
CE / CME
Overcoming Vaccine Hesitancy: From Concerns to Confidence at the Point of Care
Pharmacists: 0.75 contact hour (0.075 CEUs)
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Released: March 06, 2026
Expiration: March 05, 2027


Activity
Steps You Can Take With Every Vaccine-Hesitant Person
Rupali J. Limaye, PhD, MPH, MA:
The great news is that you hold a lot of power as an HCP. You hold the trust of patients who come and see you. Although it may seem daunting, you have the ability to talk about vaccines and address vaccine hesitancy through a number of different strategies and methods that just take a little bit of practice.
On this slide are some strategies that we suggest using with every single person who may have concerns or questions about vaccines. These can be effective approaches for people in the malleable middle.
Change Social Norms by Sharing That You and Many Others Receive Vaccines
Rupali J. Limaye, PhD, MPH, MA:
First, highlight that most people in the community are getting vaccinated and accept vaccines. Think about peer influence and highlight it for every single person with whom you talk.
Richard Zimmerman, MD, MPH, MA:
Habit and social norms really make a difference in who receives vaccines. A social group as a whole may be very hesitant, so we need to develop ways to reach out to them.
For example, I like to say, “Many patients get vaccinated, even though you don't hear about it on social media. Most of my patients take, for instance, the pneumococcal vaccine. That might not be popular on social media, but I can tell you that’s been my experience in taking care of hundreds of patients.”
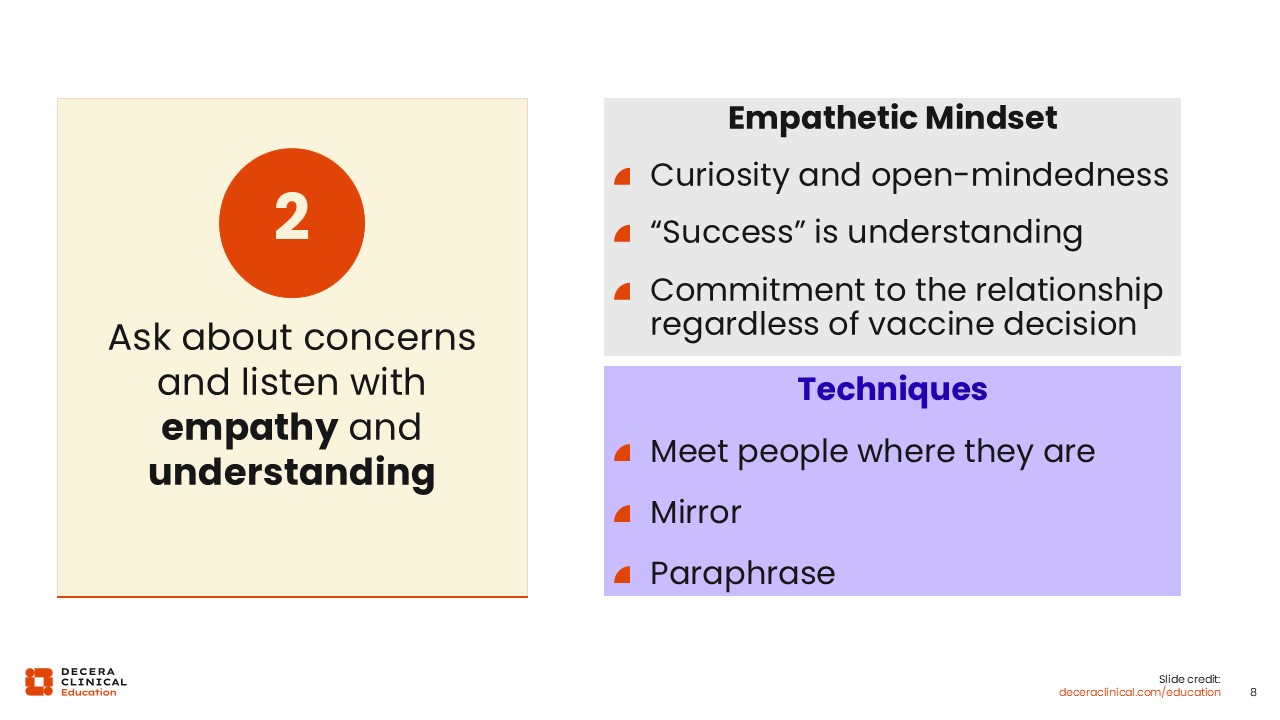
Ask About Concerns and Listen With Empathy and Understanding
Rupali J. Limaye, PhD, MPH, MA:
Another step you can take is grounding every conversation that you have in empathy and understanding. Vaccine-hesitant patients who come to you are vulnerable. They come to you with concerns. The worst thing you could do as an HCP is dismiss those concerns.
