CE / CME
New Overweight and Obesity Recommendations: Implementing Definition and Diagnostic Updates Into Your Practice
Physician Assistants/Physician Associates: 0.25 AAPA Category 1 CME credit
Nurse Practitioners/Nurses: 0.25 Nursing contact hour
Physicians: maximum of 0.25 AMA PRA Category 1 Credit™
Released: September 25, 2025
Expiration: September 24, 2026

Activity
What Is Obesity?
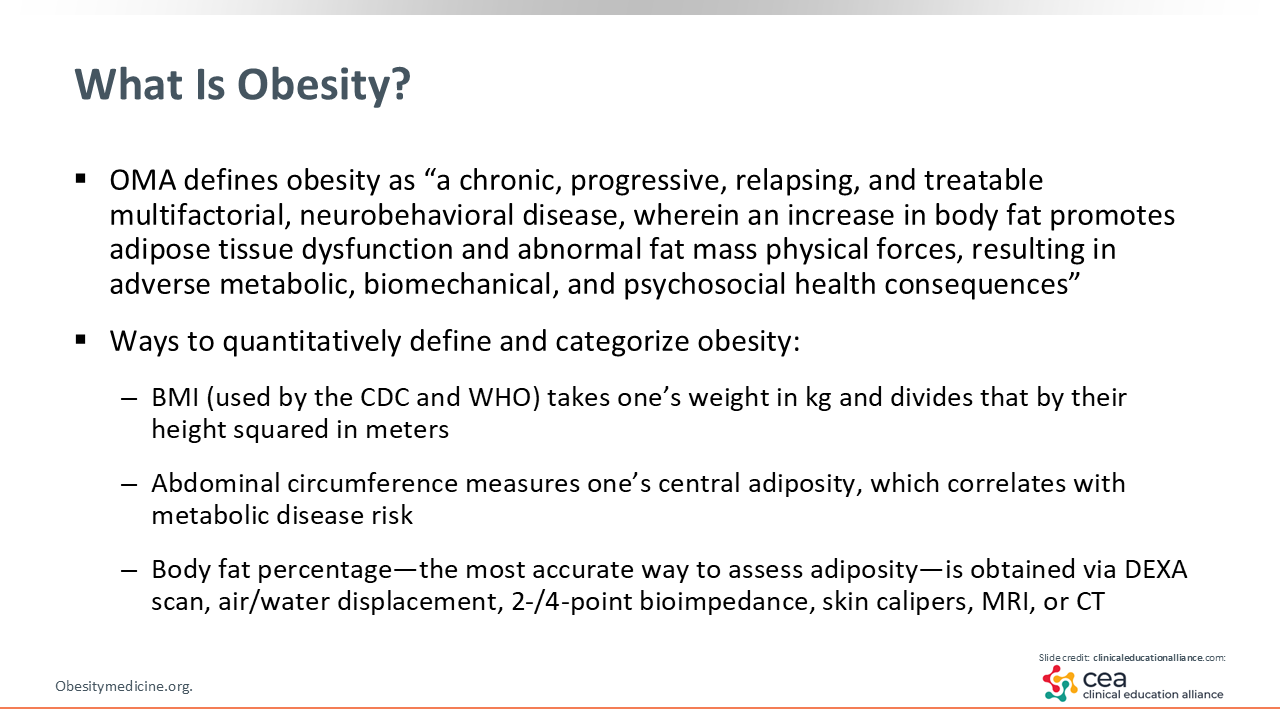
The Obesity Medicine Association (OMA) defines obesity as “a chronic, progressive, relapsing, and treatable multifactorial, neurobehavioral disease, wherein an increase of body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, biochemical, and psychosocial health consequences.”1 That is a very comprehensive and complex definition. And the disease of obesity is exactly that—comprehensive and complex.
What this definition is clarifying is that obesity is more than just someone’s weight on the scale or their BMI. This has to do with the distribution of body fat and how that is causing the pathophysiology of obesity within the patient. This pathophysiology may present itself in hormonal abnormalities, where healthcare professionals (HCPs) can see metabolic changes in lipids, blood pressure, and glucose, among other parameters. There also is an effect of excess adiposity the weight-bearing joints of the hips, knees, and ankles. Finally, excess adiposity can cause patients to breathe improperly when laying flat, which is where obstructive sleep apnea (OSA) can come into play. The take-home message is that HCPs must think of obesity as globally as this definition is instructing us to.
How do we quantify and categorize obesity?
BMI is the most common approach that we use that also is the least effective way to categorize obesity. It only takes into account the actual body weight and height of a person. Looking at the definition of obesity, it is more than just one’s body weight and height. Obesity more so has to do with the distribution of body fat (or excess adiposity) and how much of one’s weight is composed of this body fat.
A better indicator to help us to categorize obesity is abdominal circumference. This measurement is going to be more straightforward and the least costly method we have. Furthermore, HCPs can educate patients properly on taking this measurement at home.
Then there is the direct measurement of one’s body fat percentage, which is another way to classify and categorize obesity. Among men, for instance, the appropriate amount of body fat that contributes to their overall weight should be <30%. Among women, this percentage should be <35%.1 Regardless of patients’ height, age, and weight, HCPs should ensure that the amount of body fat contributing to that overall weight is in these parameters.
How can we measure body fat percentage? First, there is the dual-energy x-ray absorptiometry (DXA) scan, but unfortunately, most health insurance companies do not cover this. Rather, the DXA scan is more commonly used in research settings. Air and water displacement is another method, but that also is not typically covered by health insurance. Furthermore, patients may be required to report to special clinic locations to have these tests done.
I commonly use bioimpedance devices—we have one in my office. I also recommend obtaining a scale that measures body composition to all my patients. These cost $25 to $600, depending on how many features are included in the device.
Consistency is the most important thing to remember when measuring patients’ weight or body fat—consistency with the measurement that is used, with how that measurement is done, the time of day at which the measurement is taken, and whether or not the patient is wearing clothes. These things matter, which is why the best measurement of body composition and waist circumference is actually done in patients’ homes.
HCPs can educate patients on how to take these measurements. They can then perform the measurement(s) and provide us with the information.
