
CE
SC ICI Delivery Strategies: Practical Considerations for SC Immunotherapies
Pharmacists: 0.50 contact hour (0.05 CEUs)
Released: July 09, 2026
Expiration: January 08, 2027


Activity
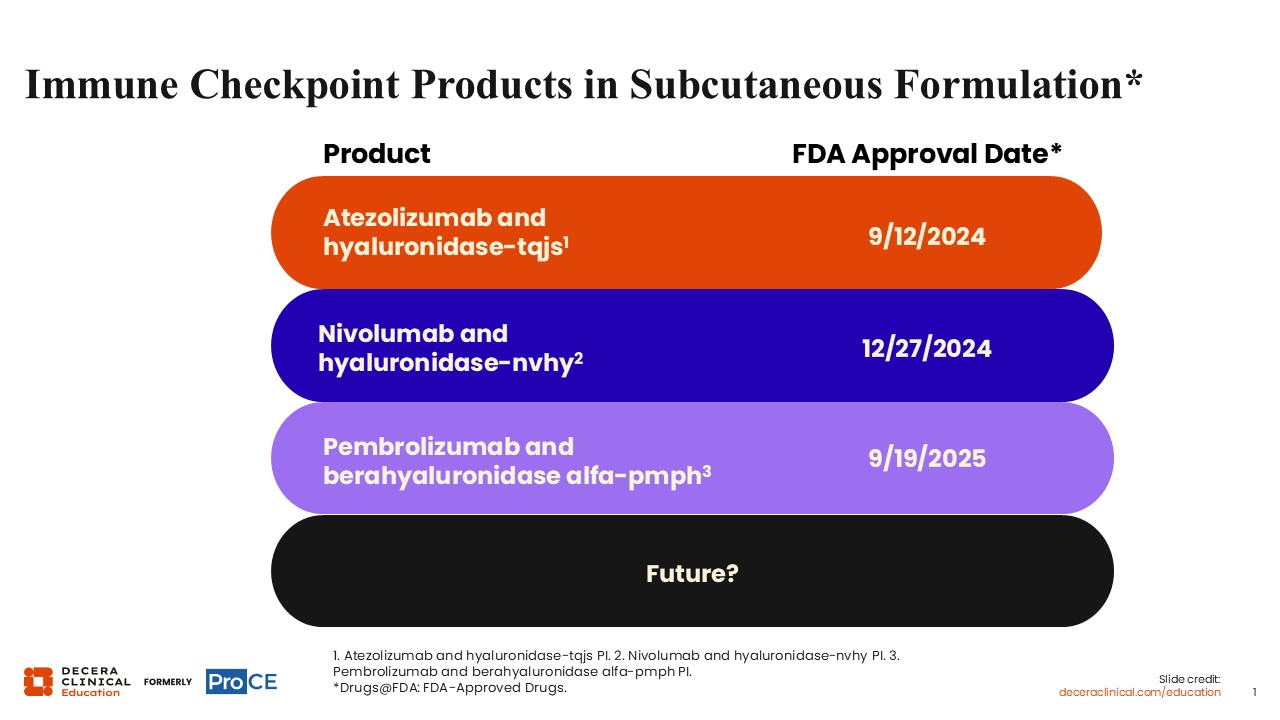
Immune Checkpoint Inhibitors in Subcutaneous Formulation
Kelly Romo, PharmD, BCOP:
A recent development in the care of patients with solid tumors using immunotherapy was the FDA approval of 3 SC ICI formulations, including atezolizumab and hyaluronidase-tqjs on September 12, 20241,2; nivolumab and hyaluronidase-nvhy on December 27, 20243,4; and pembrolizumab and berahyaluronidase alfa-pmph on September 19, 2025.5,6 But there is also potential for additional SC products in the future.