Richard Zimmerman, MD, MPH, MA:
Here is another example of a conversation I have had in clinic:
“I understand, John, that you are concerned that you are going to get flu from this vaccine. That is a concern I’ve had other people tell me about as well.
“I hear your concern that this vaccine will give you flu, but this is an inactivated vaccine, so it can’t infect you. If you got the flu after getting vaccinated last year, you may have gotten it from being in my waiting room with someone who was sick, or maybe it was because somebody with the flu came to one of the basketball games you attended, despite being sick. But this vaccine can’t give you the flu because it is inactivated. It can give you a sore arm, but it can’t give you the flu.”
Rupali J. Limaye, PhD, MPH, MA:
In those examples, you can see how we acknowledge the patient’s concerns. You can also do this by mirroring.
When someone says something like, “I have a concern about this ingredient in a vaccine,” you could say, “I understand that you have a concern about this ingredient in the vaccine. Can you tell me a little bit more about what your concern is?”
With this, you are mirroring what patients are saying, ensuring that they feel heard. In addition, you are inquiring what the concern is, so you can help resolve it.
A similar approach is paraphrasing. When someone says to you, “I know that there is something in this vaccine that is going to lead to infertility,” you could first summarize that concern and then talk about why that is not the case.
I would say, “I understand you have concerns that there might be some sort of ingredient in the vaccine that could lead to infertility. I’ve done a lot of work on this, and what I’ve and many other people have found is that there are no ingredients in this vaccine that affect fertility.”
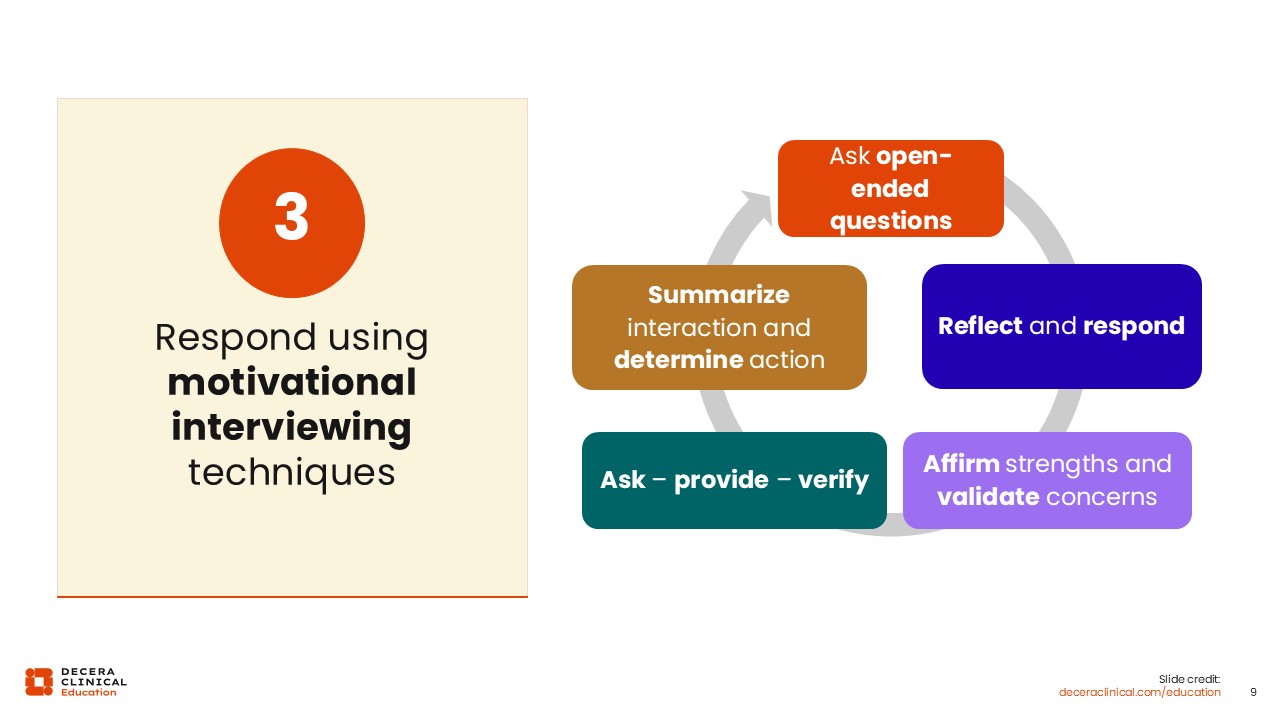
Respond Using Motivational Interviewing Techniques
Rupali J. Limaye, PhD, MPH, MA:
A third piece of advice is to use techniques related to motivational interviewing, which can be especially effective for people with more concerns or hesitation about vaccination.
