CE / CME
PrEP Made Practical: HIV Prevention in Mental Health Care Settings
Physician Assistants/Physician Associates: 0.75 AAPA Category 1 CME credit
Pharmacists: 0.75 contact hour (0.075 CEUs)
ABIM MOC: maximum of 0.75 Medical Knowledge MOC point
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Released: April 14, 2026
Expiration: April 13, 2027

Activity
Interplay Between Mental Health Conditions and HIV
This module will cover a group of people who are vulnerable to acquiring HIV, but who are not regularly seen in HIV-dedicated clinics: people with mental health conditions.
In my practice, I see people with mental health conditions in an integrated HIV clinic, where psychiatry services are built in. The reason this model works is that many people with mental health conditions like substance use disorder (SUD) and opioid use disorder (OUD) can be at increased risk for acquiring HIV. I strongly encourage HCPs to get people with either disorder started on PrEP.
Unfortunately, these patients may not adequately understand their HIV risks or know that PrEP can help them reduce this risk. That’s why you and I, as mental health care professionals, are needed to help facilitate this care.
Before getting into the details of how you can help prevent HIV in mental health care settings, I want to discuss some background information that shows why this is so important.
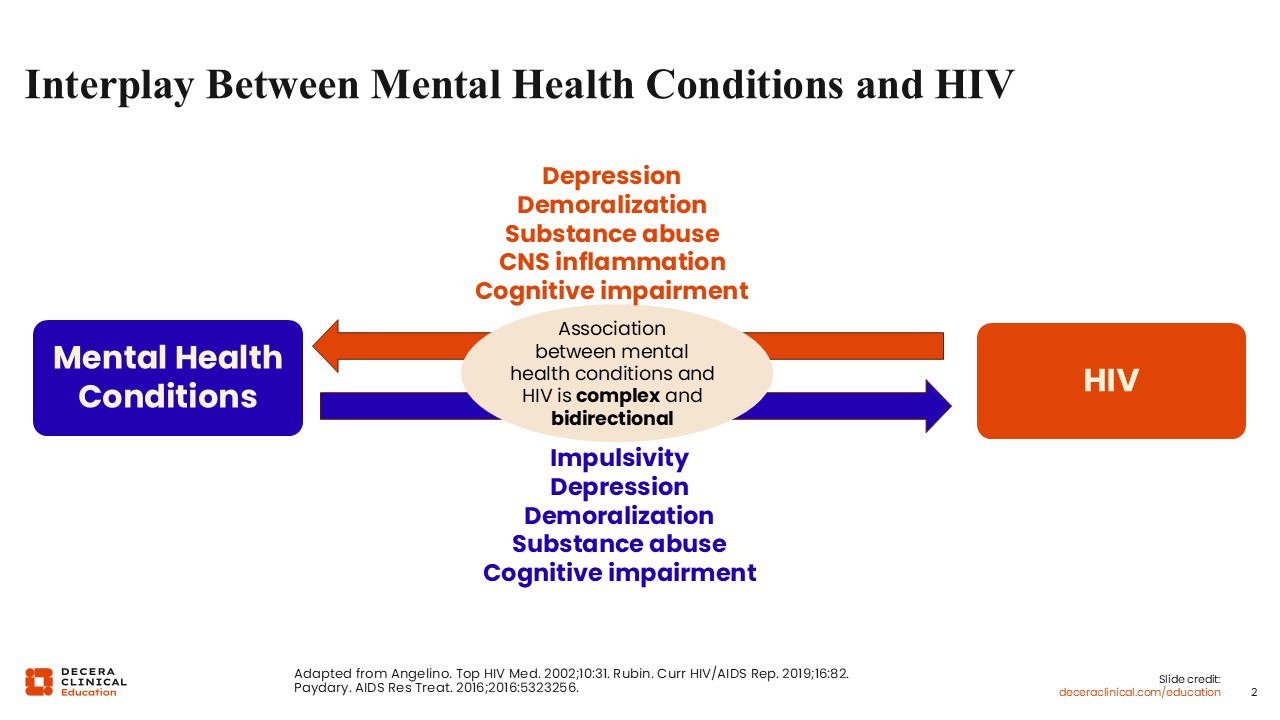
There is a significant, bidirectional relationship between mental health conditions and HIV. Mental health conditions increase impulsiveness, feelings of depression and demoralization, substance use, and cognitive impairment. All of which are known risk factors for HIV infection.
In turn, HIV worsens feelings of depression and demoralization, substance use, and cognitive impairment, and causes inflammation in the central nervous system and stigma, which cycles back around and exacerbates any present mental health conditions.
To put it simply, mental health conditions increase an individual’s risk for acquiring HIV, and HIV worsens existing mental health conditions.