Skin calipers is another way to measure patients’ body fat percentage, but I find that this can cause discomfort among patients. I also do not use waist circumference. When it is obvious that the patient is carrying excess adiposity, I do not want to bring out the measuring tape. That generally is used for those with a lower BMI, when I am trying to determine if they truly do have hidden body fat in the viscera.
In thinking of our Asian population, their cutoffs for overweight and obesity are different from what commonly is used for the general population.2 That is because they likely have hidden body fat in their viscera, so HCPs should look for a higher waist circumference.
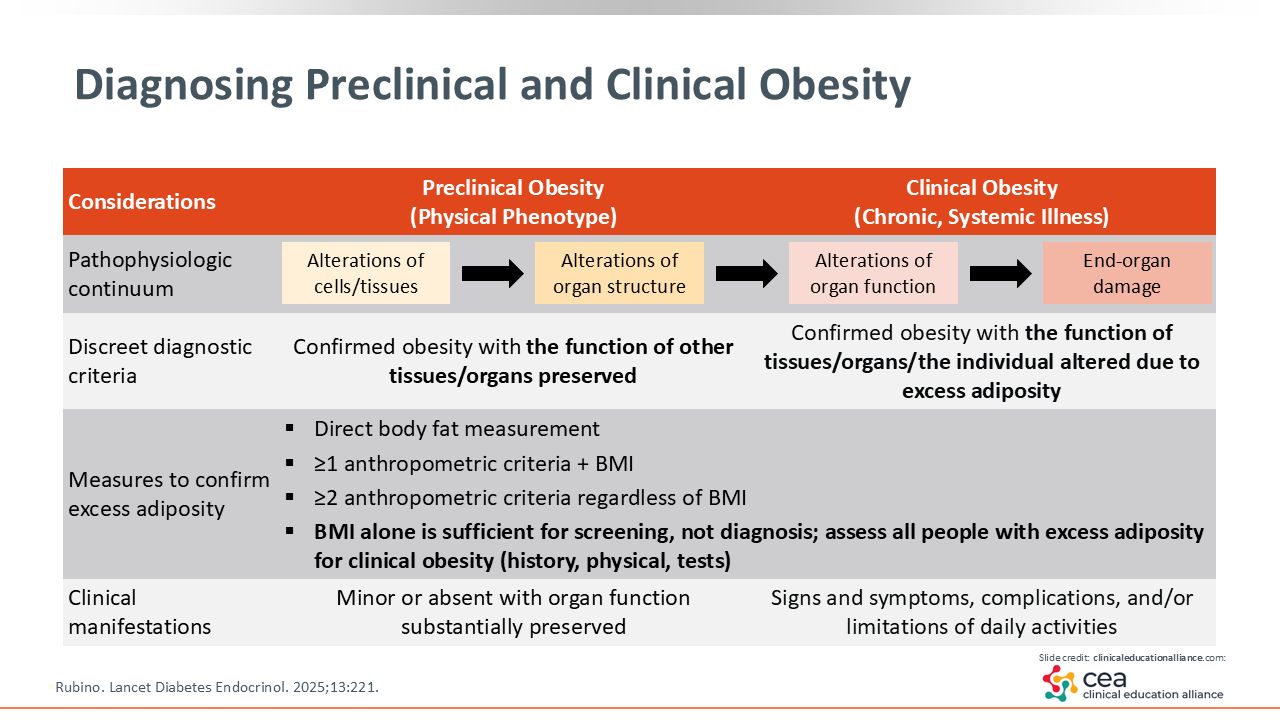
Diagnosing Preclinical and Clinical Obesity
This slide highlights a recent publication in Lancet Diabetes & Endocrinology. A group of experts came together from all over the world to lay a foundation for how we should look at obesity in its early stages, as well as clarifying when patients clinically are experiencing metabolic derangements and other impacts of the excess adiposity (or obesity).3
Although many organizations have endorsed the conclusions in this article, there are a select few that have not, including the OMA and European Society for Obesity Management. The disagreement stems from the terms “preclinical obesity” and “clinical obesity.” The OMA, in particular, feels that the distinction between the two increases the risk that patients with preclinical obesity may not receive insurance coverage for applicable treatment, which could leave millions without access to care. It also feels that having this kind of differentiation could risk delays in treatment; if HCPs must wait until patients have clinical obesity (defined in the Lancet Diabetes & Endocrinology article as having alterations in organ function and end-organ damage), they could face potentially worse long-term outcomes and more severe complications.
Furthermore, this new approach could reinforce weight-related stigma. Critics argue that framing preclinical obesity as a personal choice or risk factor, rather than a medical condition, could worsen preexisting weight-related bias and stigma in both the health system and general public.4 Finally, there is lack of clinical validation. Some point out that the proposed diagnostic criteria rely heavily on population level data and lack the sensitivity and specificity needed for individual patient diagnosis.5
That being said, overwhelming numbers of organizations have endorsed Rubino and colleagues’ conclusions. Therefore, HCPs need to understand that the premise of this is to evaluate the complete presentation of patients with overweight or clinical obesity. In addition, HCPs should ensure they are identifying early presentation of this disease, metabolic derangements, impacts on quality of life, and where patients are at on the continuum of obesity.
