CE / CME
The Latest in Obesity Management: Current Evidence for Primary Care
Physician Assistants/Physician Associates: 1.00 AAPA Category 1 CME credit
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
ABIM MOC: maximum of 1.00 Medical Knowledge MOC point
Released: September 25, 2025
Expiration: September 24, 2026

Activity
Updated Obesity Definitions: Background
It is a new day in managing patients with obesity. Rates of obesity have climbed in the United States and around the world over recent decades, to the point where most adults in the United States have overweight or obesity.1,2 But medicine has come to a place where clinical obesity can be integrated into the medical milieu in such a way that healthcare professionals (HCPs) can use better strategies to communicate with patients and develop staged, comprehensive treatment plans that address obesity across the spectrum of its related comorbidities.
Recent efforts have culminated in a publication from the Lancet Commission on clinical obesity. The article highlights problems the medical community has faced in classifying and communicating about obesity as a disease. As with other chronic diseases, HCPs often have waited too long to treat obesity. HCPs would wait until a patient had obesity-associated complications before acting, but this approach does not yield the best health outcomes. Now, with the increased focus on cardiometabolic, kidney, and liver complications, and their relationships in the context of cardiovascular–kidney–metabolic syndrome, it is recognized that obesity underlies all these conditions and many other serious chronic diseases that our patients have.
The Lancet Commission also addressed limitations with using BMI alone to diagnose obesity. Historically, BMI has been the standard measure for excess adiposity or lack thereof. Although determining BMI is a fabulous first step, because it is an objective measurement that can be reproduced and it is not associated with stigmatizing language, it is imperfect. Body shapes are all different, and BMI does not necessarily take fitness or the relevant distribution of body fat into account.
The Lancet Commission report also describes obesity as a disease based on the effects excess adiposity has on the function of organs, tissues, and the individual. The thought is that HCPs will be able to individualize shared decision-making relative to the specific obesity effects a patient experiences. This approach goes beyond thinking about a number to considering health and quality of life.
We are not just looking at a number, but we should consider patients’ quality of life and whole health as well. Tying excess adiposity to other medical conditions makes medicalization and treatment of obesity clearer, and hopefully, it will also help with policy development.3
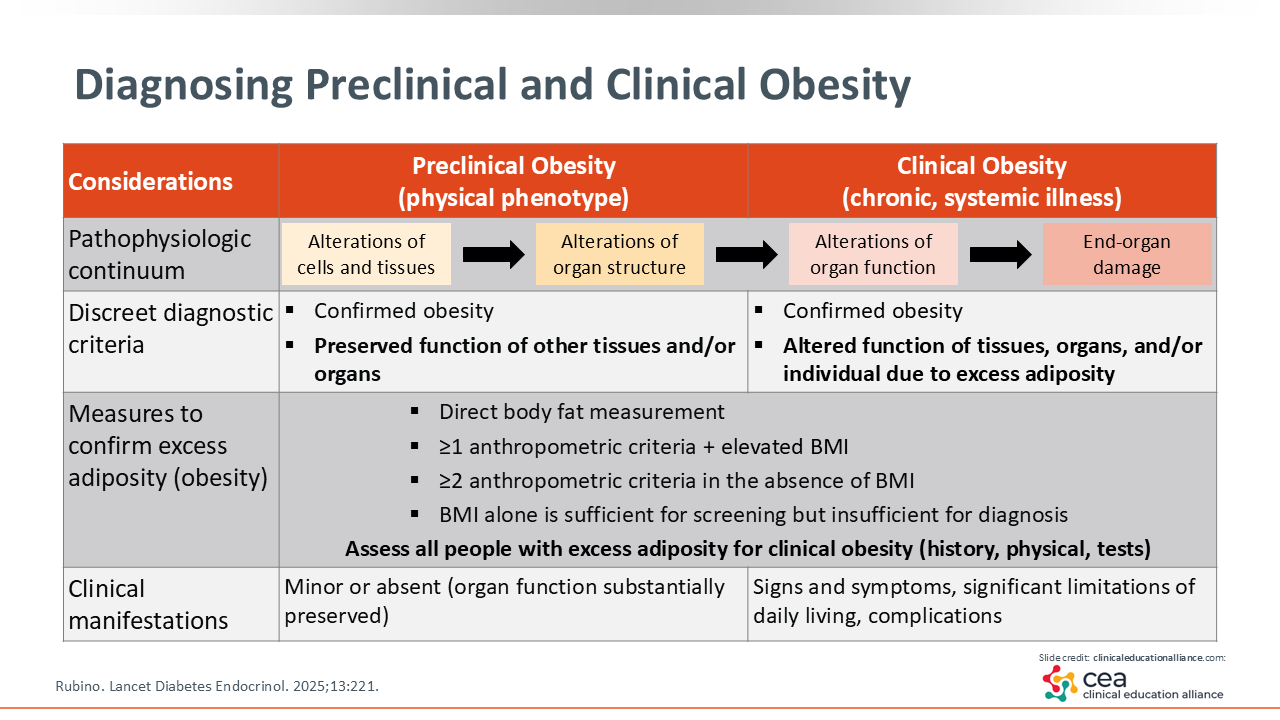
Diagnosing Preclinical and Clinical Obesity
The Lancet Commission defines obesity as a state characterized by excess adiposity, which is measured not only by BMI but also by other measurements. In addition, the Lancet Commission defines preclinical and clinical obesity stages. In preclinical obesity, HCPs have the opportunity to provide preventive healthcare if they screen, communicate, and take action.