This vicious cycle is a big problem for people with mental health conditions, which is why preventing HIV with PrEP is clearly a desirable outcome for this vulnerable population.1-3
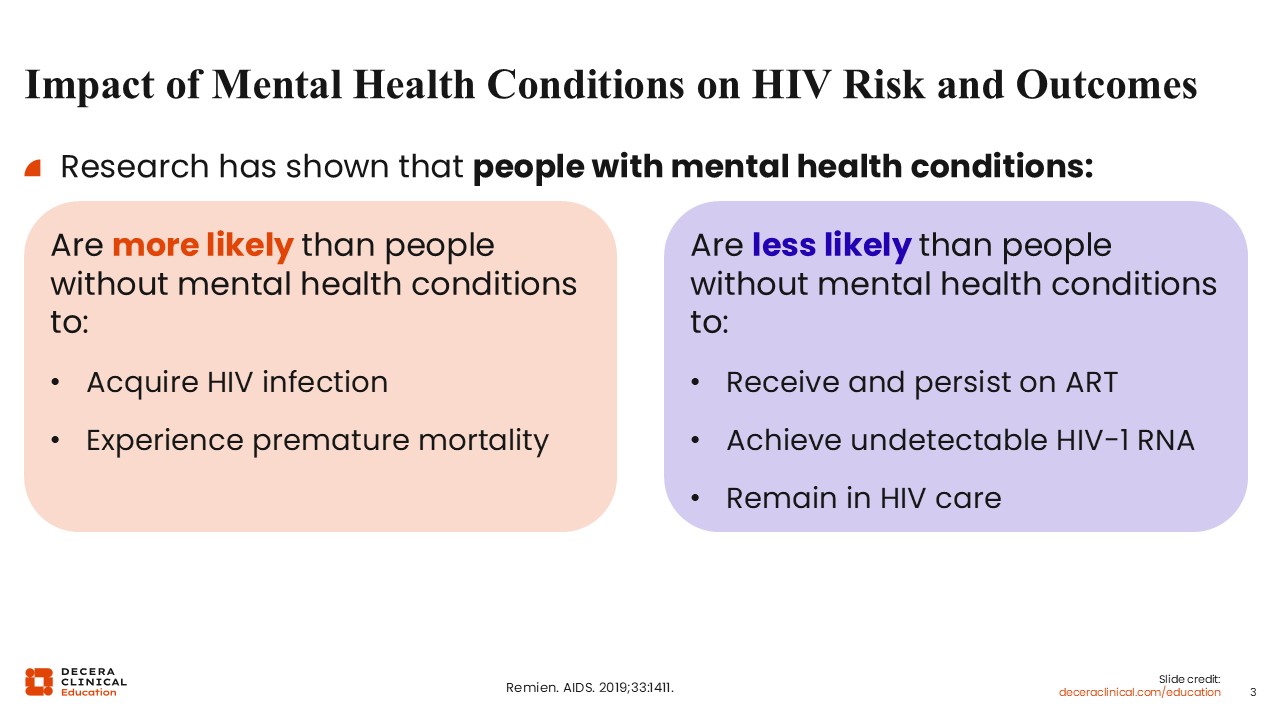
Impact of Mental Health Conditions on HIV Risk and Outcomes
Furthermore, research has shown that people with mental health conditions are more likely to acquire HIV infection and experience premature mortality. These individuals are also less likely to receive and stay on antiretroviral therapy (ART), achieve undetectable HIV-1 RNA, and remain in HIV care after acquiring HIV compared with those without mental health conditions.3
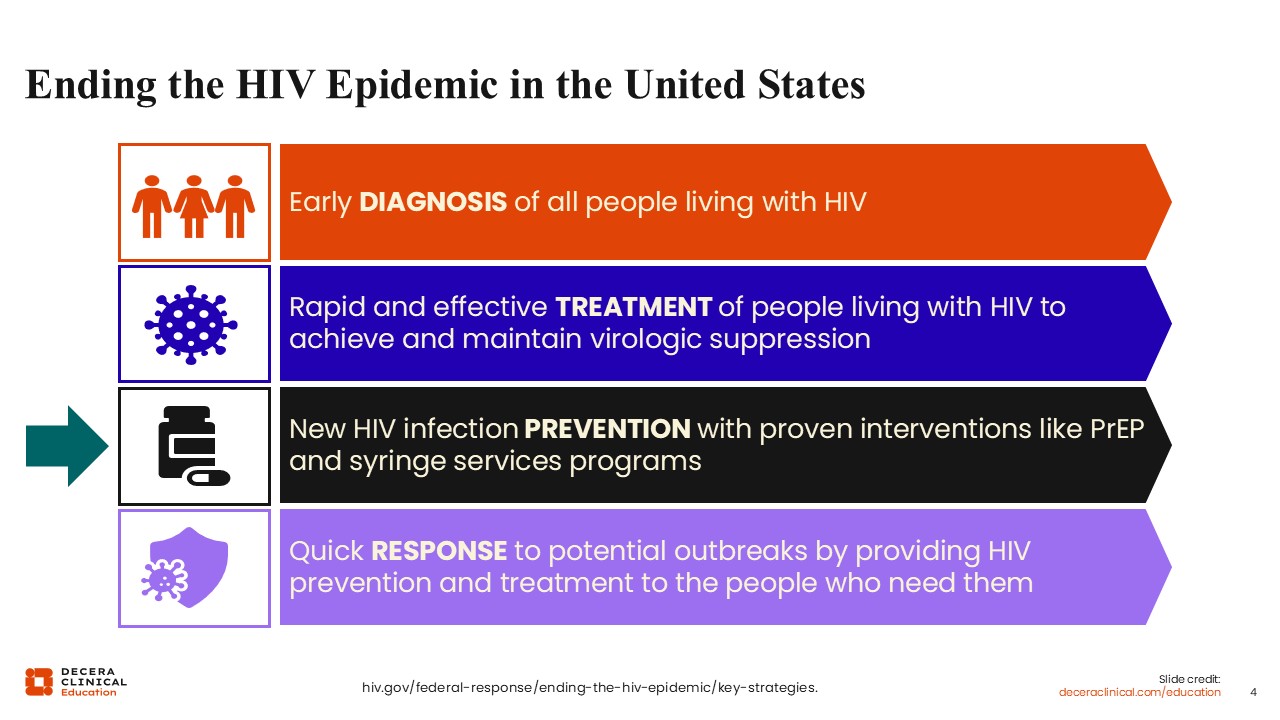
Ending the HIV Epidemic in the United States
More broadly, a top goal in medicine today is to end the HIV epidemic in the United States. Doing so requires several important points of care.
