
CE / CME
Improving Appetite, Lean Body Mass, or Physical Function in Patients With Cancer Cachexia
Physician Assistants/Physician Associates: 0.25 AAPA Category 1 CME credit
Pharmacists: 0.25 contact hour (0.025 CEUs)
Physicians: maximum of 0.25 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.25 Nursing contact hour
European Learners: 0.25 EBAC® CE Credit
Released: March 20, 2026
Expiration: September 19, 2026

Activity
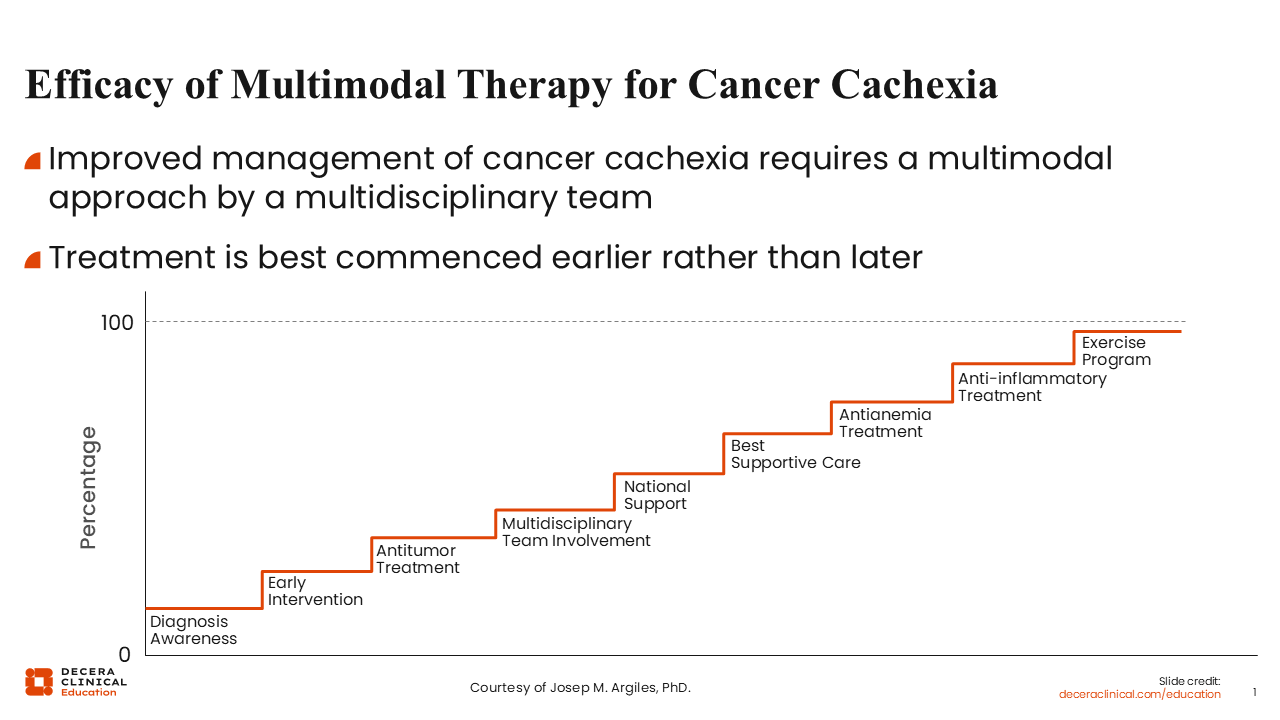
Efficacy of Multimodal Therapy for Cancer Cachexia
Cancer cachexia is a complex, multifactorial syndrome characterized by involuntary weight loss, reduced skeletal muscle mass, decreased appetite, and impaired physical function.1,2
The goal of optimizing the care of patients with cancer and cachexia should include a multimodal treatment approach at the initial onset of the syndrome. Steps involved in the multimodal treatment of cancer cachexia include early recognition of signs and symptoms, which should be promptly followed by early diagnosis of cachexia. Once the patient is diagnosed, early initiation of treatment for cachexia is needed along with the continuation of anticancer therapy. The involvement of a multidisciplinary team of investigators is important as well as institutional support, incorporation of best supportive care, and appropriate symptom management.
