shared decision-making.
When discussing administration options, HCPs should compare therapies based on patients’ health goals, daily routines, safety considerations, and access needs to determine the best fit. In addition, patients should understand that obesity often requires ongoing treatment, much like hypertension, diabetes, or other chronic conditions. Then there is the common concern of safety. A helpful approach here is to review the benefits, risks, and potential AEs that warrant attention, so patients understand what to expect during short- and long-term treatment.
Finally, stigma remains a significant issue for many. Therefore, HCPs must reinforce the principle that obesity is not a character flaw, but a treatable disease.12
Course Correction: Poll 5
HCPs must remind patients that obesity is a chronic condition often requiring treatment adjustments over time. If the first treatment plan does not produce the desired results, that should not be viewed as a failure.
Instead, we should continue to evaluate their response, tolerability, access, and goals together and make changes when needed. I often use the analogy of the tortoise and the hare. Slow and steady progress is the most sustainable path in obesity care. What matters most is continued forward movement toward improved health outcomes.
Follow-up Is Part of Your Prescription
Follow-up is part of the prescription. Patients with obesity often benefit from early and frequent follow-up when initiating an OMM. These visits provide opportunities to discuss treatment response, review AEs, and address any challenges patients may be experiencing.
Regular follow-up visits also reassure patients by clarifying whether their experiences are as expected and providing guidance when concerns arise. Ongoing support demonstrates commitment to patients' success and can be highly empowering. One approach is to ask patients, “How does it sound if we schedule regular follow-up visits to see what is working for you, what is difficult, and whether the plan needs to be adjusted?”
As discussed previously, it is important to track more than weight loss alone. HCPs should monitor patients’ laboratory values, sleep quality, mood, overall quality of life, tolerability, adherence, and access to therapy. Doing so also ensures the route of administration fits appropriately into patients' lifestyles.
A multidisciplinary, team-based approach can be particularly valuable here. Dietitians and nutrition specialists, behavioral health HCPs, physical therapists and exercise specialists, and other members of the care team can all contribute to patients’ success.
All that said, HCPs must maintain a course-correction mindset. If something is not working, reassess the situation and determine what adjustments may be necessary to ensure patients remain on track.
Patient Case: Building a Sustainable Obesity Care Plan
Looking back at our patient case, the overarching goal is to build a sustainable obesity care plan. We can accomplish this by asking the right questions and carefully considering the most appropriate approach for each patient.
It is important to remember that obesity is a chronic, relapsing, and treatable disease. Although oral treatment options expand opportunities for shared decision-making, the best treatment plan considers patients' health goals, safety needs, access to care, daily routine, and long-term management needs.
When discussing treatment options with patients, it is helpful to explore what matters most to them, whether that involves administration preferences, health goals, safety considerations, or access concerns. Patients should also understand that oral therapy is only 1 factor in treatment selection, not the sole determinant of the best therapeutic approach. Finally, HCPs should consider what support systems will help patients successfully initiate and maintain treatment over time.

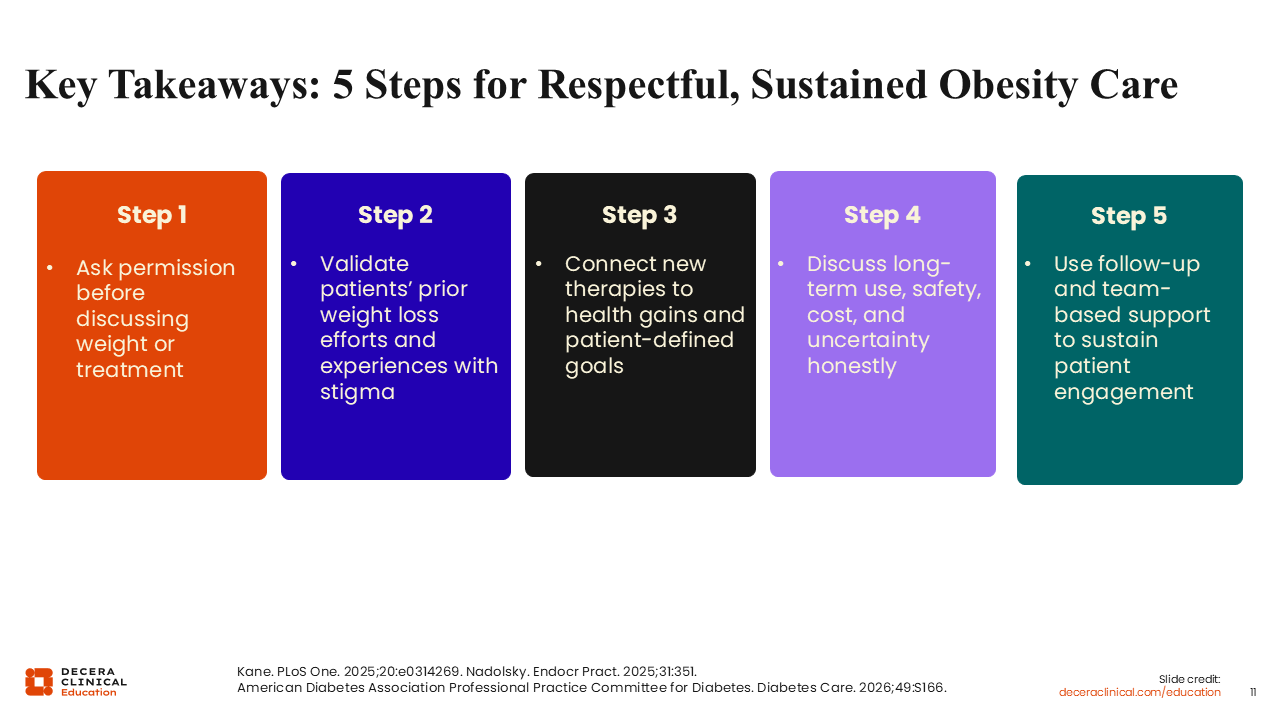
Key Takeaways: 5 Steps for Respectful, Sustained Obesity Care
There are 5 key steps for providing respectful and sustained obesity care. As mentioned, the first is to ask permission before discussing weight or obesity treatment with patients.
Next, HCPs should validate patients’ prior weight loss efforts and acknowledge their experiences with stigma. They can then connect newer therapies to meaningful health gains and patient-defined goals.
AHCPs should then discuss the long-term treatment needs, including safety, cost, and uncertainty, honestly and transparently.
The final step is to use ongoing follow-up and team-based support to sustain patient engagement and help patients achieve their long-term health goals.11-13