Preventing new HIV transmissions is key and can be effectively done with PrEP as well as by practicing safer sex and injection behaviors for certain individuals.4
Mental Health Care Professionals’ Responsibility to Prescribe PrEP
One important way to bridge this significant gap in care is to integrate HIV prevention with PrEP into mental health care. This is feasible because people with mental health conditions often see their mental health care professionals more regularly than their other HCPs, which can aid in education and ensuring persistence.
Furthermore, as a mental health care professional, you probably already discuss sexual history and sexual health with patients. PrEP can easily be a part of that conversation.
In addition, other specialists are not as knowledgeable about treating mental health conditions, and there are certain conditions, particularly SUD and OUD, that increase the need for PrEP, further highlighting the central role mental health care professionals play in preventing HIV transmission among key vulnerable populations.3,5
Mental Health Conditions Increase the Need for PrEP
Provision of PrEP in healthcare settings where people are comfortable and already frequently visiting, like mental health clinics, improves persistence. Yet 1 study found that only approximately 20% of mental health clinics in New York prescribe PrEP. This reflects a national issue regarding the separation between mental health care and medical care.
Offering PrEP in mental health care settings is critical because there are psychological benefits associated with it. For example, it allows people to take control of their HIV risk, thereby liberating them from certain fears. In addition, those who are taking PrEP often are more invested in their health and well-being. 6,7
Psychological Benefits for People Taking Control of HIV Risk
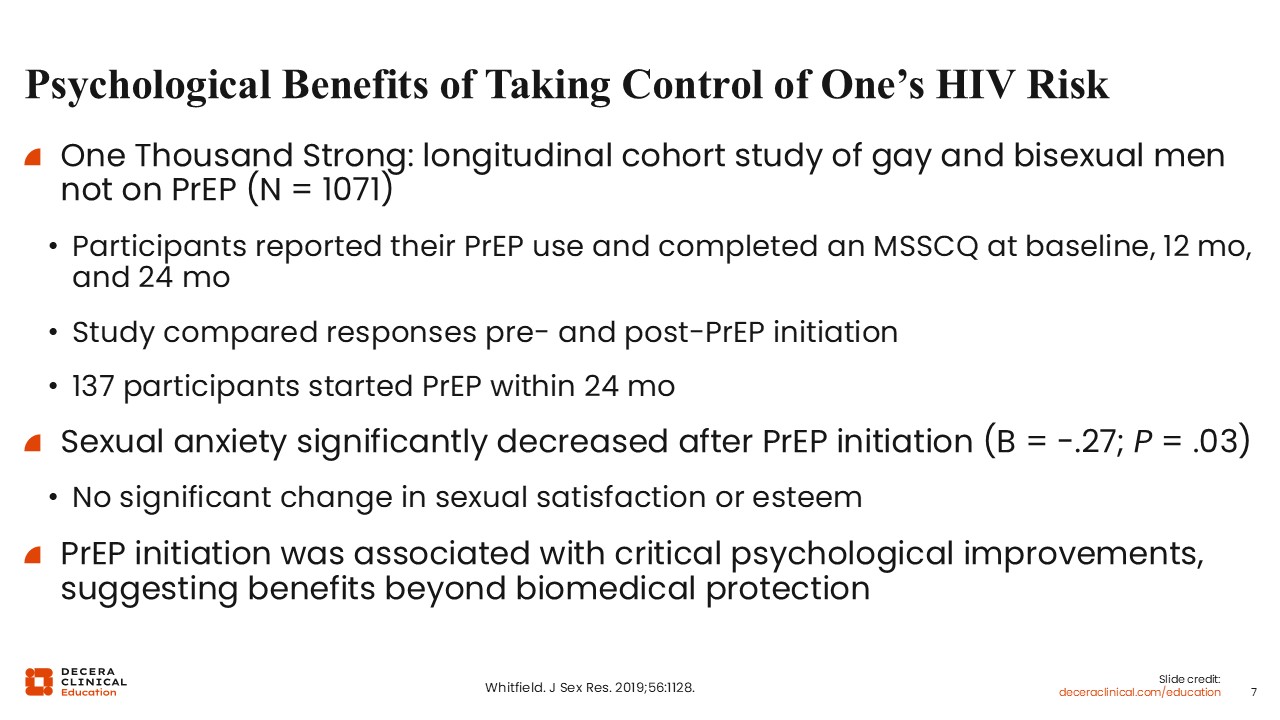
Here is 1 study that highlights the key psychological benefits of PrEP: significantly improved anxiety around sexual health and overall quality of life.