This approach includes active listening, making sure that you are recapping the conversation, and asking patients if they need additional information. This shows that you understand patients’ concerns.
We have learned that it does not help if you tell someone that the are wrong. For example, if someone says to you, “I know that Bill Gates has put something in this vaccine to poison our community.” The worst thing you can do is say, “Actually, that’s not true.”
The better way to work through this misconception is with education and discussion. You can say, “May I explain to you a little bit about how a vaccine is developed and how it's made?"
Asking permission to explain what the process is, and going through the process using words that people are comfortable with, are crucial to keeping the conversation open. These techniques are useful, especially with people who have major concerns and who will need a little more of your time.
I would start this conversation by asking open-ended questions. For example, if they say, “I don't want to get the vaccine,” I would say, “Can you tell me a little bit more about what your concerns are?”
Then, after patients tell you what their concerns are, I would reflect upon that and respond.
If a person says, “I’ve heard that this vaccine can cause a really high fever after getting it,” I would respond by saying, “Yes, this vaccine may cause some acute illness, and you may have a fever. However, this is normal, and this is simply showing that your immune system is responding to the product.”
You then want to make sure that you are affirming their strengths and that you are validating their concerns.
I would do this by saying, “You and I have the same goal. We want to make sure that you and your family are healthy. I understand that there’s a lot of information out there, and it’s hard to understand what is true and what is not true. But I’m here to tell you that there’s actually no concern about any long-term effects related to getting the vaccine and having a fever.”
You then want to ask if they have any other questions or concerns and reflect that back to them. Then, you want to verify that you are understanding their concern completely. Finally, you want to summarize this interaction.
If they ask for additional information, I would say, “I can provide you with some additional information about this product,” or, if it seems like they are ready to make a decision, I would say, “Let's go ahead and get you vaccinated today.”
Use Analogies, Visual Storytelling, and Reframing to Make Messaging Memorable and Concrete
Rupali J. Limaye, PhD, MPH, MA:
The amount of jargon in healthcare can sometimes make it difficult for patients to understand vaccine safety and efficacy. So, I recommend using analogies wherever you can.
Richard Zimmerman, MD, MPH, MA:
I sometimes use a flight simulator analogy. Pilots do flight simulator training so that they are prepared for a dangerous situation ahead of time. You do not want your pilot to learn about flying in turbulence or storms without practice. You want them to have a safe simulation so they can be prepared for a real emergency.
In a similar way, vaccines protect people by training the immune system to counter threats from pathogens. Like a flight simulator simulates bad weather conditions, the noninfectious vaccine antigens simulate attacks from viruses and bacteria, preparing the immune system ahead of time so that when an actual attack occurs, it is ready.
Another way to think about vaccines in the human immune system is as a software update. This is particularly useful for annual vaccines like flu vaccines, which are updated every year because the flu virus mutates so rapidly.
We download software updates for our phones for better protection against current viruses and threats. The annual influenza vaccine is like a software update for the immune system, so it is prepared for the viruses most likely to circulate this year.
Rupali J. Limaye, PhD, MPH, MA:
Using analogies is especially useful when we talk about risk, safety, and benefits.
For example, if someone says, “I have heard that there is a risk that my 4-month-old son can have febrile seizures after receiving these vaccines,” I would respond by saying, “He is more likely to be struck by lightning in his lifetime than to experience a febrile seizure related to these vaccines.”5,6
I find that gives patients a better idea of how low the risk is and helps put it into context. Analogies will not work for everyone, but in my experience, they are important when talking to someone whose concerns are larger than the risks really are.