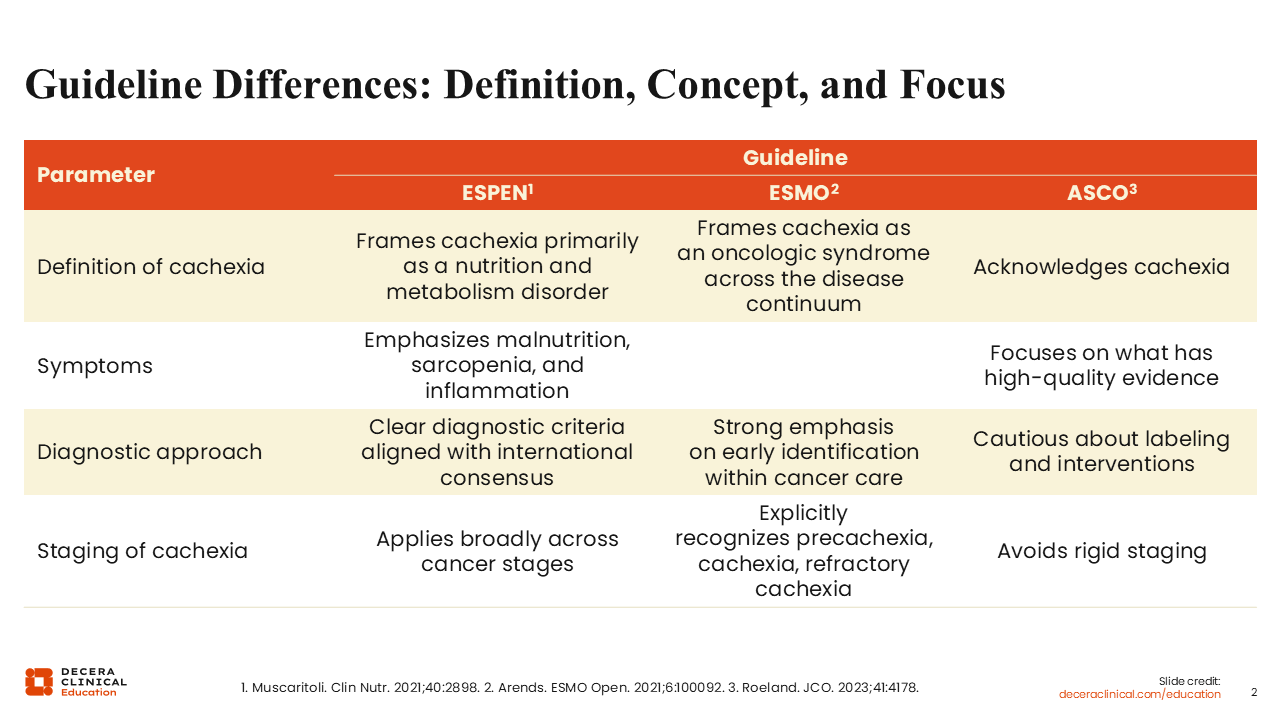
Guideline Differences: Definition, Concept, and Focus
European Society for Clinical Nutrition and Metabolism (ESPEN), European Society for Medical Oncology (ESMO), and the American Society of Clinical Oncology (ASCO) provide evidence-based guidelines for the standardization of care for patients with cancer. Regarding cancer cachexia, these societies differ in definition, symptoms, diagnostic approach, and staging of the syndrome. For instance, the ESPEN guidelines emphasize malnutrition, sarcopenia, and inflammation as key symptoms.3 The ESMO guidelines require at least 2 symptoms from the list including malnutrition, at least 1 phenotypic criterion (weight loss, BMI value, or low muscle mass), and increased acute or chronic systematic inflammation.4 The ASCO guidelines focus on symptoms with high-quality evidence, noting that insufficient protein and calorie intake are common among patients with cancer cachexia.5
In addition, although the ESMO guidelines clearly recognize 3 stages of cachexia (precachexia, cachexia, and refractory cachexia), staging using ESPEN and/or ASCO guidelines is broad and less rigid.3-5 These differences highlight some of the challenges faced by healthcare professionals (HCPs) in recognizing, staging, and treating cancer cachexia and underscore the complexities in the management of patients with cancer cachexia.
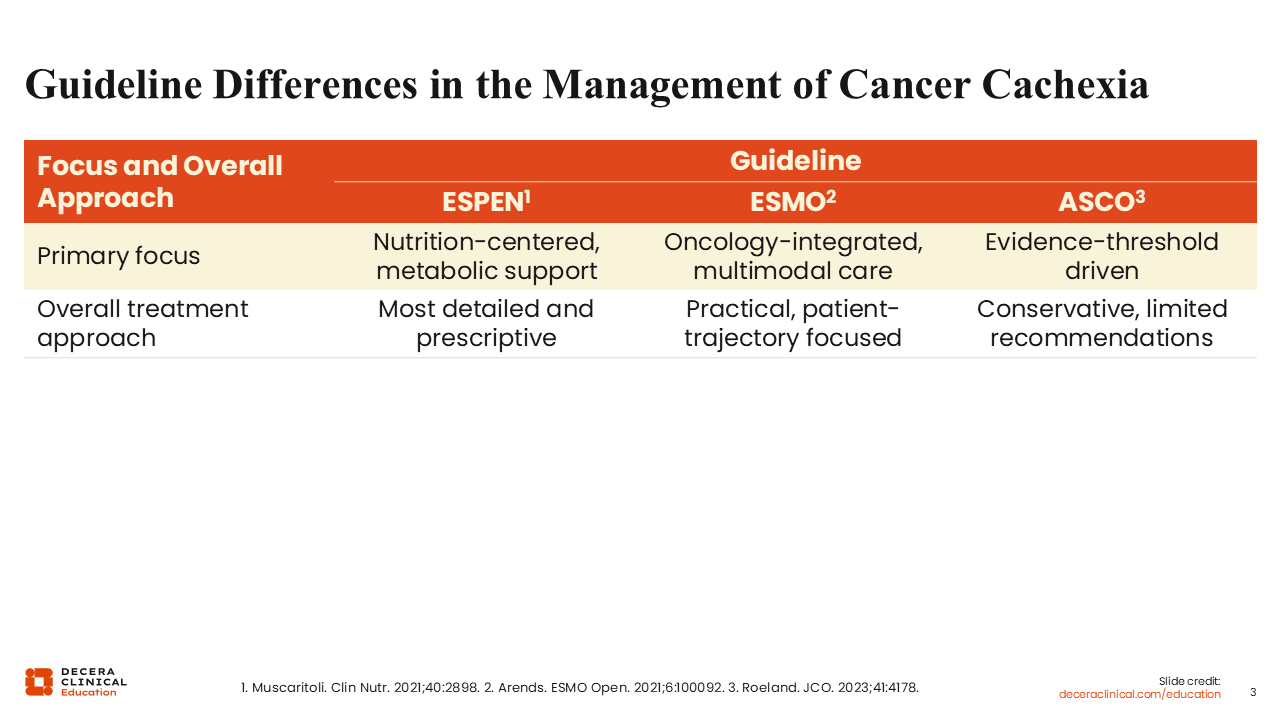
Guideline Differences in the Management of Cancer Cachexia
The guidelines for the management of cancer cachexia also differ. The ESPEN guidelines are centered on nutrition and metabolic support; the ESMO guidelines recommend an oncology-integrated multimodal care model that includes nutritional support, exercise/training, and symptom management; and the ASCO guidelines are evidence driven. Per the ASCO guidelines, HCPs may decide not to offer medications for the treatment of cancer cachexia because evidence is still insufficient to strongly endorse any pharmacologic agent to improve outcomes.5