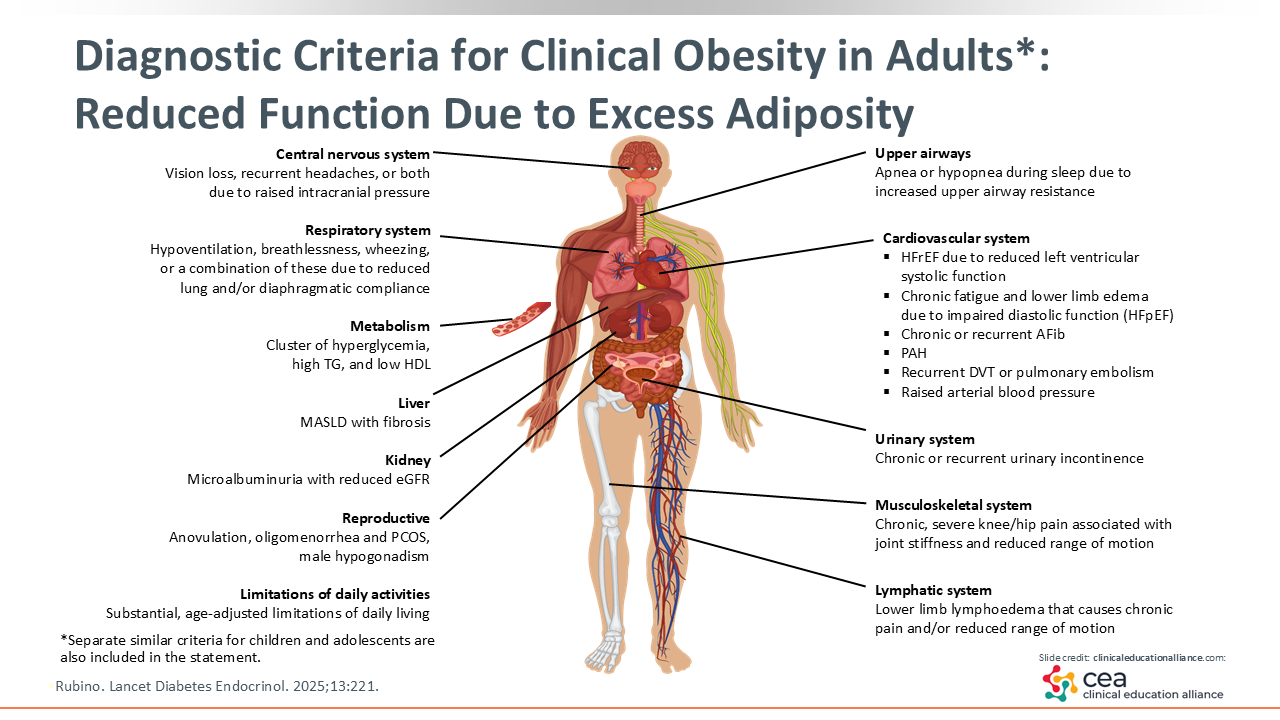
Diagnostic Criteria for Clinical Obesity in Adults: Reduced Function due to Excess Adiposity
It is well known that excess adiposity affect almost every organ system in the body.3 There are many diseases that are either directly linked, as a result of excess adiposity, or are complicated by obesity. This illustrates just how complex this disease is and why HCPs must dig deep into the comorbidities and complications that patients may present with.
One of my colleagues said, “It is like we, as HCPs, are in little silos—cardiology, nephrology, primary care, endocrinology, gastroenterology. We are constantly trimming the branches of the tree that pertain to our specialty and addressing heart failure and heart disease, dyslipidemia, liver disease, and OSA—you name it. If we would get ourselves out of the trees, onto the ground, and looking at the trunk of the trees, we would see that obesity is the cause that leads to all of these other diseases and complications that we are addressing. I encourage you to get out of the trees onto the ground [and] look at your patient holistically as to what excess adiposity can actually cause in our patients.”
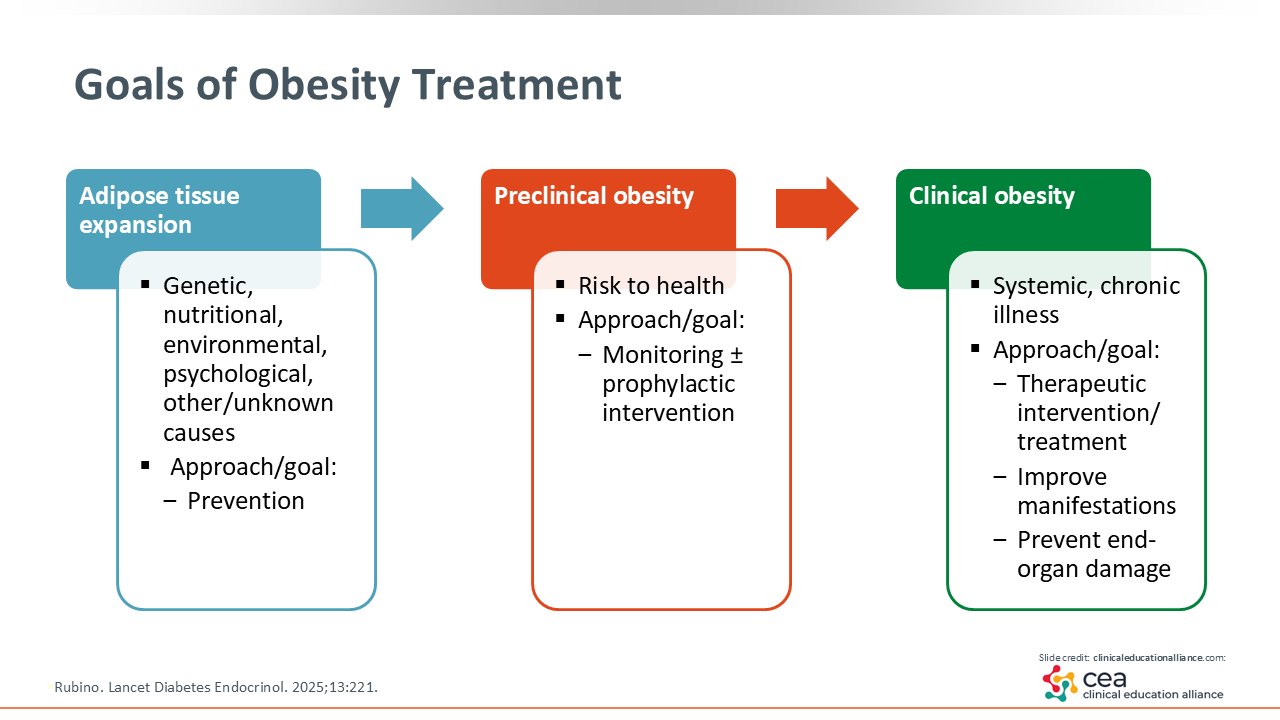
Goals of Obesity Treatment
The goals of obesity treatment are to identify where the excess adiposity is distributed in the body; that is critical. For example, women tend to carry their adipose tissue below the waistline. Although that comes with an increased risk of obesity because of metabolic derangements, fat distribution can cause changes to occur more so in the midsection as women age and experience hormonal shifts. We used to identify body shape by using specific fruit names: the apple shape for men and pear shape women.6 Again, it is where in the body the excess adiposity is located that matters. That is going inform treatment and the need for aggressive management.
