
CE / CME
Enhancing Outcomes in Obesity Care With Incretin-Based Therapy and Individualized Treatment Plans
Physician Assistants/Physician Associates: 0.50 AAPA Category 1 CME credit
ABIM MOC: maximum of 0.50 Medical Knowledge MOC point
Physicians: maximum of 0.50 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.50 Nursing contact hour
Released: July 15, 2026
Expiration: July 14, 2027

Activity
FDA-Approved Obesity Management Medications
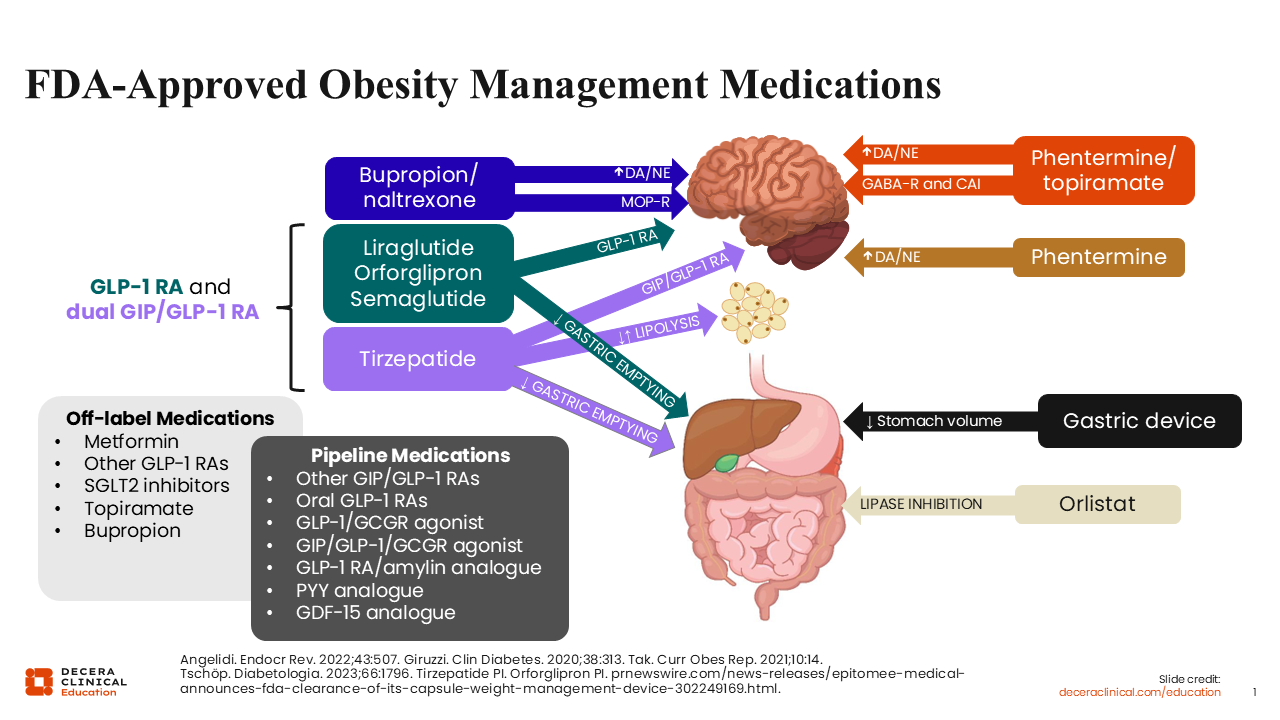
I have been practicing obesity medicine since 2008. Throughout my practice, one concept that has helped me better understand obesity as a chronic disease is the role of physiologic drivers regarding appetite. Hunger and satiety/fullness are regulated by multiple systems and pathways throughout the body, including the gastrointestinal tract and brain. As highlighted in the figure on the slide, the currently available and FDA-approved obesity medications (OMs) target these systems and pathways to help counter the natural physiologic responses that occur when a negative energy balance is created. The body responds by increasing hunger signals and decreasing satiety signals when patients decrease their caloric intake and increase their physical activity. This is what creates the tug-of-war of weight management.1
Early OM options include combination bupropion plus naltrexone, which targets dopamine and norepinephrine pathways, making this therapy particularly helpful for patients who struggle with cravings, food-related reward behaviors, emotional eating, or strong food dependencies. Combination phentermine plus topiramate also affects dopamine pathways in the brain, including gamma-aminobutyric acid (GABA) activity, which can help reduce appetite and the desire to eat. In my practice, I find this combination particularly helpful for patients with nighttime eating behaviors. Now phentermine can be used alone to decrease appetite through central satiety mechanisms, but it is only approved for short-term use in the United States as a monotherapy. Finally, orlistat inhibits fat absorption through lipase inhibition, but it is often used less frequently in obesity management due to its unfavorable safety profile (eg, gastrointestinal adverse events [AEs] and limited tolerability).2,3
More recently, incretin-based therapies like GLP-1 and dual GLP-1/GIP receptor agonists have significantly changed the obesity treatment landscape. They work through several mechanisms, such as slowing gastric emptying and promoting a greater, more prolonged sense of satiety after eating. These mechanisms are further enhanced with the GIP dual target of tirzepatide. Furthermore, central GLP-1 activity reduces appetite and hunger, and GLP-1 receptor agonists appear to decrease what many patients describe as “food noise” or persistent, intrusive thoughts about food.4-6
