CE / CME
Optimizing Shingles Vaccination: Current Trends and Expert Strategies for Improving Uptake and Series Completion
Pharmacists: 1.00 contact hour (0.1 CEUs)
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Released: January 30, 2026
Expiration: January 29, 2027



Activity
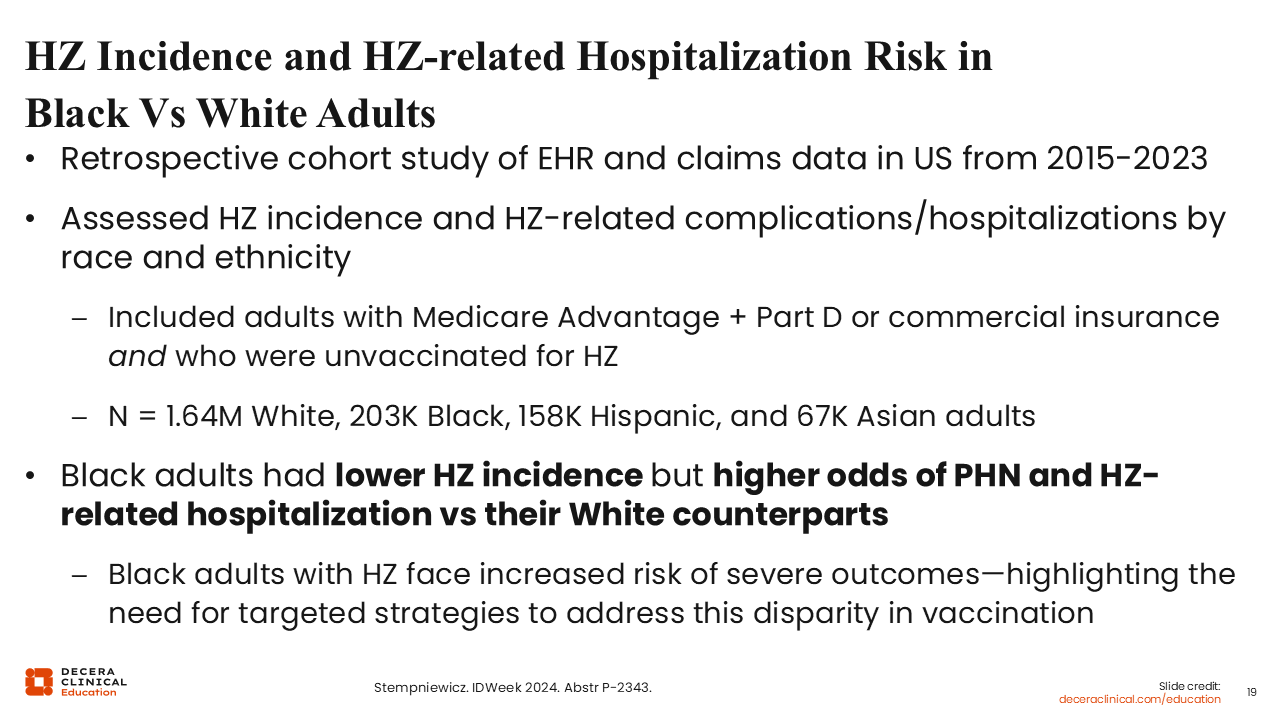
HZ Incidence and HZ-related Hospitalization Risk in Black vs White Adults
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Let us move on to disparities in the shingles vaccine access and uptake. A study presented at IDWeek in 2024—and now published— found differences in the incidence of herpes zoster infection and the development of PHN- and herpes zoster–related hospitalization by race and ethnicity. An interesting finding was that Black patients had a lower incidence of herpes zoster infection but higher odds of PHN- and herpes zoster–related hospitalization.
What does that mean? Despite the lower incidence of shingles among Black patients, they face a greater risk of severe outcomes. This emphasizes the need for reducing that health disparity with vaccination because these patients can be protected.24
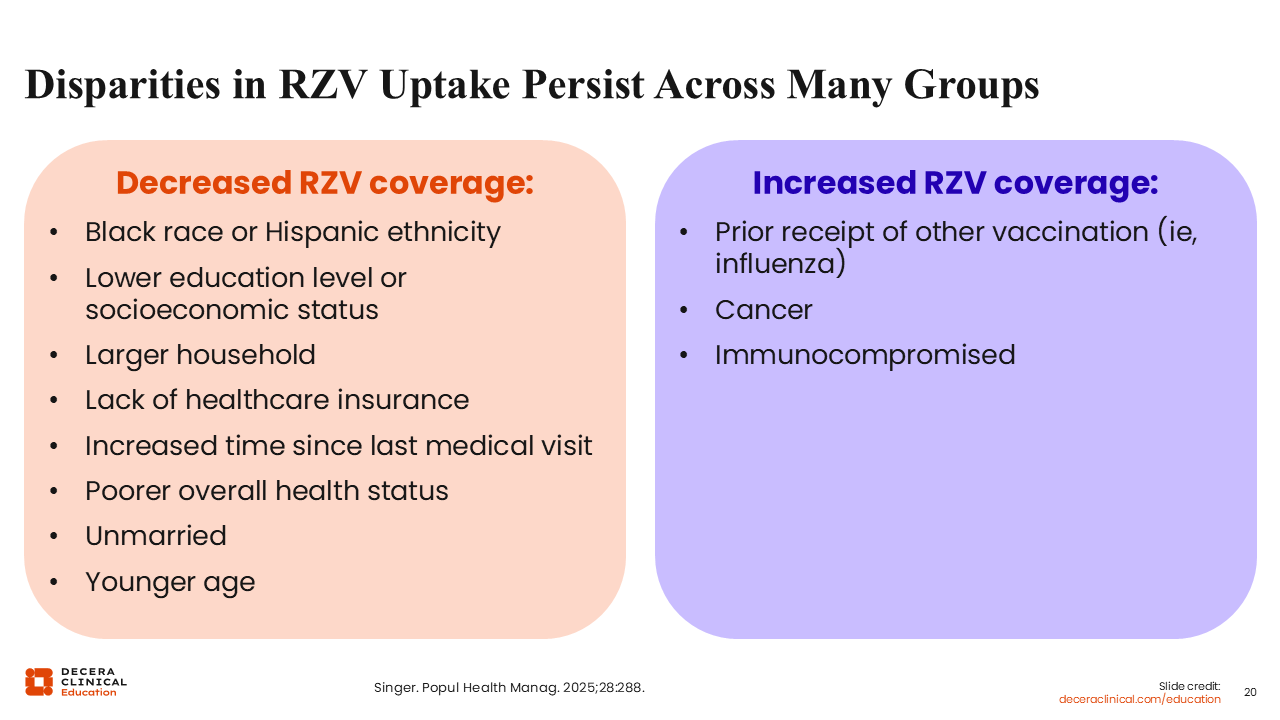
Disparities in RZV Uptake Persist Across Many Groups