Other Considerations for SC ICI Administration
Kelly Romo, PharmD, BCOP:
IV Formulations
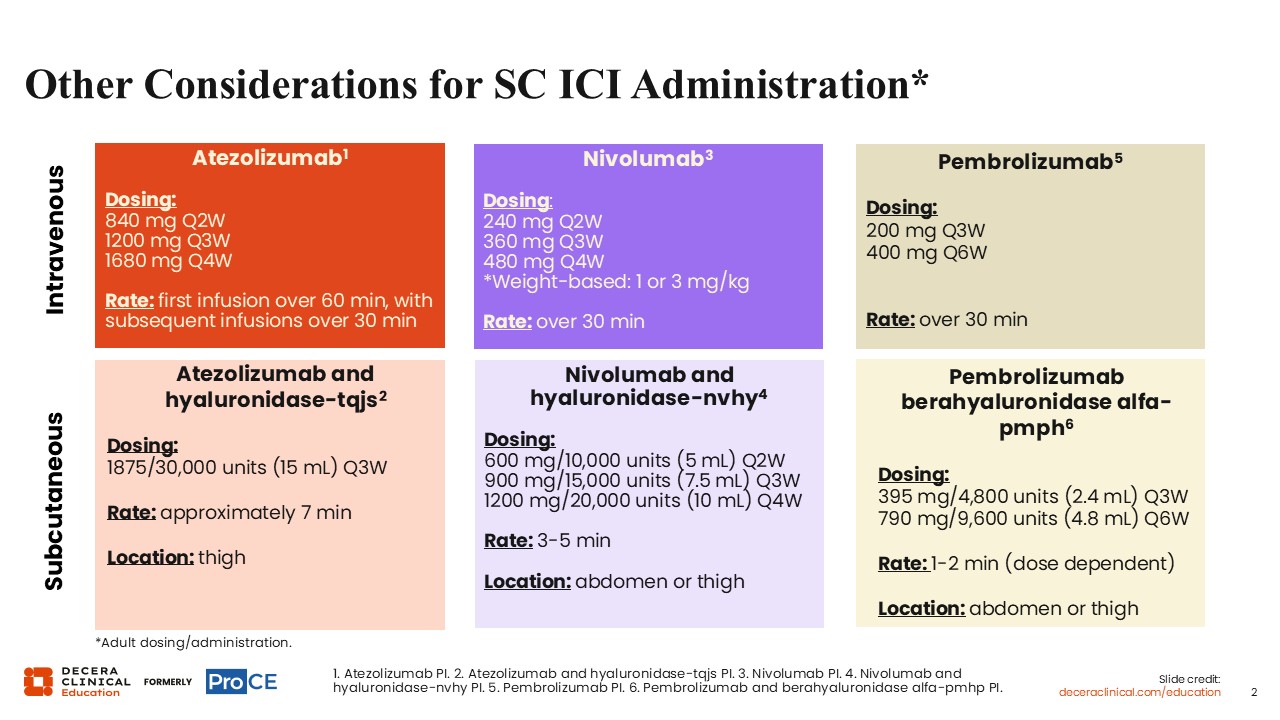
IV ICI formulations differ by product, dose schedule, and administration time. Atezolizumab may be administered as 840 mg every 2 weeks (Q2W), 1200 mg every 3 weeks (Q3W), or 1680 mg every 4 weeks (Q4W) IV infusion, with the first infusion given over 60 minutes and subsequent infusions over 30 minutes.1
Nivolumab IV dosing varies by indication and regimen and may include fixed-dose schedules of 240 mg Q2W, 360 mg Q3W, or 480 mg Q4W, as well as weight-based dosing in specific labeled settings, including selected ipilimumab-containing regimens and certain pediatric patients weighing <40 kg.3
Pembrolizumab may be administered as 200 mg Q3W or 400 mg Q6W IV infusion over 30 minutes.5
Subcutaneous Formulations
SC ICI formulations use hyaluronidase-containing products and have numerically shorter administration times. Atezolizumab and hyaluronidase-tqjs is administered as a 1875 mg/30,000 units in 15 mL Q3W SC injection, with administration in the thigh over approximately 7 minutes.2 Nivolumab and hyaluronidase-nvhy is administered as a 600 mg/10,000 units in 5 mL Q2W, 900 mg/15,000 units in 7.5 mL Q3W, or 1200 mg/20,000 units in 10 mL Q4W SC injection, with administration in the abdomen or thigh over 3-5 minutes.4 Pembrolizumab and berahyaluronidase alfa-pmph is administered as a 395 mg/4800 units in 2.4 mL Q3W or 790 mg/9600 units in 4.8 mL Q6W SC injection, with dose-dependent administration in the abdomen or thigh over 1-2 minutes.6
IV and SC ICI Administration
Kelly Romo, PharmD, BCOP:
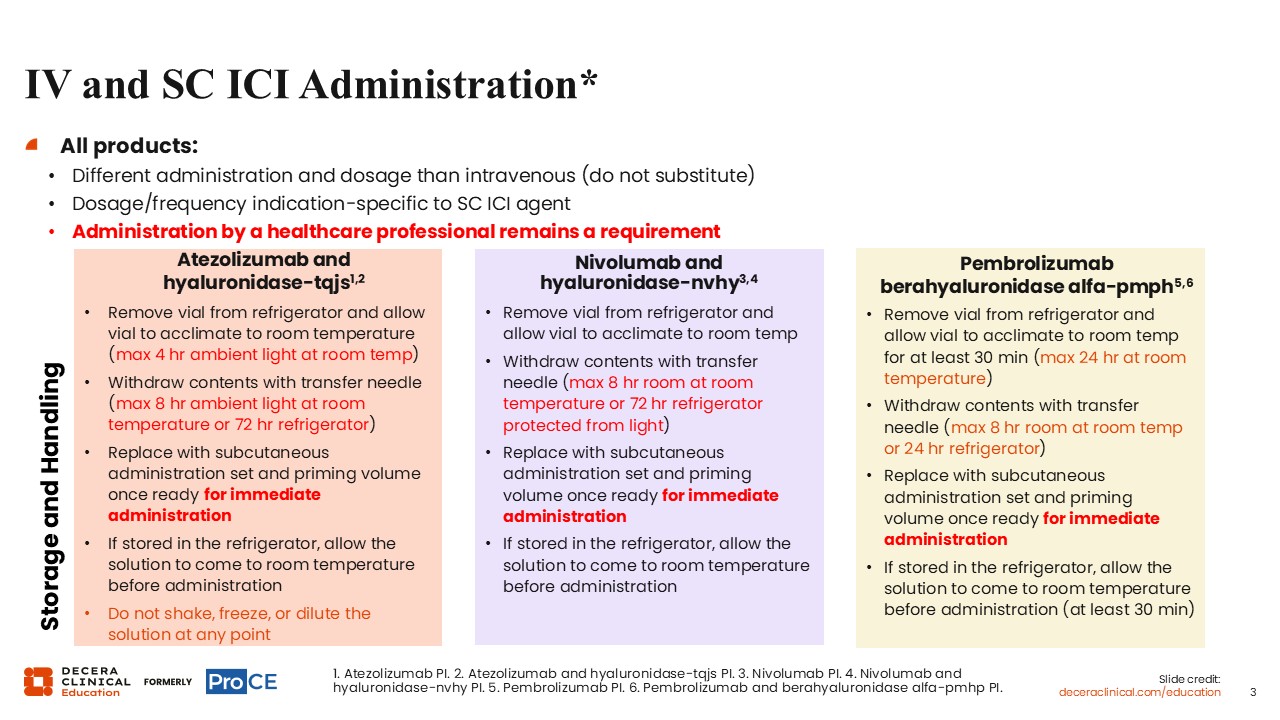
SC ICI products have different administration requirements and dosing schedules when compared with their IV formulation counterparts. It is important to note that dosing and/or handling should not be substituted directly. Moreover, dosage and administration frequency are indication specific for each SC ICI agent, and administration by an HCP remains a requirement for the SC formulations.2,4,6