The FDA-approved incretin-based therapies (ie, semaglutide, tirzepatide, liraglutide, and orforglipron) are all indicated to reduce excess body weight and maintain long-term weight loss in adults with obesity or overweight and at least 1 weight-related comorbidity. But there are a couple of caveats to this. Injectable semaglutide and liraglutide may be used in patients with obesity who are at least 12 years of age, but they must weigh more than 60 kg to comply with liraglutide’s approval. Injectable semaglutide may be used in pediatric obesity care, but oral semaglutide is only approved for use in adults.7-10
Other available approaches to obesity management include gastric devices that expand in the stomach when swallowed to reduce food intake by occupying space.11 Or off-label use of other therapies that support weight loss, as well, including metformin, GLP-1 receptor agonists with indications in diabetes only (ie, dulaglutide), sodium-glucose cotransporter-2 inhibitors, and topiramate or bupropion monotherapy.2
It is particularly exciting to see the obesity treatment pipeline continue to expand today. Investigational approaches include additional dual GIP/GLP-1, oral GLP-1, dual GLP-1/GCGR, and triple GIP/GLP-1/GCGR receptor agonists, such as retatrutide. Some newer targets comprise GLP-1/amylin-based therapies, PYY analogues, and GDF-15 analogues. Looking at this comprehensive list, a broad range of therapies are currently under development for obesity management, showcasing the potential for additional treatment options in the future.12
Clinical Roadmap for Individualized Therapy Selection
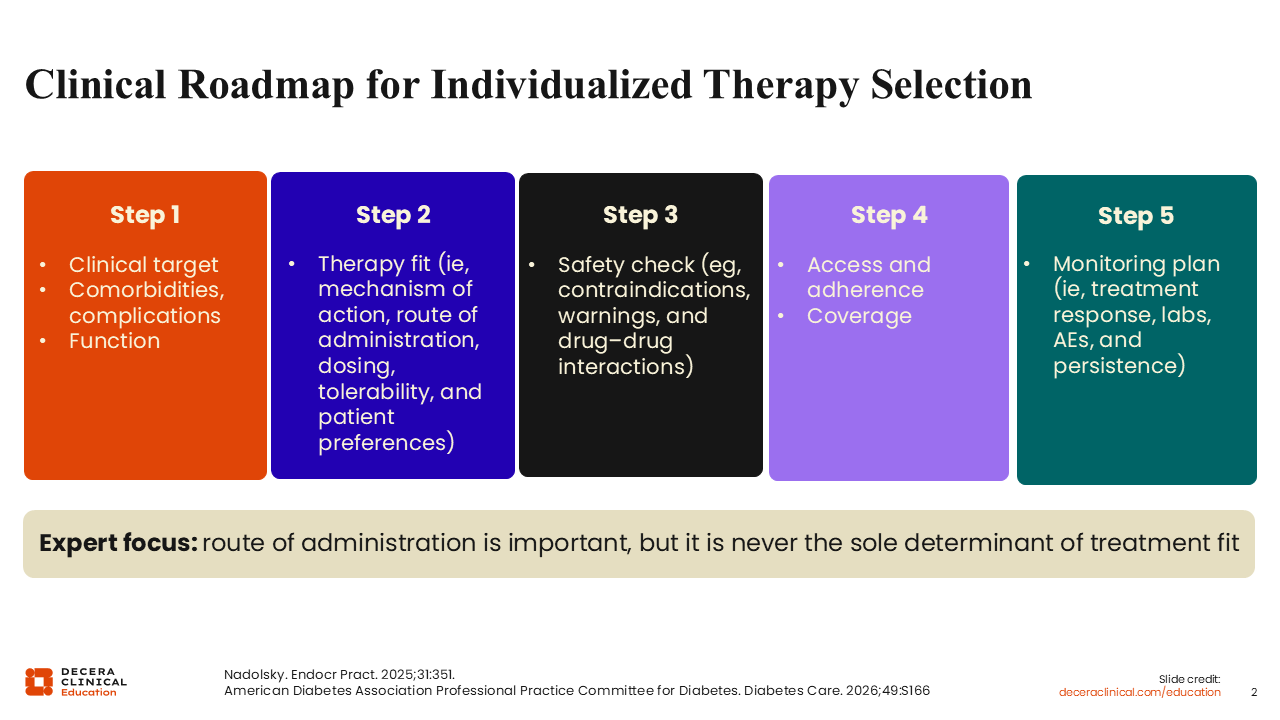
As shown, we currently have several safe and effective treatment options available for patients with obesity. But selecting the most appropriate therapy requires healthcare professionals (HCPs) to follow a structured approach that considers both clinical and patient-specific factors.
The process begins by identifying the clinical target. This includes understanding patients’ comorbidities, complications, functional limitations, and areas of risk that treatment may help improve. Note that assessing patients’ ability to function is an important component when determining an appropriate treatment strategy.
Next, HCPs must identify the right therapeutic fit. This includes evaluating the desired mechanism of action, route of administration, dosing schedule, and tolerability. At this step, patient preferences should be incorporated into the decision-making process. Although route of administration is an important consideration, it should never be the sole determinant of treatment selection.
The third step includes a review of any safety considerations, such as contraindications, warnings, precautions, and potential drug–drug interactions, associated with each OM. HCPs should also evaluate any relevant aspects of patients’ past medical history that will impact treatment selection.
HCPs should then focus on assessing access and adherence. This includes patients’ current health insurance coverage, expected out-of-pocket costs, and their willingness to commit and feasibility of maintaining long-term treatment. These factors should all be considered before initiating an OM.