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Let us consider other disparities and why they exist. First, RZV coverage remains lower among Black and Hispanic adults compared with White adults despite ACIP recommendations. RZV coverage rates are generally higher among those with an associates or more advanced degree. But coverage is significantly lower among those with low socioeconomic status or a lack of health insurance coverage. Finally, RZV coverage is significantly higher among those with coadministration of the influenza vaccination. So those who do not receive the influenza vaccine are less likely to also get the shingles vaccine.25
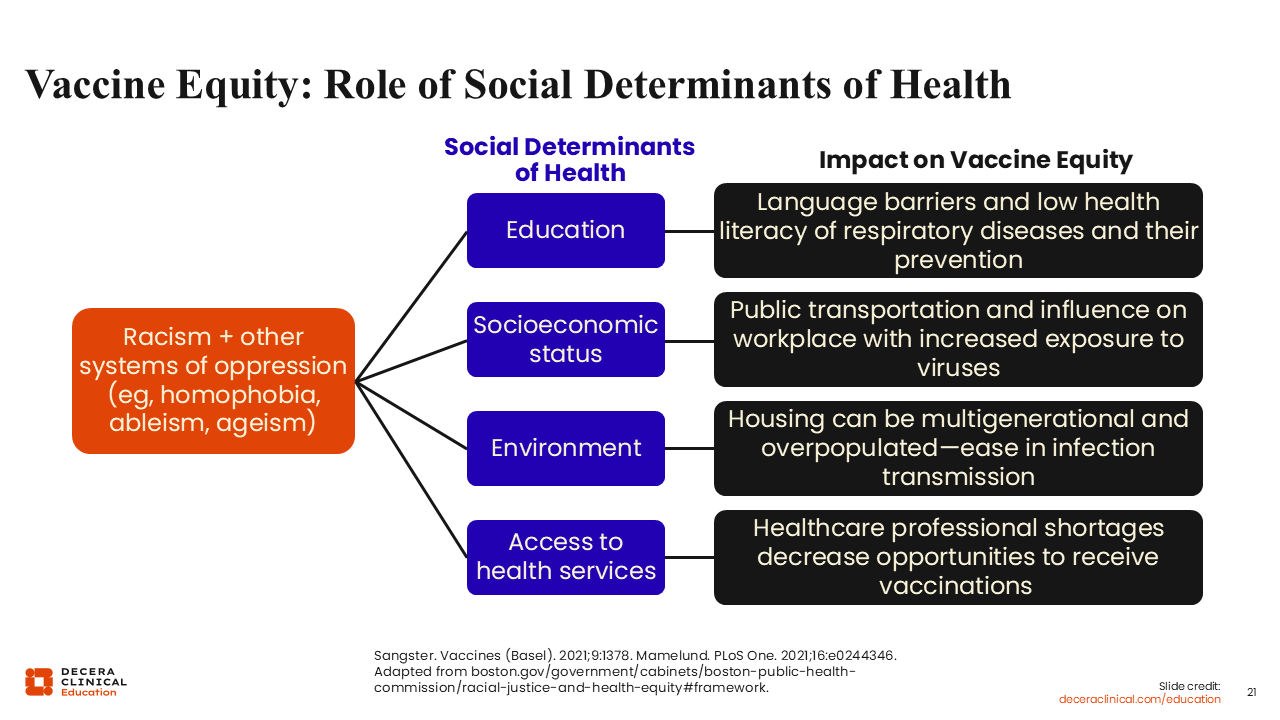
Vaccine Equity: Role of Social Determinants of Health
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Now, we must think about what supports or leads to the drivers of these inequities. When I think about it, especially from the standpoint of underserved and marginalized groups, Black and Hispanic adults being less likely to receive coverage for the RZV vaccine involves racism and other systems of oppression (homophobia, ableism, classism, ageism) that feed into social determinants of health. These all impact vaccine equity, as shown on this slide.
