CE / CME
Evolving Treatment Landscape for HER2-Positive/HER2-Low Early Breast Cancer
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
Pharmacists: 0.50 contact hour (0.05 CEUs)
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: May 01, 2026
Expiration: October 31, 2026

Activity
Tailoring the Treatment Plan to Individual Needs: Shared Decision-making
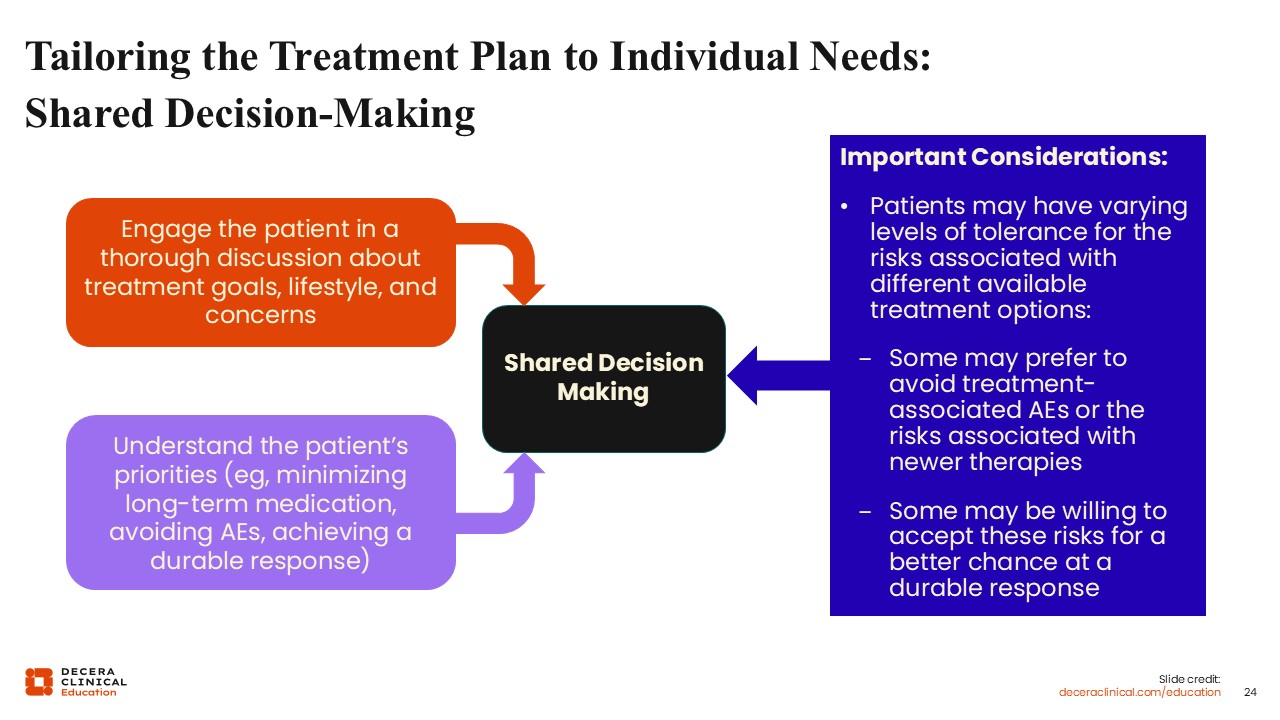
Shared decision‑making is a foundational component of care for patients with HER2‑positive EBC. Engaging patients in meaningful discussions about treatment goals, values, preferences, and tolerance for potential AEs is essential to informed decision‑making and patient satisfaction. These conversations also provide an opportunity to address patient concerns, clarify expectations, and provide support documentation for alignment between recommended therapy and individual priorities.28,29
The treatment course for HER2‑positive EBC is often prolonged, frequently extending to 1 year or longer and involving multiple phases of therapy.7 Establishing expectations early in the treatment journey and providing a clear overview of the anticipated treatment timeline, including neoadjuvant therapy, surgery, adjuvant therapy, and follow‑up, can help improve patient understanding and promote adherence to NCCN‑recommended care.