Finally, HCPs must develop a monitoring plan, which includes establishing follow-up intervals, assessing treatment response, determining appropriate laboratory monitoring, and evaluating AEs. Monitoring should also support long-term treatment persistence and ongoing patient engagement.13,14
Patient Case: Choosing the Right Therapy for the Right Patient
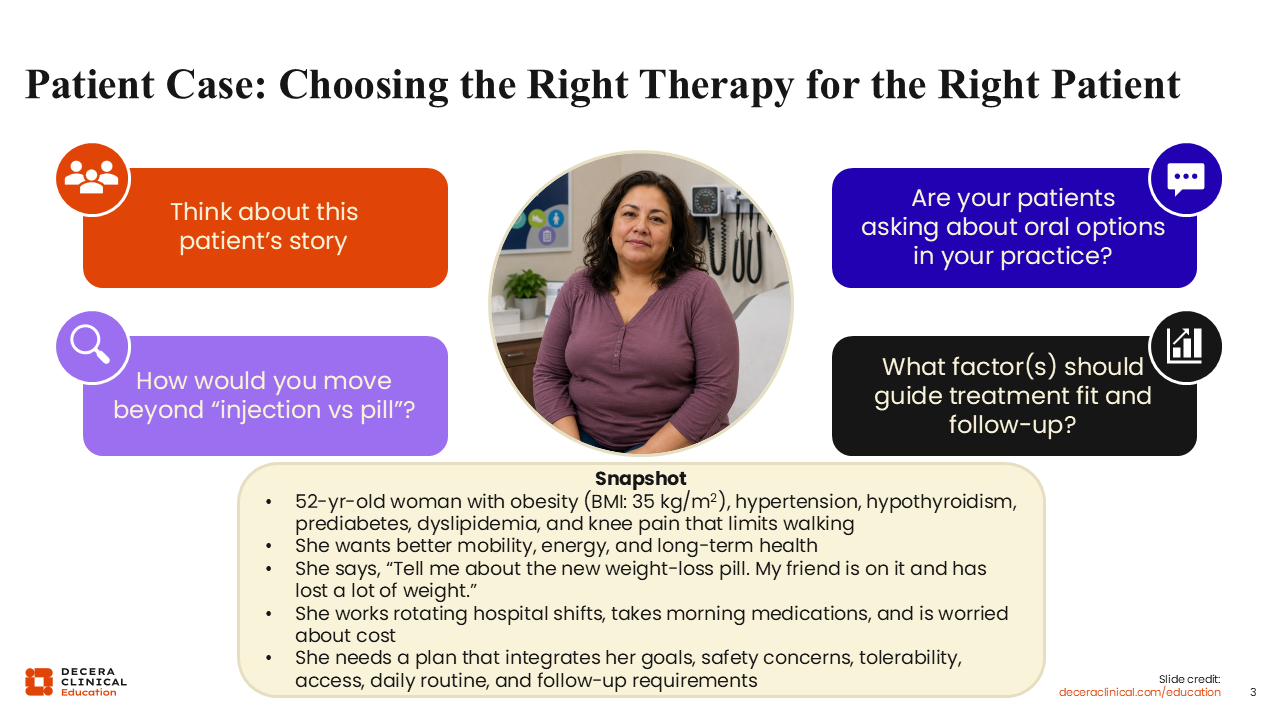
When evaluating patients, HCPS must understand the full clinical picture rather than focus solely on the choice between an injectable vs oral therapy. Patients frequently ask about oral treatment options for obesity, but effective OM selection requires consideration of a broader range of factors.
Let us put these ideas into practice. Our patient case is a 52-year-old woman with obesity (BMI: 35 kg/m2). She has comorbid hypertension, hypothyroidism, prediabetes, dyslipidemia, and knee pain. These conditions affect both her health risks and ability to engage in physical activity. She is seeking improved mobility, increased energy, and better long-term health outcomes. Note that her quality-of-life goals are important considerations when discussing treatment options and helping patients with obesity look beyond the number on the scale alone.
The patient says, “Tell me about the new weight-loss pill. My friend is on it and has lost a lot of weight.” This reflects a common situation in clinical practice, where patients may have a limited understanding of the factors that should influence treatment decisions. This is why HCPs play an important role in helping patients understand the broader clinical picture.
The patient also works rotating hospital shifts, which may make adherence to a regular dosing schedule challenging. She takes other medications in the morning and is worried about cost. She wants a treatment plan that integrates her goals and concerns about safety, tolerability, access, daily routine, and ability to participate in follow-up care. This is reasonable considering all these factors should be incorporated into standard treatment planning in obesity management.
Now take a moment to think about this patient’s story. How would you move the conversation beyond “injection vs pill”?
Patient Case: Choosing the Right Therapy for the Right Patient
The key teaching point here is that therapy selection should extend beyond simply choosing an injectable or oral OM. Consideration should be given to cardiometabolic risk, mobility limitations, mechanism of action, comorbidities, safety, dosing practicality, access and coverage, and the patient’s readiness to engage in a long-term treatment plan.
The preferred approach to obesity treatment selection incorporates patients’ complete clinical profile. Comorbid prediabetes, blood pressure, sleep quality, liver health, mobility, and overall function should all be considered when selecting a therapy for this patient. In addition, the selected OM, route of administration, and dosing schedule should align with what the patient can realistically adhere to and sustain over long-term care.

Course Correction: Poll 3
When I select an OM, I start with the patient’s disease targets, such as prediabetes, blood pressure, sleep quality, liver health, mobility, and overall function. Then I align the route of administration and dosing schedule with what the patient can realistically sustain in their daily life.