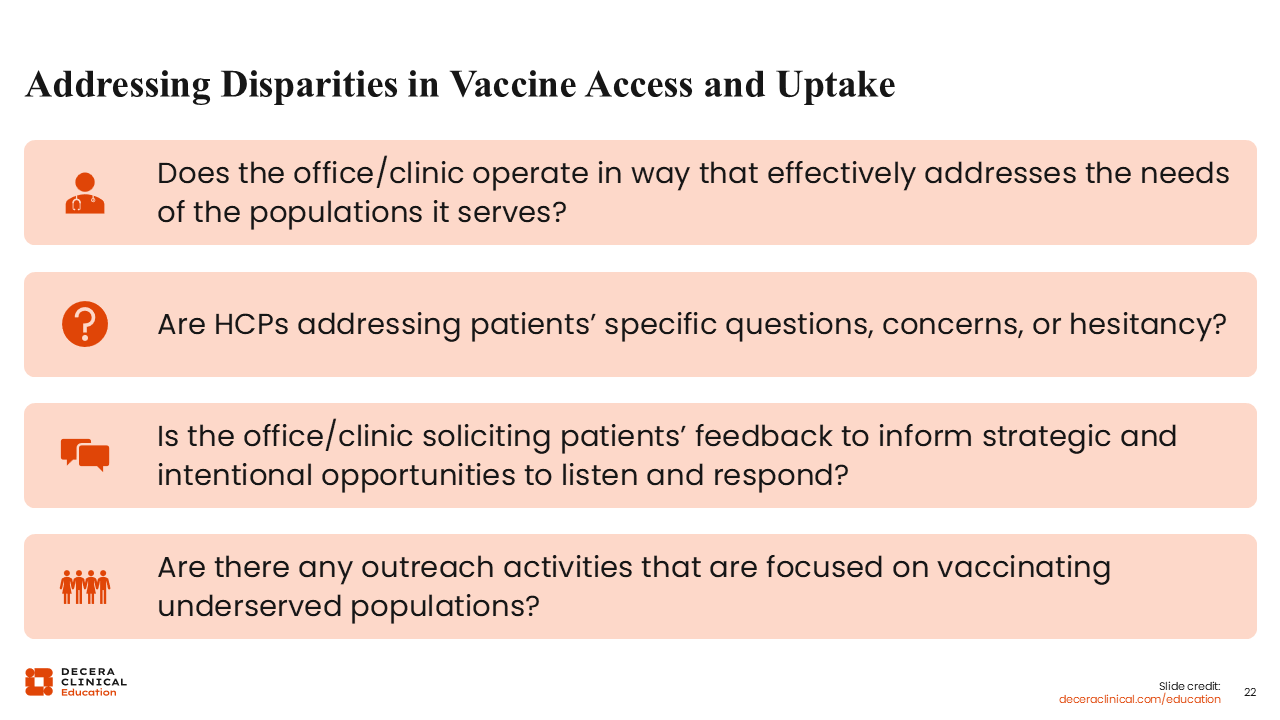
Addressing Disparities in Vaccine Access and Uptake
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Some questions to ask yourself when addressing health disparities in vaccine access and uptake are on this slide.
I think the second question, about addressing specific concerns or hesitancy-related questions, is critical. Sometimes a concern hits a point that we do not want to dip into as HCPs, but this is the oath that we took. We all agreed to do no harm and do good unto our patients. Therefore, we must have these conversations with patients.
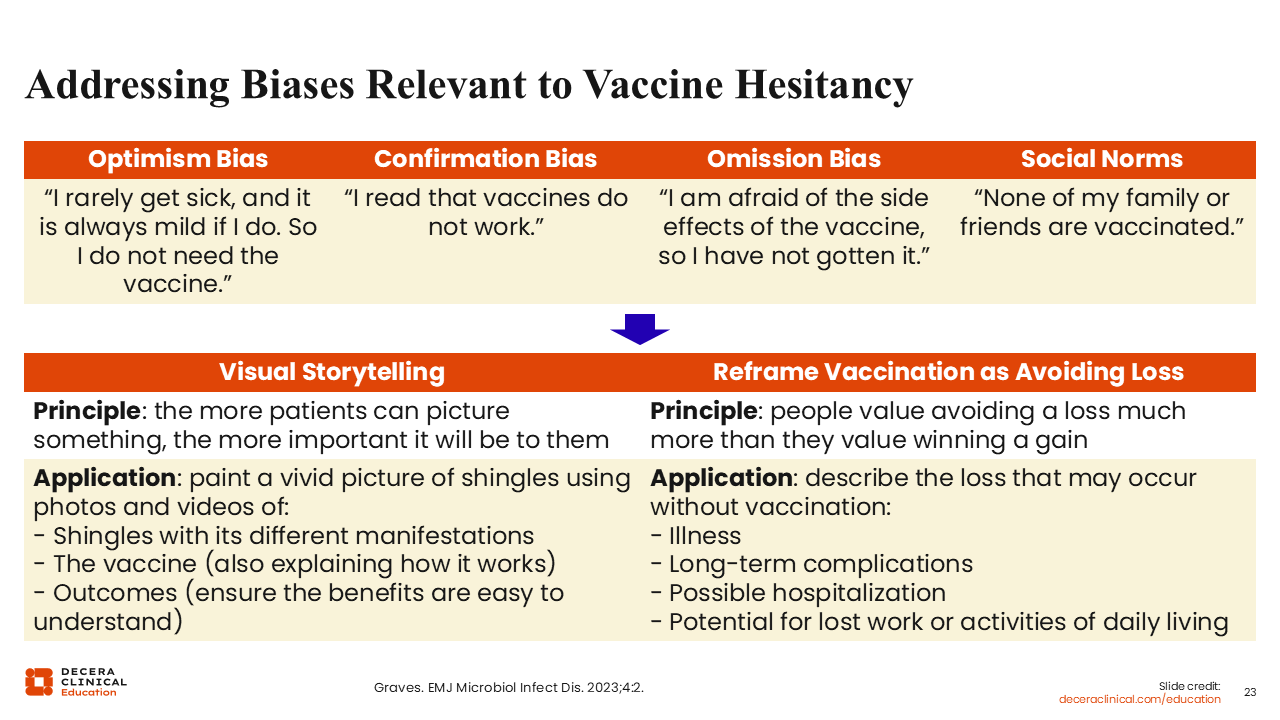
Addressing Biases Relevant to Vaccine Hesitance
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
How can we combat biases to improve vaccine uptake? Well, we can do visual storytelling. As HCPs, there is a real role for us to be storytellers.