Among these 3 professional bodies, ESPEN offers the most detailed and prescriptive guidelines for the treatment of cancer cachexia.3 The ESMO guidelines are more practical with a focus on the disease course of the individual patient, whereas the ASCO guidelines are on the conservative side with limited recommendations about the choice of pharmacologic agents.4,5
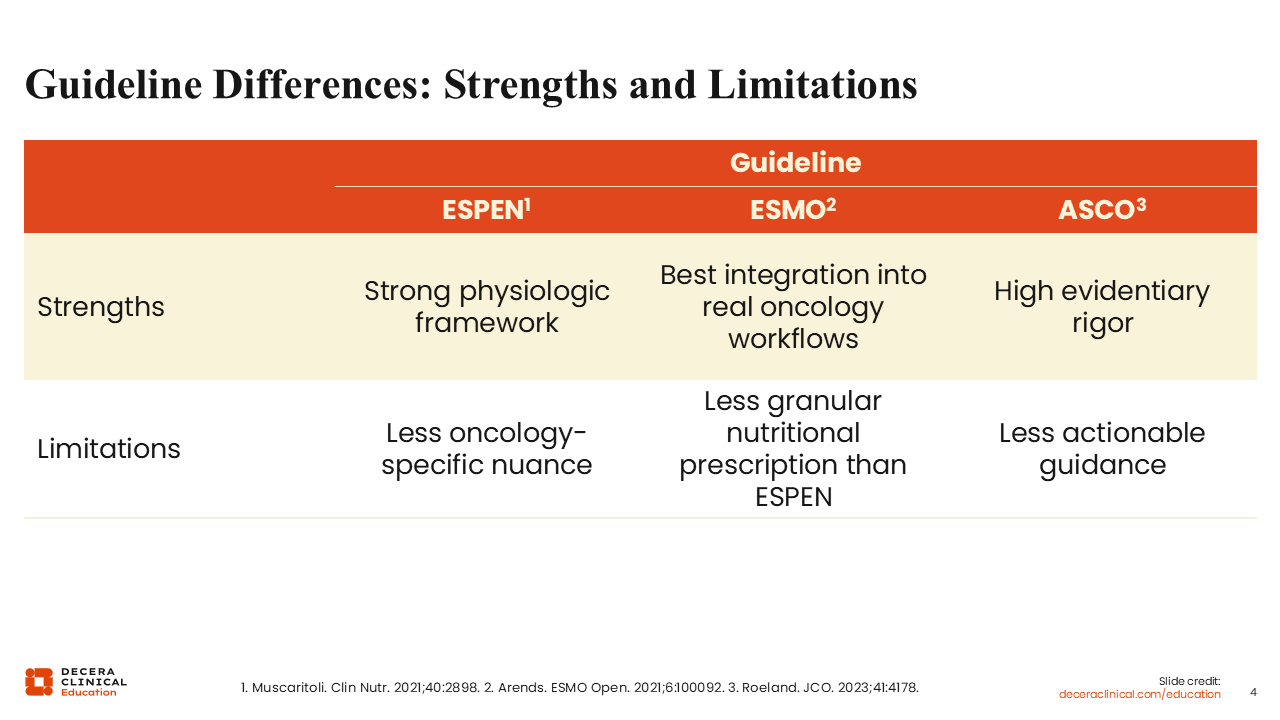
Guideline Differences: Strengths and Limitations
The framework for each of these guidelines has strengths and limitations. In general, the ESPEN guidelines have a strong physiologic framework with less oncology-specific nuance.3 The ESMO guidelines more carefully integrate the diagnosis and treatment of cancer cachexia into real oncology workflows.4 By so doing, however, the ESMO guidelines seem to provide less granular nutritional prescriptions compared with the ESPEN guidelines. As previously highlighted, the ASCO guidelines are focused on rigorous and proven evidence, thereby providing less actionable guidance for treating HCPs.5
Nutritional Interventions: Guideline Differences
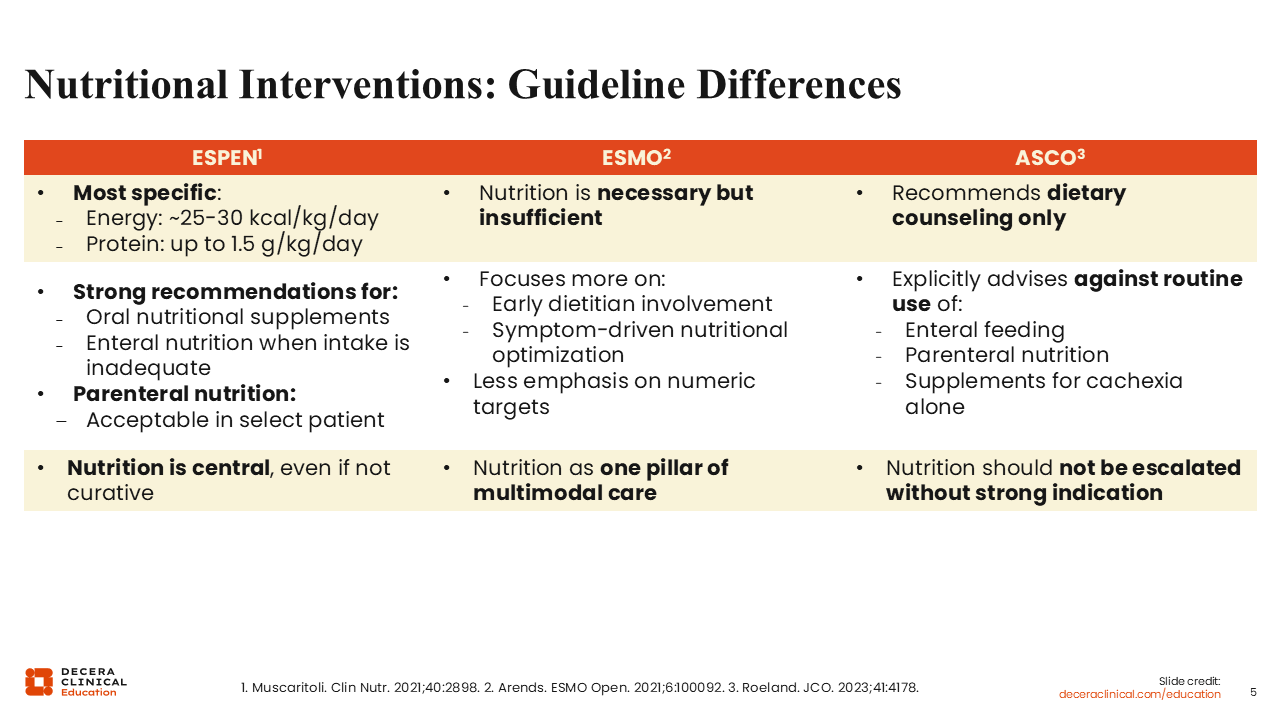
In the management of patients with cancer cachexia, these 3 professional bodies acknowledge a role for nutritional intervention but in different capacities.3-5 The ESPEN guidelines recognize nutritional intervention as central.3 Among the 3 bodies, the ESPEN guidelines are the most detailed and provide specific recommendations regarding daily calorie (~25-30 kcal/kg/day) and protein (up to 1.5 g/kg/day) intake. ESPEN also has a recommendation for the use of additional oral and/or enteral nutritional supplements when food intake is not sufficient.
On the other hand, the ESMO guidelines note that although nutritional intervention is necessary, by itself, it is not sufficient.4 The ESMO guidelines recognize nutritional intervention as 1 pillar of a multimodal treatment approach for patients with cancer cachexia. ESMO focuses more on the involvement of a dietitian at the onset of cachexia with less emphasis on food intake with numeric specifications compared with the ESPEN and ASCO guidelines.3-5