Storage and handling instructions also vary by product.2 Atezolizumab and hyaluronidase-tqjs should be removed from the refrigerator and allowed to acclimate to room temperature, with a maximum of 4 hours in ambient light at room temperature before withdrawal. After withdrawal with a transfer needle, the product may be kept for up to 8 hours in ambient light at room temperature or up to 72 hours refrigerated. Once ready for immediate administration, the transfer needle should be replaced with an SC administration set and priming volume. If refrigerated, the solution should be allowed to return to room temperature before administration to the patient. Of importance, the prepared product should not be shaken, frozen, or diluted at any point.
Similar to SC atezolizumab, nivolumab and hyaluronidase-nvhy should be removed from the refrigerator and allowed to acclimate to room temperature.4 After withdrawal with a transfer needle, the SC nivolumab product may be kept for up to 8 hours at room temperature or up to 72 hours refrigerated and protected from light. Once ready for immediate administration, the transfer needle should be replaced with an SC administration set and priming volume. If refrigerated, the solution should return to room temperature before administration.
Similarly, pembrolizumab and berahyaluronidase alfa-pmph should be removed from the refrigerator and allowed to acclimate to room temperature for at least 30 minutes, with a maximum of 24 hours at room temperature before withdrawal.6 Following withdrawal with a transfer needle, the product may be kept for up to 8 hours at room temperature or up to 24 hours refrigerated. Once ready for immediate administration, the transfer needle should be replaced with an SC administration set and priming volume. If refrigerated, the solution should return to room temperature for at least 30 minutes before administration.