The main principle is that the more patients can picture something, the more important it is for them. As you discuss the presentation of shingles and vesicular rash with patients, they may respond, “Oh, my goodness, that probably feels very terrible.” For the other manifestations of shingles, we can tell patients, "Think about how that will feel. Think about the pain that it would cause."
Many patients know at least 1 person who has suffered from PHN, and that is enough for them to understand the importance of vaccination. The testimony of "my brother had PHN and he has not had the same quality of life since" can become the story that sits in people's minds. They might think, "The vaccine can prevent this, so it is something that I should get."
Another approach is to present the shingles vaccine as a preventative—reframing it as avoiding a loss. People do not want to be hospitalized or have long-term complications. These things can then lead to the inability to work and income loss. That is a conversation to have with patients.26 Not only are these vaccines good for preventing complications, but they also can prevent hospitalization.
A big part of the human experience is community, socialization, and integration with others. Preventing shingles allows people to further integrate into their family and loved ones as they age.
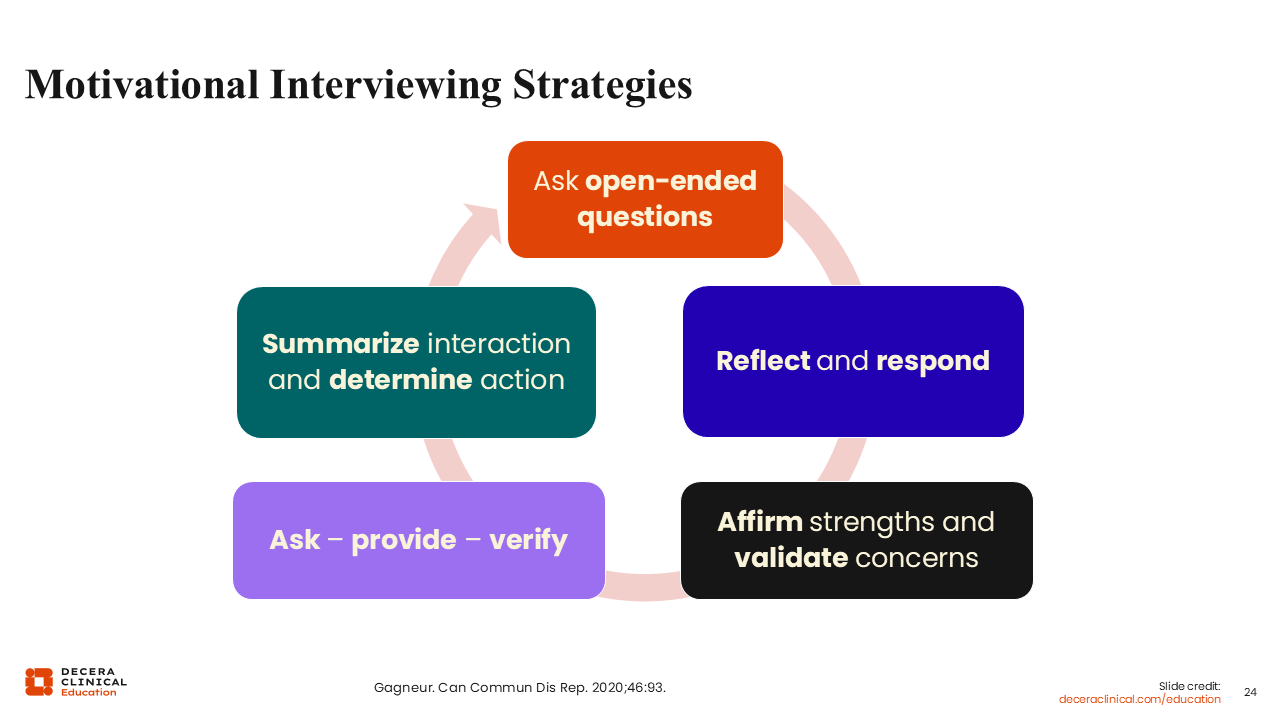
Motivational Interviewing Strategies
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
What can HCPs do to encourage shingles vaccine uptake? First, we can employ motivational interviewing strategies. That means, for example, asking patients open-ended questions and reflecting on their answers before responding.27 Other strategies are shown on this slide.