The longitudinal cohort study called One Thousand Strong evaluated 1071 gay and bisexual men not on PrEP. They reported their PrEP use and completed the Multidimensional Sexual Self-Concept Questionnaire at baseline, 12 months, and 24 months.
The analysis compared participants’ responses pre and post PrEP initiation. Results showed that 137 participants started PrEP within 24 months, and that their sexual anxiety significantly decreased after PrEP initiation.8
Who Should Be Considered for PrEP?
To whom should you consider offering PrEP? According to the CDC, all sexually active adults and adolescents without HIV must be informed about PrEP.
In addition, anyone who requests PrEP should be prescribed it, including those without reported HIV risk factors, provided that you have evaluated them and think it is a reasonable thing to do.9
People who request PrEP may have undisclosed risk behaviors; therefore, it is reasonable to discuss the risks and benefits of PrEP with them even if you don’t think they are at risk of acquiring HIV.
Available PrEP Options
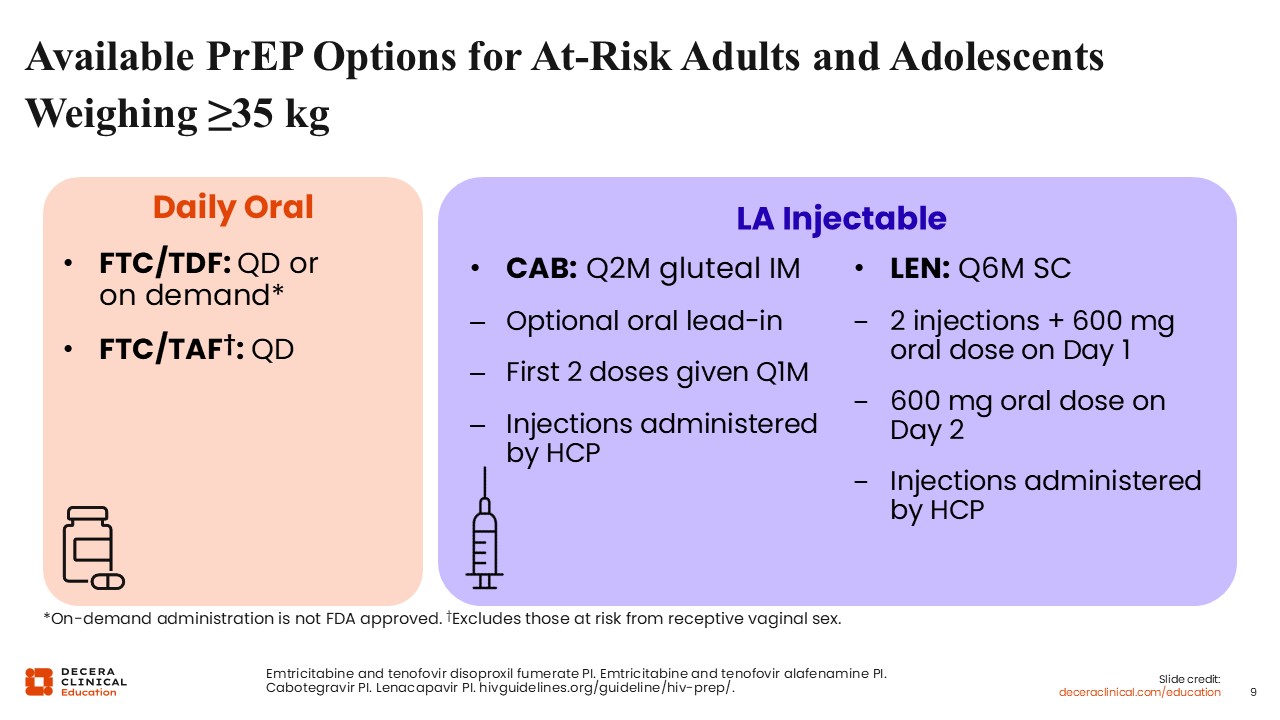
Even if you are not an HIV specialist, understanding the PrEP options is simple. In the US, there are 4 currently available and approved PrEP options, which are all indicated to reduce the risk of sexually acquired HIV in adults and adolescents weighing at least 35 kg.
The first 2 options, both guideline recommended, are daily oral PrEP: emtricitabine (FTC)/tenofovir disoproxil fumarate (TDF) and FTC/tenofovir alafenamide (TAF). Both can be taken with or without food.