Deeper Dive Into SC Technology
Kelly Romo, PharmD, BCOP:
Hyaluronidase depolymerizes hyaluronic acid in the connective tissue matrix, decreasing tissue viscosity and increasing tissue permeability of SC ICI agents.7,8 The pharmacodynamic effect is described as transient, with the dermal barrier generally restored within 24 hours or less following administration. This transient mechanism is key, particularly with large-volume SC administration. For instance, atezolizumab and hyaluronidase-tqjs 15 mL SC injection is given in the thigh.2
2 Injection-Site Options for SC Immunotherapy: Abdomen or Thigh
Kelly Romo, PharmD, BCOP:
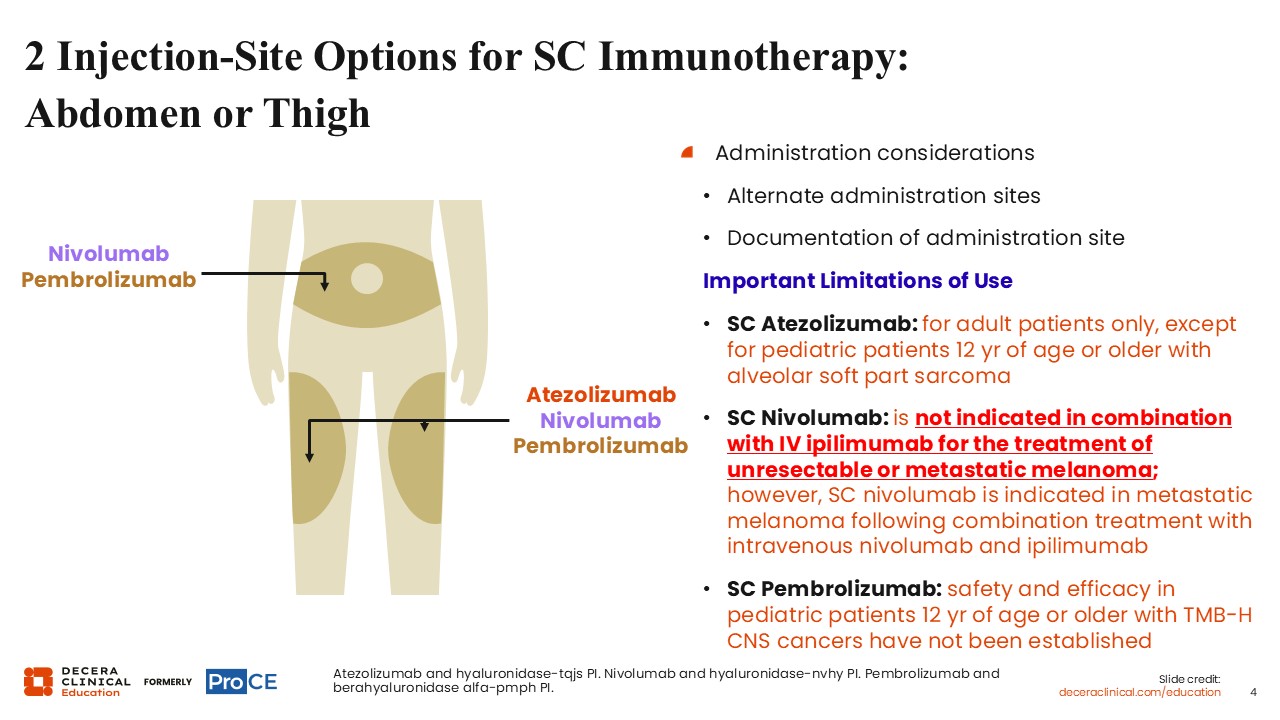
SC immunotherapy administration considerations include alternating administration sites and documenting the administration site. Nivolumab and pembrolizumab have 2 injection-site options: either in the abdomen or thigh.4,6
Atezolizumab, however, can only be administered in the thigh, with alternation of site between injections being highly recommended.2
Other SC administration considerations include:
- SC atezolizumab and hyaluronidase-tqjs is indicated for adult patients only, except for pediatric patients 12 years of age or older with alveolar soft part sarcoma.2
- SC nivolumab is not indicated in combination with IV ipilimumab for unresectable or metastatic melanoma; however, SC nivolumab is indicated in metastatic melanoma following combination treatment with IV nivolumab and ipilimumab.
- For SC pembrolizumab, safety and efficacy in pediatric patients 12 years of age or older with tumor mutational burden–high central nervous system cancers have not been established.
The main takeaway is that SC immunotherapy products differ in approved injection-site options and patient/use limitations, so HCPs should verify product-specific labeling, alternate and document administration sites, and avoid assuming interchangeability across agents.
Comparing HRQoL, Resource Use, Convenience, and Patient Satisfaction for IV vs SC ICI Administration
Kelly Romo, PharmD, BCOP:
A consideration for pursuing IV ICI vs SC ICI administration is when infusion-site reaction, skin irritation, bruising, or platelet concerns are elevated.9,10
Use of SC ICI over IV ICI is preferred when there is potential to reduce chair-time resource use and improve patient satisfaction because infusion visits may be less convenient and more time-consuming for the patient.