Overall, I think the most important thing is to tailor those analogies to who you're speaking to.7
Another great way to talk about the benefits of vaccines is with visual storytelling. For example, you can do this with the ongoing measles in the United States to show patients that, unfortunately, children who are infected with measles are really struggling. However, you must be judicious when using this technique. I think sometimes showing some of the effects of the disease can be helpful, but in other instances, it is too much of a shock factor. The storytelling approach should focus more on the end goal.
You can also reframe vaccination as being about avoiding loss. You could use a different analogy to show that vaccination is a preventive approach to ensuring that your child grows up healthy or that you stay healthy.
Here, I often liken vaccines to car seats. You hope that you will never get into an accident, but if you do, you know that your children are protected because they are in the car seat. Similarly, you hope your children never are exposed to measles. But if they are, they are protected because they have gotten the vaccine.
Give a Personal and Presumptive Vaccine Recommendation
Rupali J. Limaye, PhD, MPH, MA:
So the final technique we recommend is presumptive recommendations. That is, we should presume that patients will accept the vaccine. You can do this as simply as saying, “You're due for a shot today. Let me get it ready for you.”
When we talk about presumptive communication, we are essentially telling people that this is the norm.
Richard Zimmerman, MD, MPH, MA:
A presumptive approach can also build on discussions of risk and preventing loss.
For instance, I might find myself saying, “Mr. Jones, you have COPD, and you will be at really high risk for pneumonia and hospitalization if you do not get your flu and RSV vaccines. I have seen patients who have been hospitalized with one of these viruses, and they sometimes don’t get to go home. They have to go to a long-term care facility or a rehab facility. I don’t want that for you. Let’s get you vaccinated today.”
Rupali J. Limaye, PhD, MPH, MA:
It is also important to talk about what vaccines you have done with your family. This helps build trust between you and your patient.
You can even say something like, “This is what I did for myself. This is what I did for my kiddos, and this is what I would recommend for my friends.”
It is critical to try to focus on the personal aspect of it rather than only talking about it medically.

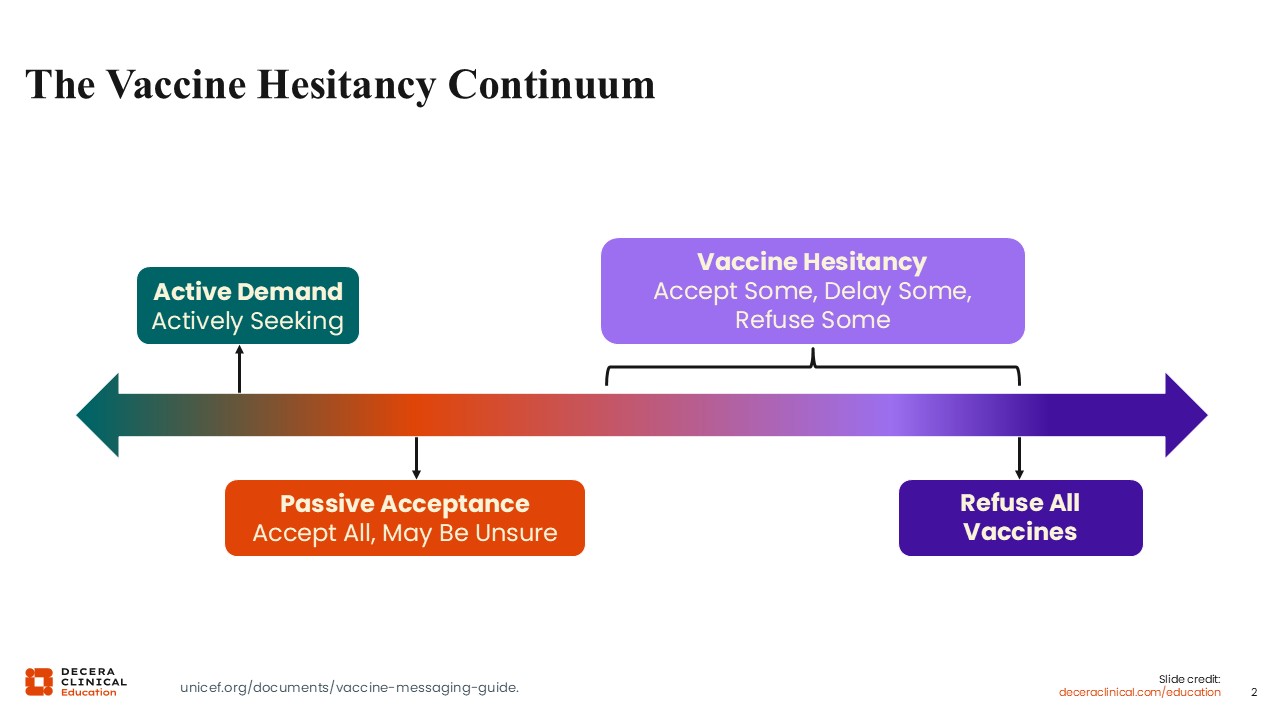
Effective Techniques Across the Vaccine Hesitancy Continuum
Rupali J. Limaye, PhD, MPH, MA:
Given that, vaccine hesitancy is not a binary behavior; we know that people fall along this continuum. What we really want to focus on is where you want to use the techniques we reviewed.8
Presumptive communication, talking about a personal recommendation, tailoring your message, using analogies, using motivational interviewing, and highlighting social norm—I would really focus on using these for people that are in the malleable middle.