Clear communication strategies, including the use of written treatment plans and educational materials, can further support patient comprehension and reduce decisional conflict.29 Involving caregivers when appropriate may also enhance adherence and provide additional psychosocial support. A multidisciplinary care model incorporating oncologists, nurses, pharmacists, and other HCPs plays a critical role in supporting patients throughout treatment, facilitating AE management, and optimizing clinical and patient‑reported outcomes.
Navigating the Healthcare Ecosystem: Addressing Potential Healthcare Disparities
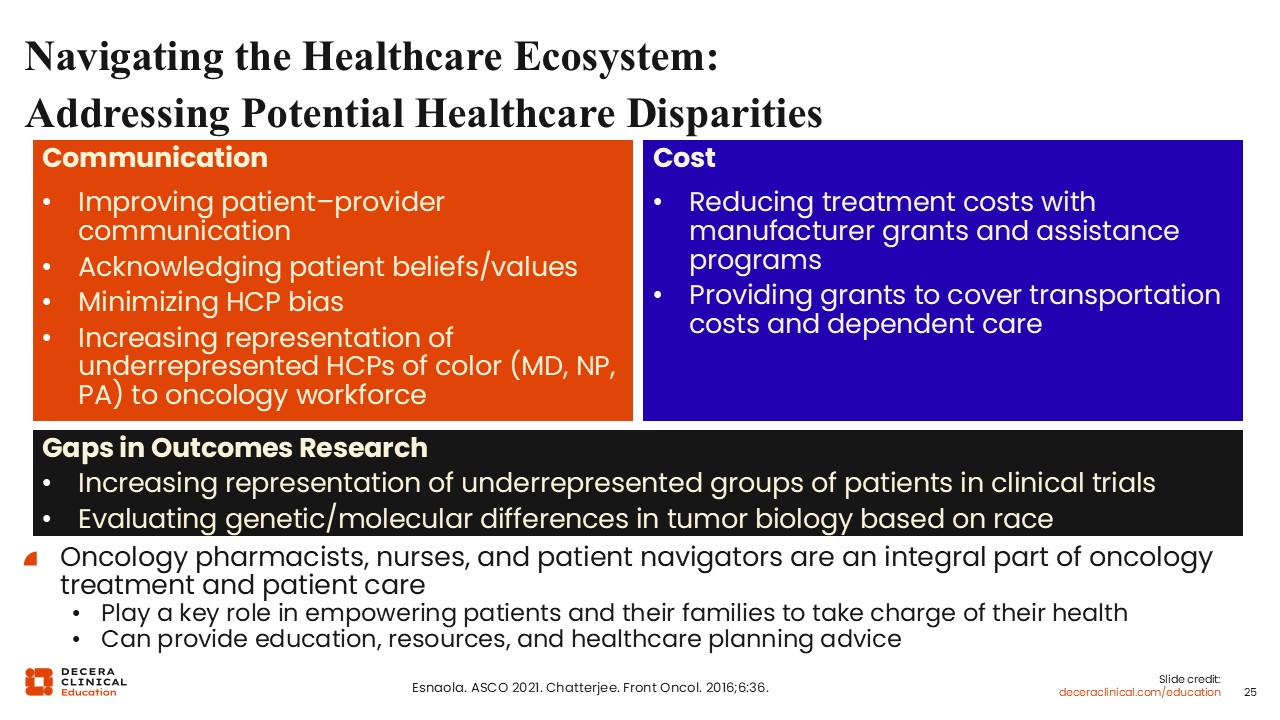
To address potential healthcare disparities, there has been a significant focus on improving patient–HCP communication by acknowledging individual patient beliefs and values. Efforts include minimizing HCP bias and actively increasing the representation of HCPs of color—such as physicians, nurse practitioners, and physician associates—within the oncology workforce.