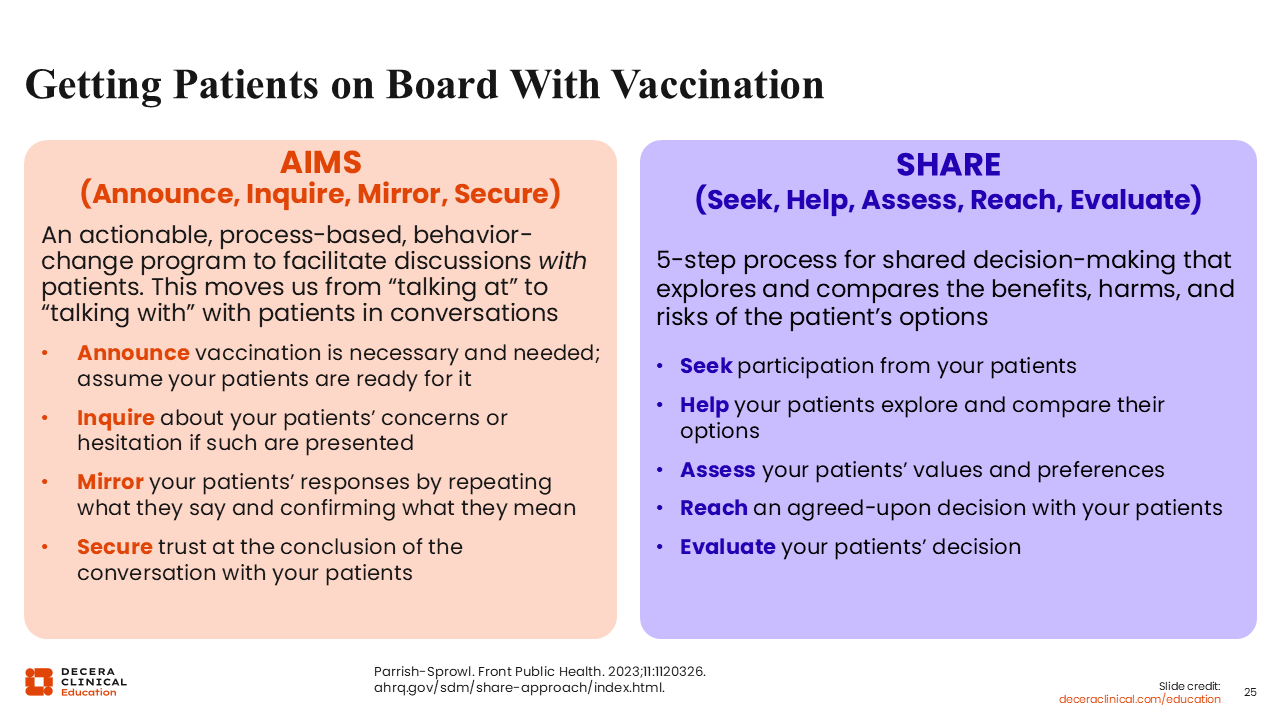
Getting Patients on Board With Vaccination
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
This slide illustrates some guiding points for getting patients on board with vaccination. There are “AIMS” and “SHARE”—2 different, evidence-based frameworks HCPs can use.28,29
Something that a colleague told me once is that she would listen to what it was that patients brought forth. She would respond, "Yes, you have heard this information. I am not going to invalidate that you have heard this information, and…" After that "and," she would provide patients the facts. I think that is a great way for us to approach the shingles vaccine, especially in the current climate. We should acknowledge what patients have heard, after which we, as knowledgeable HCPs, should provide any information that we have.
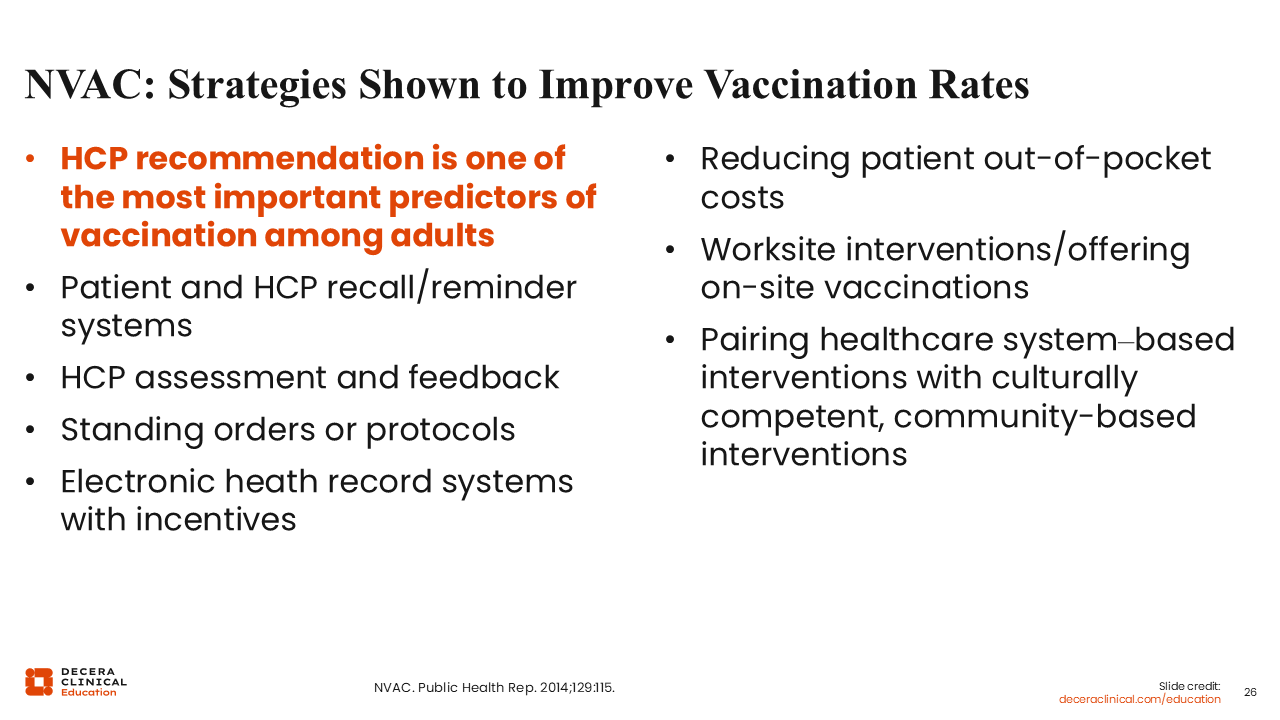
NVAC: Strategies Shown to Improve Vaccination Rates
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
There other strategies that can help us improve vaccine uptake. For example, HCP recommendation is one of the strongest predictors of vaccination. So please remember the power of your own recommendation.
Recall and reminder systems, standing orders and protocols, and incentives are all tools we can use to improve shingles vaccine uptake.
We should also try to reduce patients’ out-of-pocket costs when possible. Many people who are 65 years of age or older do not know that their vaccine is covered by Medicare Part D. That cost factor can be prohibitive. We must bring up these coverage opportunities (Medicare Part D, commercial health insurance, etc).