Which technique you should use depends on what their concern is and their level of trust with you. For example, if the person just needs a nudge, I focus on social norms and use the presumptive approach.
However, for the person with a lot more concerns, I use motivational interviewing because that is geared toward people with more significant concerns.
All of these different approaches can be used across the continuum. You can use them across different people and across different vaccines. It depends on what you feel comfortable using and what you feel is working with your patients.
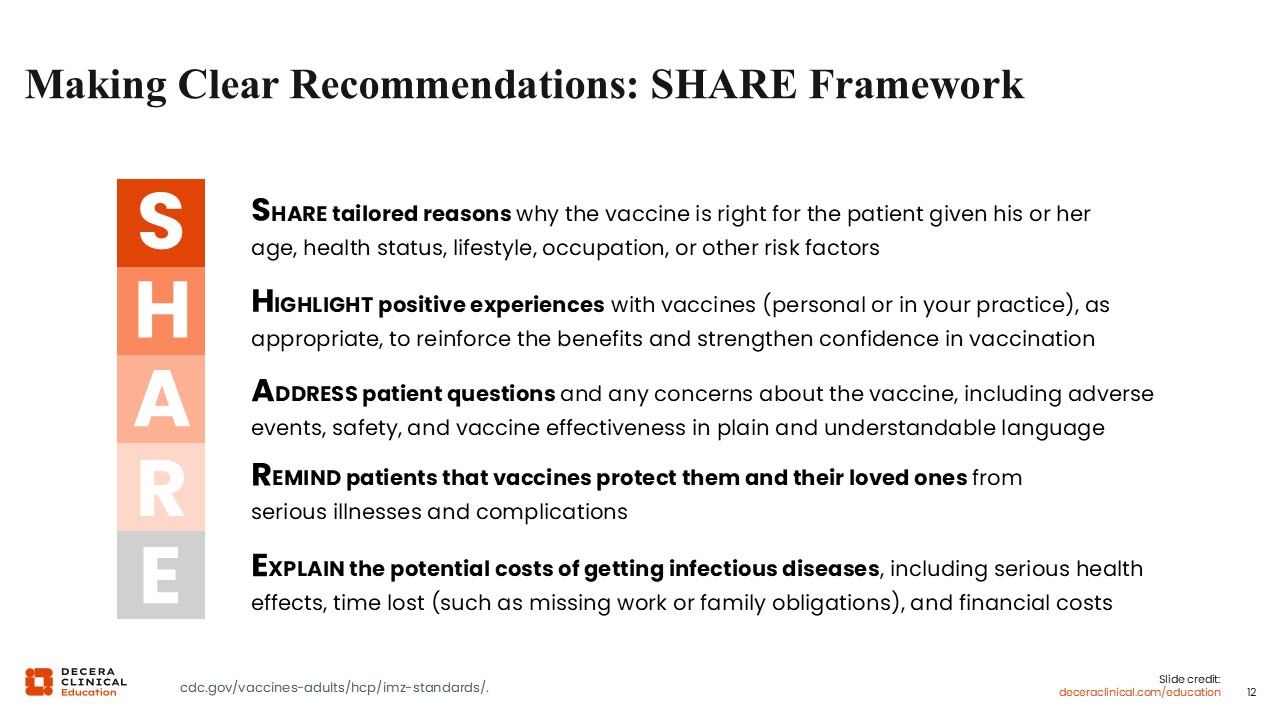
Making Clear Recommendations: SHARE Framework
Richard Zimmerman, MD, MPH, MA:
Another helpful tool is the SHARE framework: sharing tailored reasons why the vaccine is right for a particular patient based on age, lifestyle, occupation, or other risk factors. This is particularly important for risk-based vaccination.