It also is important to recognize that obesity pathophysiology is a continuum, and HCPs can intervene at any time. Early in the pathophysiology of obesity during the initial buildup of adiposity, particularly visceral adiposity, alterations in cells and tissues are subclinical. Although that impact may not be physically felt, it is not benign. As adiposity increases, it can result in alterations in organ structure and function. If patients live with excess adiposity long enough or if it is progressive, it can cause clinical symptoms or clinical abnormalities that could be biochemical or structural in nature. If obesity persists, it can lead to end-organ damage.
Of importance, HCPs should not wait for damage to occur before diagnosing obesity. Preclinical obesity can occur years to decades before there is end-organ damage, so HCPs have an opportunity to preserve patients’ health and prevent disease by diagnosing obesity. This requires a high index of suspicion and willingness to have open conversations with patients about excess adiposity and its impact on health.
In addition to BMI, which continues to be a measurement for assessing excess adiposity, HCPs should confirm an obesity diagnosis using direct body fat measurements or anthropomorphic criteria (eg, waist-to-hip ratio, waist circumference). These measurements allow HCPs to identify excess visceral adiposity, which may be present in patients who do not have elevated BMI or are absent in patients who have elevated BMI. This information is valuable in clarifying which patients would likely benefit from intervention.
Another point to highlight regarding preclinical obesity is that HCPs should not expect patients to present with complaints. With preclinical obesity, patients will not have symptoms and they may not have lab abnormalities, so this is a clinical diagnosis. The goal, of course, would be to prevent progression to clinical obesity, where patients would have signs and symptoms that change the way they live.3 These might include effects on activities of daily living, such as the inability to walk regularly or breathe well, presence of obstructive sleep apnea (OSA), insulin resistance, and/or changes in triglycerides. The goal is to address obesity earlier.