Finally, we can pair healthcare system–based interventions with culturally competent and community-based interventions.30
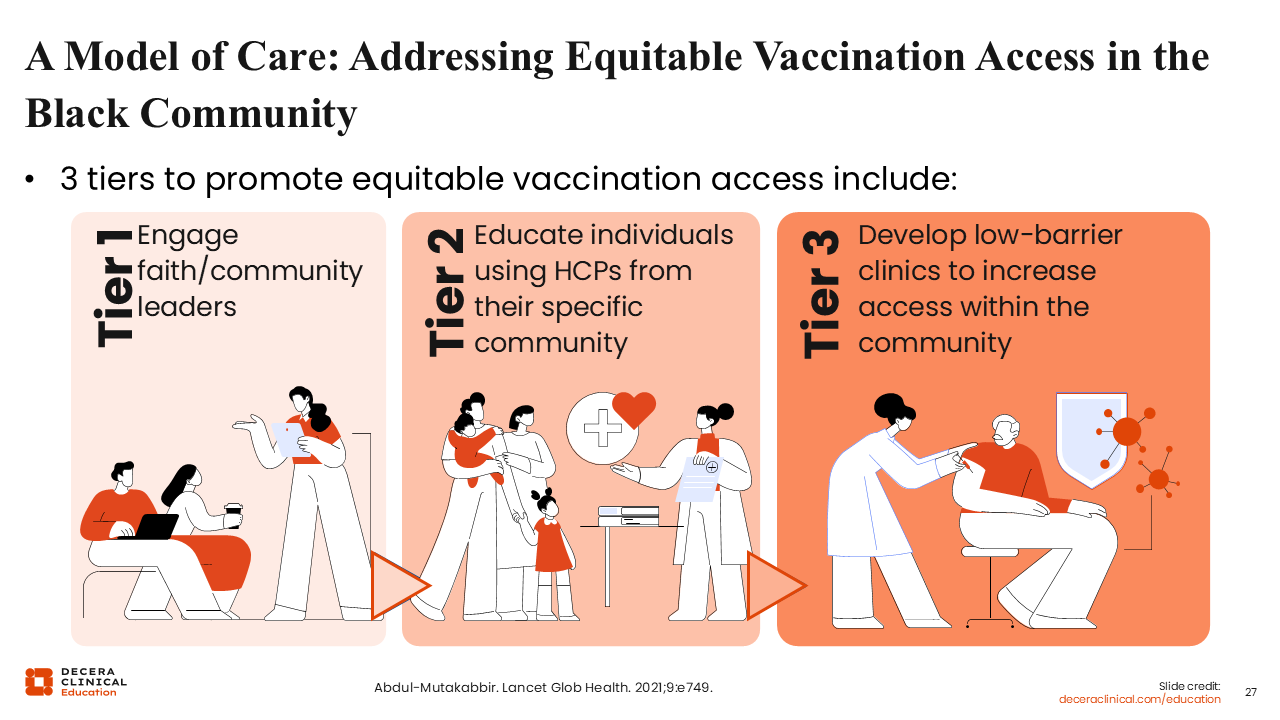
A Model of Care: Addressing Equitable Vaccination Access in the Black Community
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Here’s an example for the non-Hispanic Black community—the community that I identify with— where I worked with local organizations to develop a community-based approach to increase vaccine uptake. This work started during the COVID-19 pandemic to improve vaccination among community members.
There are 3 tiers. In tier 1, we started by engaging faith and community leaders. I worked with the community to reach out to their local churches and faith leaders to see if my team could conduct an educational intervention there.
In tier 2, we then provided the education within the community. We identified 4 churches to visit from September to December. And we went into these churches to provide a 45-minute education session about preventable viruses and vaccines.
In tier 3, We provided the vaccines that we discussed within the education session via low-barrier clinics. In these clinics, we tried to address any barriers patients faced within a single setting. This approach allowed us to address the education and access limitation to vaccination all in 1 fell swoop.31
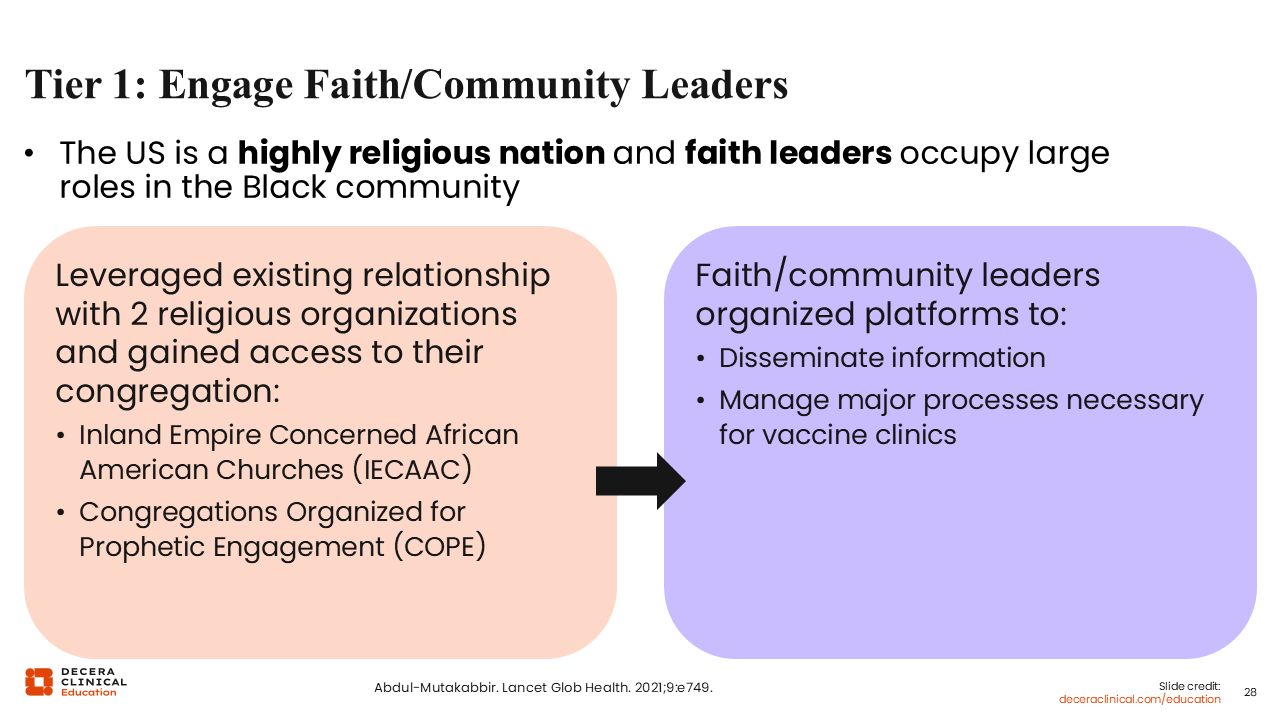
Tier 1: Engage Faith/Community Leaders
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Going into more detail about tier 1, HCPs must work with a community-based organization to do this. That community-based organization helps with facilitating communication with local churches and their parishioners. In the United States, especially for historically marginalized groups, faith leaders and community play a big role.