Financial barriers could potentially be addressed by reducing treatment expenses through manufacturer grants and assistance programs whenever available. In addition, providing specific grants to cover transportation costs and dependent care may help patients maintain access to their necessary treatments.
Current research goals continue to include increasing the representation of underrepresented patient groups in clinical trials. Furthermore, there is a focus on evaluating genetic and molecular differences in tumor biology specifically based on race to better understand outcomes across diverse populations.
All HCPs play a role in improving health equity. Oncology pharmacists, nurses, and patient navigators are integral to patient care, playing a vital role in empowering patients and their families to take charge of their health. They serve as essential resources by providing education, necessary support materials, and personalized healthcare planning advice.
Clinical Trial Participation: Patient’s Considerations
Black patients’ willingness to participate in clinical trials appears to be influenced less by race or psychological stressors such as anxiety and depression than by whether patients are engaged and adequately informed about clinical trials they may qualify for.
Many patients are simply not asked about clinical trial participation, highlighting the importance of initiatives such as the Just ASK™ Increasing Diversity in Cancer Clinical Research program. The content points to a need for better medical information and support, including clear direction and recommendations from HCPs, information about risks, benefits, and treatment alternatives, and a clearer description of the clinical trial process. Patients may also be encouraged by testimonials from people like themselves who have participated in clinical trials. In addition, addressing logistical barriers, such as transportation and access to dependent care, may help improve willingness to participate and overcome some of the challenges these populations face.
Data from a qualitative study of 91 interviews across 5 US cancer centers found that intrinsic bias contributed to disparities in clinical trial enrollment.30 Interactions with underrepresented patients of color were often perceived as challenging, and these patients were not viewed as ideal research participants. Combined with limited clinic time and negative perceptions of minorities, these attitudes led to withholding clinical trial information from underrepresented patients of color. Race was also perceived as irrelevant in clinical trial recruitment by some of the research staff. Related findings showed that oncologists' implicit bias affected the care patients received: non-Black oncologists with higher implicit bias scores spent less time with Black patients and communicated less with them, and this was associated with lower patient confidence in treatment recommendations.
Connecting Patients With Available Resources
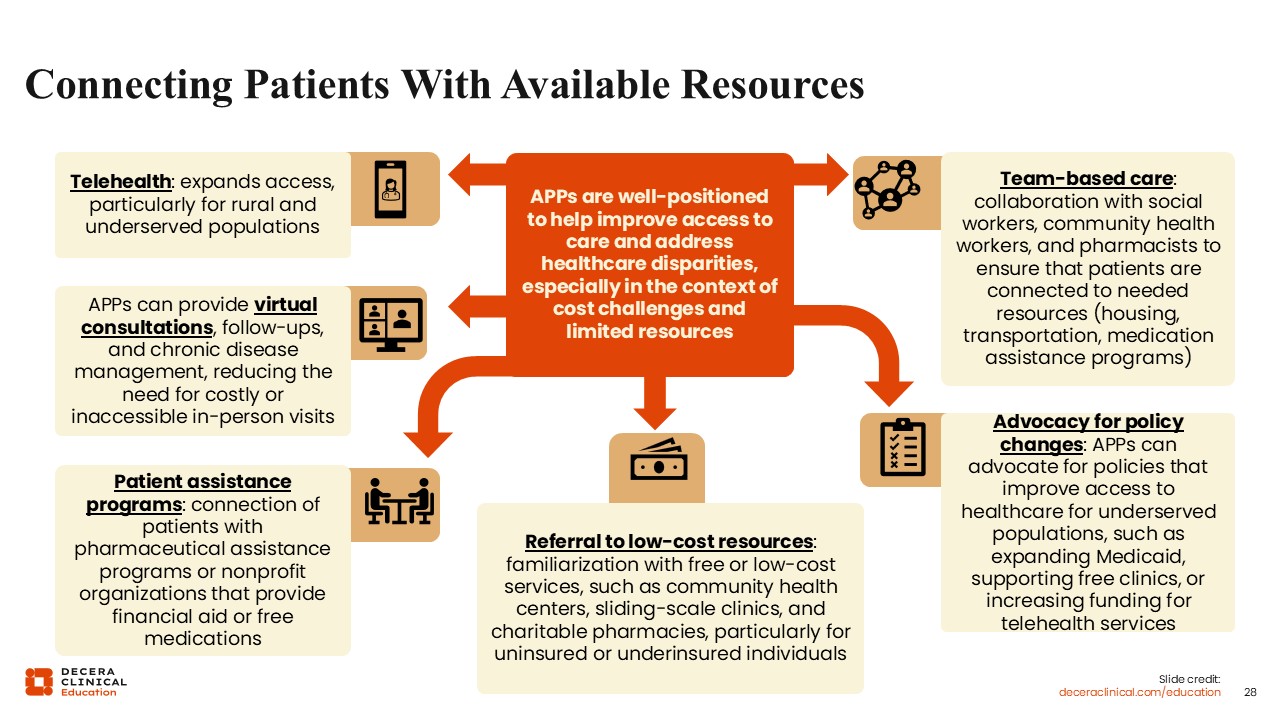
Oncology HCPs are essential for improving healthcare access and addressing disparities, particularly when facing cost barriers or limited resources. By leveraging diverse strategies, they bridge the gap between patients and the support they need.