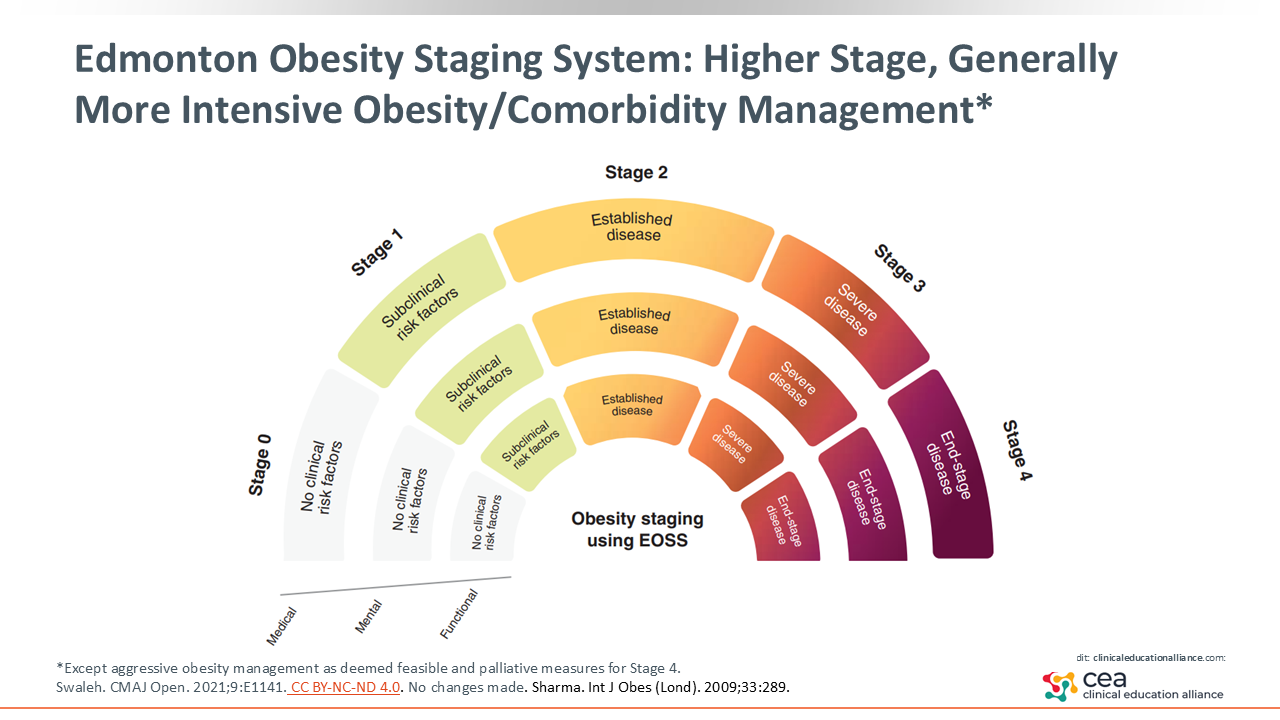
Edmonton Obesity Staging System: Higher Stage, Generally More Intensive Obesity/Comorbidity Management
The Edmonton Obesity Staging System is another tool to consider. It ranges from stage 0 to stage 4.4,5 Management interventions intensify with disease severity, with the exception of stage 4. At stage 1, treatment focuses on counseling and lifestyle measures, At stages 2 and 3, obesity intervention beyond lifestyle management and more aggressive obesity treatment are recommended. At stage 4, obesity intervention is as aggressive as deemed feasible, and palliative care is recommended.
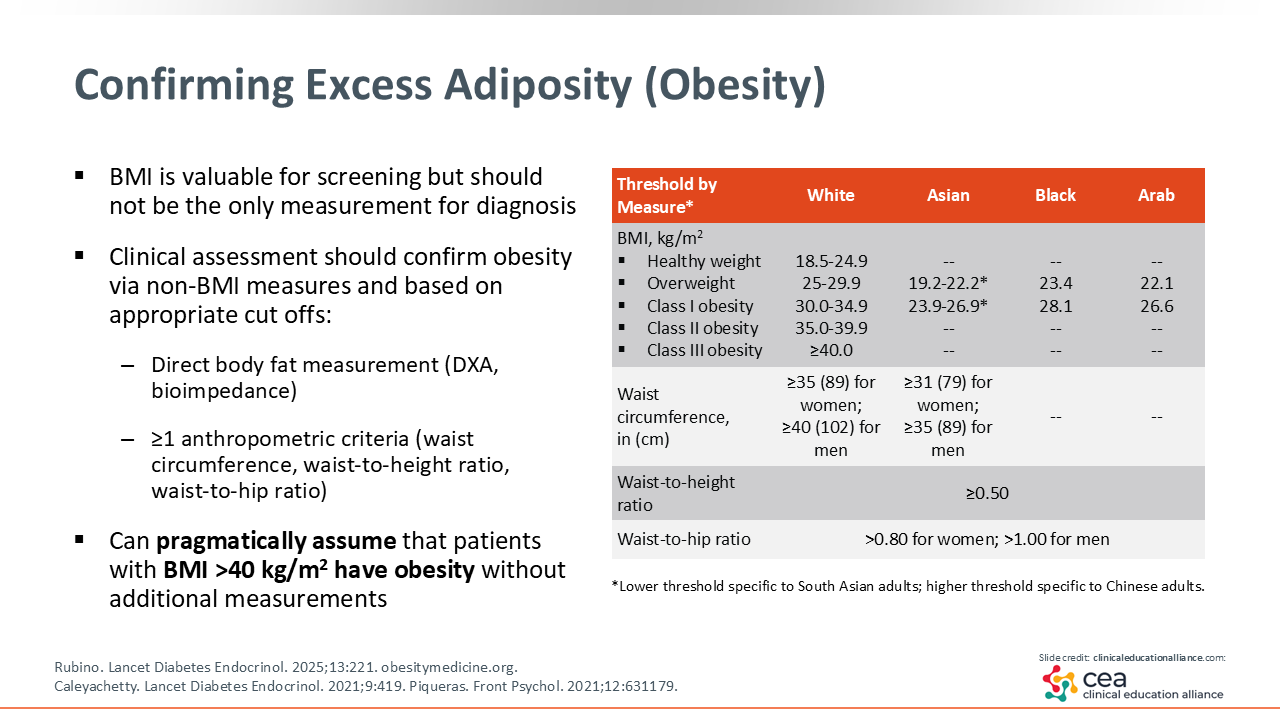
Confirming Excess Adiposity (Obesity)
Although BMI is a valuable screening tool, HCPs should use other measurements like waist circumference, waist-to-hip ratio, waist-to-height ratio, or direct measurements, such as DXA and bioimpedance that have become more accessible for primary care practice, to assess the presence and distribution of excess adiposity.3 DXA and bioimpedance are options for direct body fat measurements. In fact, my organization has both of these machines in our center, so we have better ways available to us to assess how the body’s fat is distributed.
There also are some ethnic and/or geographic differences in normalcy in terms of weight/body fat distribution. In European-based ethnic groups, the range for healthy BMI is 18.5-24.9 kg/m2. In Asian populations, a BMI of 19.2-22.2 kg/m2 has been classified overweight, although variability exists in thresholds among Asian populations. In European populations, obesity has been indicated by a BMI >30 kg/m2, which differs considerably from other world populations.6,7