The overall advantages of SC ICI use include decreased patient treatment burden, improved efficiency of healthcare systems and resources overall, ease of administration for SC agents, reduced time spent in the oncology clinic, and the potential for outpatient or injection-clinic administration by a qualified HCP.
Current Challenges and Limitations of IV and SC ICI Administration for Patients With Solid Tumors
Kelly Romo, PharmD, BCOP:
For IV ICI administration, infusion chair-time availability is expected to remain limited, with only modest improvement anticipated from SC availability or implementation.9,10 Delays in treatment initiation may continue to occur and may contribute to psychological burden for patients waiting to begin therapy after a cancer diagnosis.
For SC ICI administration, ongoing implementation challenges include pharmacy impact, on-site logistics, personnel training, amended treatment times, premedication and offset timing, batching logistics, custody ownership, patient education on efficacy and expectations for the new formulation, insurance reimbursement implications, and prior authorization.
We should also note that IV administration remains the approved method for complex drug regimen combinations.3,4
SC ICI Product Specifics: Pricing
Kelly Romo, PharmD, BCOP:
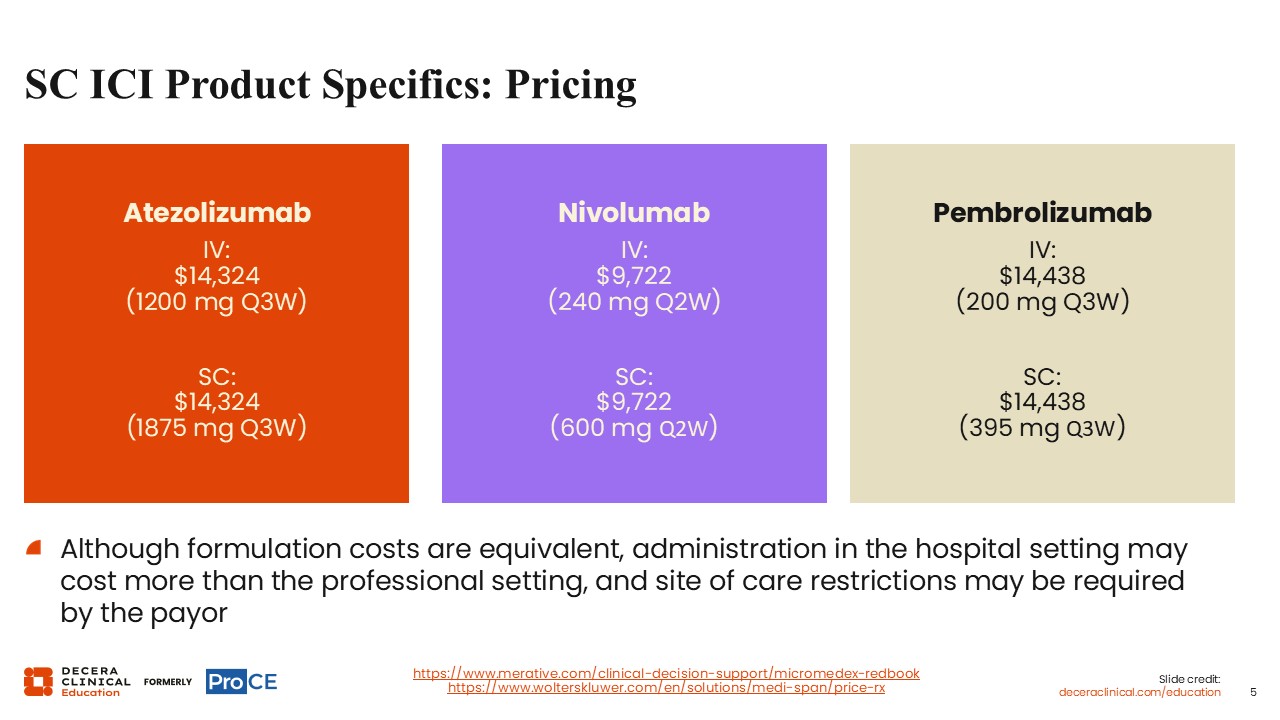
The listed average wholesale price as of May 2026 shows equivalence between IV and SC formulations for each of the approved IV and SC formulations.11,12
At the time of this publication, atezolizumab pricing is listed at $14,324 for IV 1200 mg Q3W and SC 1875 mg Q3W. Nivolumab price is listed at $9722 for IV 240 mg Q2W and SC 600 mg Q2W. Pembrolizumab is listed at $14,438 for IV 200 mg Q3W and SC 395 mg Q3W.