There are many different causes for developing preclinical or clinical obesity. There are genetic causes, as unfortunately many genes have been identified. Furthermore, it is difficult to pinpoint a specific antiobesity treatment based on a genetic risk factor. We, of course, know that there are environmental factors at play. Then there are psychological and emotional components that consider what happens in the brains of patients with overweight or obesity and what drives the forces of this adipose tissue and where it is distributed in the body. The goal here is to identify those who are at risk and prevent progression at the earliest stage possible.
Per the Lancet Diabetes & Endocrinology article, preclinical obesity is a risk to patients’ overall health. Therefore, the goal is to start monitoring patients. We also need additional studies to find out what exactly else is going on in the body. Then HCPs may need to intervene in some way to prevent progression to clinical obesity, where patients would have systemic and potentially chronic illness. At this point, HCPs should work with patients to reduce their excess weight and aggressively manage any present comorbidities or complications to prevent severe outcomes like mobility restrictions that interfere with quality of life as well as increase the risk of morbidity and mortality.3
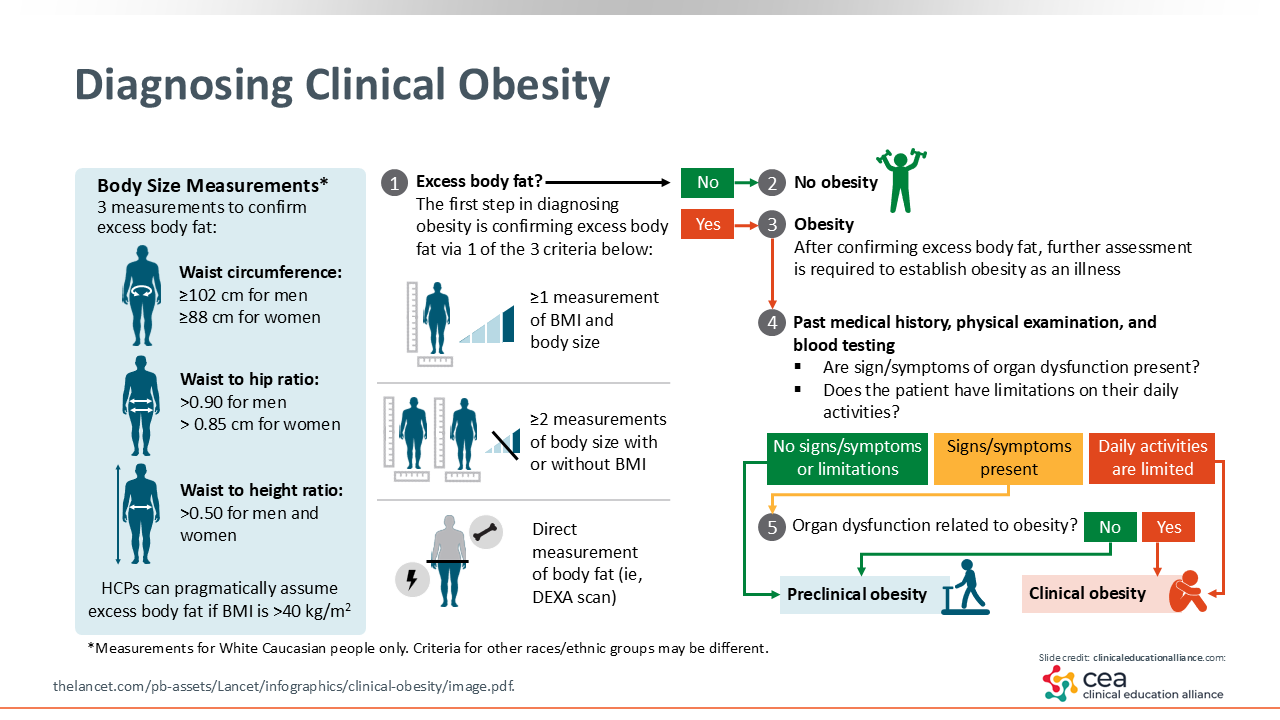
Diagnosing Clinical Obesity
The commission for the Lancet Diabetes & Endocrinology identified better ways to assess body fat, either through direct body fat measurement like a DXA scan, bioimpedance device, or MRI or by using at least 2 anthropometric measurements, such as waist-to-hip ratio, waist-to-height ratio, and waist circumference, regardless of BMI. Are patients experiencing excess adiposity through those measurements? If the answer is “no,” then those patients do not appear to have clinical obesity.
Upon determining the presence of obesity using these measures, HCPs should then assess if and how the excess adiposity is affecting patients. HCPs must determine what else could be going on with patients who are impacted by obesity. Therefore, getting a more comprehensive past medical history, physical examination, and some additional blood testing can be done.3,7
The commission used this information to identify health initiatives and overcome misconceptions about obesity.