When using anthropomorphic criteria like waist circumference or waist-to-height ratio, it is critical that HCPs use these in a way that is reproducible and scientific. Before implementing these measures in to practice, review resources to ensure it is being done in a way that adds value to a BMI measurement. This is particularly important when assessing patients with overweight because differences in waist circumference measurements will yield different interpretations regarding their adverse health risk.8
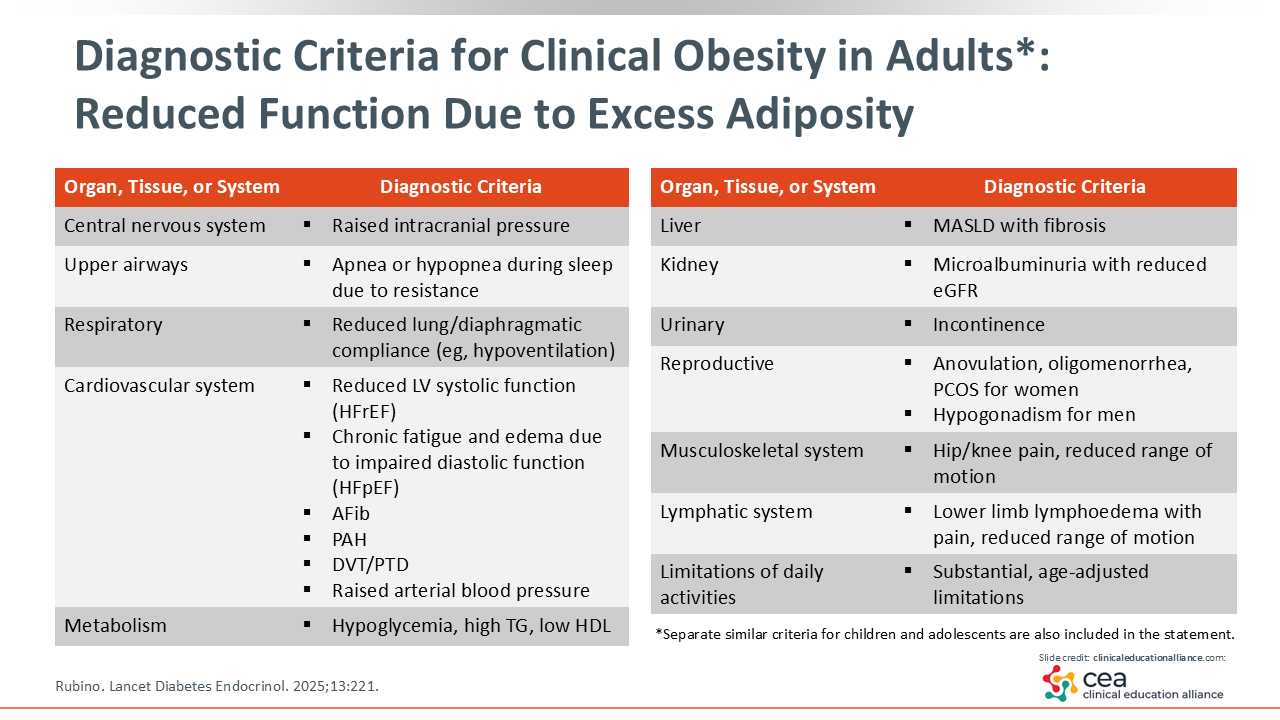
Diagnostic Criteria for Clinical Obesity in Adults: Reduced Function due to Excess Adiposity
Clinical obesity comprises more than what is physically seen with patients. It is vital that HCPs recognize that excessive adiposity can affect almost all systems of the body. There certainly are changes in the central nervous system. Many patients have trouble with their respiratory system in terms of OSA, hypoventilation, and/or exacerbation of other lung conditions. In addition, metabolic abnormalities, such as insulin resistance, dyslipidemia, and abnormal glucose and fat metabolism, are well recognized. There is potential for reproductive system abnormalities associated with excess adiposity, such as polycystic ovary syndrome, hypogonadism, and disrupted ovulation and menstrual periods.
Awareness of the effects of obesity on the liver is growing. Approximately one third of the world's population and approximately 70% of US patients with type 2 diabetes (T2D) have metabolic dysfunction–associated steatotic liver disease (MASLD), which is a leading cause of liver transplant.9,10 Although MASLD is common, it is a silent disease, and it is important for HCPs to recognize that it is may contribute to the diagnosis of clinical obesity. With excessive adiposity is also an increased risk of CKD, particularly with microalbuminuria. That microalbuminuria can be a marker of an inflammatory state.