Evidence Snapshot: Current and Emerging Incretin-Based OMs
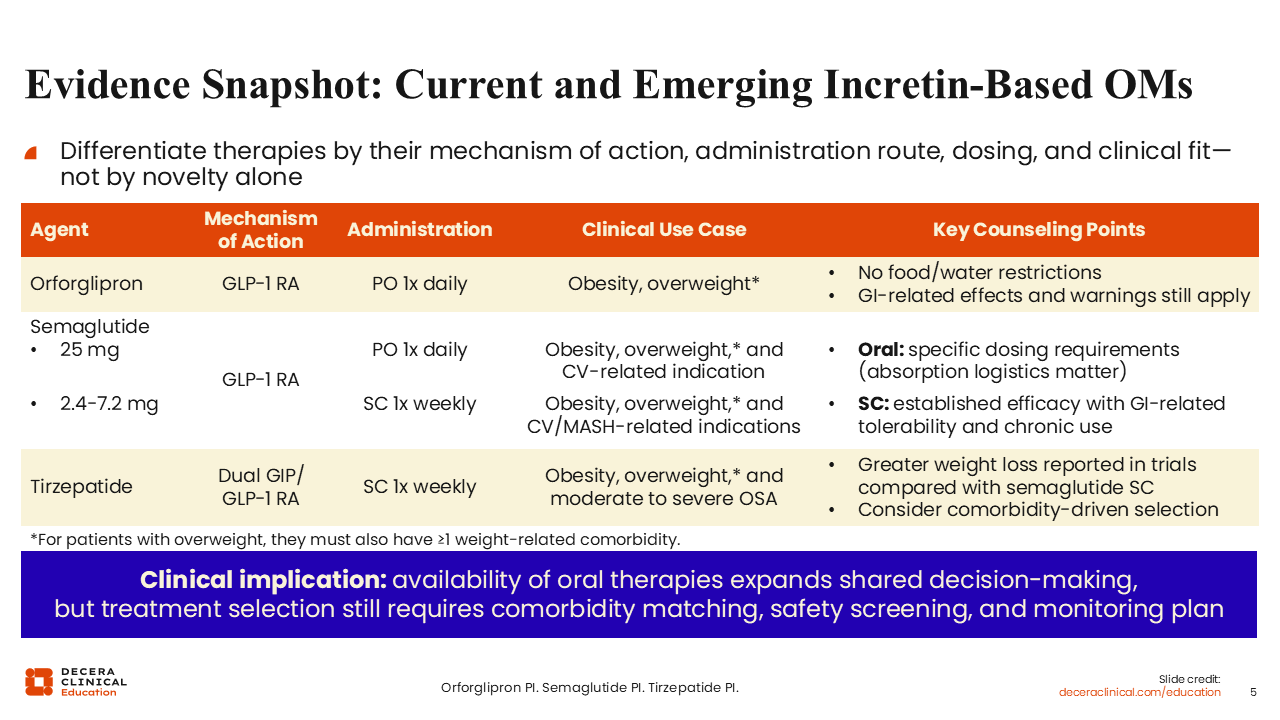
As previously mentioned, several incretin-based OMs are now available for obesity management. These therapies are unique because they differ in their mechanisms of action, routes of administration, dosing schedules, and clinical considerations.
For example, orforglipron is an oral, nonpeptide GLP-1 receptor agonist. It is indicated to reduce excess body weight and maintain long-term weight loss in adults with obesity or overweight and at least 1 weight-related comorbidity. Because it is a small-molecule therapy, it does not require the food and water restrictions associated with peptide- and oral-based OMs. However, gastrointestinal AEs and class-related warnings remain important considerations when thinking about this therapy as a treatment option.9
Today, semaglutide is available in both oral and injectable formulations. Oral semaglutide carries the same overweight and obesity indication as orforglipron, but it is also approved to reduce the risk of major cardiovascular events (MACE) in adults with obesity or overweight and established cardiovascular disease. Because it is a peptide, oral semaglutide requires a specific absorption mechanism involving salcaprozate sodium. As a result, it must be taken in the morning on an empty stomach with no more than 4 oz of water, followed by at least 30 minutes before eating, drinking, or taking other medications. The semaglutide tablet should not be crushed, split, or chewed.
In contrast, injectable semaglutide is administered once weekly. It carries the same overweight and obesity indication as oral semaglutide, except that the injectable formulation may also be used in pediatric patients with obesity who are at least 12 years of age. In addition, it is approved to reduce the risk of MACE in adults with obesity or overweight and established cardiovascular disease as well as to treat adults with metabolic dysfunction–associated steatohepatitis (MASH) and moderate to advanced liver fibrosis. As with other GLP-1 receptor agonists, gastrointestinal AEs require ongoing monitoring with injectable semaglutide use.8
Tirzepatide is different because it is a dual GIP/GLP-1 receptor agonist that is administered once weekly. It has the same obesity and overweight indication as orforglipron and is additionally approved to treat adults with moderate to severe obstructive sleep apnea. Of note, clinical trials have demonstrated greater average weight loss with tirzepatide vs injectable semaglutide. Furthermore, its weekly administration may be advantageous for some patients, including those who have variable daily schedules or difficulty with adhering to daily dosing.10
Although both oral and injectable OM options are available, treatment selection should continue to focus on patients’ comorbidities, safety considerations, monitoring requirements, and individual preferences to determine which is the best match.