For instance, persons who have chronic cardiac diseases or pulmonary diseases are at risk for pneumococcal bacterial infection, RSV, flu, and COVID. So we can give recommendations tailored to these particular medical conditions.9
Another example of tailoring recommendations to medical conditions is recommending the hepatitis A and B vaccines for protection against further liver damage in patients with hepatitis C. We cannot cure hepatitis C, but we can protect patients from worse liver outcomes from hepatitis A and B, like inflammation, cirrhosis, and liver failure.9
The H in the SHARE framework is for highlighting positive experiences from vaccines. Similar to the reframing we discussed earlier, rather than addressing the problems we see in people who have not been vaccinated, we highlight how vaccines have improved lives.
I think of a dear family friend from my church who was an engineer, a most kind man, who was crippled in adulthood by polio. It is devasting to see him using his crutches, taken from the prime of life to permanent disability. My father took care of him as he developed postpolio syndrome. The pain that went with that, the degradation in physical functioning, was excruciating. I wish we could have prevented his illness, but at the time, the polio vaccine was not available. He was not vaccinated in time, and so he unfortunately suffered from it. Now, we have essentially eradicated this devastating disease, thanks to the polio vaccine. No one else has to suffer this same loss.9
We also want to address patient questions using language that is accessible to patients when discussing adverse events and safety.
As previously discussed, it can be helpful to use analogies, such as the likelihood of getting hit by lightning vs the likelihood of severe vaccine reactions.
I also remind patients that they are protecting their loved ones with vaccination. Parent to child, grandparent to grandbaby, or child to grandparent—nobody wants to be the conduit of infection.9
The last component of the SHARE framework is explaining the potential costs of vaccine-preventable diseases. That may mean time off from work, resulting in a financial hit. Among older patients, hospitalization with some of these diseases may mean that they are not able to return home. That is a powerful motivator.9
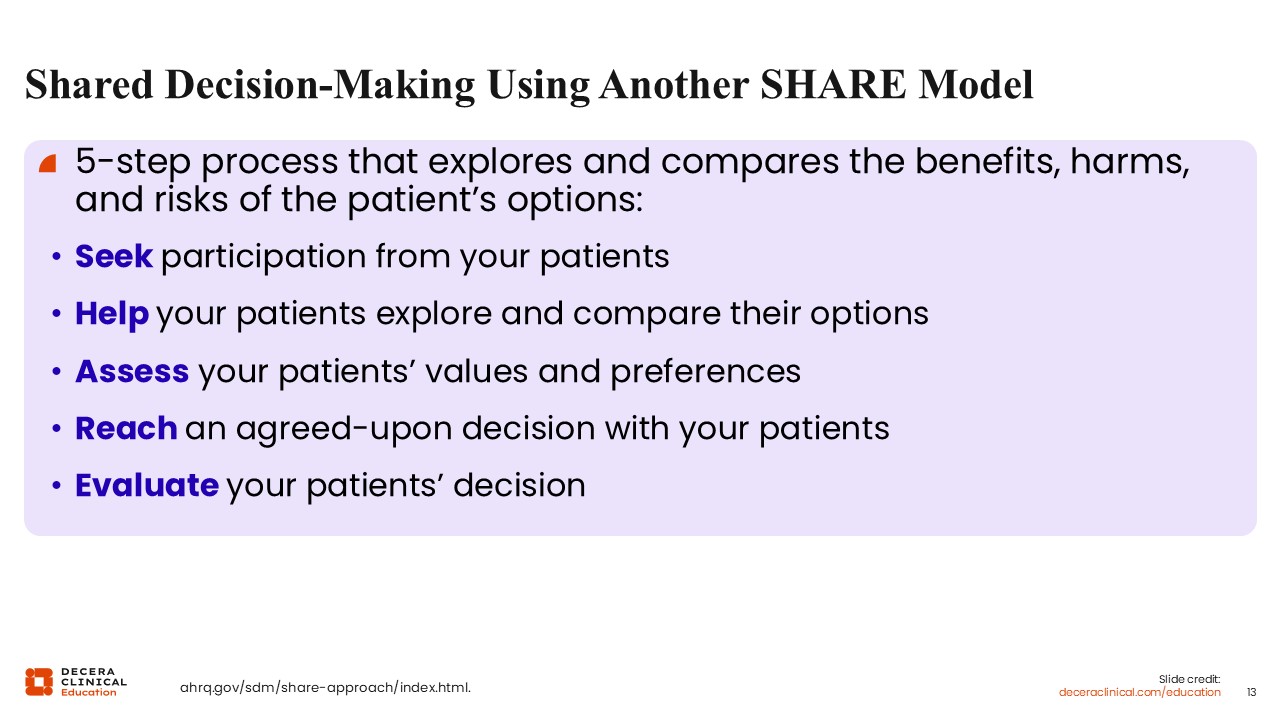
Shared Decision-making: Another SHARE Model
Richard Zimmerman, MD, MPH, MA:
Another version of the SHARE acronym can help explore the benefits, harms, and risks of vaccinating.
To use this model, first seek participation with your patients so that you know what they are thinking. Then, help them to compare their options. Some people might choose to delay a vaccine if they are adamantly refusing to do all the vaccines at once. You could schedule an extra visit.
Next, assess their values. If there are 2 vaccine options, sometimes people are more open to receiving one than the other. For instance, if somebody does not want an mRNA vaccine, they may be open to a protein vaccine.