Most patients will speak about the limitations in their daily life. For example, they may have joint pain and/or an inability to do daily tasks and other things that are usually self-fulfilling. If patients are having trouble with doing an activity, they might be inclined to do it less, and that decrease in activity can contribute to more weight gain.
Then there is heart failure—a silent condition for many patients. Although HCPs might be waiting for clinically obvious heart failure, it can occur silently in many patients with obesity. Therefore, HCPs must understand that the risk does not just comprise heart failure with reduced ejection fraction but heart failure with preserved ejection fraction as well because of the systemic resistance that can occur with excess body fat. Finally, general healing can be impaired in patients with obesity because of abnormal circulatory or lymphatic flow.
Clearly, there are many conditions associated with obesity, so it is important to keep them in mind and assess for them in patients who have obesity. Do a sleep study for OSA/hypopnea, and look for atrial fibrillation, heart failure, or pulmonary arterial hypertension. Patients often present with fatigue or edema, so HCPs should consider impaired diastolic function and heart failure with preserved ejection fraction. Furthermore, patients can have deep vein thrombosis, so HCPs should screen for musculoskeletal abnormalities along with cardiometabolic and renal abnormalities. Measure patients’ Fibrosis-4 score and look at an annual microalbumin as early biomarkers. Also get a good reproductive history to assess for abnormal ovulation/menstruation or hypogonadism.3
The goal is not for HCPs to be overwhelmed, but they should have a broad lens to screen for these abnormalities because patients might have some of these conditions—add this as a component of the comprehensive evaluation of patients as an entry point for diagnosis and treatment.