Although formulation costs are shown as equivalent, administration in the hospital setting may cost more than administration in the professional setting, and site-of-care restrictions may be required by the payer.
Potential Challenges With SC Administration of ICIs
Kelly Romo, PharmD, BCOP:
Potential challenges with SC ICI administration include variability in absorption and bioavailability compared with IV administration, privacy considerations for injections in the thigh or abdomen, and patient-specific factors such as weight and extent of SC tissue that may affect tolerability of the SC route.
Standardized dosing can also be challenging because absorption and bioavailability may vary across administration sites and among patients. These differences make a single flat SC ICI dose for all patients difficult to apply and may complicate the generalizability of study findings across patients and administration locations.
Nuances to Consider for SC ICI Treatment in Older or Frail Patients
Shawna Kraft, PharmD, BCOP:
For older or frail patients receiving SC ICIs, treatment planning should include comprehensive geriatric assessment and attention to frailty, which has been associated with inferior survival and increased complications.13,14 Performance status also matters: ICI efficacy appears lower among patients with Eastern Cooperative Oncology Group (ECOG) performance status (PS) ≥2, although irAE rates may be similar to those reported in patients with ECOG PS <2.
Available ICI data in patients aged 80 years or older suggest comparable efficacy and irAE rates, but patients aged 90 years or older discontinued treatment approximately twice as often despite similar irAE rates.15 These findings support individualized counseling and monitoring for older or frail patients rather than assuming that age alone determines suitability for SC ICI treatment.
Counseling Patients and Caregivers About irAEs
Shawna Kraft, PharmD, BCOP:
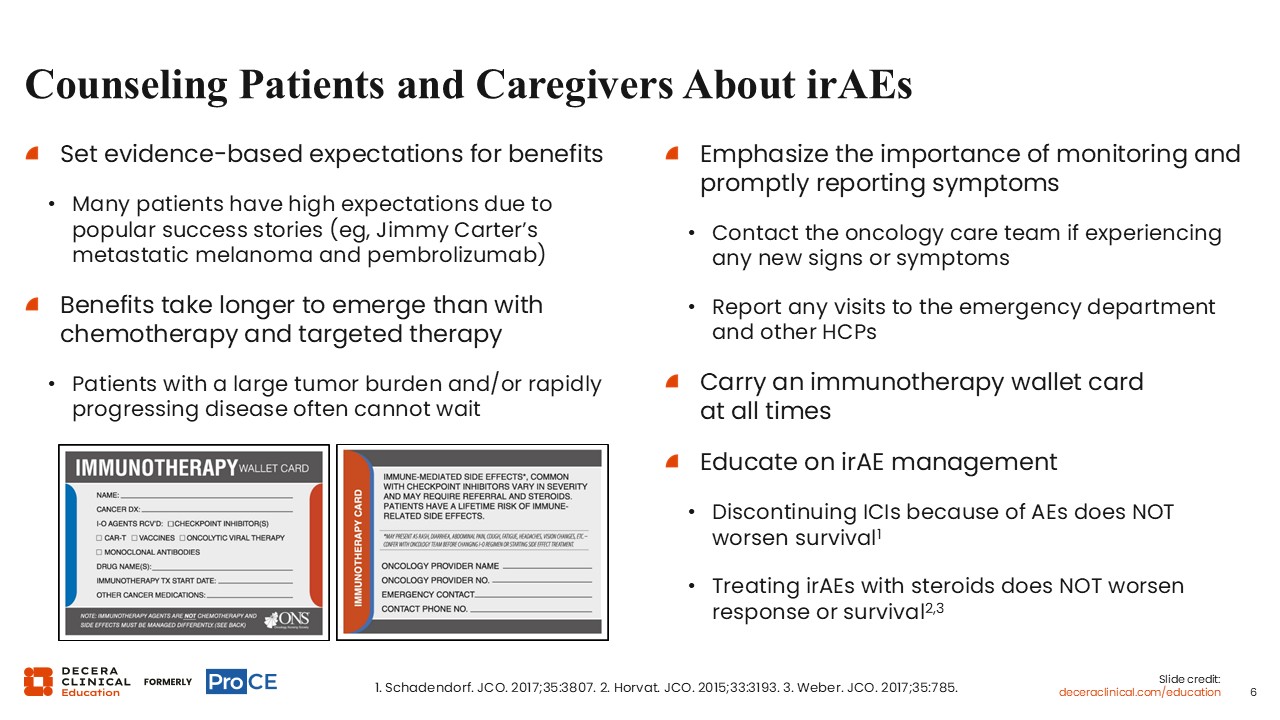
Patient and caregiver counseling should set evidence-based expectations for immunotherapy benefit. Although many patients may have high expectations because of well-known success stories, responses to ICIs can take longer to emerge than responses to chemotherapy or targeted therapy, and patients with large tumor burden or rapidly progressing disease may not be able to wait for delayed benefit.16
Kelly Romo, PharmD, BCOP:
Counseling should also emphasize early recognition and prompt reporting of potential irAEs.16-18 Patients should contact the oncology care team for any new signs or symptoms, report emergency department visits or visits with other HCPs, and carry an immunotherapy wallet card at all times. When irAEs occur, patients and caregivers should understand that appropriate management, including ICI interruption or corticosteroids when needed, does not appear to compromise survival or treatment response.