Using the 5 C’s: OM Selection Framework
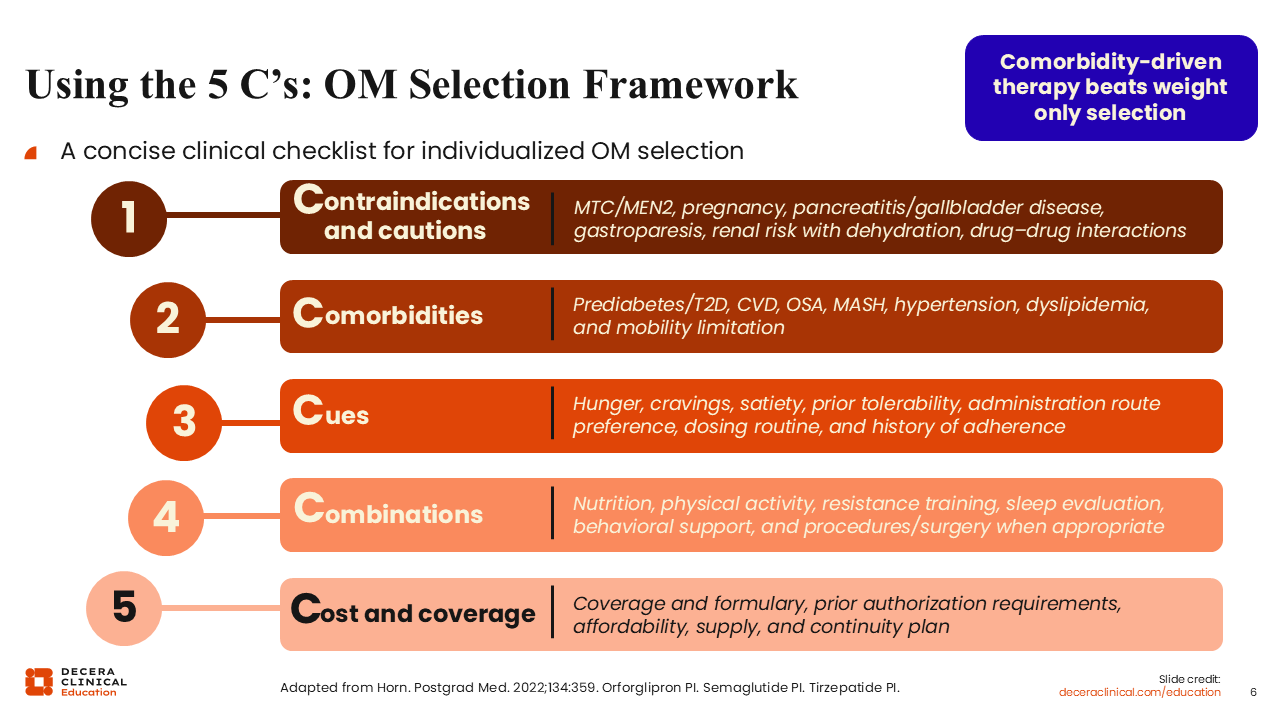
One framework that can support shared decision-making in obesity management is “the 5 C’s.” This approach provides a structured checklist to go over with patients when selecting the most appropriate OM.
The first C asks HCPs to consider the relevant contraindications and cautions. For incretin-based therapies, in particular, a personal or family history of medullary thyroid cancer or a history of multiple endocrine neoplasia type 2 represent 2 important contraindications. Acute pancreatitis has been reported, although rates are not necessarily higher than expected. Acute gallbladder disease may also occur and should be considered since gallbladder events can accompany weight loss itself. Gastroparesis is another important consideration, and acute kidney injury may occur if severe gastrointestinal AEs lead to dehydration. Finally, pregnancy is a contraindication for all OMs.
Potential drug–drug interactions must also be reviewed with particular attention paid to insulin and sulfonylurea, including glipizide, glyburide, and glimepiride. That is because concomitant use of these therapies may increase patients’ risk of hypoglycemia.7-10
Next, HCPs should evaluate any present comorbidities, such as prediabetes, type 2 diabetes, cardiovascular disease, obstructive sleep apnea, MASH, hypertension, dyslipidemia, and mobility limitations. Clinically meaningful weight loss can improve many of these comorbidities, and certain OMs may offer additional benefits in specific patient populations.
HCPs also must examine patients’ cues. Patients may present with different drivers of eating behavior, including hunger, cravings, reduced satiety, or difficulty maintaining fullness between meals. Prior treatment tolerability, administration route preference, dosing routines, and adherence history are additional cues that can provide important guidance.
The fourth C requires HCPs to consider treatment combinations. In general, OMs should be incorporated into comprehensive treatment plans that include nutrition, physical activity, behavioral modification, and appropriate lifestyle support. Similarly, physical activity recommendations should be individualized based on patients’ ability and should include resistance training to help patients preserve muscle mass. Adequate sleep is also important, as lack of sleep can contribute to appetite dysregulation. Further assessment should evaluate patients’ support systems, remain attentive to potential eating disorders, and consider referrals for metabolic or bariatric surgery when appropriate.
Finally, HCPs must address cost and coverage. Coverage requirements, formulary restrictions, prior authorization needs, affordability, and access should be reviewed before initiating an OM. Patients must also understand that obesity is a chronic disease and OMs are intended to be part of a long-term management strategy rather than a short-term intervention.15
Course Correction: Poll 4
A daily oral OM may be an excellent option for some patients, but it is not always the best choice. It is important to understand each patient’s daily routine to determine whether their preferred OM can realistically be incorporated into their life/routines.
One advantage of daily dosing is the potential for a more consistent therapeutic effect. Daily oral OMs may provide a steadier pharmacologic effect because of their continuous dosing, whereas weekly injectables may produce a stronger response early in the dosing interval, with diminished responses seen later in the week.
HCPs should evaluate patients’ daily routines, including their wake-up rituals, eating behaviors, whether they take other medications, how they manage their work schedules, and how they handle potential gastrointestinal AEs, before selecting the best route of administration. Oral therapies that require fasting or specific administration instructions may not be practical for all patients.
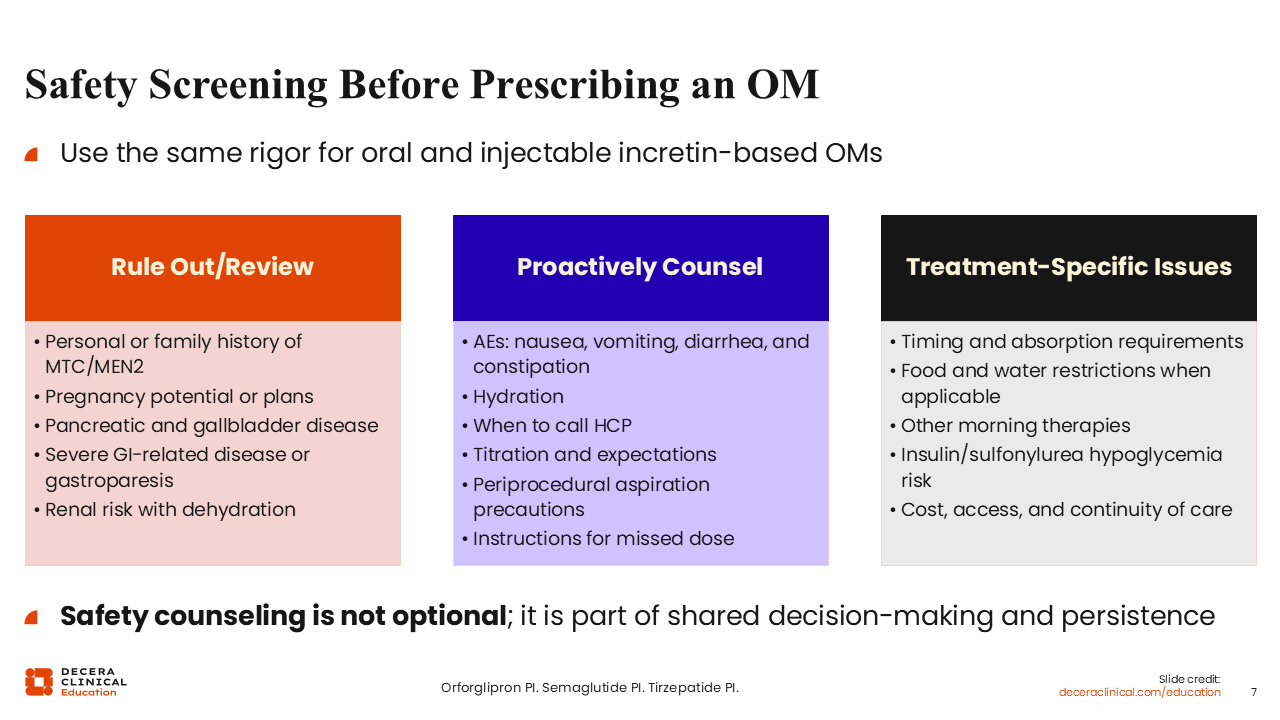
Safety Screening Before Prescribing an OM
Reviewing all safety considerations is an essential step before prescribing an OM. For both oral and injectable incretin-based therapies, HCPs must assess patients for absolute contraindications. In addition, pregnancy intentions should also be discussed, especially since patients’ fertility may improve as they lose weight. Those who previously believed they could not become pregnant might require counseling regarding adequate contraception and pregnancy planning during treatment. Other considerations include current or a history of pancreatic, gallbladder, or inflammatory bowel disease; severe gastrointestinal disorders; gastroparesis; and renal risk associated with dehydration.
After ruling out these concerns, HCPs can then counsel patients on the potential AEs associated with OM use. The most common include nausea, vomiting, diarrhea, constipation, and, in some cases, gastroesophageal reflux symptoms. Adequate hydration is important because OMs can reduce both appetite and thirst. Patients should also be encouraged to contact their care team if such AEs develop, as most can be managed via dose adjustments or supportive measures.
Regarding titration, dosing should be individualized according to patients’ treatment response and tolerability. That said, advancement to the maximum dose is not always necessary, and a slower titration may be appropriate for patients experiencing AEs. In addition, HCPs must set clear expectations with patients regarding weight loss. They should understand the average outcomes associated with each OM and be able to establish realistic goals.
Periprocedural considerations are important, as well. Patients undergoing general anesthesia should inform their surgeon and anesthesiologist that they are taking an OM. Because GLP-1 receptor agonists delay gastric emptying, this may increase patients’ aspiration risk. Appropriate medication interruption before surgical procedures should follow current recommendations and clinical judgment.
The final step in proactively counseling patients requires HCPs to address missed doses. In many cases, OMs can simply be resumed; however, prolonged interruptions may require reinitiation of dose escalation, especially in patients with a history of gastrointestinal AEs.
Then there are treatment-specific considerations like administration timing, absorption requirements, food and water restrictions when applicable, drug–drug interactions, hypoglycemia risk, and issues related to cost, access, and continuity of care. All of which further inform patients and guide shared decision-making.
Each of these points is important because safety counseling is an essential component of OM selection. It helps support informed decision-making and long-term treatment persistence.8-10
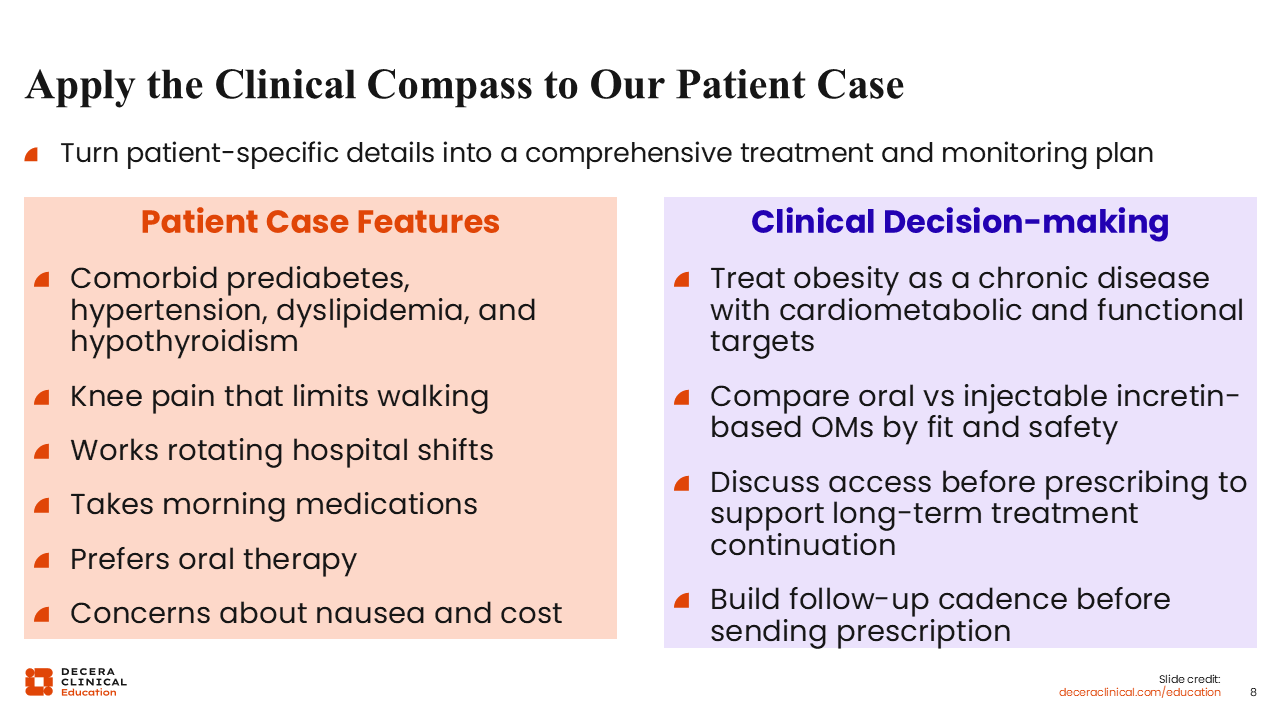
Apply the Clinical Compass to Our Patient Case
When applying these principles to our patient case, we need to first consider her comorbidities. She has obesity alongside prediabetes, hypertension, dyslipidemia, hypothyroidism, and knee pain that limits walking. Her mobility limitations should be factored into our physical activity recommendations. For example, lower-impact activities, such as water-based exercise, cycling, or elliptical training, may help reduce stress on the joints while supporting the patient’s weight management and overall health.
The patient also works rotating hospital shifts, which may affect her medication scheduling and adherence. In addition, she currently takes morning medications, which could complicate the use of oral OMs with specific timing requirements. Although some patients can separate their medications by adjusting the administration timing, dosing schedules must be individualized.
Furthermore, the patient prefers oral therapy and has concerns about costs and AEs like nausea. These preferences are important and should be incorporated into the decision-making process.
Remember, shared decision-making involves more than simply choosing the options patients initially request. Yes, their preferences should be integrated into the process, but it must coincide with clinical judgment and evidence-based obesity management principles. Obesity is a chronic disease; it requires long-term treatment and has important cardiometabolic and functional implications.
When evaluating patients’ treatment options, oral and injectable therapies should be compared based on clinical fit and safety. Access and coverage should be reviewed before prescribing to support long-term treatment continuation. A follow-up plan should also be established before treatment begins; for patients starting an OM, monthly follow-up during initiation and dose titration is appropriate.
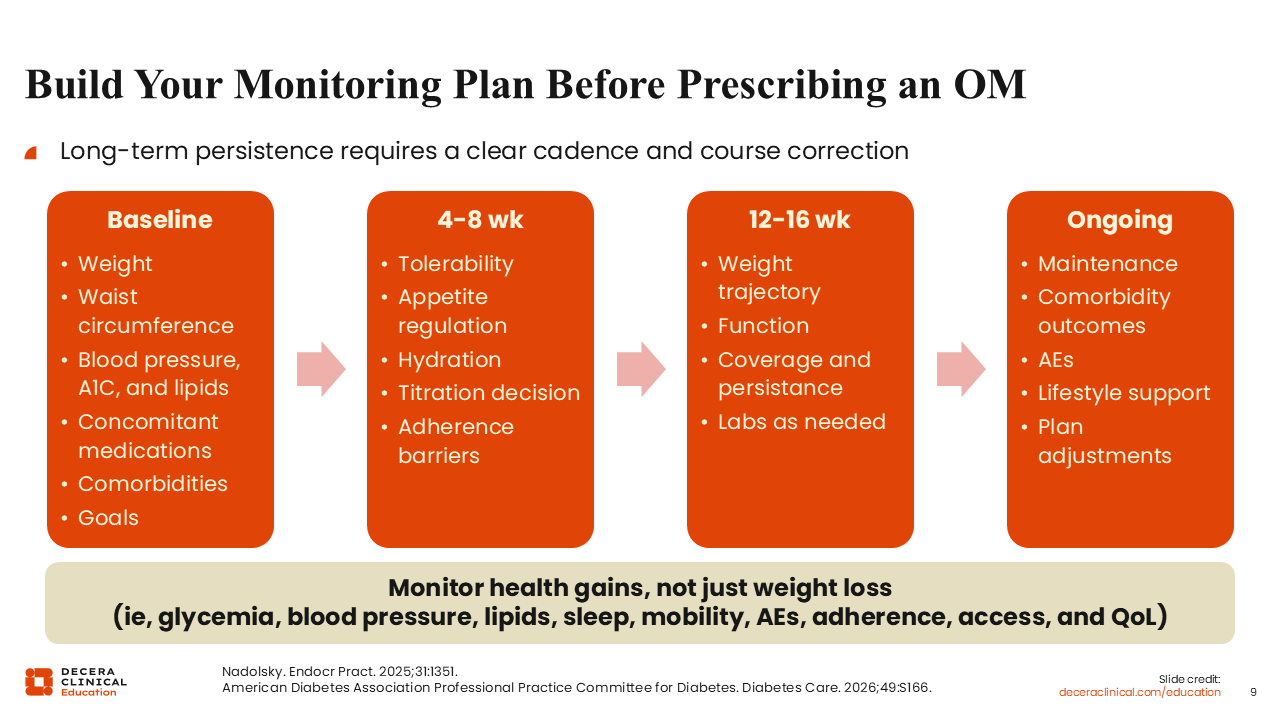
Build Your Monitoring Plan Before Prescribing an OM
Long-term obesity management requires a structured monitoring plan that supports treatment response, safety, and persistence.