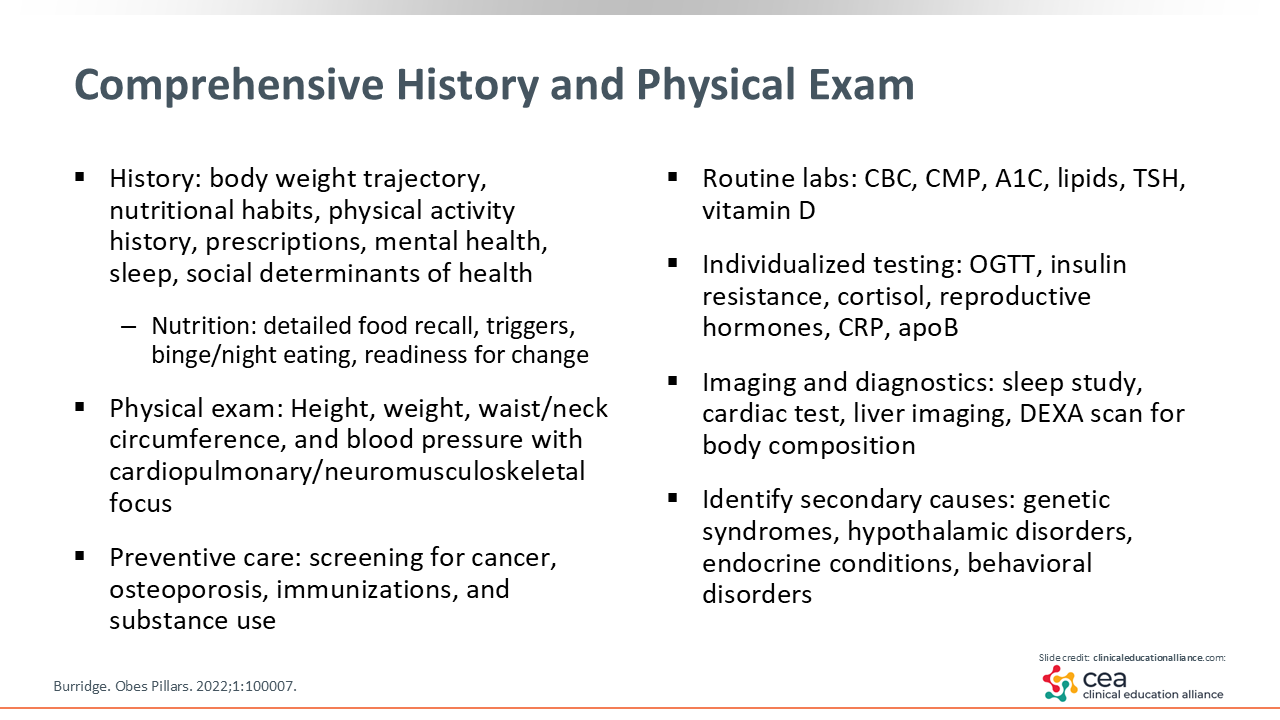
Comprehensive History and Physical Exam
Comprehensive past medical history and physical examination is where it all starts. Regarding past medical history, we want patients to provide us with as much information as possible. Some of the details listed on the slide are things that I ask patients to obtain for me before their initial appointment.
For body weight trajectory, the best way for patients to figure this out is to map it or graph it at certain times of their life. What was their initial lowest body weight and when did they start to notice changes? You might see a woman say, “Oh, when I started my cycle, I gained 10 lb. Then I went off to college and gained another 15 lb. I did Weight Watchers in my 20s and lost 15 lb.” How they map out their weight trajectory will give HCPs a lot of information.
I also have patients identify when changes in their medical status occurred and when certain medications (ie, antidepressants) were started. Were there changes in their sleep cycles? What other things were going on that can help me and the patient to identify what some causative agents might have been?
Nutrition is critical. Patients may tell you that they do not eat much. In fact, I find many of my patients are so caloric restrictive that this is a reason why they are not losing weight. Getting a detailed food recall is important. HCPs should help patients think about what and identify why they ate what they ate. How were they feeling? What were they expecting to gain after eating? How did they feel afterward? Those things are important to understand.
One of the most important pieces of information is understanding how ready patients are at this time in their lives to initiate the change that is going to be required for them to begin the journey of optimizing their weight and total body fat into a healthier position.
Other things that HCPs must do when seeing patients is, of course, to get their height and weight. We want that baseline BMI, even though it is not the greatest marker, because it helps us at least identify patients who are at increased risk. If their BMI is elevated, it informs HCPs to do some of the other measurements like waist circumference that are now recommended to confirm excess adiposity.
Neck circumference and blood pressure also are important measurements to track. In fact, a neck circumference of 16-17 inches or more increases one’s risk for OSA.8 Getting a blood pressure reading in the office may not be the most accurate way to determine if patients have hypertension. HCPs should know about white coat hypertension, so we want to make sure that patients are not exhibiting elevated blood pressure (≥130/80 mm Hg).9
Focusing on the cardiopulmonary musculoskeletal impacts of obesity, is excess adiposity causing problems with the patients’ knees, hips, and ankles? Are they experiencing exercise intolerance, an inability to lay flat when they sleep, or shortness of breath with mild activity? Those are the kind of things HCPs should be looking out for.
Of course, HCPs should screen for other related complications that can be prevented. For example, there are certain cancers that are related to obesity. Osteoporosis is a concern because of the excess adiposity and likely some issues with malnutrition and/or vitamin D. Are patients up to date on their immunizations? And then depression and stigmatization of obesity is so prevalent. Is there substance abuse or use that patients may have implemented to cope with what is going on with them?
Next are routine labs that HCPs should obtain, such as a complete blood count, comprehensive metabolic panel, liver and kidney status, fasting glucose, A1C, and lipids. Thyroid-stimulating hormone is typically done because people may think that they have overweight or obesity because their levels are high or because they have hypothyroidism. Unfortunately, it is usually the other way around; it is the overweight and obesity that contribute to hypothyroidism. But getting this measurement regardless is important. In addition, vitamin D is a fat-soluble vitamin. In people with excess adiposity, vitamin D is sequestered in the body fat tissue. Patients tend to have low levels regardless of their skin color.10 So measuring vitamin D can help HCPs address and ensure that patients do not develop secondary complications.
What are some other tests to consider? One that I typically order is a fasting insulin level with a fasting plasma glucose. With those 2 values, HCPs can determine patients’ homeostatic insulin-resistant calculation. For instance, a person has a fasting insulin of 13 µU/mL and a glucose of 94 mg/dL, which is not even prediabetes. When using a HOMA-IR calculator, which can found online, the patient’s insulin resistance ratio would be 3, and anything above 2 is considered insulin resistance.11 Fasting insulin levels can be critical in determining those who are at risk for developing diabetes and other related complications.
Furthermore, cortisol levels are important to measure, and probably the best way to assess this is with a dexamethasone suppression test. Then, of course, HCPs can measure patients’ reproductive hormones—testosterone, estrogen, and progesterone. C-reactive protein might be helpful, too. I tend to find that these levels are elevated because overweight and obesity is a disease of inflammation. I do not necessarily include that all the time, but I will go that extra step of getting the apolipoprotein B and the lipoprotein (a) markers when I am measuring lipids. This is because these biomarkers help risk stratify those with dyslipidemia.