After these steps, hopefully, you can reach a decision. Sometimes patients will want to delay vaccination, in which case that next visit can be scheduled soon.
Finally, help them to evaluate their decision, reinforcing your care for them, but also encouraging them to be vaccinated.10
Facilitating Discussions With Patients: The AIMS Model
Richard Zimmerman, MD, MPH, MA:
The AIMS model is another way to facilitate discussions with patients. This model has only 4 components, whereas many other models have 5 or more. This is a simple one that we can all memorize and use: announce, inquire, mirror, and secure.11
Resources to Consult for Vaccine Recommendations and Info
Richard Zimmerman, MD, MPH, MA:
We are now in a situation where decades of harmony between the CDC and professional societies on vaccine schedules for children, adolescents, and adults is no longer maintained. There is a difference between the groups’ recommendations, and I do not know when or if a harmonized schedule will occur again.
These are various recommendations and sources of information that you can refer to in order to make informed decisions about vaccination.
There are particular locales that have decided which recommendations to adhere to. For instance, the Commonwealth of Pennsylvania has decided that its official schedule is the American Academy of Family Physicians (AAFP) immunization schedule, supplemented by the American College of Obstetricians and Gynecologists (ACOG) immunization schedule for pregnant women.12
The American Academy of Pediatrics (AAP) has provided a vaccination schedule for 2026 that has been endorsed by the AAFP, the Infectious Diseases Society of America (IDSA), and others.13
This demonstrates that professional societies are getting together to create a harmonized “professional societies” pediatric vaccine schedule. The IDSA has guidelines for immunocompromised persons, and the American College of Physicians (ACP) has an adult immunization schedule. These schedules will receive ongoing updates.14,15
I suspect that we will end up with 3 or 4 harmonized professional society schedules and a somewhat overlapping, but also somewhat different, CDC schedule. I think those schedules will be: the AAP childhood immunization schedule endorsed by the AAFP; an adult immunization schedule, jointly proposed by the AAFP and ACP; the ACOG vaccine schedule for pregnant women, which may also overlap with the AAFP guidelines; and the IDSA guidelines for immunocompromised persons.
In addition, the Vaccine Integrity Project is collating up-to-date literature reviews. Those literature reviews summarize key issues of vaccine effectiveness and safety and are shared with professional societies so that they can make recommendations on the basis of the latest evidence.16
It is unfortunate we no longer have one single source, but that is the reality today. HCPs would also need to look at what guidelines are used by their state and by their particular professional society.
For an example of how to address caregiver concerns about the vaccine schedule and changing pediatric vaccine recommendations, view the following demonstration video:
