CE / CME
HBV in Key Communities: Strategies to Overcome Barriers and Elevate Care
Pharmacists: 0.75 contact hour (0.075 CEUs)
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Released: March 12, 2026
Expiration: March 11, 2027

Activity
Road to Cure
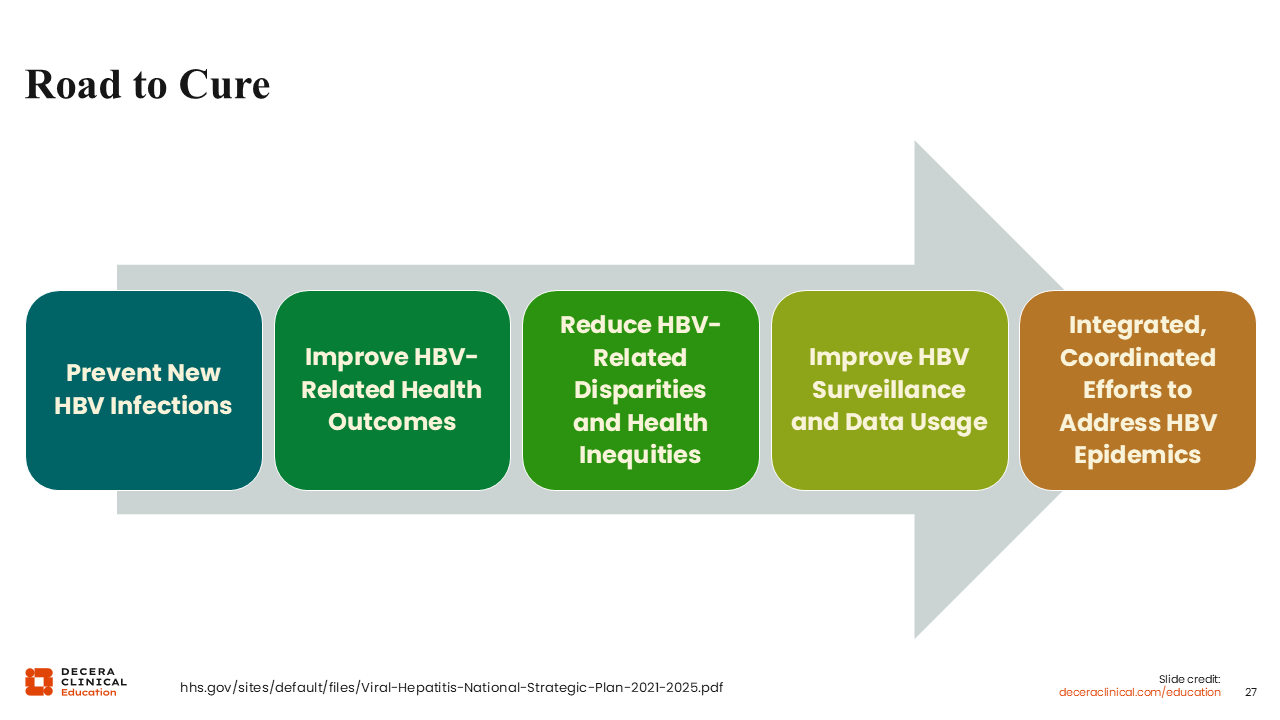
The road to cure remains a long one, with goals reaching beyond just development of improved therapies. In order to eliminate hepatitis B, we must approach the issue from multiple angles.
Preventing new infections is the first step on this road, highlighting the importance of vaccines. We must not lift our foot off the gas pedal. It’s up to us to ensure that infants get vaccinated, not just to avoid vertical transmission, but to avoid other household exposures during early infancy, from family members, other children, or caregivers.62
The next step is to improve HBV-related health outcomes. This means that, for people with HBV, HCPs must do a better job with screening, timely diagnosis and treatment, keeping people in care, and appropriate monitoring for disease progression.
Many people with HBV are not getting HCC screening and are being diagnosed with late-stage liver cancer, for which there are few effective interventions. In contrast, early-stage liver cancer can be curable and resectable. When diagnosis occurs too late, liver transplantation may be the only remaining option—and unfortunately, some patients are not even eligible for that.62
Reducing HBV-related disparities and health inequities goes hand in hand with improving HBV-related health outcomes. A key solution here is improving access to HBV care for key populations by simplifying treatment strategies and enabling people to be cared for by their primary care doctors so they don't have to seek specialized care from a hepatologist.62
HCPs can also improve HBV surveillance and data usage by leveraging electronic medical records and working with health departments that do HBV surveillance. This would allow for better identification of communities burdened with HBV that need extra care and assistance.62
Ultimately, all these steps come together to form an integrated and coordinated effort to address hepatitis B epidemics. For example, New Jersey, where I am located, has a very high population of people who are born outside the US, with high rates of hepatitis B and late-stage liver cancer. This indicated a significant gap in HBV diagnosis and screening.
In response, the New Jersey healthcare system implemented an automated HBV screening system in emergency departments. This system uses electronic medical records to identify patients who present to the emergency room and have not already been screened for HBV.
This system enabled New Jersey HCPs to scale up HBV screening, in what I would describe as a microelimination initiative. I think global HBV elimination will require synergy between many different microelimination approaches in different settings and communities.62
Community Engagement is Central
Community engagement across the care continuum is another critical component of our journey towards HBV cure. HCPs must work closely with community partners, especially those who represent people with higher rates of hepatitis B, to improve screening, access to care, and consistent monitoring.
In terms of screening, there are many successful examples of groups that conduct HBV screenings in community settings, such as churches, schools, or community groups.
Community partners can also provide a lot of education. For example, newspapers or media outlets in languages other than English can help overcome language barriers in immigrant communities and increase awareness of the burden of HBV. In turn, increased awareness increases screening and diagnosis. Once people are diagnosed, they can be linked to care and provided treatment, thereby preventing disease progression and facilitating ongoing monitoring to prevent HCC.
High-burden communities often experience lower rates of HBV screening and treatment, and higher rates of cirrhosis and HCC. Culturally competent care is key for reaching these groups, and working with community groups is the best way to learn how to provide culturally comprehensive care. HCPs coming from academic centers or the larger healthcare facilities often don't understand the cultural nuances in these groups. So, it is important to partner with community leaders to engage patients who could become candidates for future therapies in the pipeline. The key is to let people know that getting care now helps set them up to be candidates for future cure—they may not be eligible if their disease progresses past a certain point.
Culturally responsive engagement is also crucial for keeping patients informed and building trust in the healthcare system. Without that foundation of trust, people often can be very suspicious of innovations and clinical trials. In fact, it is critical for key communities to be informed and participate in clinical trials, and to be prepared to better digest what the new science is saying.
Hep B Foundation Resources
A group that does great work in this area is the Hepatitis B Foundation. I recommend all HCPs avail themselves of the resources here for their patients.63
The Hepatitis B Foundation has many resources that are easy for patients to understand. They have fact sheets, infographics, blogs, and podcasts with many great guests. This also can be helpful for patients who have questions they aren’t comfortable sharing with their HCP.
I often recommend that patients familiarize themselves with these resources as well, especially if they're newly diagnosed and feeling lost and overwhelmed. They may feel a lot of self-stigma. They may not know how to address having hepatitis B with their family members and partners, and hearing stories from other people can help them not feel alone.63
For these patients, the Hepatitis B Foundation’s "JustB" is a collection of stories told by people affected by hepatitis B, featuring people from all over the world at various stages of life and of diverse genders. I always tell patients to look into this, to help them realize they're not alone. There are a lot of people living with hepatitis B.63
The Hepatitis B Foundation also has a discrimination registry and some resources on Know Your Rights. If patients feel like they are facing discrimination or have issues with employment, they can turn to these resources. It is illegal to discriminate against people with hepatitis B from employment or school based on the Americans With Disabilities Act.63
The Hepatitis B Foundation also provides a global online support group for people with hepatitis B. In addition to peer support, the group includes researchers who communicate new research findings in lay language. This is particularly important as we move toward curative therapies, ensuring that patients are informed about progress and have a better understanding of what is coming down the pipeline.63
So, I encourage HCPs to share these resources with their patients.
Key Points
The CDC now recommends universal HBV screening and vaccination. There has been a shift in the AASLD treatment guidelines towards expanded treatment eligibility for more timely treatment, with shared decision-making for certain groups.
A survey conducted by the Hepatitis B Foundation to inform the WHO guidelines revealed shocking data: Globally, approximately 50% of patients with HBV said their doctor never discussed treatment with them. At a minimum, HCPs must make sure to inform patients of their treatment options. Patient preferences and values should be considered equally during shared decision-making, and if a patient desires treatment and is willing to take medication, there are very few scenarios in which I would say they are not eligible. Thus, shared decision-making is critical in hepatitis B care.
With regards to monitoring, qHBsAg can be a valuable tool in clinical practice, particularly with a growing pipeline of investigational HBV therapies aimed at functional cure or HBsAg loss. I am especially awaiting data from the phase III bepirovirsen studies, as patients with low baseline qHBsAg may be strong candidates for this therapy.
Finally, engagement in care is essential. Keeping patients connected to care allows for appropriate long-term monitoring and ensures they are well positioned to benefit from emerging therapies