In terms of imaging and diagnostics, the DXA scan will likely not be covered by health insurance. But we should send patients for sleep and cardiac studies, especially if they are having symptoms of orthopnea or exercise intolerance. Liver imaging is a questionable one. Patients with obesity probably will have elevated liver enzymes. The best thing to do in this situation is to order a Fibrosis-4 test, which screens for fibrosis. Positive results signify the need for another study to determine if patients are at risk for metabolic dysfunction–associated liver disease. That is when HCPs should refer patients to hepatology. Again, we want to identify these secondary causes and address them whenever possible.
Finally, HCPs must ensure that patients with any mental health issues have access to a clinical psychologist or therapist. That is going to be important in their overall health management.12
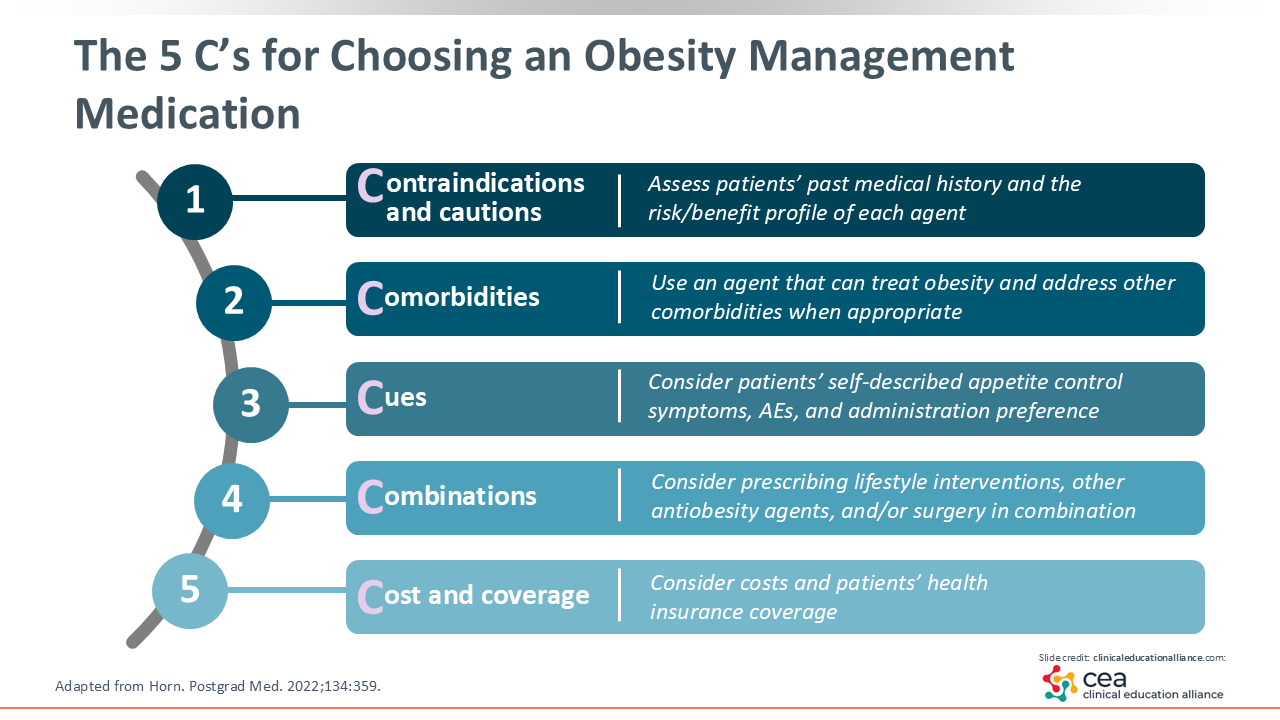
The 5 C’s for Choosing an Obesity Management Medication
When deciding on treatment, HCPs must think about contraindications and cautions. What else is going on with patients that would make the antiobesity medications (AOMs) we currently have available appropriate for them? Do they have underlying blood pressure issues? Do they have a history of anxiety? Or perhaps they maybe have an arrhythmia? Some of the available AOMs may not be appropriate treatments for certain patients.
What about comorbidities? When choosing an AOM, we want a medication that not only will induce weight loss, but also hopefully will address some of the other underlying conditions that the patient has. Are they having problems with their lipids? Are they presenting with prediabetes that might affect our choice of an AOM?
Regarding cues, what is causing patients to have an increased appetite? Is it mood (ie, boredom, sadness, anger) related? What is the trigger? HCPs can use this information to inform the choice of AOM, especially if an agent can help patients overcome these barriers.
As we already know, managing other chronic conditions like hypertension seldom takes one agent to adequately address it. Most of my patients with hypertension take at least 2 agents, if not more. The same is seen with type 2 diabetes; patients are taking at least 2 agents at a time. This can be true with managing obesity. In addition to lifestyle interventions and AOMs, HCPs might need to use more than one type of AOM, depending on the mechanism of action and/or the amount of weight patients need to lose to improve their overall health. Bariatric surgery can be done in addition to taking AOMs.