In contrast to the ESPEN and ESMO guidelines, ASCO recommends dietary counseling only and clearly advises against the routine use of enteral feeding, parenteral nutrition, and/or oral supplements in the management of cachexia. Being more evidence based, the ASCO guidelines do not recommend the escalation of nutritional intervention unless there is a strong indication for it.5
Despite these differences, all 3 professional bodies have consistent cautionary notes regarding the management of patients with cancer cachexia. Force feeding and the aggressive use of artificial nutrition in end-of-life settings should be avoided. The use of unproven supplements as sole therapy is not recommended. Similarly, all 3 bodies recognize the importance of early intervention as opposed to delaying treatment of cancer cachexia because it is clear that early intervention is critical to achieve positive outcomes.
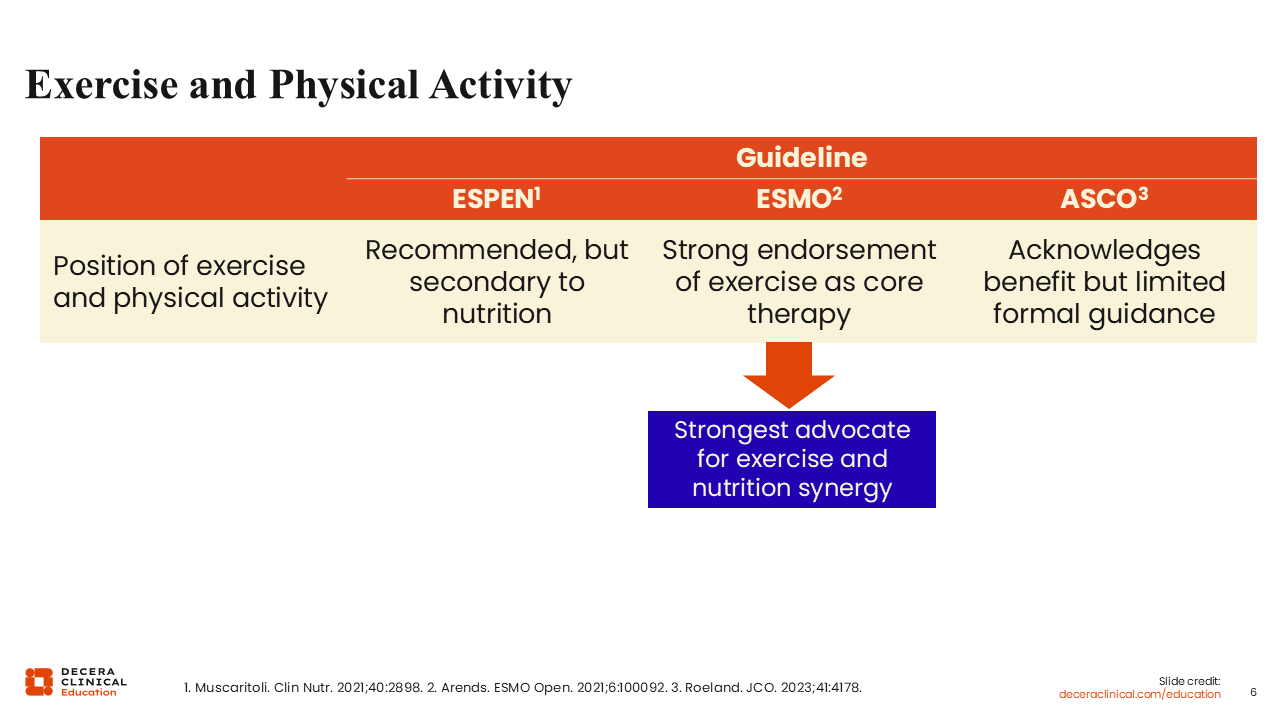
Exercise and Physical Activity
There are differences in the recommendations for the use of exercise and physical activity in the care of patients with cancer cachexia.3-5 Of note, ESMO is the strongest advocate for the use of exercise and physical activity incorporated into the multimodal treatment of patients with cancer cachexia.4 The ESPEN guidelines have an order of preference and positions nutritional intervention above the use of exercise and physical activity.3 Although ASCO acknowledges that exercise and physical activity play a role in the treatment of patients with cancer cachexia, it provides limited formal guidance on how to incorporate exercise and physical activity into patient care.5
Pharmacologic Therapy
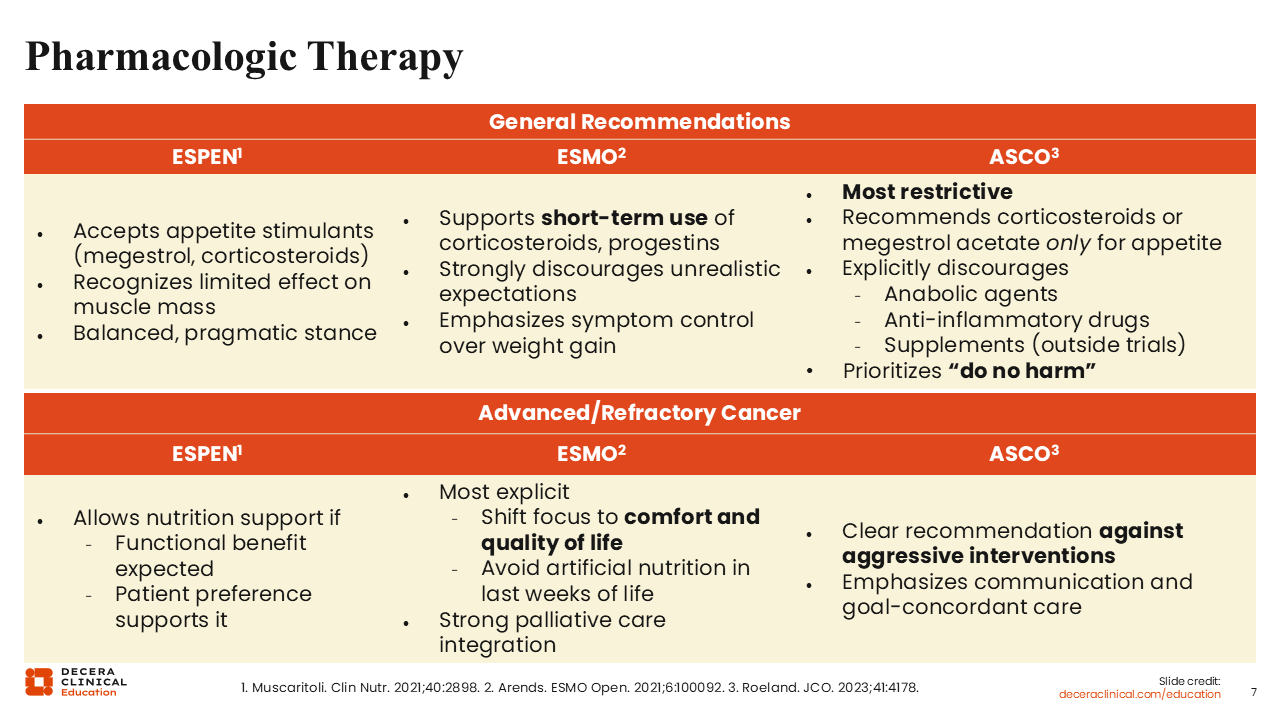
Aside from the use of nutritional intervention and/or functional performance, it is recognized that pharmacologic intervention plays a role in the management of patients with cancer cachexia, at least in some scenarios. In general, the ESPEN guidelines allow for the use of appetite stimulants, such as megestrol acetate and corticosteroids, and recognize that these agents exert limited effects on improving muscle mass for patients with cachexia.3 The ESMO guidelines support the use of steroidal therapy in the short term, with an emphasis on overall symptom control vs a focus on weight gain only.4