On-demand or 2-1-1 dosing with FTC/TDF, which is PrEP taken immediately before and for 2 days after sex, is also guideline recommended for certain populations, even if that dosing is not approved by the FDA.10-12
FTC/TDF is not recommended for use in people with renal or bone disease, but FTC/TAF is safe to use in these populations.11,12
The third PrEP option is the long-acting injectable cabotegravir (CAB). Instead of a daily pill, it is administered every 2 months as an intramuscular injection in the gluteal muscle. The initial doses are given monthly for the first 2 months. You have the option of starting CAB with an oral lead-in dose, which is something that I always use. It helps protect people as the drug levels build up and allows me to assess tolerability. These CAB injections must be administered by an HCP.13
The final PrEP option is another long-acting injectable called lenacapavir (LEN). Its maintenance doses are administered every 6 months via subcutaneous injection. The dosing schedule for LEN is a lead-in of two 1.5-mL injections and two 300-mg tablets on Day 1. Then it is administered via two 300-mg tablets only on Day 2, which is followed by twice annual injections thereafter. Like CAB, HCPs are required to deliver all LEN injections.14
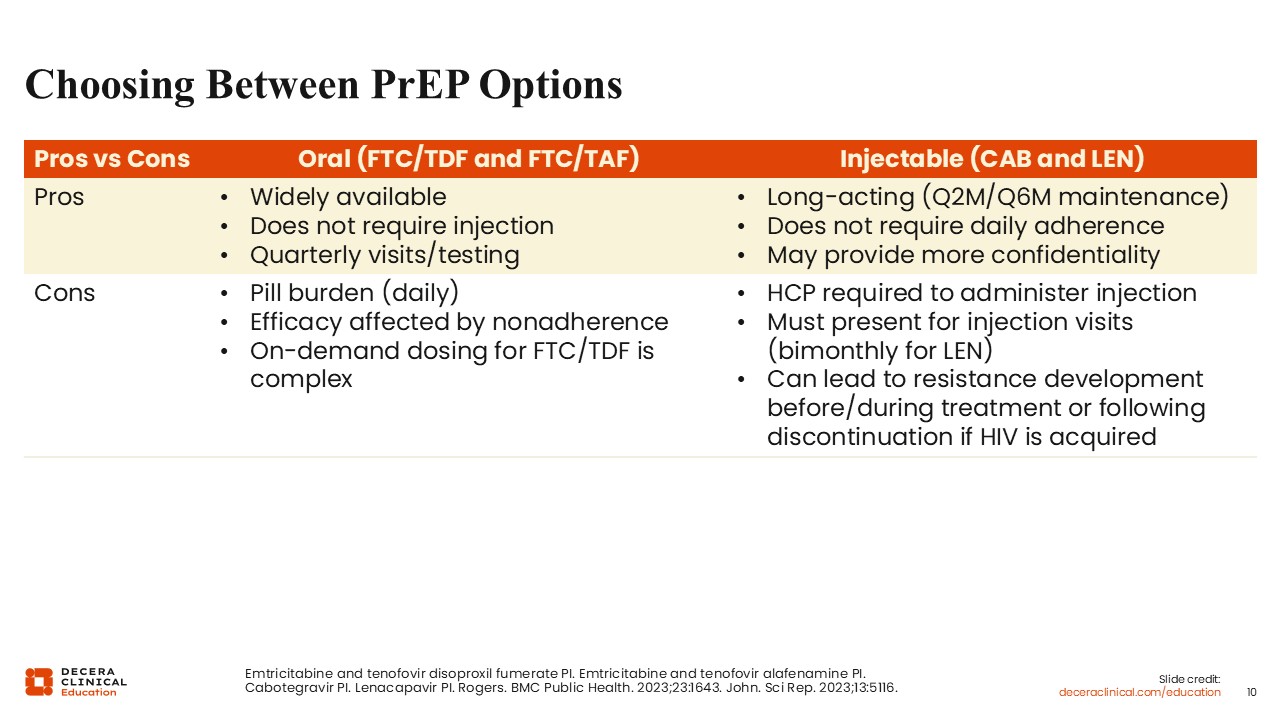
Choosing Between PrEP Options
With so many PrEP options, it is likely that every patient can find one that best fits their needs and lifestyle.
Oral options are easy to use and do not require HCPs to deliver the drugs. Furthermore, oral PrEP is widely available, can be easily refilled as a prescription, and is convenient for many. Patients generally need to present for visits and testing once a quarter only. Comparison studies also have shown that both oral PrEP options (FTC/TDF and FTC/TAF) are well tolerated. However, this dosing has a pill burden and requires people to be adherent to daily pills to remain effective in preventing HIV.15
Some people prefer the on-demand dosing, that is 2-1-1 or event-driven dosing, where patients take 2 doses right before sex and 1 dose daily for the next 2 days after sex. It is a reasonable option for men who have sex with men, as it has been used successfully in studies. But this dosing schedule is complex and can be hard for some people to remember. Furthermore, not everybody knows when they are going to have sex.
For people who cannot adhere to daily pills, long-acting injectables can help. CAB and LEN PrEP options, with maintenance doses administered every 2 and 6 months, respectively, can also provide confidentiality and decreased stigma since they are administered in the healthcare setting vs keeping pills at home.
Although injection visits can be rescheduled to maintain efficacy, it is undesirable to have people on CAB or LEN if they are not going to present for their injection visits. This is especially true for those who will remain adherent for a while and then stop a year or 2 later.
Many patients report injection-site pain and postinjection issues with CAB and LEN, which is important to discuss with patients. Also, although all PrEP options are incredibly effective at preventing HIV when taken properly, and long-acting options help with adherence, there is also a risk of resistance development if HIV is acquired during or after long-acting PrEP. That is important for HCPs to understand and monitor.10,13,14,16,17
I believe that all PrEP-providing HCPs should know how to administer these agents, even if they do not have people currently on long-acting injectables.