Then the last C stands for cost and coverage. We cannot do anything if it is out of reach for our patients. Does their health insurance cover what we are recommending? And even if they cover it, what is the out-of-pocket cost for the patient? Is it affordable and feasible? Can patients afford their recommended treatment if their health insurance does not cover it? There are many options that patients can access out of pocket. But again, it is going to depend on how much of it they can actually afford.13
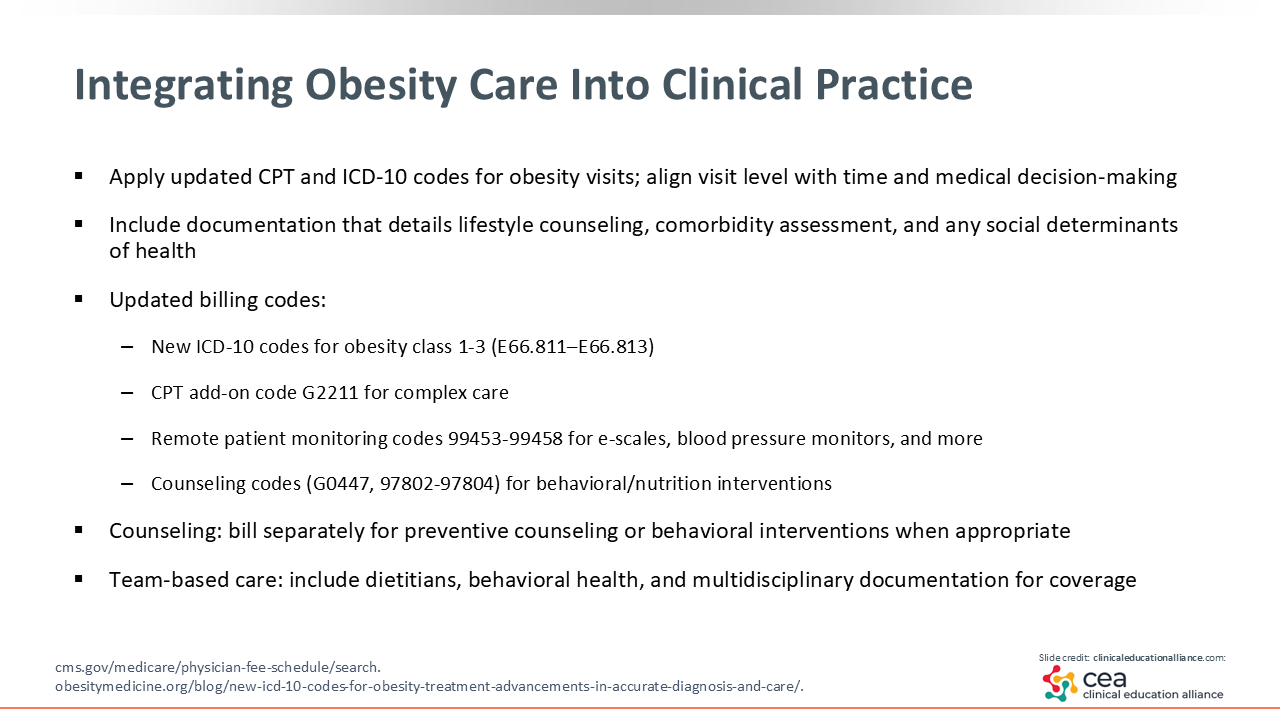
Integrating Obesity Care Into Clinical Practice
How do we integrate all of this into our clinical practice? This is probably where most of us struggle. HCPs should ensure that they are using the appropriate codes for reimbursement. We have updated ICD-10 codes that further classify obesity into classes. Class 1 (E66.811) comprises a BMI of 30.0-34.9 kg/m2; class 2 (E66.812) includes a BMI of 35.0-39.9 kg/m2; and class 3 (E66.813) encompasses a BMI of 40.0 kg/m2 and higher.14 These ICD-10 codes help us better identify and quantify patients’ level of obesity and HCPs need to use them.
There are some add-on codes that we can use, too. G2211 should be used for complex care; it is a specific code for Medicare. It does not require a specific type of HCP nor a specific intervention or visit. It suggests that outside of obesity or whatever you are seeing patients for, there are other things that are complicating the clinical decision-making. Whether or not it is covered by commercial insurers, that is currently undecided. Some health insurances will cover it, whereas others will not. That is something HCPs should double check with your commercial payers on.
Then there are remote patient monitoring codes that HCPs can use, especially if patients are sending data on their weight or blood pressure from their home. These are all Medicare codes (as shown on the slide), so HCPs should check with their commercial payers regarding the codes they use/require.
Finally, there are several counseling codes that can be used. G0447 actually describes face-to-face behavioral counseling for obesity, and 97802 through 97804 report 15-minute increments of nutritional interventions. Depending on how much time you are spending with the patient, that will determine how you bill for the visit.15
A note on nutritional interventions: Some codes rely on a registered dietitian to submit for payment and cannot be used as incident to. So HCPs should familiarize themselves with these codes. Talk with the commercial payers to understand what is covered by them and how to avoid a delay in reimbursement.
One would typically bill for preventive counseling separately, especially when seeing patients with obesity who are covered by Medicare. We cannot include any other discussion in that appointment when billing specifically for obesity.
Finally, obesity management is team based; you cannot do this all yourself. Some of these codes must be used by HCPs outside primary care. And we should want to use a team-based approach to ensure our patients get all of the support that they need.
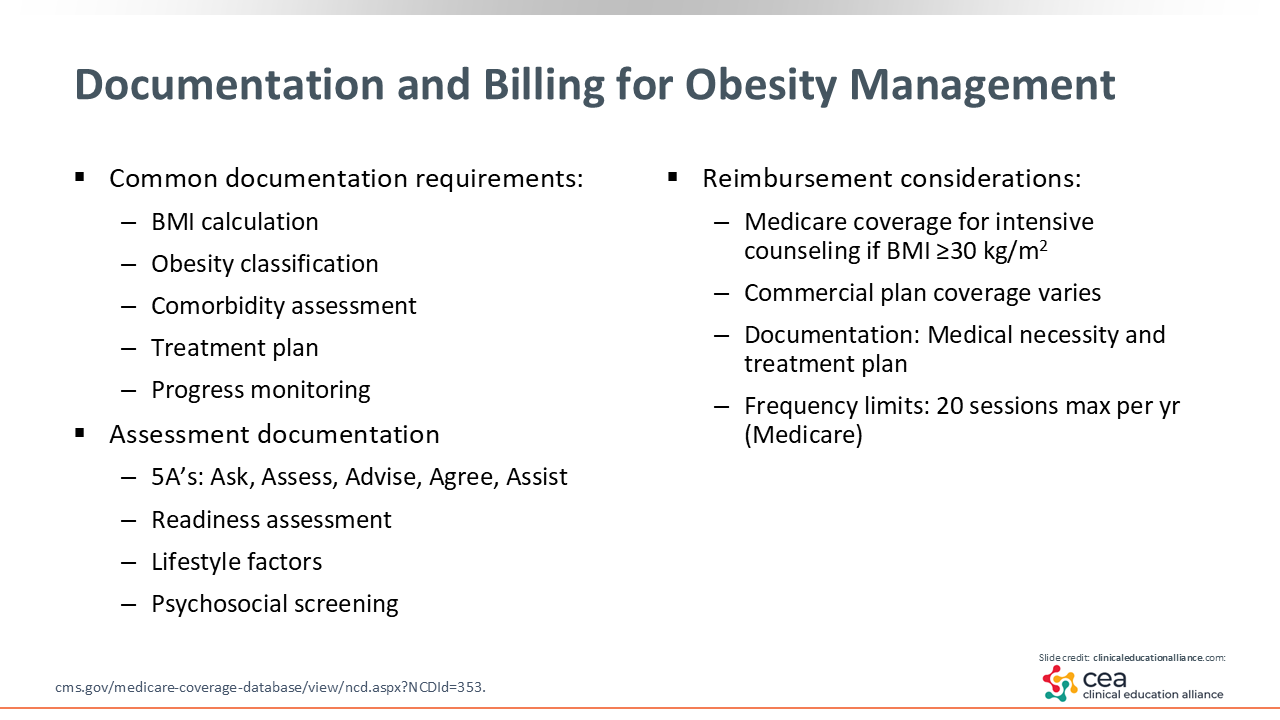
Documentation and Billing for Obesity Management
In terms of adequate documentation, ensure your note can support everything you do. If your medical charts are audited, insurance companies want to make sure that your documentation is supporting what you are charging. Ensure that you are identifying patients’ BMI and obesity classification. What is your assessment of the patient? What else is going on with them that complicates your treatment plan? How often are you going to be following up with the patient?