Other Key Considerations
Shawna Kraft, PharmD, BCOP:
Other key considerations include the need for a multidisciplinary approach to optimize SC ICI administration. The relative roles of multidisciplinary specialists may shift as SC ICI administration moves from hospitals to local settings.
Kelly Romo, PharmD, BCOP:
Monitoring considerations include irAEs and comorbidities. The irAE section emphasizes recognizing and addressing irAEs as early as possible, including symptom red flags, same-day escalation triggers, and on-call pathways. Patient and caregiver education should reinforce monitoring and prompt reporting of irAEs. Baseline assessment should include autoimmune disease, organ function, and medications.
Takeaways: Models to Consider
Shawna Kraft, PharmD, BCOP:
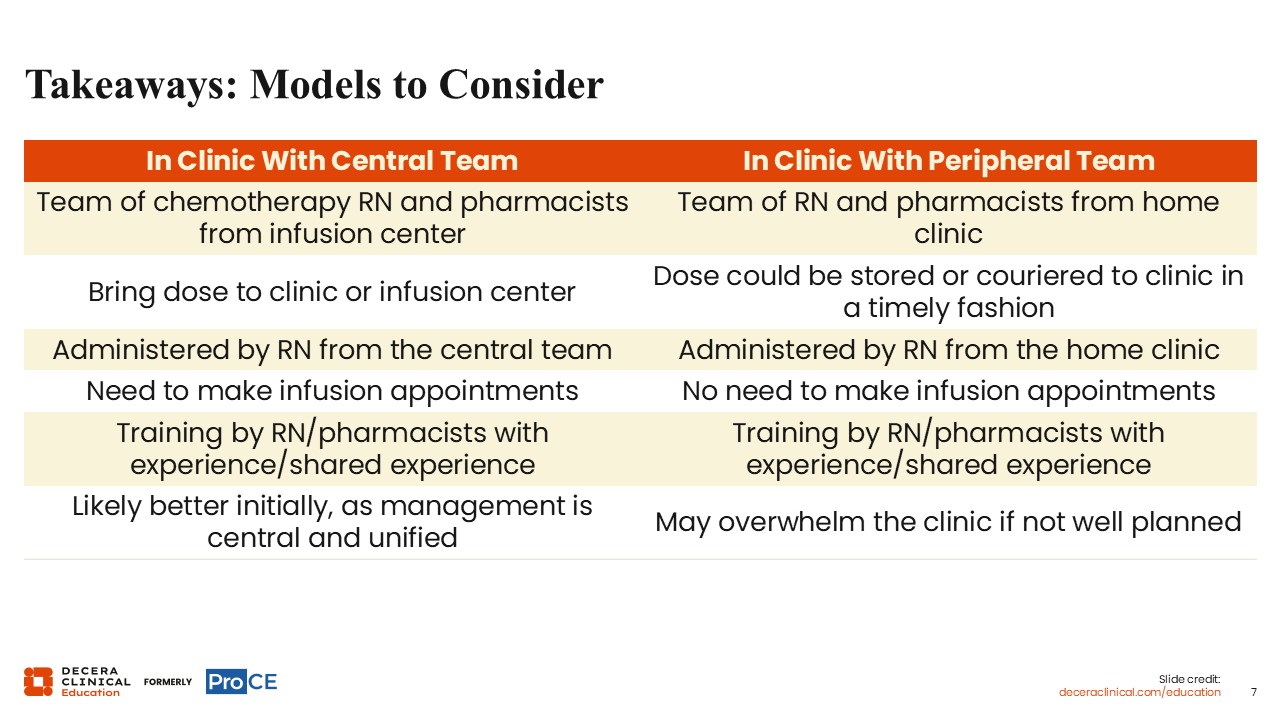
Two care models are compared: an in-clinic model with a central team and an in-clinic model with a peripheral team. The central-team model uses a chemotherapy registered nurse (RN) and pharmacists from the infusion center, brings the dose to the clinic or infusion center, and uses an RN from the central team for administration. Infusion appointments are needed, and training is provided by experienced RNs and pharmacists. This model is likely better initially because management is central and unified.