For example, HCPs should apply ice before administering a CAB or LEN injection; giving people topical or oral analgesics can also help. When removing the needle, HCPs should take it out following the same angle that was used to insert it, and the needle should sit for a moment after administration to prevent leakage at the site. Finally, HCPs should always bandage the injection site after each injection.
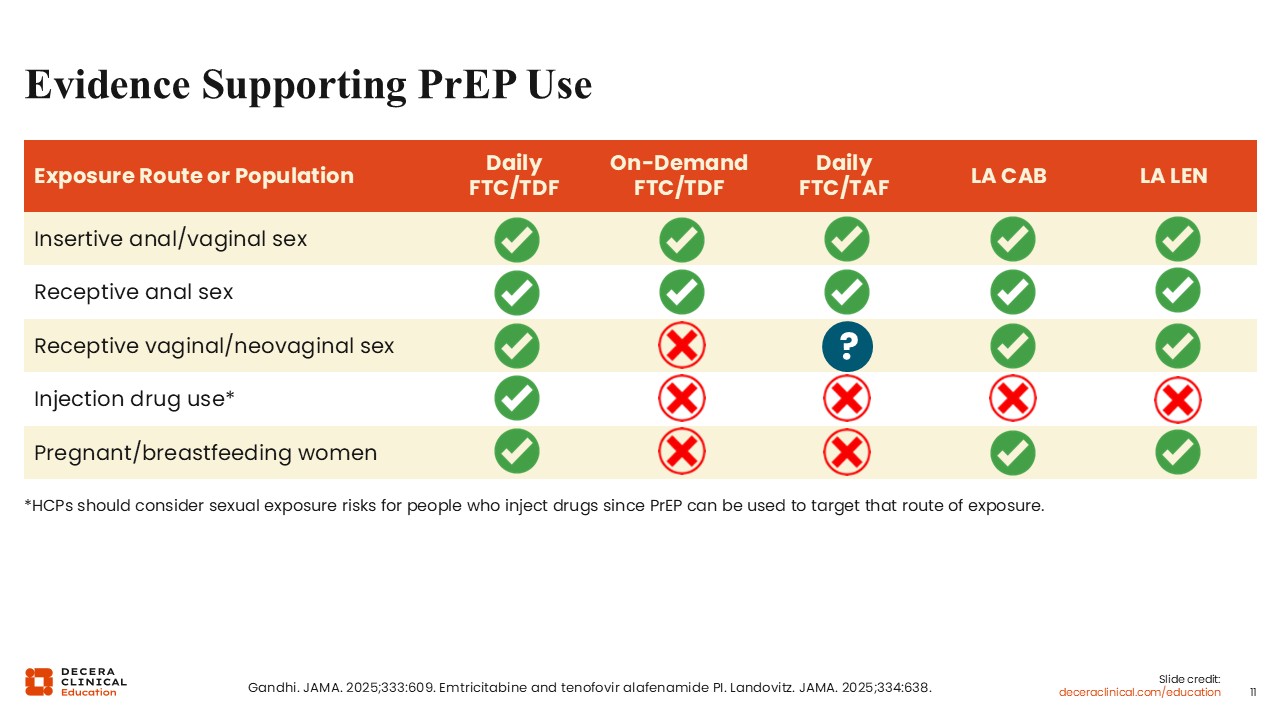
Evidence Supporting PrEP Use
This slide illustrates the populations in which each PrEP option has proven efficacy. There is good evidence supporting daily oral PrEP use in nearly every population. Daily FTC/TDF has had more studies done, showing it to be effective in insertive anal and vaginal sex, receptive anal sex, receptive vaginal/neovaginal sex, and injection drug use, as well as among those who are pregnant or breastfeeding.
Fewer studies evaluated on-demand FTC/TDF, which is only proven effective in insertive anal and vaginal sex as well as receptive anal sex.
Daily FTC/TAF is also effective in insertive anal and vaginal sex as well as receptive anal sex. There is a question about its efficacy in receptive vaginal/neovaginal sex; the jury is still out on that. The same goes for injection drug use or among those who are pregnant or breastfeeding.
Both long-acting CAB and LEN are effective in insertive anal and vaginal sex, receptive anal sex, and receptive vaginal/neovaginal sex, as well as among those who are pregnant or breastfeeding.12,18,19 Even though there is no proven efficacy in injection drug use, that does not mean it will not become an option for this population one day.