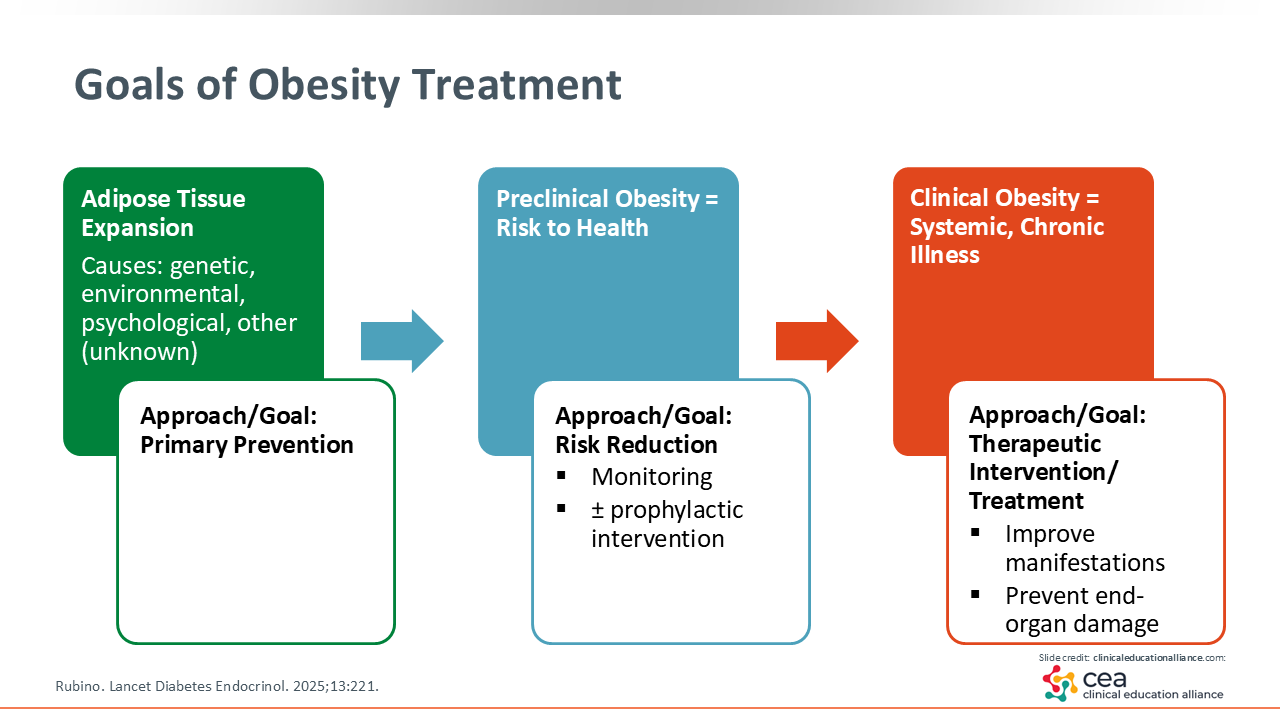
Goals of Obesity Treatment
It is important to recognize that excessive adiposity is affected by factors relating to patients themselves, the environment, and genetics. For patients, there might be a collection of approximately 20 things that are within their control and that might be relevant to their risk of obesity. However, there probably are 100 things outside of their bodies that might also contribute to their risk. When talking with patients, HCPs should take a comprehensive approach and ask what factors have contributed for each given person. Which factors are modifiable and which need attenuation? Taking the time to pose these questions will help minimize stigma patients might feel because patients often blame themselves. This also will allow HCPs to develop individualized treatment plans that should address barriers patients face.
For patients with preclinical obesity, it is important to communicate the potential risks to their health, develop a plan for monitoring them and their health, and explain steps that are included in the plan to prevent disease. For those with clinical obesity, HCPs must be able to recognize the systemic and inflammatory components of this disease and perform targeted screening for dysfunction. In particular, HCPs should recommend interventions that can improve the overall health of patients, including looking at what biomarkers might be relevant and need to be addressed.3
Case 1: Key Points on Diagnosing Clinical Obesity
For this patient, elevated BMI, confirmation of obesity via elevated waist circumference, and an obesity-related complication would confirm a diagnosis of clinical obesity. For other answers, more information on excess adiposity and its distribution and/or the presence of ≥1 obesity-related complication are needed to diagnose clinical obesity.
Through this patient case, it is now clear that new Lancet Commission recommendations provide more specificity in terms of diagnosing obesity. Rather than relying on a single number alone (eg, BMI), related complications are also taken into account. Hopefully, the new definition helps HCPs add a secondary assessment in their routine evaluation of patients with an elevated BMI. HCPs should look for potential complications/comorbidities early, so they can be more aggressive with their treatment approach in patients with clinical obesity. Recognize that if there is end organ damage one place, then it may also be somewhere else. This approach to obesity staging and treatment can help in identifying individualized treatment approaches, avoiding undertreatment and overtreatment.3