Kelly Romo, PharmD, BCOP:
The peripheral-team model uses an RN and pharmacists from the home clinic, with the dose stored or couriered to the clinic in a timely fashion and administered by an RN from the home clinic. Infusion appointments are not needed. Training is also provided by experienced RNs and pharmacists, but it is important to note that this model may overwhelm the clinic if not well planned.
Takeaways: SC vs IV ICI Administration
Shawna Kraft, PharmD, BCOP:
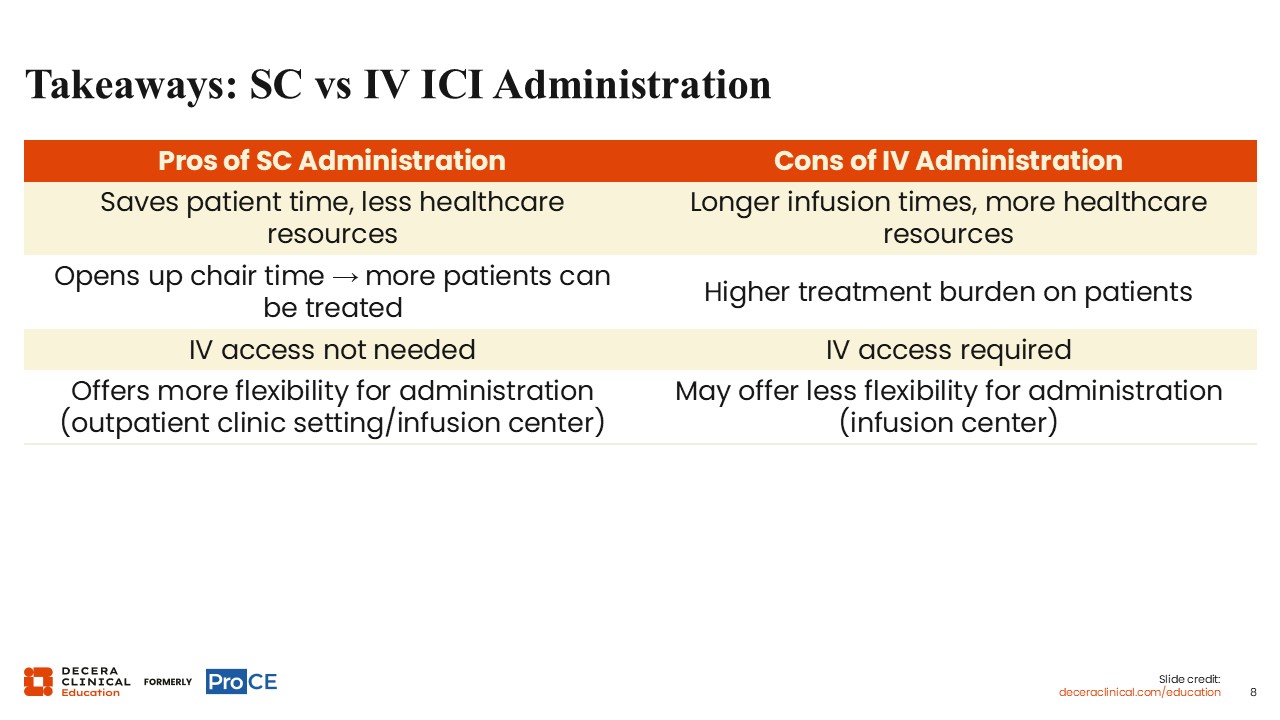
The takeaways compare advantages of SC administration with disadvantages of IV administration. SC administration may save patient time, require fewer healthcare resources, open infusion chair time so more patients can be treated, avoid the need for IV access, and offer more flexibility for outpatient clinic or infusion-center administration.
Corresponding IV administration considerations include longer infusion times, greater healthcare resource use, higher treatment burden for patients, need for IV access, and potentially less flexibility because administration may be tied to the infusion center.
Takeaways: Thoughts for the Future
Kelly Romo, PharmD, BCOP:
Future considerations include embracing SC ICIs in appropriate patient scenarios to benefit overall healthcare resources. Starting the process early may streamline acquisition, administration, billing, and reimbursement.
It is important to consider patient goals and treatment preferences, including patient power and requests for SC drugs. Additional agents are expected to enter this space, requiring monitoring of HCP uptake and product cost.