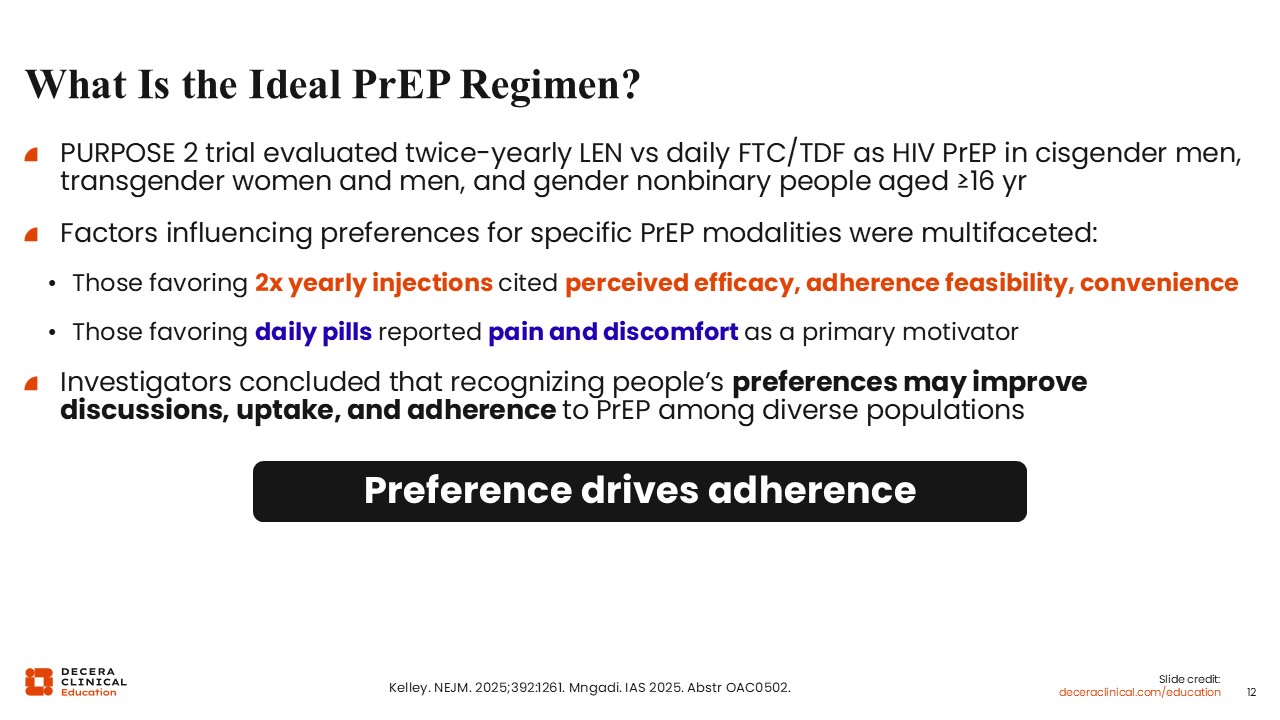
What Is the Ideal PrEP Regimen?
When it comes to choosing the ideal PrEP regimen, the choice will depend on each person’s health goals and preferences. This was illustrated in the phase III PURPOSE 2 trial that evaluated patient-reported outcomes with twice-yearly LEN vs daily FTC/TDF in cisgender men, transgender women and men, as well as gender nonbinary people who were at least 16 years of age.20
The study found that the factors that influenced people’s PrEP choice were multifaceted. Those who preferred LEN perceived efficacy, adherence feasibility, and convenience as top concerns.
By contrast, those who favored FTC/TDF worried more about the pain and discomfort of injections.21
Considering people’s individual concerns and preferences is the best way to help them decide which PrEP option will fit their needs.
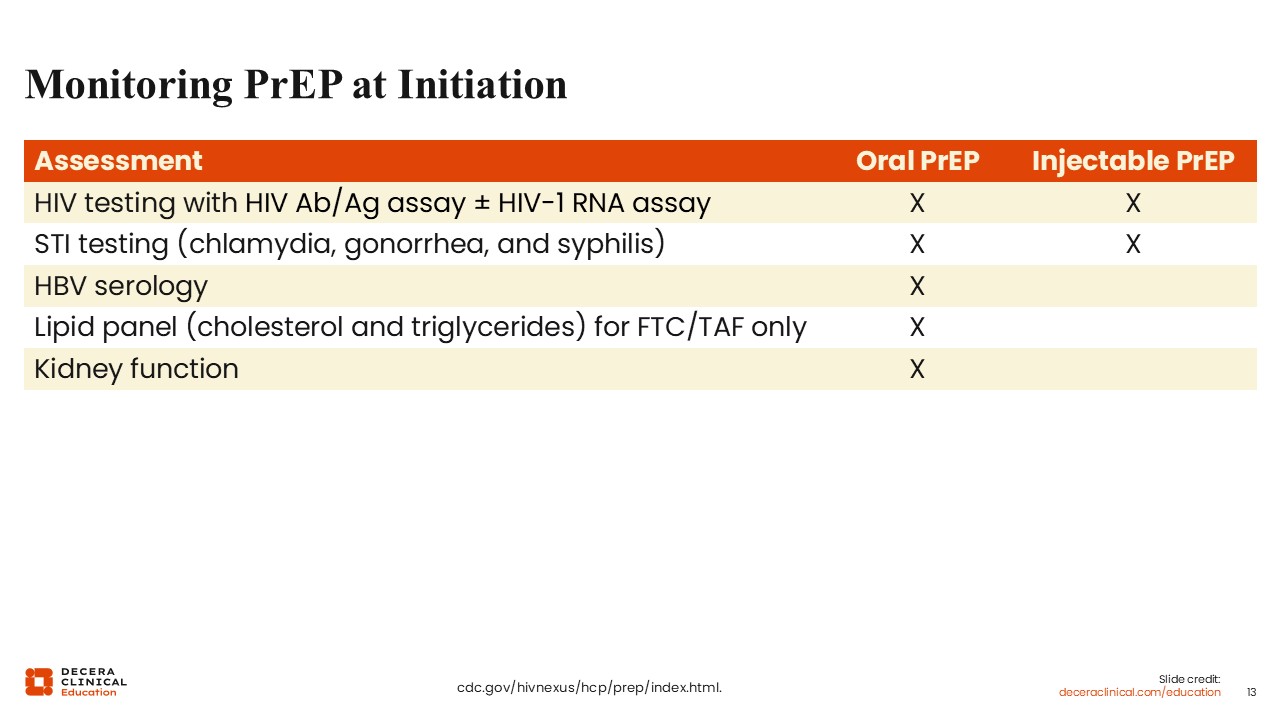
Monitoring PrEP at Initiation
What do you need to do before initiating PrEP?