Telehealth and Virtual Consultations
Telehealth serves as a vital tool for expanding access to rural and underserved populations. HCPs utilize virtual platforms to provide consultations, follow-up care, and chronic disease management. This reduces the burden of costly or inaccessible in-person visits, ensuring continuity of care regardless of a patient's physical location.
Patient Assistance Programs
To combat financial barriers, HCPs should identify at-risk individuals and help connect them with assistance programs and various nonprofit organizations. These resources offer critical financial aid or free medications, ensuring that treatment remains attainable for those in need.
Referral to Low-Cost Resources
HCPs maintain familiarity with a network of free or low-cost services. This includes directing uninsured or underinsured individuals toward community health centers, sliding-scale clinics, and charitable pharmacies to minimize out-of-pocket expenses.
Team-Based Care
Collaboration is central to patient support. HCPs may work alongside social workers, community health workers, and pharmacists. This multidisciplinary approach ensures patients are linked to essential nonmedical resources, such as housing, transportation, and medication assistance.
Advocacy for Policy Changes
Beyond clinical care, HCPs advocate for systemic improvements. This includes supporting policies that expand Medicaid, increasing funding for telehealth, and bolstering free clinics to create a more equitable healthcare landscape for all underserved populations.
Key Takeaways
As the treatment landscape for HER2-positive EBC continues to evolve, ongoing research and emerging data will further refine how HER2-directed therapies are optimally sequenced and individualized across patient populations.
Today, HER2-positive EBC is moving from a one-size-fits-all model toward a response-guided strategy in which the neoadjuvant setting response defines what comes next. pCR identifies patients with a more favorable prognosis, whereas residual disease marks a high-risk population in whom postneoadjuvant escalation can materially change outcomes. That treatment paradigm first established T-DM1 with the KATHERINE trial and is now being advanced further by DESTINY-Breast05, where T-DXd achieved a 3-year iDFS of 92.4% vs 83.7% with T-DM1 in patients with residual disease. Yet the scientific progress is not reaching every patient equally. Real-world studies continue to show underuse of guideline-recommended HER2-directed therapy, socioeconomic as well as racial and ethnic differences in neoadjuvant treatment patterns and pCR, including persistently worse pCR outcomes for Black patients in HER2-positive cohorts. At the same time, adults 70 years of age or older remain underrepresented in pivotal trials, leaving a persistent evidence gap around the balance between chemotherapy benefit and toxicity. The next advance in HER2-positive EBC, therefore, is not only better drugs, but improvements in clinical practices that lead to more equitable, response-adapted, and age-informed care.