It has been great for me to not only work with the community directly, but to learn from the community in this way. In my work, we also used a survey-based study to collect perspectives on how folks in the community felt about the vaccine, if they received previous education, or if they had previous knowledge of them. Tier 1 has been very impactful.31
Tier 2: Provide Vaccine Education Through Black HCPs
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
With Tier 2, what HCPs should do is provide vaccine education. When I am providing this education, I talk through all of those points that Drs Restrepo and Carrico brought up. I discuss the pathophysiology of the disease, how herpes zoster looks, and more of more importance, how herpes zoster presents on darker skin tones. This is important because it is the lack of knowing how it is supposed to appear that prevents people from being diagnosed, which then can lead to long-term complications.
Next, I talk about the mechanism of the vaccine. I try to show the community that I respect them enough to ensure that they are educated on every element of the vaccine.
I do not dumb it down. Rather, I translate the medical information in an easy, accessible way. I talk about how the vaccine works and the fact that an adjuvant is included in the zoster vaccine option.
I also discuss the AEs that could be experienced after vaccination, especially considering that myalgias or arthralgias can keep people from getting the second dose. I also talk about the importance of receiving the second dose, but I want to let them know what to expect. I do not want to mince that information either because I do not want that to be the limitation for uptake.
The biggest part for me is discussing the impact of vaccination in underserved communities. I do not think folks are aware of the complications and how they are more likely to experience them because of the health disparities their community faces. So I work hard to ensure the community receives all this information.31
In my work, what we have seen is an increase in people’s willingness to receive the vaccine after attending education sessions. We also have seen folks actually get vaccinated directly following the education session. So it has been such a great moment of growth. I am actually preparing a publication about this, as it has been a fruitful experience.
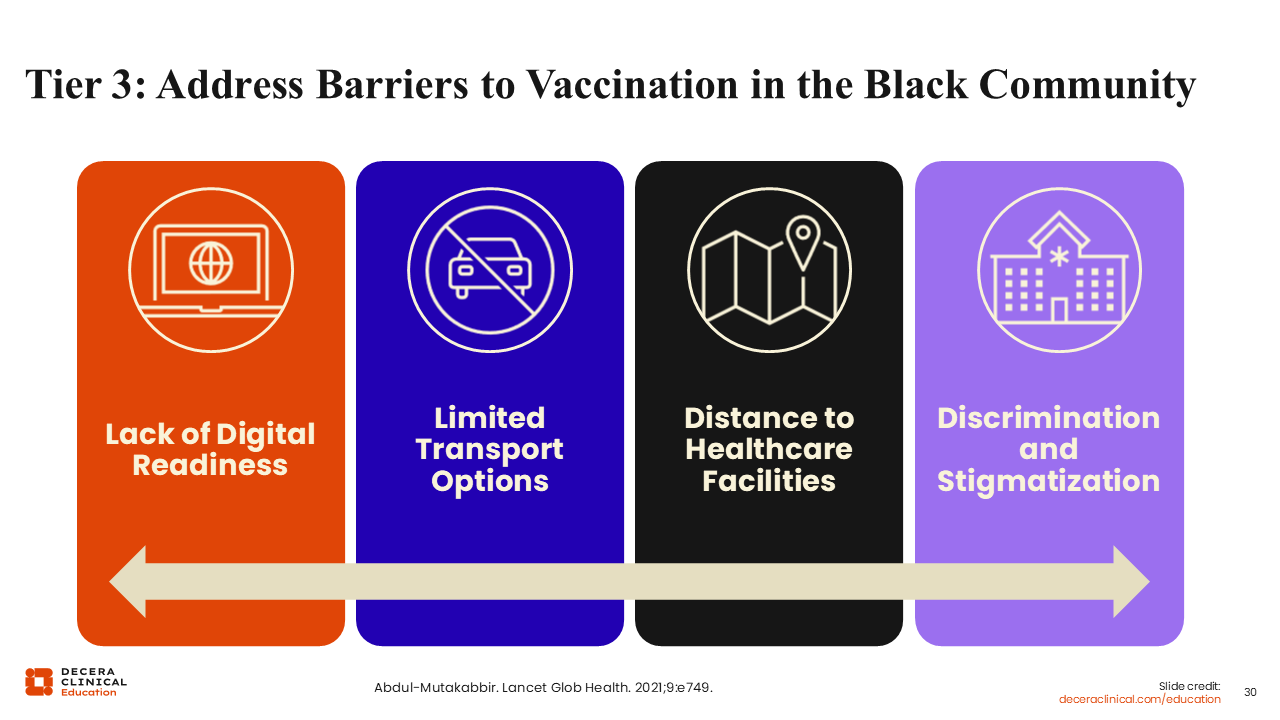
Tier 3: Address Barriers to Vaccination in the Black Community
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
Last is tier 3, where HCPs provide the vaccines. HCPs should do so by taking out many of the limitations that are present in everyday practice. For example, my team and I understood that digital readiness—the need for people being able to reserve spots online—could be a limitation for receiving vaccines. Therefore, we offered everything on site, so that would not be a barrier.