The first thing you must do at initiation is take a careful baseline assessment. People must be tested for HIV via an antibody/antigen assay, with or without an HIV-1 RNA assay, to confirm that the person is not already living with HIV. This is critical because PrEP regimens are for prevention; they are not complete treatment regimens.
Next, avoid initiating PrEP in people with active sexually transmitted infections (STIs). That means we need to screen for active chlamydia, gonorrhea, and syphilis infections and treat those right away before starting PrEP.
There are some additional requirements when initiating oral PrEP. This includes testing people’s hepatitis B virus (HBV) serology and kidney function and, for FTC/TAF, checking lipids. PrEP is not contraindicated in those with active HBV infection; this is simply a screening requirement.9
Finally, not explicitly stated in the CDC guidelines but critical at PrEP initiation, is to carefully evaluate people on adherence and risk reduction. People must understand why PrEP is important for their health and how adherence will impact its efficacy. This will help ensure persistence.
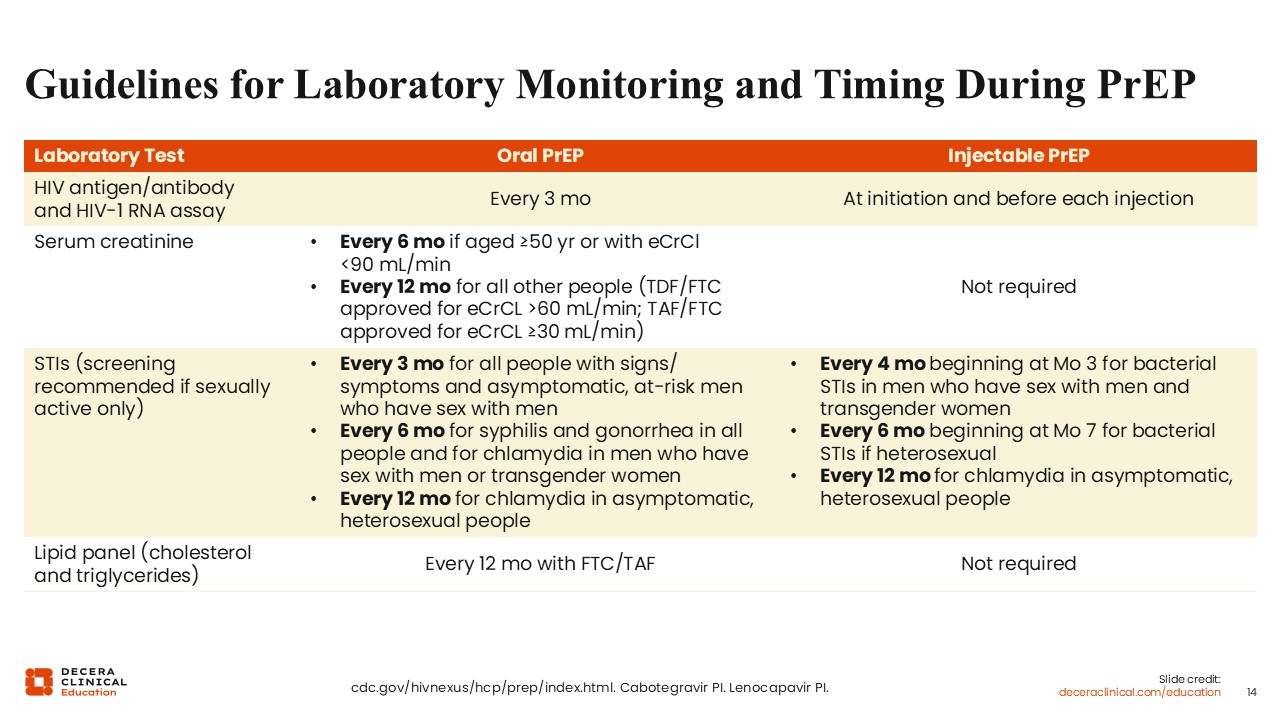
Laboratory Monitoring and Timing During PrEP
After completing baseline assessments and initiating PrEP, there are additional tests and measures that HCPs must continue to monitor. For example, all oral PrEP users should be tested for HIV every 3 months, whereas those on long-acting injectables should be tested for HIV before each injection.13,14 The reason for this is that people can have a low level of infection while taking PrEP and not realize it. Then you would have both the drug and virus on board, which could lead to resistance, so you want to retest people as recommended throughout their course.
Depending on the PrEP regimen, there are other monitoring recommendations listed on this slide, including kidney function via serum creatinine, monitoring for active STIs, and lipid monitoring,9 which might be reasonable in people taking psychoactive therapies.