The ASCO guidelines are the most restrictive, with recommendations for the use of corticosteroids and megestrol acetate only for appetite stimulation.5 The ASCO guidelines strongly discourage the use of nonsteroidal anti-inflammatory drugs or the use of anabolic steroids such as oxandrolone or nandrolone, selective androgen receptor modulators such as enobosarm, or ghrelin agonists such as anamorelin for appetite stimulation. Even the use of supplements outside of a protocol setting is discouraged in the ASCO guidelines.
In the end-of-life setting, the ESPEN guidelines allow nutritional support if benefit is anticipated and if the patient prefers this support. The ESMO guidelines primarily focus on the patient’s comfort and quality of life in this setting. By contrast, the ASCO guidelines do not support the use of any form of aggressive intervention, with more emphasis placed on communication with the patient and caregiver(s) to provide treatment goal-concordant care.
Japanese Society for Palliative Medicine Guidelines
ESPEN and ESMO are professional bodies in Europe and ASCO is a professional body in the United States of America. Currently, no disease‑modifying pharmacologic agent is approved by the FDA or the European Medicines Agency (EMA) specifically for the treatment of cancer cachexia. However, in Japan, anamorelin, an oral selective agonist of the ghrelin receptor, is approved for patients with cancer cachexia.6
In Japan, there is no standalone guideline for the treatment of patients with cancer cachexia.7 Rather, the Japanese Society for Palliative Medicine (JSPM) guidelines have a focus on the symptoms and supportive care for patients with advanced cancers. The JSPM guidelines include recommendations for cancer pain management, palliative sedation therapy, gastrointestinal symptom management, respiratory symptom management, guidelines for infusion therapy, management of urologic symptoms, and evidence-based summaries of complementary and alternative therapies for patients with advanced-stage cancer.