Specifically for Medicare, we must document the “5 A’s”: ask for permission, assess what is going on, advise patients about their treatment options, agree on a treatment plan, and assist them with follow-up as well as evaluating that plan. This includes assessing patients’ readiness, identifying the lifestyle modifications they have already tried, and screening for psychosocial concerns like depression and eating disorders.
When billing for obesity, Medicare also has certain parameters that HCPs must follow. You cannot have more than 20 sessions per year.16 In my practice, I personally bill for a 95214 or 15-minute visit; I base it on time because some of the reimbursement considerations can get into the weeds and you do not necessarily get the reimbursement that you were hoping for. But so long as your documentation supports what it is you are billing for, you will be fine.
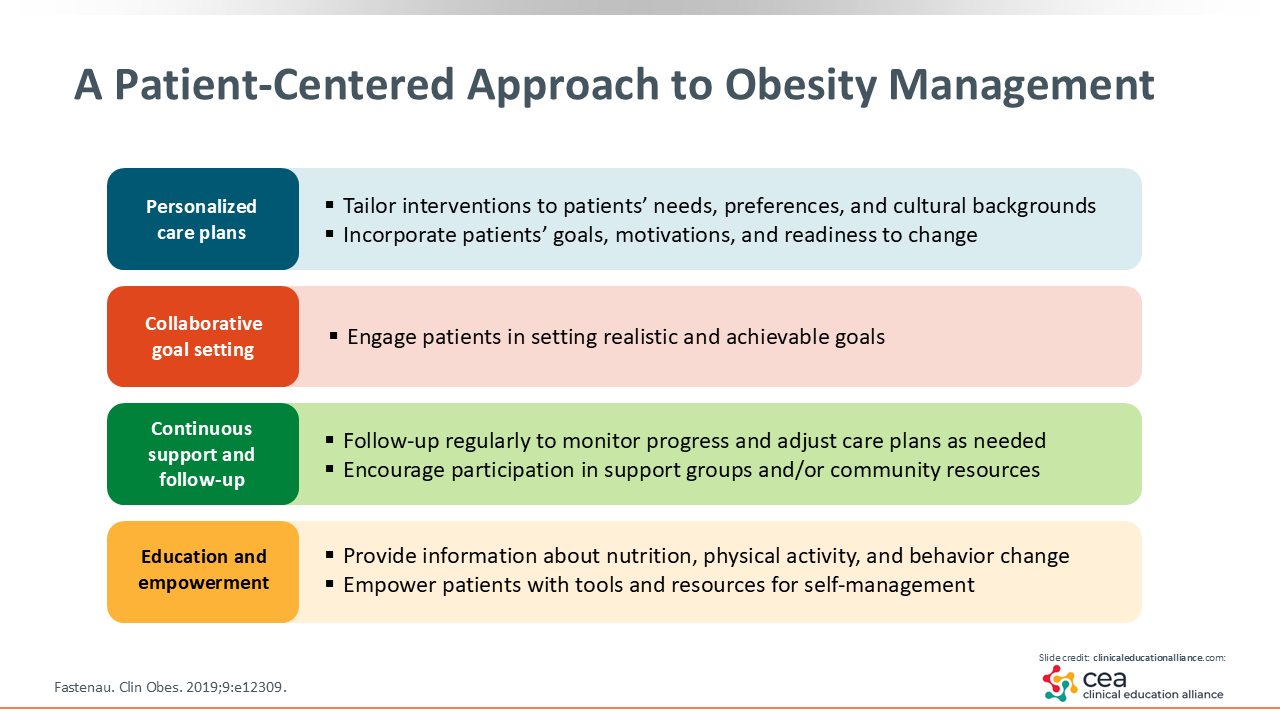
A Patient-Centered Approach to Obesity Management
Of course, patients must be at the center of all of this. We must understand what they believe overweight or obesity means to them. Patients may not care that they are dealing or contending with overweight or obesity because there are other things going on in their lives. Or they may not relate their disease of overweight or obesity as the common denominator for everything else that is going on with them.
HCPs must get patients involved in understanding their disease, helping us to identify what the barriers are, addressing these barriers to help them better manage, and referring to the right person to help identify some of those challenges if we cannot.
This also requires collaboration. What we think is important may not be what patients think is important. Perhaps they want to exercise but do not own a pair of walking shoes. We need to find out where they are and then set goals in small steps that are achievable. If their first goal is going to be to get a pair of walking shoes, then the next goal might be to put them on and next goal might be to walk in place for 5 minutes daily. That is what I mean by small steps. This way patients see that they can achieve these goals and move forward.
Once we have developed the treatment plan, HCPs should meet with patients on a regular basis to see how they are doing and make adjustments as needed. Here, HCPs can further encourage patients to get involved with whatever resources are available online or in their communities.
Finally, we must make sure that we provide patients with the resources and tools to achieve their goals. That includes us as HCPs. We must stay on top of what is important and what needs to be addressed in patients with overweight or obesity.17