We also addressed the transportation need. If community members were already at church, then we offered this clinic in the church. In doing so, we limited the need to drive longer distances to access local healthcare facilities.
I worked with an independent pharmacy that provided many of their own services, too. The pharmacy staff called the people who received the first dose to tell them when it is time to return for dose 2.
Finally, we worked hard to remove discrimination and stigmatization. We wanted to make this a great setting that is comfortable and fun for people. We wanted the community to associate vaccination with a good time. With this, we ensure that vaccination is a decision that people continue to make—that vaccine uptake is continued and long-lasting.31
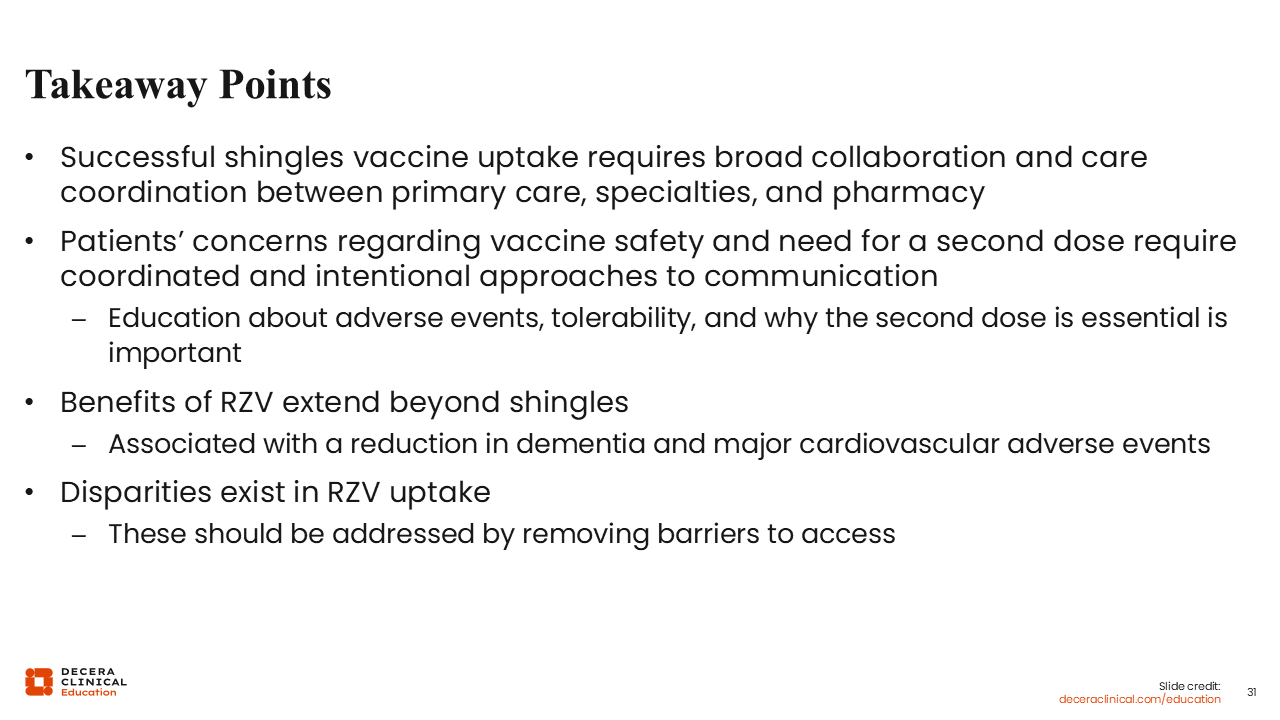
Takeaway Points
Ruth Carrico, PhD, DNP, FNP-C, FAAN:
Successful shingles vaccination requires a broad collaboration. We must ensure that we have care coordination across primary care, specialties, and pharmacy. In addition, we should address patients’ concerns about the safety and benefits of the shingles vaccine.
Dalilah Restrepo, MD:
Vaccination is a journey. It is not simply at 1 point in time that we recommend it. If patients decline at that moment, we do not just close the door on them.
As HCPs, we have been on this journey longer than our patients have because we have been studying this for years. It is much easier for us to come to a conclusion after we read a clinical trial and have all the background information needed; patients, on the other hand, have just started their journey.
In my practice, I also use opportunities presented in the hospital to discuss vaccination with patients. Remember, we are trying to help patients avoid hospitalization with most vaccines. When they do end up in the hospital with an illness, this is a prime opportunity. I have had a lot of success with this when patients are admitted for myocardial infarction, transient ischemic attack, or herpes zoster itself. The next day, I come into in the patient’s room and their whole family is receptive to hearing about shingles vaccination.
HCPs should prioritize preventing patients from landing in the hospital in the first place. No discussion regarding longevity and wellness should be had without discussing vaccination.
Jacinda (JAM) Abdul-Mutakabbir, PharmD, MPH:
The first interaction is not the only interaction you will have with patients. There have been times when I have recommended vaccination in education sessions, and someone will attend 4 sessions before they decide that they want to be vaccinated. You must be open and receptive; do not take a “no” as a shot to your ego. This is more than a single decision that patients make. Furthermore, it is our job to ensure that they have all the information necessary to make an informed decision for themselves.
There are numerous checkpoints in healthcare where HCPs outside of primary care can be involved in helping improve vaccine uptake. So empower your staff and the people around you to engage in vaccine conversations with their patients. We do not want all the pressure placed on 1 particular discipline.
Ruth Carrico, PhD, DNP, FNP-C, FAAN:
Bringing it home, this is a team-based opportunity across the healthcare continuum and within every discipline. Patients are the constant in the equation of healthcare, and every opportunity we have for interaction should include discussion about vaccines, including the shingles vaccine.