Cancer Cachexia Guidelines in Real-life Practice
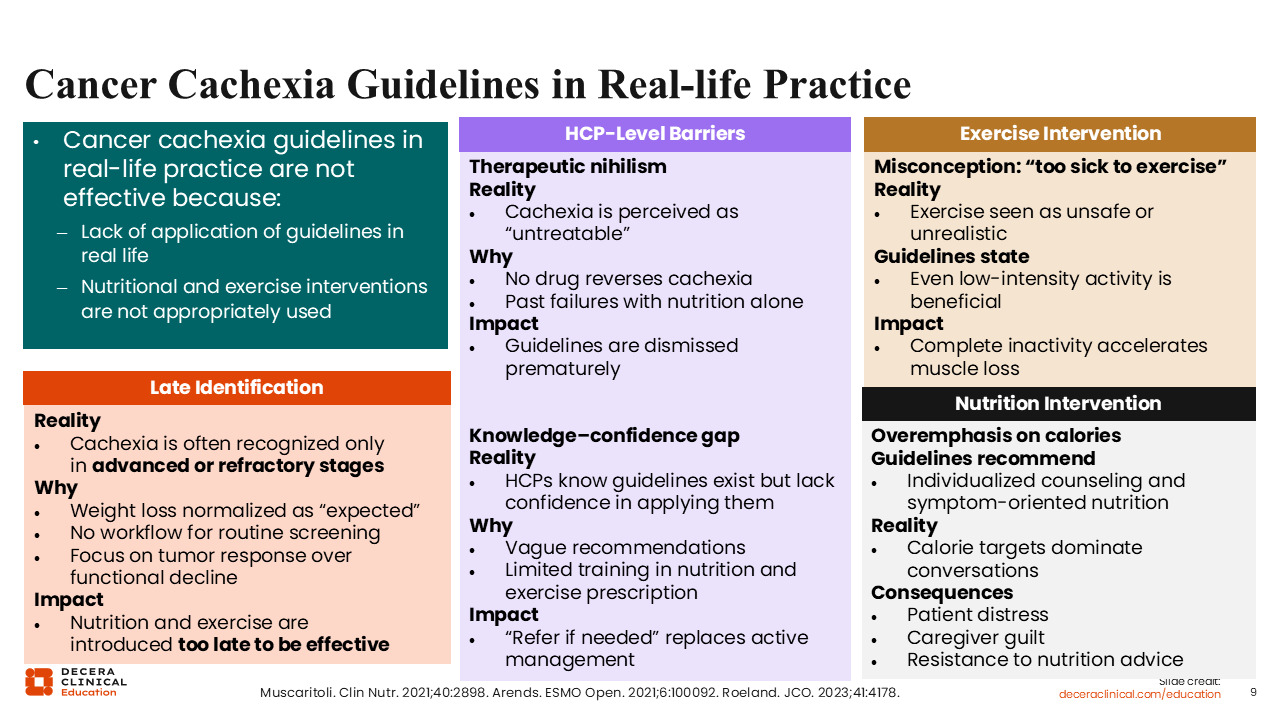
In real-world clinical practice, these guidelines and recommendations are not effective in the management of cancer cachexia for multiple reasons.3-5 In our world today, cachexia is still underrecognized and underdiagnosed. In many cases, it is diagnosed when it is in the advanced or refractory stage. Since there are different guidelines with varying and likely confusing recommendations, it is challenging for HCPs to apply these guidelines in the real world. In addition, the different guidelines are nonstandardized, and HCPs have limited training in when and how to prescribe nutrition and/or exercise for patients with cancer cachexia.
The reality is that the signs and symptoms of cachexia, such as unintentional weight loss, can easily be normalized as expected symptoms for patients with advanced cancer receiving anticancer therapy. Of note, some HCPs still perceive cachexia as an “untreatable” condition. If the syndrome is mostly identified in its late or advanced stage, the effectiveness of interventions, such as nutritional support and exercise, becomes significantly diminished.
Even though most HCPs are aware that guidelines such as ESPEN, ESMO, and ASCO exist for the management of cancer cachexia, there is a lack of confidence in how to appropriately apply these recommendations, especially when the guidelines are vague and overly broad. A major huddle in Europe and the United States is the lack of any pharmacologic agent with FDA or EMA approval for cancer cachexia. Without sufficient training on how to provide an individualized and multimodal treatment approach for all patients with cancer cachexia, with particular emphasis on early-onset diagnosis, the successful application of these guidelines will remain abysmal.