Before initiating an OM, HCPs should complete a baseline assessment of patients’ weight, waist circumference, blood pressure, A1C, lipids, concomitant medications, comorbidities, and goals (ie, both weight- and health-related). Of note, it is critical to review concomitant medications with patients because some may contribute to weight gain or interfere with obesity treatment.
At approximately 4-8 weeks after initiation, HCPs should monitor patients’ tolerability, appetite regulation, hydration status, and adherence. I routinely ask my patients about their hunger and appetite because excessive appetite suppression may indicate a need to slow dose escalation or reduce the dose entirely. Conversely, persistent hunger may suggest the need for further dose titration. Regardless, the information gathered during these follow-up visits guides subsequent treatment decisions and helps identify barriers to adherence.
At approximately 12-16 weeks, HCPs’ evaluation should assess patients’ weight trajectory, functional status and mobility, pain, affordability, and continued access to therapy. Follow-up laboratory testing may be appropriate as well to measure cardiometabolic response and guide ongoing management.
Long-term monitoring must focus on maintaining an effective and sustainable treatment response. I often describe this as finding the “Goldilocks balance,” where patients can eat regularly, feel satisfied with small to moderate portion sizes, and maintain adequate nutrition without experiencing excessive hunger or appetite suppression. Comorbidity outcomes should also be monitored over time. Improvements in glycemic control, blood pressure, lipids, sleep quality, mobility, and overall health status are important indicators of treatment success. Note that blood pressure requires particular attention because antihypertensive therapy may need to be adjusted as weight loss progresses. Furthermore, patients should be advised to report symptoms suggestive of orthostatic hypotension.
Now your ongoing assessments are what will include AE monitoring, reinforcement of lifestyle modifications, support for increased physical activity, and encouragement of resistance training to help preserve muscle mass. Treatment plans should be adjusted as needed based on patients’ response, tolerability, and evolving needs.
The key message here is that obesity management extends beyond weight loss alone. That is why HCPs must evaluate patients’ overall health outcomes, including glycemic control, blood pressure, lipid levels, sleep quality, mobility, pain, AEs, treatment access and adherence, and quality of life.13,14
Course Correction: Poll 5
When developing a treatment plan for this patient, the most appropriate approach is one that integrates their comorbidity risk, preferences, dosing feasibility, safety considerations, coverage, and long-term monitoring.
Route of administration is an important consideration, but it should not drive treatment selection by itself. The decision-making process should also account for the patient’s cardiometabolic risk factors, current medication schedule, ability to adhere to treatment, tolerability concerns, and access to therapy. In totality, a comprehensive treatment plan incorporates all these factors and supports long-term obesity management rather than focusing solely on whether an OM is administered orally or by injection.
Expert Takeaways for Therapy Selection
Again, a stepwise approach can help guide individualized decision-making in obesity care. First, HCPs must identify the clinical target. This should consider any present comorbidities, complications, functional limitations, and patient goals, all of which will guide initial discussions and help define treatment priorities.
Next, HCPs should differentiate the available OMs based on their mechanism of action and potential impact on any present comorbidities. This includes evaluating GLP-1 receptor agonists vs dual GIP/GLP-1 receptor agonists, oral vs injectable therapies, and emerging treatment options to determine the most appropriate clinical fit.
The third step asks HCPs to apply appropriate safety rigor. That means screening for contraindications, reviewing the warnings and precautions, discussing potential AEs, and counseling on treatment-specific administration and titration requirements.
HCPs should then plan for treatment persistence, which might require them to address coverage, affordability, daily routines, treatment adherence, and follow-up requirements with patients. This should all be done before initiating an OM.
The final step requires HCPs to treat obesity as a chronic disease. Ongoing reassessment, dose adjustments, and course correction should be expected as part of the long-term management strategy. Weight maintenance is an important therapeutic objective, just as maintenance of blood pressure, glycemic, and lipid control are important in other chronic diseases.
Finally, shared decision-making remains the foundation of this process. Effective shared decision-making incorporates both patient preferences and clinical judgment regarding comorbidities, long-term benefits, safety considerations, and practical treatment options.13,14
Patient Case Takeaway: Individualizing Obesity Therapy Selection
The key takeaway from this patient case is that obesity should be recognized as both a chronic and treatable disease.
OM selection should always consider patients’ goals, cardiometabolic risk, preferences, dosing feasibility, safety concerns, tolerability, cost, and coverage. Furthermore, treatment planning should always include a structured, longitudinal monitoring strategy that supports treatment response, persistence, and ongoing assessment of overall health outcomes.