Nutritional Support in Patients Receiving Chemotherapy Practices and Views of Oncologists
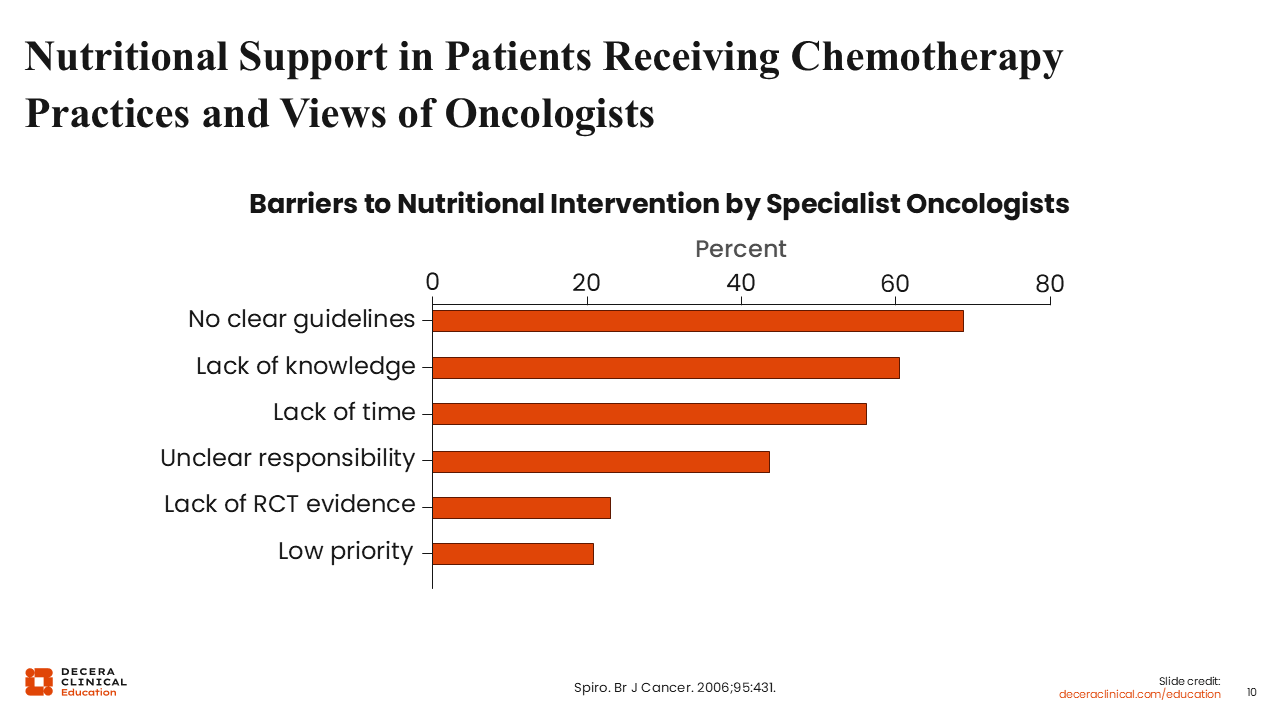
A survey using questionnaires was conducted to determine the views and practices of oncologists in the United Kingdom regarding nutritional support for patients with cancer receiving chemotherapy.8 The aims of the survey were to understand the extent to which oncologists are able to identify malnutrition, to provide an understanding of the importance oncologists place on nutrition as a variable in patient care and treatment outcome, and to identify the barriers faced in the decision to incorporate nutritional support into treatment.
Among approximately 350 responses, >60% noted the lack of clear guidelines and approximately 60% indicated the lack of knowledge as the primary hurdle. Other reasons affecting the use of nutritional support included the lack of time, lack of clarity on whom in the healthcare team this responsibility lies with, and the lack of evidence from randomized, controlled trials. In approximately 20% of the responses, the use of nutritional intervention was low on the order of priority.
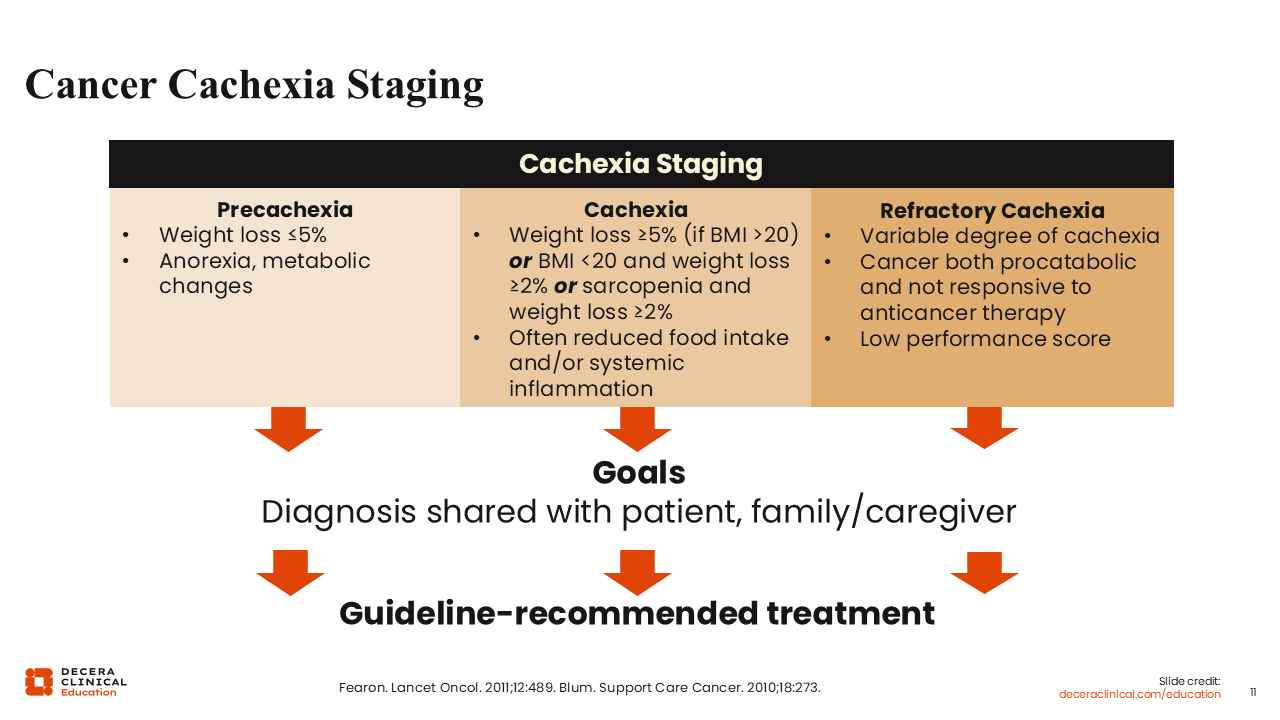
Cancer Cachexia Staging
Cancer cachexia progresses along a clinical continuum of 3 stages: precachexia, cachexia, and refractory cachexia.1,9-12 It is important to reiterate that early identification in the precachexia stage is particularly crucial for a timely intervention, as this will lead to improvements in patient outcomes and is associated with a high potential to prevent progression to more advanced stages of cachexia. It is also important that the HCPs discuss the diagnosis and guideline-recommended treatment options with the patient and caregiver(s).
Multidisciplinary and Multimodal Management of Cancer Cachexia
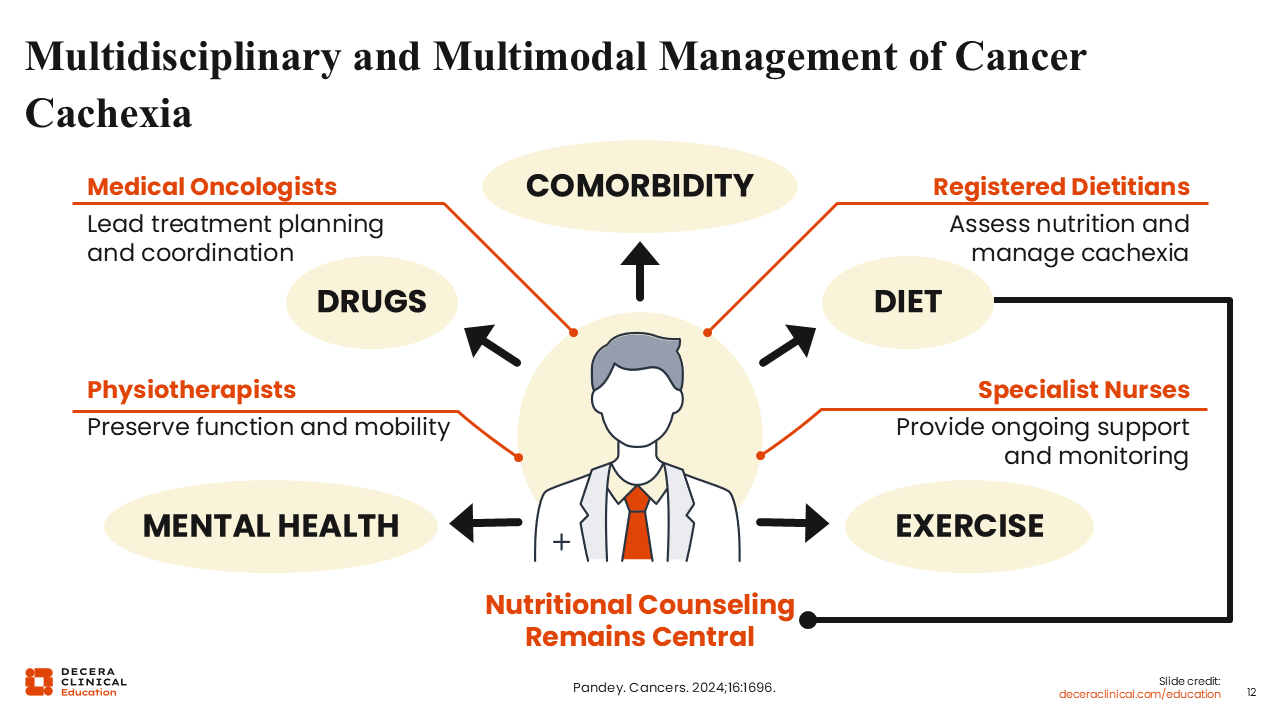
To achieve optimal and effective treatment outcomes, management of patients with cancer cachexia requires collaboration among a multidisciplinary care team of experts including medical oncologists, dietitians, specialist nurses, and physiotherapists.13 This multimodal and multidisciplinary approach will ensure that the patient receives appropriate pharmacologic treatment, as indicated, with patient-centric consideration for preexisting comorbidities and concomitant medications. Also, this approach takes the dietary, mental, emotional, and physical health into full consideration on an individualized basis and ensures the overall well-being of the patient.
Of importance, nutritional counseling remains a central aspect in the management of patients with cancer cachexia.
Nutritional Counseling Remains Central
Pertaining to nutritional counseling, a high protein intake of ≥1.2-1.5 g/kg/day in combination with omega-3 fatty acid supplementation (eicosapentaenoic acid/docosahexaenoic acid) to modulate inflammation and support anabolism is recommended for patients with cancer cachexia.14-16 As previously stated, it is important for nutritional intervention to be integrated with the use of exercise therapy and pharmacologic support as needed on a patient-specific basis. It is particularly exciting that there are multiple ongoing clinical trials investigating novel strategies and multimodal approaches for the treatment of patients with cancer cachexia (BENITA, EMC2APA, MOONRISE, 220582, C-SPCC-1, 213/18, 2022-223-02).
Overall Conclusions
In conclusion, it is important to utilize patient and caregiver empowerment strategies to achieve optimal treatment outcomes.17-19 Patient and caregiver education on the signs and symptoms of cancer cachexia is crucial. HCPs need to proactively explain to patients and their caregivers that cachexia is a cancer-related metabolic syndrome that is treatable and a syndrome that is not caused by a lack of effort or love. Patients and their caregivers need to know that minimal or reduced food intake is an aspect of the syndrome that will not be resolved by force feeding.
The provision of emotional support for patients with cancer cachexia is also important. Setting functional goals, such as maintaining energy levels for meaningful activities, may provide more relevant markers of success than weight management alone.
Overall, cancer cachexia is a treatable multifactorial syndrome that requires early recognition, early diagnosis, and immediate use of appropriate interventions designed to fit an individual patient’s specific condition. To achieve optimal patient outcomes, the treatment of cancer cachexia should not be a one-size-fits-all approach.